
Abstract
Objective:
We assessed and compared the performance levels of a fiber-coupled fluorescence affinity sensor (FAS) for glucose detection in the intradermal tissue and intravascular bed during glucose clamping and insulin administration in a large animal model.
Research Design and Methods:
The FAS (BioTex Inc., Houston, TX) was implanted in interstitial tissue and in the intravenous space in nondiabetic, anesthetized pigs over 6–7 h. For intradermal assessment, a needle-type FAS was implanted in the upper back using a hypodermic needle. For intravenous assessment, the FAS was inserted through a catheter into the femoral artery and vein. Blood glucose changes were induced by infusion of dextrose and insulin through a catheterized ear or jugular vein.
Results:
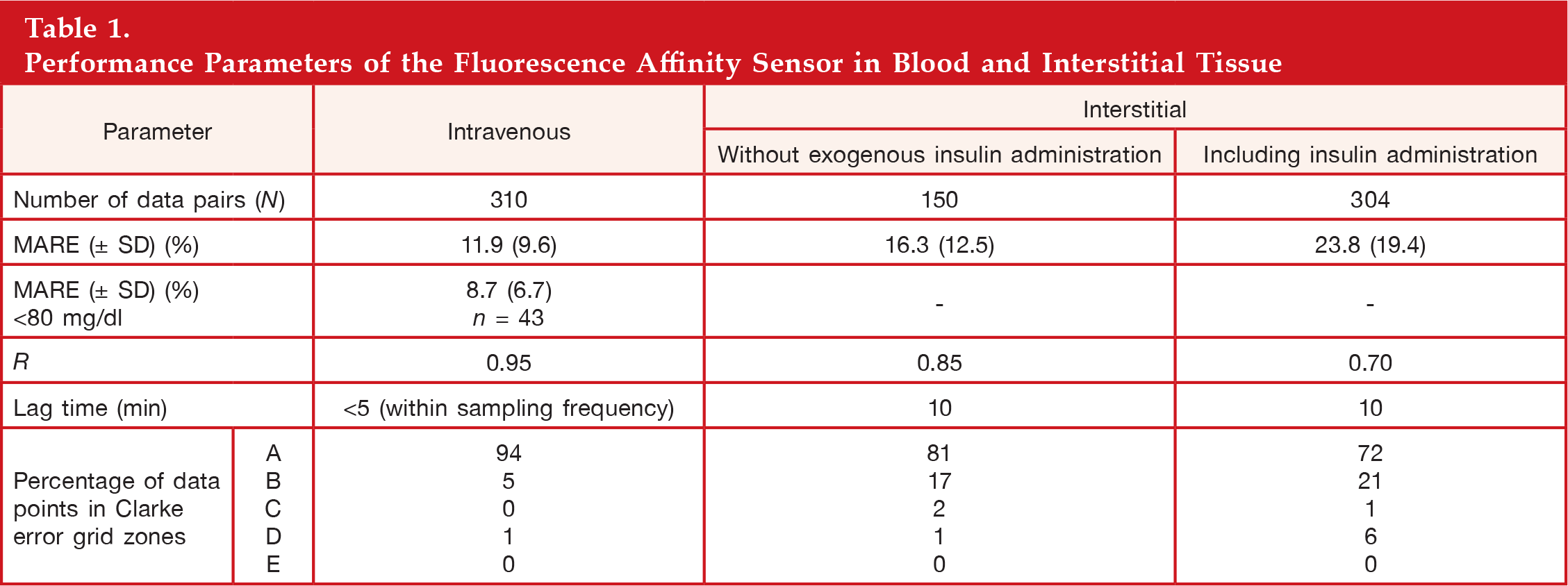
Based on retrospective analysis, the mean absolute relative error (MARE) of the sensor in blood and interstitial tissue was 11.9% [standard deviation (SD) = ±9.6%] and 23.8% (SD = ±19.4%), respectively. When excluding data sets from sensors that were affected by exogenous insulin, the MARE for those sensors tested in interstitial tissue was reduced to 16.3% (SD = ±12.5%).
Conclusions:
The study demonstrated that the performance level of the FAS device implanted in interstitial tissue and blood can be very high. However, under certain circumstances, exogenous insulin caused the glucose concentration in interstitial tissue to be lower than in blood, which resulted in an overall lower level of accuracy of the FAS device. How significant this physiological effect is in insulin-treated persons with diabetes remains to be seen. In contrast, the level of accuracy of the FAS device in blood was very high because of high mass transfer conditions in blood. While the use of the FAS in both body sites will need further validation, its application in critically ill patients looks particularly promising.
Introduction
The Diabetes Control and Complications Trial demonstrated that intensive management of blood glucose in people with type 1 and 2 diabetes is an effective means to prevent or at least slow progression of diabetes complications such as kidney failure, heart disease, gangrene, and blindness.1–4 Furthermore, other studies have shown that hyperglycemia is associated with poor outcomes in critically ill patients.5–9 Through better management of hyperglycemia in those hospitalized patients, studies have found that this can lead to reductions in complications (ventilation, earlier discharge), infection, mortality, and morbidity and to overall better outcome in intensive care unit settings.10–15 Various confounding factors—lability of health status of critically ill patients and subjects with type 1 diabetes, mediocre point-of-care glucometer accuracy, matrix effects in blood samples, and interfering components—indicate the imperfection of current state-of-the-art management of glycemic excursions in diabetes patients and critically ill patients. To address the need, implementation of an intravenous or subcutaneous glucose-monitoring device is currently being considered to be the most feasible solution. Combining such a continuous glucose-monitoring device with an insulin pump, both controlled by a closed-loop algorithm, is the general goal in order to provide a robust system that can minimize hyperglycemic and hypoglycemic episodes to a healthy level. 16
Several companies have commercialized subcutaneous glucose-monitoring devices based on electroenzymatic sensors.17–21 Some of them have been investigated for their suitability as part of a closed-loop system.22–25 On the other hand, fluorescence affinity sensors (FASs) have been generally recognized as a viable alternative to electroenzymatic sensors for glucose monitoring. They would benefit from the fact that signal generation is based on a binding equilibrium (that means without consuming glucose) and is not sensitive to oxygen and other electrode-active interferences.26–39 Also, the fluorescence signal is available immediately after system turn-on during operation, while the electroenzymatic sensors require a certain warm-up time until stable signal levels are reached.
The fiber-coupled FAS device (BioTex Inc., Houston, TX) was developed to detect glucose levels in body fluids.40,41 The sensor determines glucose concentration by measuring the fluorescence at 675 nm (glucose sensitive) and 780 nm (glucose insensitive) as the result of the competitive displacement of dextran from concanavalin A hydrogel by glucose (see
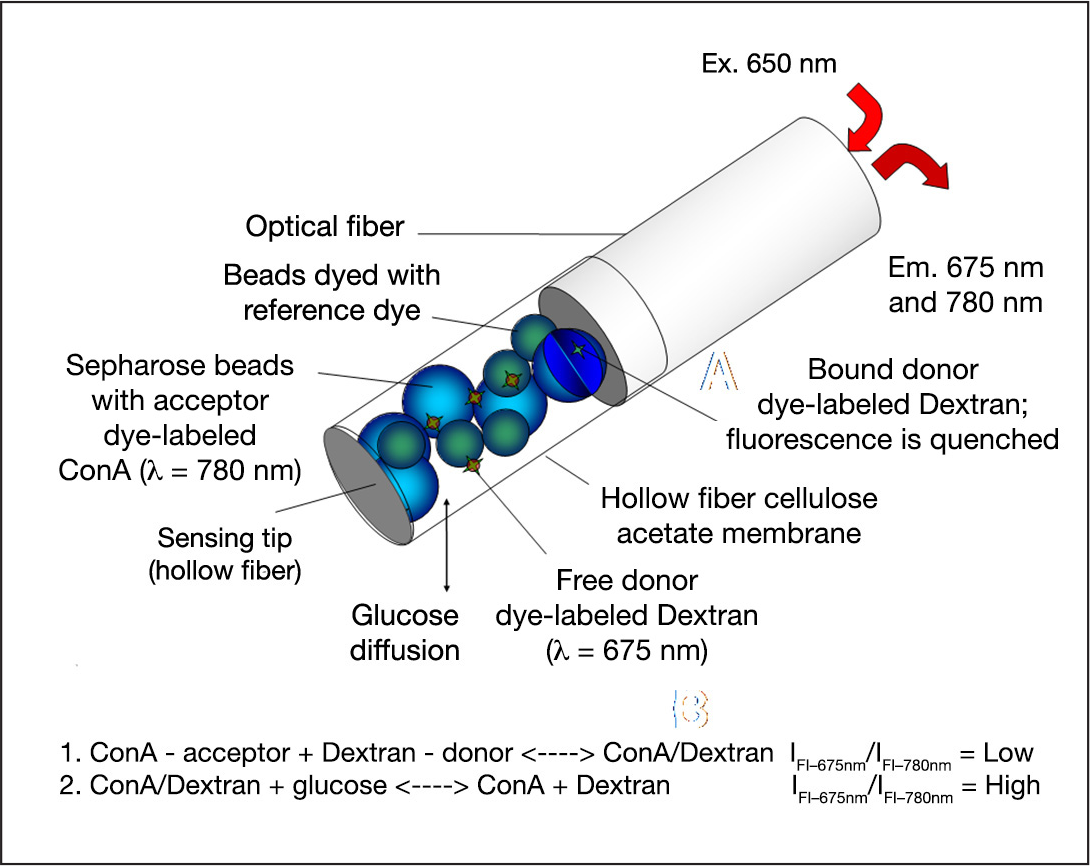
Detection scheme of the FAS for determining glucose concentration. ConA, concanavalin A.
To account for optical effects in the detection fluid, the fluorescence ratio of 675 nm (glucose sensitive) versus 780 nm (glucose insensitive) is determined. At increasing glucose concentrations, the fluorescence ratio signal increases proportionally to the glucose concentration. The near-red long-wavelength dyes possess strong fluorescent efficiency and excellent photostability. Further, the near-infrared wavelength region confers the ability to monitor inexpensive excitation and detection components. The feasibility of the subcutaneous sensor to detect glucose accurately in small and large animals and, more recently, in humans was demonstrated.42,43
In this article, we studied the performance of the FAS device in interstitial tissue and in blood of a large animal model to better understand how the site of implantation can affect sensor accuracy. The obvious differences between blood and interstitial tissue are the lack of lag time required for glucose to pass the blood–tissue barrier and the highly convective mass transfer conditions in blood. We were also interested in finding out whether the accuracy of the FAS device in the interstitial tissue would be influenced by exogenous insulin, which was demonstrated to affect the relationship between interstitial glucose concentration and glycemia. Answering those questions will be helpful in gauging the practical implications of the FAS device for continuous glucose monitoring in the different respective body environments.
Materials and Methods
Fluorescence Affinity Sensor Design and Manufacture
The FAS device is a needle-type, fiber-optic-based glucose sensor whose detection principle is based on fluorescence resonance energy transfer of the glucose-specific chemistry—housed in a hollow fiber—in response to glucose level changes.
A detailed description of the design, manufacture, mechanism, and in vitro and in vivo performance of the BioTex (Houston, TX) FAS was reported in an earlier paper.
41
In brief, one end of a 165 μm diameter multimode polymer-coated optical fiber was mechanically spliced to two 105 μm diameter silica optical fibers (
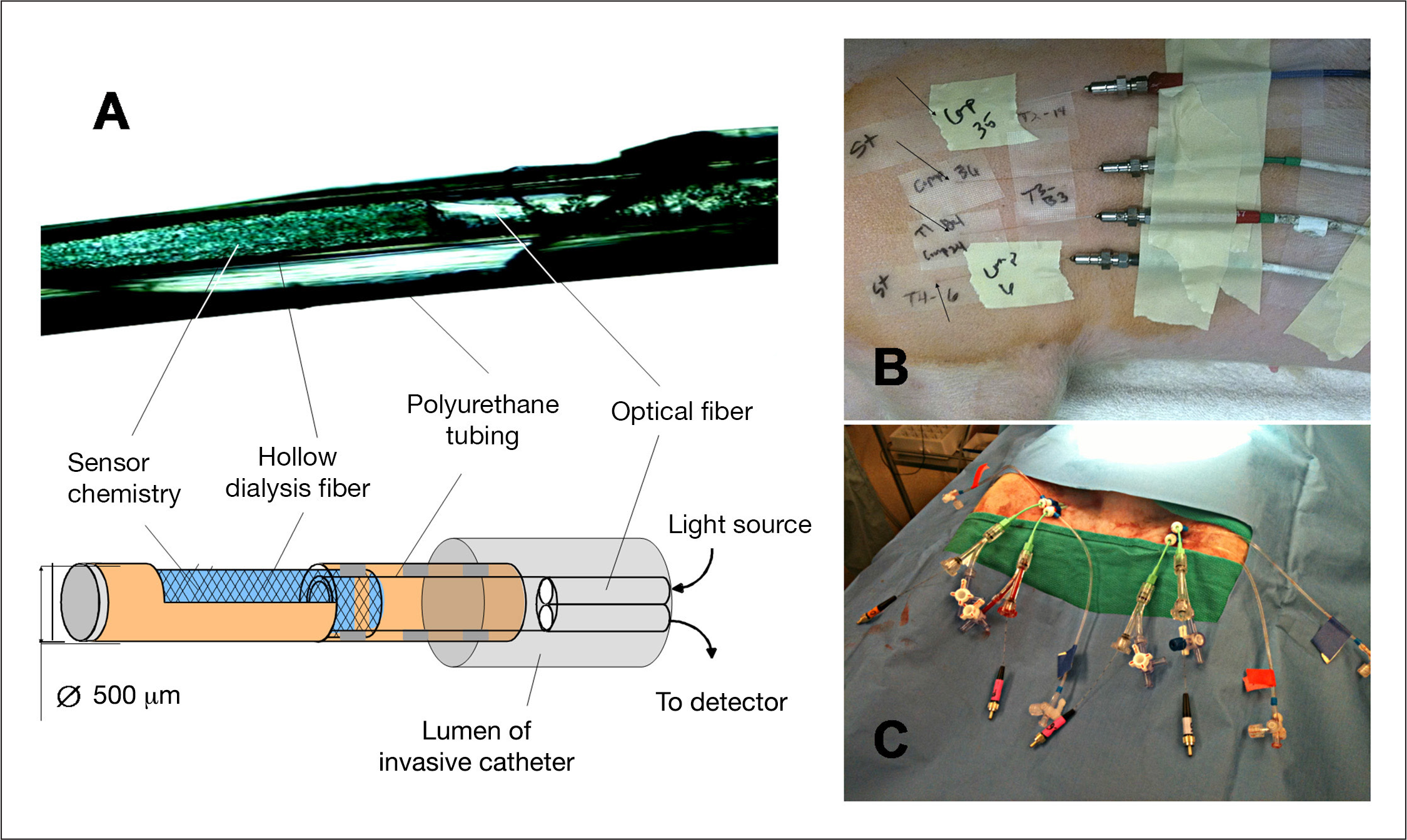
The BioTex FAS and the experimental setup during animal trials.
Fluorescence Affinity Sensor Hardware and Fluorescence Detection
After the sensors were placed in skin and blood vessels, the proximal end of the FAS optical fiber (approximate length 100 cm) was connected to the FAS detector instrumentation. The FAS detector instrumentation consisted of a light source and a wavelength-specific light detector (USB-2000 spectrophotometer) connected to a laptop computer that runs the glucose-signal analyzing software GSpectrum. The optical fiber connecting the FAS with the FAS instrumentation transmitted excitation light (λ = 647 nm) to the sensor. The fluorescence generated by the FAS chemistry in response to glucose was coupled back through the same optical fiber into the light detector. The light detector captured wavelength-specific fluorescence between 650 and 900 nm. Raw spectral intensity data were obtained by averaging three spectra taken within 30 s at 5 min intervals. Raw spectral data were then corrected by subtracting background intensity calculated as mean value from 1500 to 1800 pixels, and the ratio was taken by averaging 20 pixels at 675 nm (glucose-sensitive peak) and 780 nm (glucose-insensitive peak); this is defined as the ratio signal. The software automatically updated the FAS signal every 5 min.
Fluorescence Affinity Sensor Implantation into Interstitial Tissue in Pigs
Juvenile farm pigs (nondiabetic, weighing 20–30 kg) were included in this study. Pigs were pre-anesthetized with ketamine (1 ml/50 kg), scrubbed thoroughly on the dorsal site with povidone and warm water, and then maintained with 1–4% isoflurane by mask. To implant the sensors, a 16 G intravenous catheter was inserted into the intradermal tissue (approximately 2 cm) at a shallow angle between shoulder and midline of the pig (
Animal studies were carried out at an Association for the Assessment and Accreditation of Laboratory Animal Care-accredited facility (Stillmeadow Inc., Sugarland, TX) and in accordance with an Institutional Animal Care and Use Committee-approved protocol (#15300–11).
Fluorescence Affinity Sensor Insertion into Femoral Blood Vessels
Juvenile farm pigs (nondiabetic, 20–25 kg) undergoing procedures were sedated using Telazol 4–6 mg/kg and atropine sulfate 0.02–0.05 mg/kg and intubated. Then isoflurane was administered via facemask to induce general anesthesia for surgical interventions at a rate of 0.5% to 3.0%. Percutaneous access or surgical cutdowns were performed to access and catheterize the right and left femoral vein and artery. Two additional percutaneous jugular access sheaths were placed for dextrose infusion and glucose sampling. Up to four FAS devices per animal were implanted, two per access point using a 5–8 French-size intravenous catheter (
The animal study was performed in the Cardiovascular Research Laboratory at Texas Heart Institute in accordance with an Institutional Animal Care and Use Committee-approved protocol (#2012–09).
Glucose Clamp
In both experiments, glucose clamping was performed to maintain the subject's BG concentration at a relatively constant level over a period of time using a rate-controlled infusion of 50% dextrose. Multiple cycles (4–6) of increasing and decreasing glucose (40–360 mg/dl) were performed. Within each cycle, the animal's BG was maintained for 30–60 min.
Statistical Analysis
Measured FAS data points (ratio signal) were paired with the corresponding BG concentrations collected at the same time.
For retrospective calibration, all data points collected from 100 min until the end of the experiment were included in the calibration for all sensors shown here. Data pairs from the initial 100 min were excluded from the analysis to minimize bias when comparing the accuracy of different sensors in different body locations during the acute phase, because a few sensors needed time to equilibrate to the in vivo environment. Correlation coefficient (R) and mean absolute relative error (MARE) were computed to assess measurement accuracy. For each sensor, the minima of R was calculated for different lag-time offsets (delay in sensor response over glucose concentration change in capillary blood) from 0 to 20 min at 5 min intervals. Clarke error grid analysis was used to investigate the therapeutic significance of the differences in glucose concentrations between references and all sensor readings. For assessing clinical significance, the percentage of points in the A, B, C, D, and E regions of the Clarke error grid was then calculated for all matched data pairs except those collected during the first 100 min.
Results and Discussion
Accuracy of Fluorescence Affinity Sensor in Interstitial Tissue
The performance of the FAS implanted in interstitial tissue is shown in
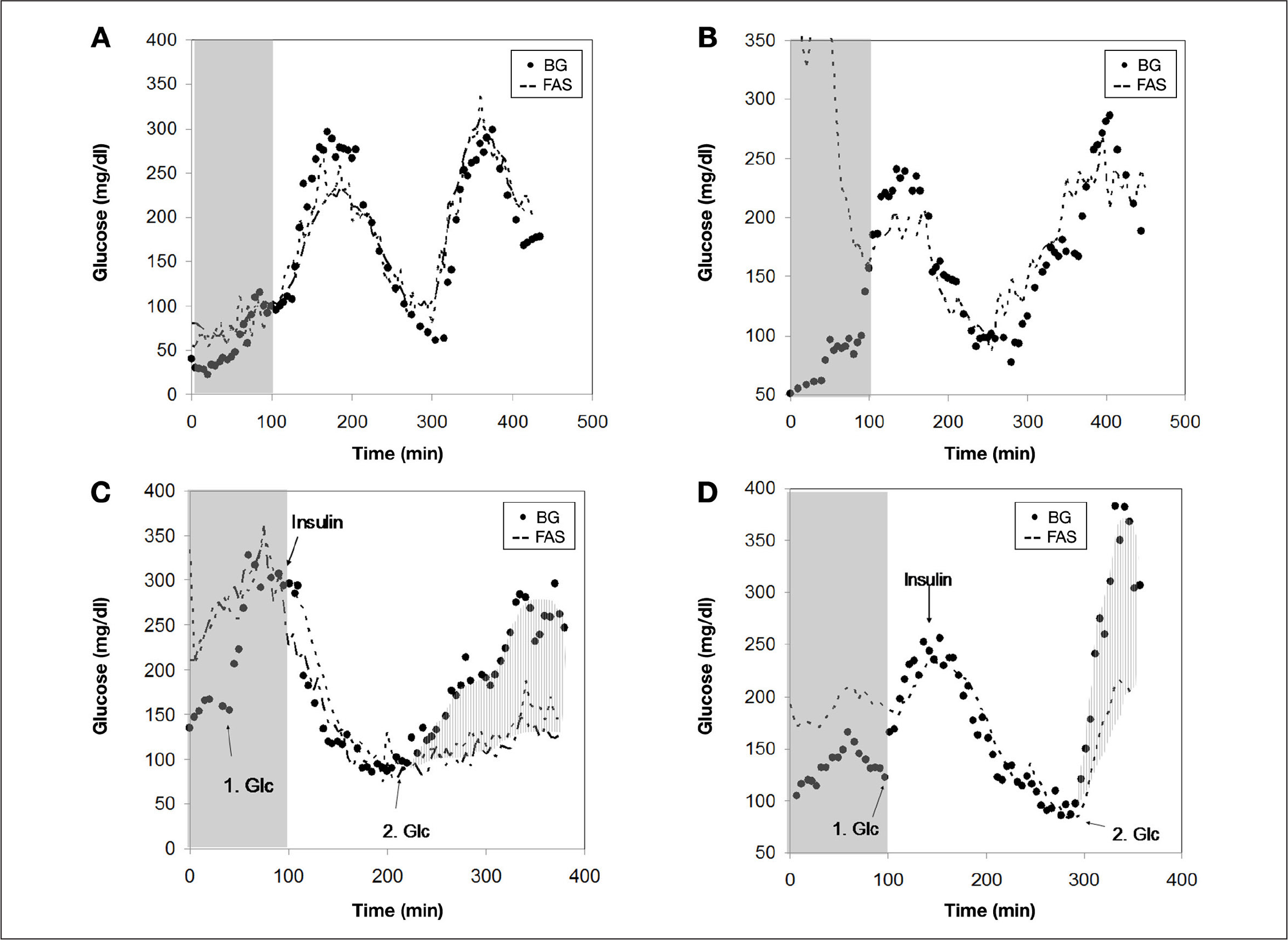
Glucose infusion responses by the FAS implanted in interstitial tissue of pigs. Note that no insulin was administrated in
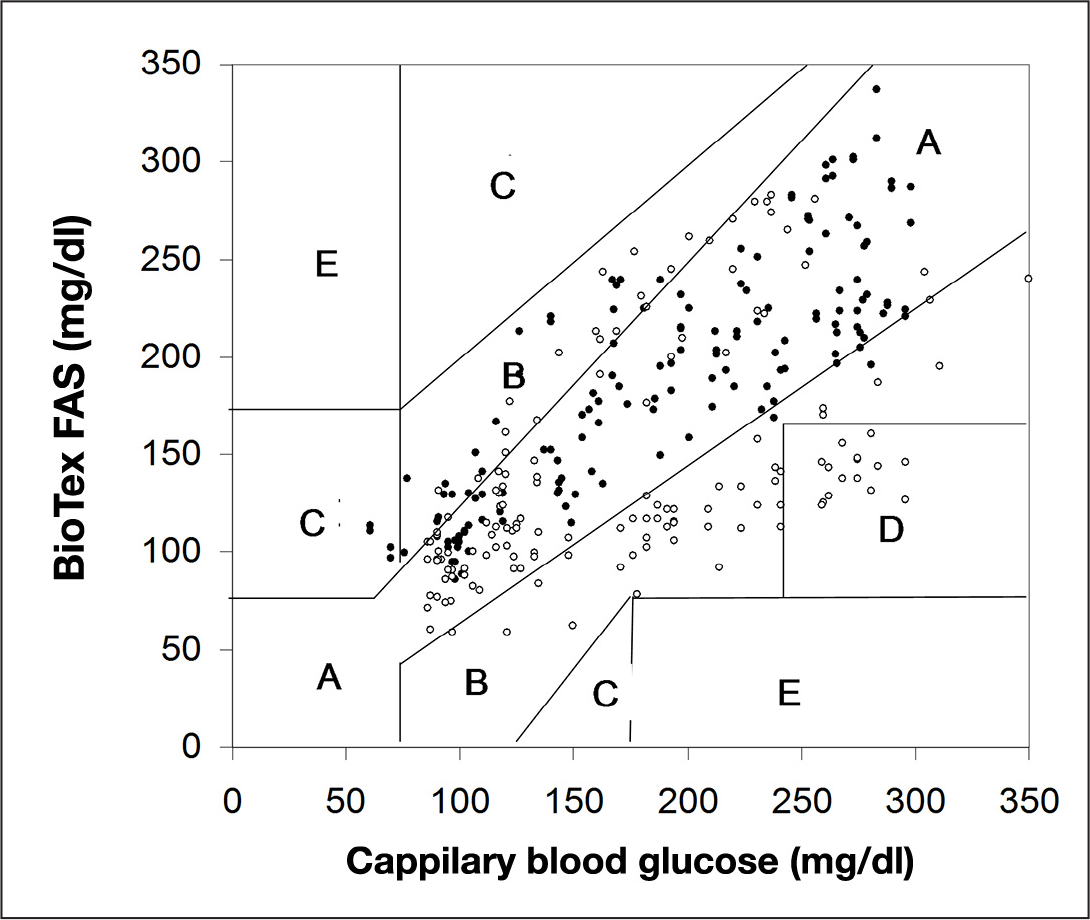
Clarke error grid analysis of FAS data in interstitial tissue. Solid and empty circles indicate data points collected from sensor data with and without exogenous insulin administration.
Performance Parameters of the Fluorescence Affinity Sensor in Blood and Interstitial Tissue
The particular phenomenon of measuring a reduced interstitial glucose concentration compared with plasma glucose after insulin-induced hypoglycemia during a second glucose load was previously observed in rats and humans. In both cases, an electroenzymatic glucose monitor was used.44–46 This suggests that this not an artifact related to the type of glucose-sensing device used but hints at an inherent physiological effect of endogenous insulin on the glucose metabolism in interstitial tissue. Aussedat and coauthors 44 proposed a model that suggests that hypoglycemia induced by exogenous insulin suppresses the transfer of glucose into interstitial tissue. As a result, interstitial glucose remains lower than plasma glucose during its return to basal value, suggesting that the stimulatory effect of endogenous insulin on peripheral glucose uptake is protracted. This model was validated through a number of experiments. 44 What does it mean for the subcutaneously implanted FAS? First, one could argue that, for in vivo assessment of FAS accuracy, data points collected during such a metabolic event should be excluded from the analysis since the reference BG concentration significantly deviates from the glucose concentration in the interstitial tissue, which is not device related. Second, the question, of course, is how significant this physiological observation is in insulin-treated patients with diabetes. It remains to be seen whether new approaches for correct interpretation of glucose excursions measured with the subcutaneous FAS will need to be implemented to compensate for such events.
Fluorescence Affinity Sensor Accuracy in Blood
The response of the FAS in blood vessels during glucose clamps and insulin infusion is shown in
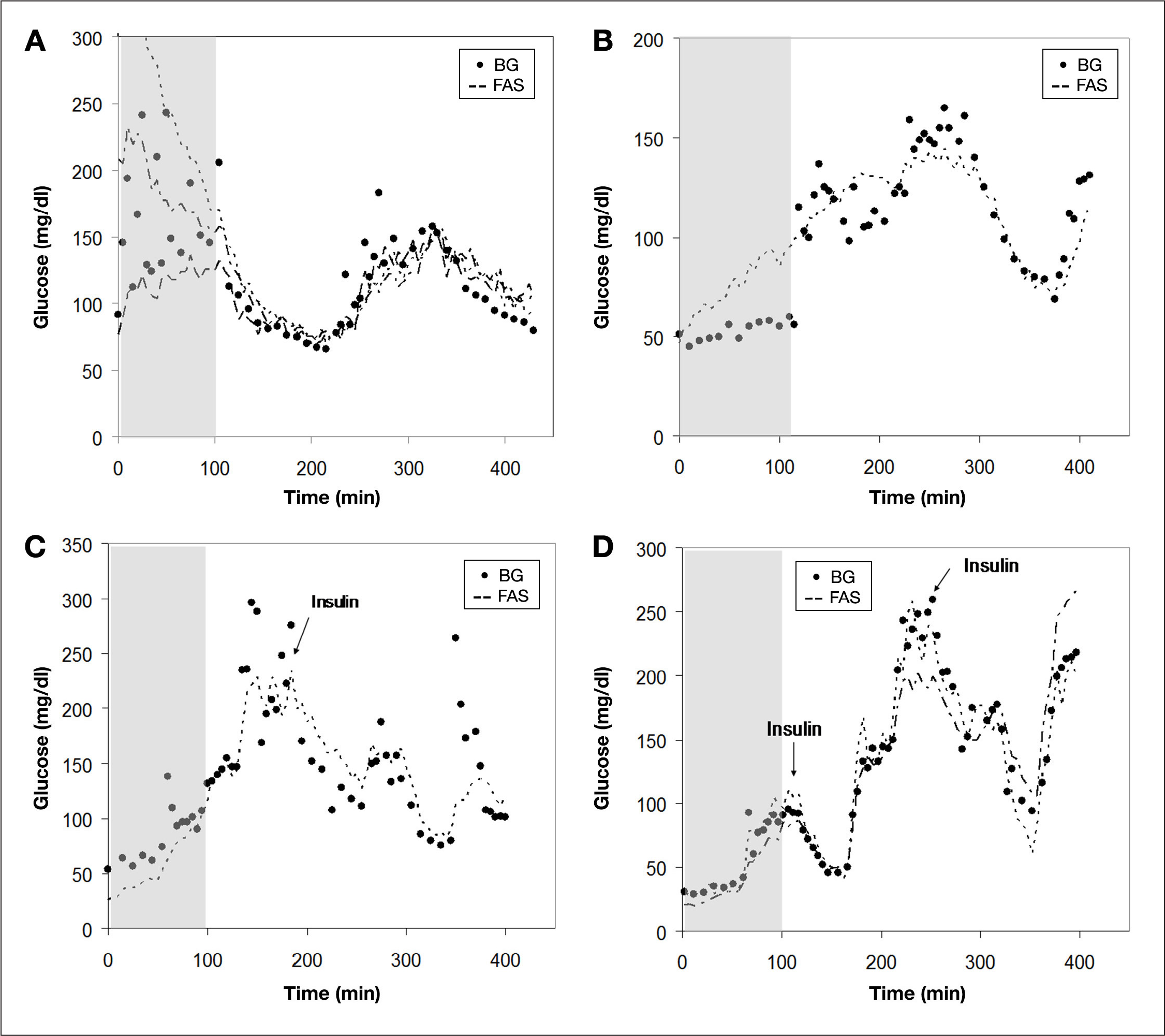
Response of the FAS implanted in femoral artery and vein of anesthetized pigs to infusions of glucose and insulin. Note that no insulin was administrated in
No differences in time lag and accuracy were noticed between sensors residing in the femoral artery or femoral vein, which indicates that the lower flow rate in the vein is not rate limiting for good mass transfer of glucose. Since the animal was continuously infused with heparin, it was not surprising that we did not see any sign of blood clots around the sensor after removal. The percentage of data points falling in the clinically safe zones A and B were 99%, with 94% in A, 5% in B, 0% in zone C, and 1% in zone D (see
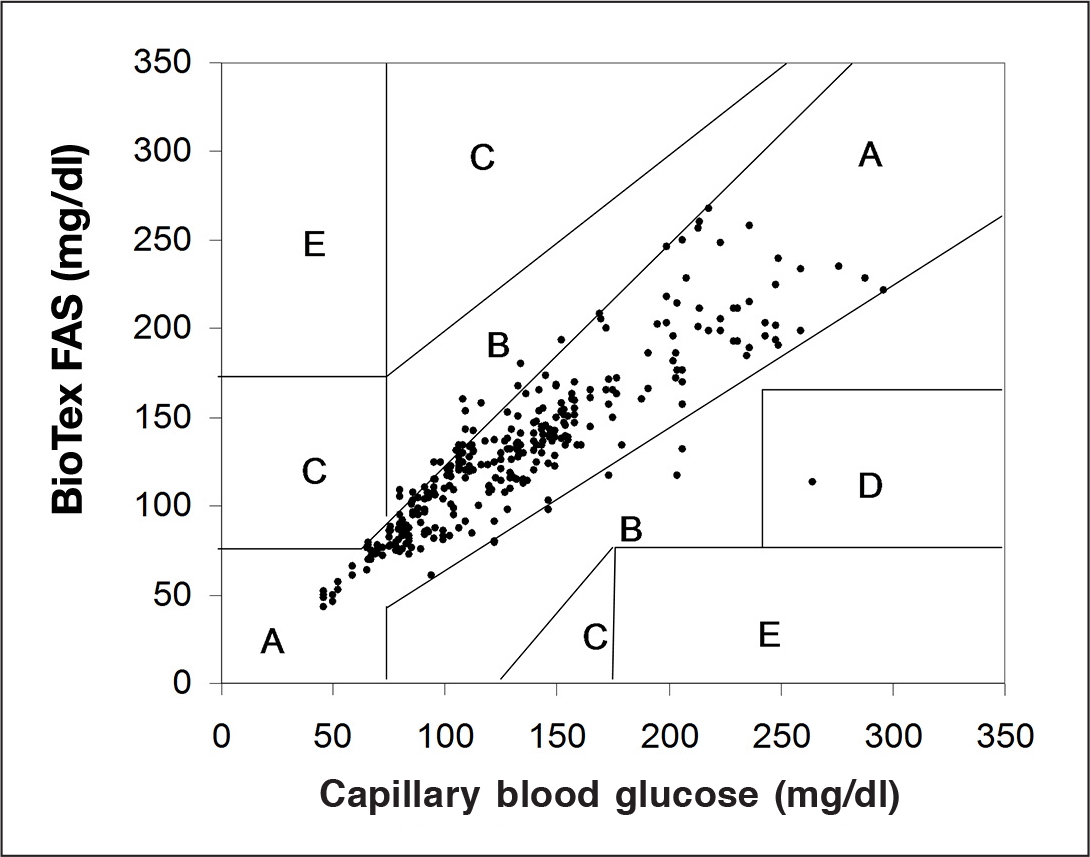
Clarke error grid analysis of FAS data in blood.
Conclusions
In this study, the response performance of FAS was studied and compared in two different body sites—blood and interstitial tissue. We demonstrated that the FAS can perform on a very high accuracy level in the two different environments in the body. However, the effect of exogenous insulin on the physiological relationship between glucose concentration in interstitial fluid and blood significantly compromised the accuracy of the FAS in the animal. If it may be indeed relevant for insulin-treated patients with diabetes, the ramification for correct interpretation of glucose excursions would be significant and must be addressed, probably through an intelligent device control algorithm. In contrast, the intravenous FAS data suggest that the blood vessel is a more suitable site for highly accurate glucose detection because of nonsignificant lag times due to high mass transfer conditions in the intravascular bed. The potential use of the FAS as a glycemic monitor in clinically ill patients looks especially promising. However, further in vivo studies over a longer period of time will be required for additional validation.
Footnotes
Abbreviations:
Funding was provided by the National Institutes of Health Grant #2R44-DK076352.
Acknowledgments:
The authors greatly thank the staff from the Cardiovascular Research Laboratory at the Texas Heart Institute and Stillmeadow Inc. for their support during the animal trials.