
Abstract
Objective
There is a lack of consensus regarding postoperative care for pediatric patients with obstructive sleep apnea (OSA) following adenotonsillectomy. At our institution, all patients with severe OSA are routinely admitted to the pediatric intensive care unit (PICU), raising concerns about the optimal use of health care resources. The objective of this study was to identify the risk factors necessitating PICU admission for pediatric patients who underwent adenotonsillectomy for OSA.
Methods
An 8 year retrospective cohort study was conducted at a tertiary care pediatric hospital among consecutive patients with confirmed OSA undergoing adenotonsillectomy. All patients for whom a preoperative PICU request was made were included. A patient requiring PICU-level care was defined as needing respiratory support, such as intubation, positive pressure ventilation, or high-flow nasal cannula.
Results
A total of 112 medical charts were included in the analysis. Only 13 patients (11.6%) had respiratory complications requiring PICU-level care. No preoperative or intraoperative variables were predictive of need for PICU. Early-postoperative need for supplemental oxygenation (P = .002, OR = 6.7) and respiratory retraction (P < .000, OR = 27.4) were significant predictors of PICU-level airway escalation. Nearly all patients (11/13) requiring escalated airway measures were identified in the first 4 hours postoperatively.
Conclusion
A small subset of subjects with OSA required PICU-level care after adenotonsillectomy. Our data suggest that pediatric patients with OSA undergoing adenotonsillectomy may be safely monitored outside of an ICU setting for an extended period before determining eventual care setting.

Keywords
Introduction
Obstructive sleep apnea (OSA) affects 2 to 6% of children1,2 and represents a significant source of morbidity in the pediatric population. History and physical examination aid in the diagnosis, but confirmation is unequivocally achieved with polysomnography (PSG). 3 In resource-limited settings, nocturnal oximetry is an acceptable alternative to PSG. Untreated OSA can have repercussions on neurocognitive and behavioral development and may lead to cardiovascular dysfunction. Adenotonsillar hypertrophy is the most common cause of OSA in children. In this population, adenotonsillectomy is the preferred treatment. 4
Adenotonsillectomy is one of the most-frequently-performed surgical interventions in children and is considered the most effective treatment for OSA in children. While generally safe, the procedure is not without risks. Hemorrhage and dehydration are the two most frequent complications. In the apneic population, the primary concern is respiratory compromise. Major postoperative respiratory complications include pulmonary edema, laryngospasm, and bronchospasm. Exacerbation of apnea and hypoxia are considered minor complications. Patients with severe preoperative OSA, aged less than 3 years, with craniofacial abnormalities, growth retardation, hypotonia, and obesity are thought to be at increased risk of respiratory compromise. 5
Based on clinical experience and literature, patients with OSA and obesity appear to have heightened sensitivity to narcotics and other anesthetic drugs with central respiratory and sedative effects. 6 These drugs can lead to a reduction in respiratory rate, tidal volume, and even respiratory drive, resulting in hypoventilation, hypoxemia, and hypercapnia.
It is widely accepted that children under 3 years old should be hospitalized for monitoring after adenotonsillectomy, 7 but the duration and setting of monitoring are less clear. Due to the lack of clear guidelines, post-adenotonsillectomy care for children varies significantly from one institution to another. 8 The risk of respiratory compromise in the immediate postoperative period has prompted many centers to adopt protocols for systematic admission to the pediatric intensive care unit (PICU) for respiratory monitoring in high-risk patients. 9 Other centers rely on monitoring adverse events in the post-anesthesia care unit (PACU) to determine whether further PICU admission is necessary. 10
There is, therefore, no consensus on postoperative care for patients with OSA following adenotonsillectomy. Currently, PICU admission is based on institutional policies or surgeon preference, with limited evidence supporting clear guidelines. 8 Hence, our objective was to identify risk factors that necessitate elective admission to the PICU to use resources judiciously in our tertiary pediatric center.
Materials and Methods
Chart Review
This is a retrospective cohort study evaluating patient records from a single tertiary care pediatric hospital in Montreal, Canada, between May 2015 and November 2023. Pediatric patients (<18 years old) with confirmed OSA and for whom a request was made for elective PICU admission after adenotonsillectomy were retrospectively identified for inclusion in the study. Information obtained from patient medical records include demographic data, relevant comorbidities, preoperative overnight pulse oximetry data [McGill score (MOS), SpO2 nadir, 4% oxygen desaturation index (ODI), preoperative continuous positive airway pressure (CPAP)] use, indication for surgery, anesthetic records [American Society of Anesthesiology (ASA) score], surgical records [surgical technique, surgical time, intraoperative complications], PACU and PICU records [postoperative sedation, opioid use, hemorrhage, stridor, retractions, oxygen support]. Overnight oximetry data were scored by trained pulmonologists. Determination of the presence of stridor and retractions was based on nursing, respiratory therapy, and provider notes. Patients with trisomy 21 (T21) were considered separately from those with other genetic syndromes, due to patients with this syndrome having a particular propensity to suffer from OSA. This study received approval from the Institutional Review Board at CHU Sainte-Justine (2024-6326).
Inclusion and Exclusion Criteria
Included patients were those admitted to the PICU electively for adenotonsillectomy. These patients were admitted to the ICU based on having one or more of the following characteristics: less than 3 years of age with severe OSA on overnight pulse oximetry (MOS4, SpO2 nadir <80%), craniofacial anomalies, T21, or severe comorbidities. Patients older than 3 years of age with a combination of comorbidities as described above were also candidates for PICU. Exclusion criteria included patients who underwent adenoidectomy alone and those who were ultimately not transferred to PICU postoperatively as planned, after shared decision between surgeon and anesthesiologist.
Need for PICU-Level Care
A patient requiring PICU-level respiratory support was defined as having escalated airway management [the use of high-flow nasal cannula (HFNC) oxygen supplementation, noninvasive positive pressure ventilation (NIPPV), or endotracheal intubation]. The presence of one or more of the previous criteria justified the need for PICU admission.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics 29.0.1.0. Continuous variables were summarized using mean and standard deviation (SD) for normally-distributed variables and median and interquartile range (IQR) for non-normally-distributed variables. Categorical variables were summarized using counts and proportions. In univariate analysis, statistical significance (P < .05) was determined using the chi-squared test for categorical data and hypothesis testing using independent-samples Mann-Whitney U test for continuous data. Effect sizes with confidence intervals were reported for chi-squared testing using odds ratio [OR] and a confidence interval [CI] of 95%. Missing data after a second chart review were inferred if possible. If data were missing at random, it would be imputed using multiple imputation by chained equations [MICE]. 11
Results
Over an 8.5-year period [May 2015-November 2023], a total of 141 patients met criteria for inclusion. After an initial chart review, 24 patients were excluded for having adenoidectomy alone, and 5 more were excluded for having not been transferred to the PICU postoperatively. No patients underwent other airway procedures at the time of adenotonsillectomy. Their hospital stay was without incident. Of the 112 eligible patients, 13 [11.6%] required PICU-level care, while 99 [88.4%] did not. Of those who required PICU-level care, 7 required HFNC oxygenation, 8 required NIPPV, and 1 required endotracheal intubation.
Demographic Characteristics and PICU Requirement
Demographic data are presented in Table 1. Forty-three percent of patients were under the age of 3 years and were not significantly more likely to require PICU level of care [P = .39]. Median body mass index [BMI] was 16.4 kg/m2 [IQR 5.5 kg/m2] and was not related to increased need for PICU surveillance [P = .51]. According to standards defined by the Centers for Disease Control and Prevention [CDC],12,13 12 patients [10.7%] were underweight, 59 [52.7%] were of healthy weight, 8 [7.1%] were overweight, and 33 [29.5%] were obese. The most common comorbidity was genetic syndromes, being 35 patients [31.2%], followed by 21 [18.8%] with a congenital heart disease, 20 [17.8%] with a neuromuscular syndrome, 19 [17%] with asthma, 13 [11.6%] with dysphagia, 10 [8.9%] with gastroesophageal reflux disease [GERD], 19 [17.0%] with T21, and 2 [1.8%] with sickle-cell anemia. None of the analyzed comorbidities increased the risk of meeting criteria for PICU stay (see Table 1 for p-values). Three patients required CPAP and two required HFNC prior to surgery. These patients all received postoperative oxygenation equal to their preoperative parameters, with no airway management escalation required.
Demographic Characteristics and Comorbidities and Risk for Needing PICU Surveillance.

Abbreviations: IQR, interquartile range. CPAP, continuous positive airway pressure. HFNC, high-flow nasal cannula. NIPPV, noninvasive positive pressure ventilation. CI, confidence interval.
a. According to standards defined by the Centers for Disease Control and Prevention (CDC), underweight children have a BMI <5th percentile for age.
b. According to standards defined by the CDC, healthy weight children have a BMI from the 5th to 84.9th percentile for age.
c. According to standards defined by the CDC, overweight children have a BMI from the 85th to 94.9th percentile for age.
d. According to standards defined by the CDC, obese children have a BMI ≥95th percentile for age.
e. Premature birth is defined as earlier than 37 weeks gestation.
f. Preoperative CPAP or HFNC use was not included in univariate analysis because these patients received preemptive oxygenation equivalent to their preoperative parameters. None of these patients required escalation of airway management.
Nocturnal oximetry results and PICU requirement
Nocturnal oximetry data analysis is presented in Table 2. Seventy-two patients (64.3%) scored MOS4, while 94 (83.9%) had severe OSA based on an ODI ≥ 10. Neither MOS nor ODI significantly predicted the need for PICU stay (p = .125 and p = .403, respectively). Nadir SpO2 did not significantly differ between groups either, with a median of 71.0% (IQR 12.0%) in the group not requiring PICU stay and 72.0% (SD 18.0%) in the group requiring PICU stay (p = .607).
Nocturnal oximetry results and risk for needing PICU surveillance.
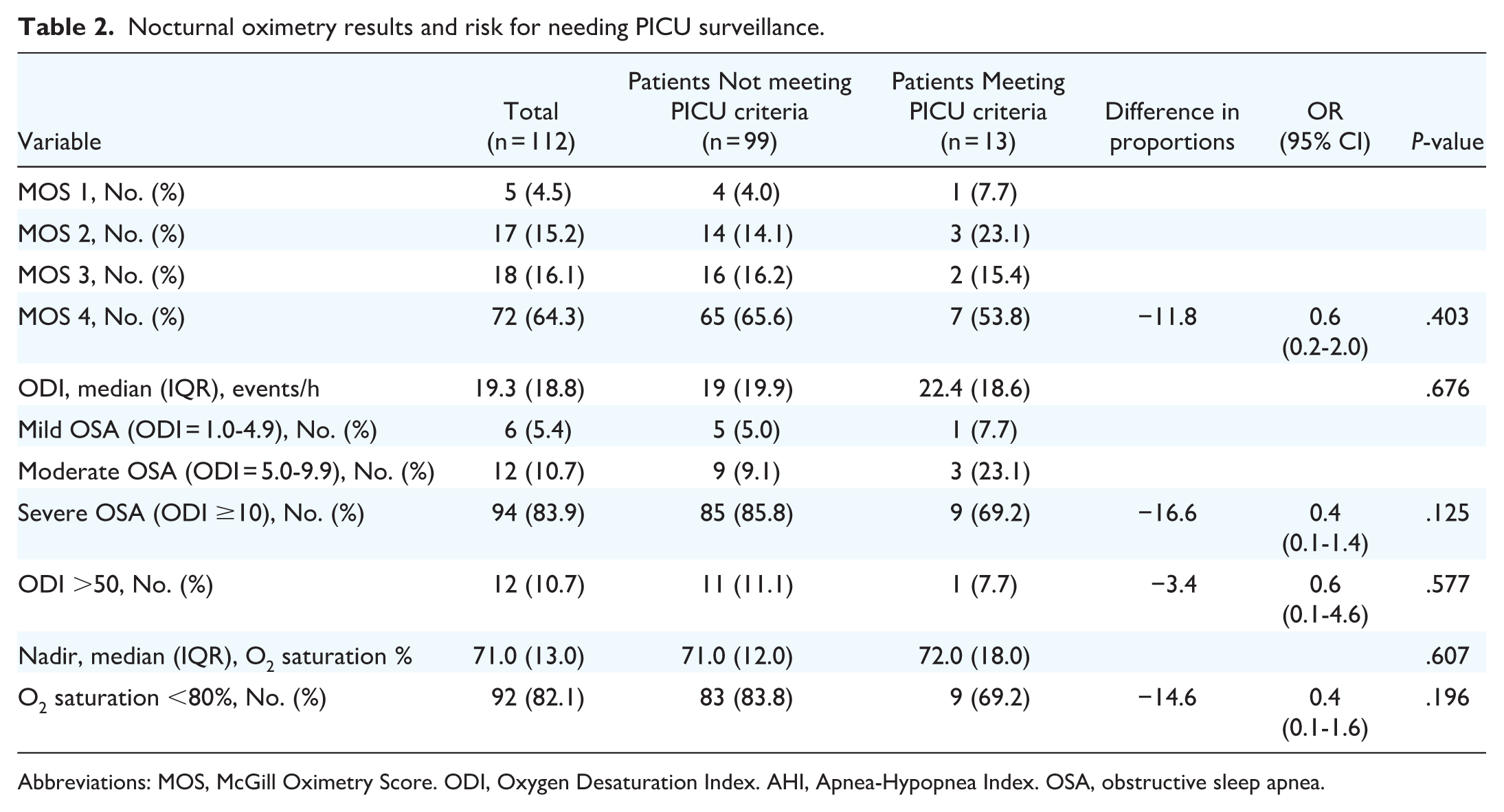
Abbreviations: MOS, McGill Oximetry Score. ODI, Oxygen Desaturation Index. AHI, Apnea-Hypopnea Index. OSA, obstructive sleep apnea.
Intra- and Postoperative Parameters and PICU Requirement
Intra- and postoperative data analyses are presented in Table 3. Patients requiring supplemental oxygen therapy were significantly more likely to require PICU stay with an OR of 10.1 [CI 95% 2.1-48.0]. Eleven of thirteen patients (84.6%) who required the PICU received supplemental oxygen compared with 35 of 99 patients (35.4%) who did not require PICU. Those who demonstrated respiratory retractions in the postoperative period were at significantly-higher risk to require PICU stay with an OR of 9.7 (CI 95% 2.4-38.9). Six of thirteen patients (46.2%) who required the PICU had respiratory retractions, while 6 of 99 patients (6.1%) who did not require PICU had respiratory retractions. Patients with postoperative stridor were significantly more likely to require PICU with an OR of 5.6 (CI 95% 1.5-20.3). At least one episode of postoperative desaturation was also significantly more likely to require PICU services with an OR of 6.3 (CI 95% 1.3-30.1). Only 10/46 (21.7%) patients who desaturated and did not require ICU had desaturation events below 80%, while 7/13 who (53.8%) required ICU had desaturation events below 80%. Duration of surgery and use of opioids did not significantly increase the risk of PICU necessity (P = .778, P = .499, respectively).
Intra- and Postoperative Parameters and Risk for Needing PICU Surveillance.

Desaturation was defined as an oxygen saturation <92%.
Timing of respiratory events and interventions
Table 4 presents data related to timing of respiratory events. Of patients who required supplemental oxygen and PICU stay, 10 of 13 (76.9%) received oxygen in the immediate postoperative period, with an OR of 6.7 (CI 95% 1.7-25.9) when compared to those who did not require PICU stay. Of patients who exhibited postoperative respiratory retractions and required PICU stay, 6 of 6 (100%) first had retractions in the immediate postoperative period, with an OR of 27.4 (CI 95% 5.6-133.7) when compared to those who did not require PICU stay. Of patients with stridor, 3 had stridor immediately postoperatively, while 2 had stridor 4 hours after surgery, 3 had stridor 12 hours after surgery, and none after 24 hours postoperatively.
Timing of postoperative respiratory events.

Abbreviations: HFNC, high-flow nasal cannula. NIPPV, noninvasive positive pressure ventilation.
Sensitivity and specificity
Postoperative events that significantly predicted the need for PICU are reported in terms of sensitivity, specificity and the area under the curve (AUC) in Table 5. Receiver-operator characteristic (ROC) curves are shown in Figure 1. While stridor and respiratory retractions showed high specificity and low sensitivity for PICU necessity, desaturation and O2 supplementation showed opposite trends. O2 supplementation showed the highest level of discrimination with an AUC of 0.746.
Sensitivity and specificity of postoperative respiratory events.
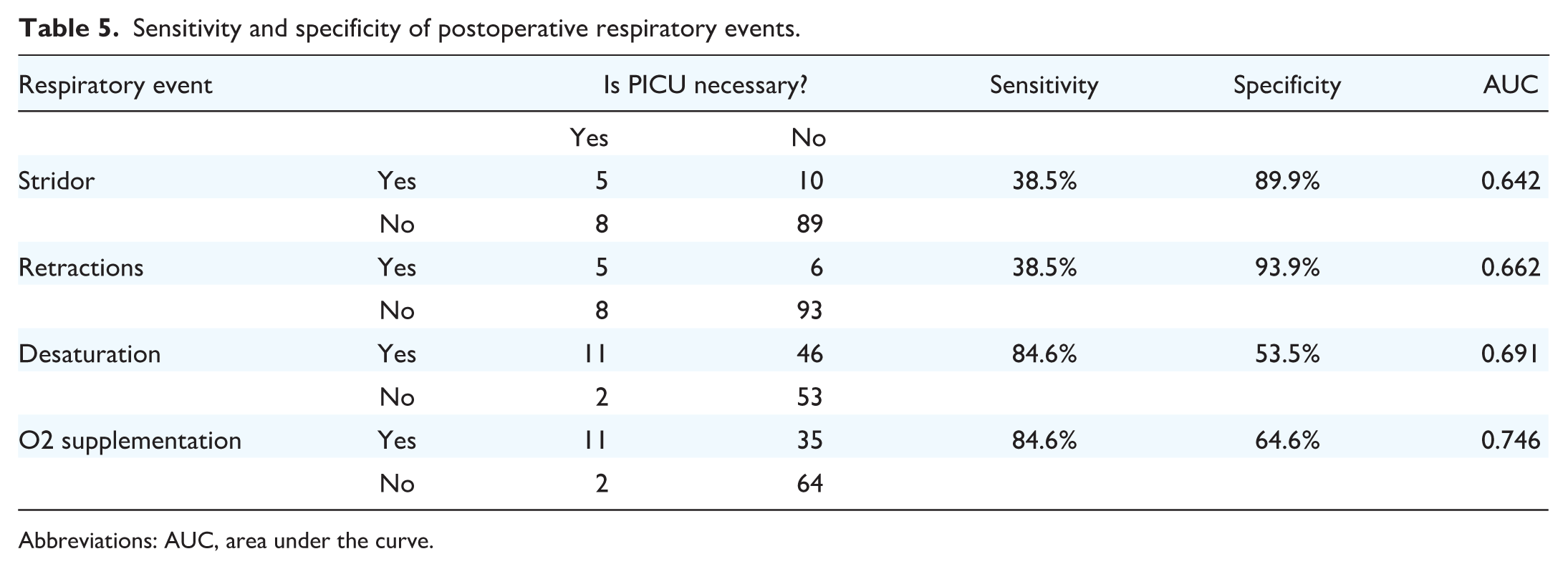
Abbreviations: AUC, area under the curve.

Receiver operating characteristic curve of stridor, respiratory retractions desaturation, and O2 supplementation.
The timing of airway escalation is evidenced from the first use of a higher order airway device (HFNC, NIPPV, or intubation). The number of patients requiring HFNC immediately postoperatively, in the first 4 hours postoperatively, 4 to 12 hours postoperatively, and 12 to 24 hours postoperatively were 6 (46.2%), 6 (46.2%), 4 (30.8%), and 4 (30.8%), respectively. Overall, 7 (53.8%) patients required HFNC in the first 24 hours after surgery. The number of patients requiring NIPPV immediately postoperatively, in the first 4 hours postoperatively, 4 to 12 hours postoperatively, and 12 to 24 hours postoperatively were 2 (15.4%), 6 (46.2%), 6 (46.2%), and 4 (30.8%), respectively. Overall, 8 (76.9%) of patients required NIPPV in the 24 hours postoperative period. No patients required endotracheal intubation in the 24 hours postoperative window. Overall, airway escalation took place immediately after surgery in 8/13 patients (61.5%), while 3 more occurred in the first 4 hours after surgery (23.1%), 1 occurred in the 4 to 12 hours window, and 0 occurred in the 12 to 24 hours window. One patient was intubated 7 days after surgery due to acute chest syndrome.
Discussion
In the current retrospective cohort study, we report on a sample of 112 pediatric patients with OSA who required PICU surveillance after adenotonsillectomy according to institutional guidelines. Our analysis shows that only 13 (11.6%) of these patients were retrospectively found to require PICU stay for airway management purposes. While there were no preoperative patient factors that predicted the need for PICU admission, we found that almost all patients who will go on to require airway escalation were identified within the first 4 hours postoperatively. The presence of stridor, respiratory retractions, desaturation, and need for supplemental oxygen in the early-postoperative period all strongly predicted the need for PICU transfer, reinforcing the importance of these early signs of respiratory compromise. Furthermore, stridor and respiratory retractions were highly specific, while desaturation and O2 supplementation were highly-sensitive predictors. Overall, O2 supplementation was the best discriminator of the need for PICU transfer.
As noted above, obstructive sleep apnea is highly prevalent in the pediatric population internationally. Adenotonsillar hypertrophy is the most common etiology and adenotonsillectomy is the accepted first-line treatment for this indication. While rates of morbidity and mortality are low, these patients carry an increased risk of perioperative respiratory complications. 14 Recent studies15 -17 report that between 18% and 26% of patients with OSA undergoing adenotonsillectomy require ICU for the escalation of respiratory support, such as high oxygen, NIPPV, or intubation. Unfortunately, there is no consensus nor guideline, on the level of postoperative care required.
With so much heterogeneity in the literature on risk factors for respiratory complications in patients with OSA following adenotonsillectomy17,18, it begs the question of whether valuable resources, such as PICU beds, are being properly utilized. A study by Lavin et al 16 defined ICU need as supplemental oxygen requirements greater than 2 L between 2 and 24 hours postoperatively, more than two desaturation events in a 2 hour period, or more than hourly nursing intervention. Like the current study, only 18.2% of patients admitted to ICU utilized the resources necessary by the criteria defined. The authors concluded that most high-risk adenotonsillectomy patients do not utilize critical care resources. This supports the idea that PICU resources may not be used in an efficient manner in the setting of high-risk patients undergoing adenotonsillectomy. An additional finding was that young age, gastrostomy tube status, and neuromuscular disorders significantly predicted critical care resource utilization, which was not supported in our study.
The American Academy of Pediatrics (AAP) recommends that patients at high risk of postoperative respiratory complications should be monitored as inpatients. 14 Guidelines for the setting of postoperative monitoring have yet to be established, however. Similarly, the American Academy of Otolaryngology (AAO) 19 recommends for patients <3 years of age or presenting with severe OSA (AHI ≥10 obstructive events/hour, oxygen saturation nadir <80%, or both) to be monitored in hospital, and patients with preoperative AHI >30 can be admitted to the ICU. One particular study by Rhodes et al 20 found that patients with an AHI >50, an oxygen nadir <80%, or less than 2 years of age were significantly more likely to be admitted to the PICU. There has been no consensus, however, on the use of overnight pulse oximetry as a tool to predict the need for PICU postoperatively. To our knowledge, our study is the first to investigate associations between overnight pulse oximetry parameters and the need for PICU postoperatively, and none of these parameters significantly predicted a significantly-higher likelihood of requiring PICU resource utilization. The findings of this study are important in that it provides evidence that this more available and cost-effective method of investigating pediatric OSA should not be used to stratify patients risk of requiring postoperative ICU management.
According to the American Society of Anesthesiologists (ASA), 7 patients at increased perioperative risk of respiratory depression have more severe sleep apnea, systemic administration of opioids, use of sedatives, site and invasiveness of surgical procedure, and the potential for apnea during rapid eye movement (REM) sleep on the third or fourth postoperative day (ie, “REM rebound”). In the current study, degree of sleep apnea, administration of opioids, and use of sedatives were not risk factors for respiratory depression requiring PICU-level escalation. REM rebound was not analyzed, and surgical invasiveness was constant.
At our institution, all patients less than 3 years of age with severe OSA on overnight pulse oximetry (MOS4, SpO2 nadir <80%), craniofacial anomalies, T21, or severe comorbidities are systematically requested beds at the PICU after adenotonsillectomy. However, in the current study, neither age, preoperative oximetry parameters, nor serious comorbidities incurred a higher risk of need for PICU.
As recommended by the ASA, 7 all patients with OSA undergoing adenotonsillectomy are monitored in the PACU with continuous pulse oximetry. While the literature is insufficient to establish recommendations for the postoperative setting to monitor these patients, nor the duration of monitoring in the PACU, the ASA recommends monitoring in the PACU until patients are no longer at risk of respiratory depression. Unfortunately, the definition of no longer being at risk of respiratory depression is unclear. Previous studies21,22 have reported predictors of PICU transfer from data in the recovery room, such as oxygen desaturation <90%, PACU stay >100 minutes, oxygen requirement >40% FiO2, and the occurrence of a severe respiratory event. In the present study, those who required supplemental oxygen or exhibited respiratory retractions immediately postoperatively at greater risk of airway escalation requiring PICU (OR = 6.7, OR = 27.4, respectively). Moreover, the need for PICU as defined in this study was able to be accurately predicted in the first 4 hours after surgery in nearly all patients. Similar results have been found for other types of surgery such as supraglottoplasty. 23
At our tertiary care institution, it is determined preoperatively whether patients will require elective admission to the PICU. A more efficient use of resources may be to observe patients for 4 hours in the PACU to determine the definitive level of care necessary. The results from this study may provide the necessary evidence to implement such practices and lead to substantial cost-savings. It is important to be aware this may cause stress on PICU bed management since some of these beds may need to be reserved on a “ready in case” basis. Our hope is, however, that with the overall reduced number of PICU beds needed by our patients overall, it would still be a net-positive result for cost-saving and resource management. An excellent potential solution to the issues discussed in our study would be to have a stepdown unit, which provides a lower level of care with less resources than the PICU for patients who cannot be safely monitored on a regular ward. In these stepdown units, patients will have access to HFNC, NIPPV, but without the resources of a full intensive care unit. We believe that, based on our findings, such a unit would be more than sufficient for our postoperative adenotonsillectomy patients.
Our study has several limitations. First, the small sample size in the group requiring PICU is both an important result and a limitation of this study. While it is significant that so little patients who were electively admitted to the PICU required these services, the small sample size may lead to type II error and thus low power. In addition, because there were so few patients in this group, multiple logistic regression analysis would not yield statistical relevant results. Another limitation to this study is that due to feasibility issues, only elective PICU admissions were included, and not those with unplanned PICU admissions as well. Lastly, although the rates of desaturation and O2 supplementation were significantly higher in patients requiring ICU, there was still a high proportion of those who did not require ICU who had these events. In future studies, to improve recovery room decision-making, we encourage studies that will characterize the desaturation events in the postoperative period to investigate whether we can better stratify these patients who would not need ICU.
Conclusion
The current literature lacks consensus and clinical guidelines to guide postoperative care of pediatric patients with OSA following adenotonsillectomy. This has led to potential poor utilization of resources for postoperative care of these patients. In the current retrospective cohort study, only a small proportion of patients who were electively admitted to the PICU required the advanced respiratory care of this clinical setting. Patients who do go on to require escalated airway therapy may be readily identified early in the postoperative period, suggesting the potential need for extended PACU surveillance to determine definitive care.
Footnotes
Acknowledgements
We would like to thank all pediatric otolaryngologists in our center who have performed the surgeries over the years, as well as the intensivists who cared for our patients.
Author’s Note
This research was presented as a podium presentation for the Poliquin prize competition during the 78th Canadian Society of Otolaryngology-Head & Neck Surgery in Montreal on June 2, 2024.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors have no funding, financial relationships, or conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.