
Abstract
A 70-year-old obese male with moderate obstructive sleep apnea (OSA) sought alternative treatment after failing to tolerate positive airway pressure (PAP) therapy. He underwent drug-induced sleep endoscopy (DISE) with a nasal cannula and oral thermistor to differentiate nasal from oral breathing and a thoracoabdominal belt to track respiratory effort. DISE revealed a complete velum collapse in the anterior-posterior direction, consistent with his awake, supine computed tomography scan, yet the oral thermistor confirmed stable mouth breathing without respiratory distress. A mouth closure maneuver partially reopened the velum and appeared to enlarge the retroglossal airway. This case underscores the importance of evaluating a patient’s primary breathing route during DISE, as standard interpretations of airway collapse may be misleading without this information. Mouth breathing may bypass obstructions at the velum, affecting PAP efficacy and influencing treatment decisions. To address this gap in the VOTE (velum, oropharyngeal lateral walls, tongue base, and epiglottis) classification system, we propose “VM” to denote velum collapse in the context of mouth breathing. This addition could aid in tailoring OSA treatments, particularly for patients who predominantly breathe orally. Our findings advocate for a more patient-specific approach to DISE interpretations, emphasizing the physiological and anatomical aspects of airway collapse.
Keywords
Introduction
Drug-induced sleep endoscopy (DISE) is used in the evaluation of obstructive sleep apnea (OSA) to characterize the anatomic site(s) and severity of upper airway collapse. Results of a DISE examination are utilized to guide patient selection for positive airway pressure (PAP) alternative treatment. In a standard DISE procedure, the surgeon utilizes videoendoscopy alone. More recently, our group has integrated PAP titration with simultaneous measurements of airflow and respiratory effort. 1 These physiologic measures obtained during DISE have been shown to identify central apnea and predict response to hypoglossal nerve stimulation.2,3 Herein, we present a common DISE finding of complete palatal collapse. However, monitoring nasal and oral airflow provided an alternative interpretation of palatal collapse. While sleep surgeons are trained to assess the location, severity, and direction of airway collapse, the patient’s route of breathing is not systematically evaluated. As our case illustrates, this omission can significantly influence how collapse is interpreted, particularly at the velum, and impacts selection of effective OSA treatment options.
Case Report
A 70-year-old male with obesity (body mass index 30 kg/m2) and essential hypertension was referred by his sleep medicine physician for evaluation and possible surgical treatment of OSA. The patient was initially diagnosed with OSA due to daytime fatigue, difficulty concentrating, and snoring. Subsequently, he tried continuous positive airway pressure (CPAP) with both nasal and full-face masks but was unable to consistently tolerate therapy. He denied any nasal congestion or obstructive symptoms at his initial visit. An updated in-lab polysomnography sleep test was performed, which showed an apnea–hypopnea index (AHI) of 17 events/h with clustering of events during rapid eye movement (REM) sleep. Since the patient’s OSA was inadequately managed with all nonsurgical options, he elected to undergo a complete evaluation for surgical treatment.
DISE was performed according to a protocol published previously (University of Pennsylvania IRB: 853096). 1 Once an appropriate depth of sedation was achieved, the patient was fitted with a nasal CPAP mask (Respironics, Murrysville, PA, USA) custom-made to allow for the passage of a flexible pediatric bronchoscope. No topical nasal decongestants nor anesthesia was given prior to the procedure. A pressure-transducing nasal cannula was placed along with an oral thermistor to provide measures of nasal and oral breathing respectively. A thoracoabdominal belt (Nox Medical, Alpharetta, GA) continually monitored the patient’s respiratory effort. Additionally, this patient underwent a standardized computed tomography (CT) scan of the head and neck according to an established protocol to assess for anatomic contributors to OSA. 1 During CT image acquisition, the patient was placed supine and asked to breathe through their nose if possible.
Results of the patient’s DISE examination showed a complete collapse of the velum in the anterior-posterior direction. Partial oropharyngeal wall and tongue base collapse were also noted. Despite the complete collapse of the velum, the patient’s arterial oxygen saturation remained stable with no increase in respiratory effort. An oral thermistor confirmed that the patient was breathing through his mouth (Figure 1A). This phenomenon continued for an additional 10 minute until mouth closure maneuver was performed, at which time the velum was no longer completely collapsed and the lumen of the retroglossal airway was increased (Figure 1B). His coronal CT scan was notable for a narrow, high-arched palate (Figure 1C, intermolar distance = 23 mm). Despite being instructed to breathe nasally, the sagittal view demonstrated a complete collapse of the velum, parted lips, and patent oropharyngeal airway, which all suggest that this patient may be a habitual mouth breather (Figure 1D).
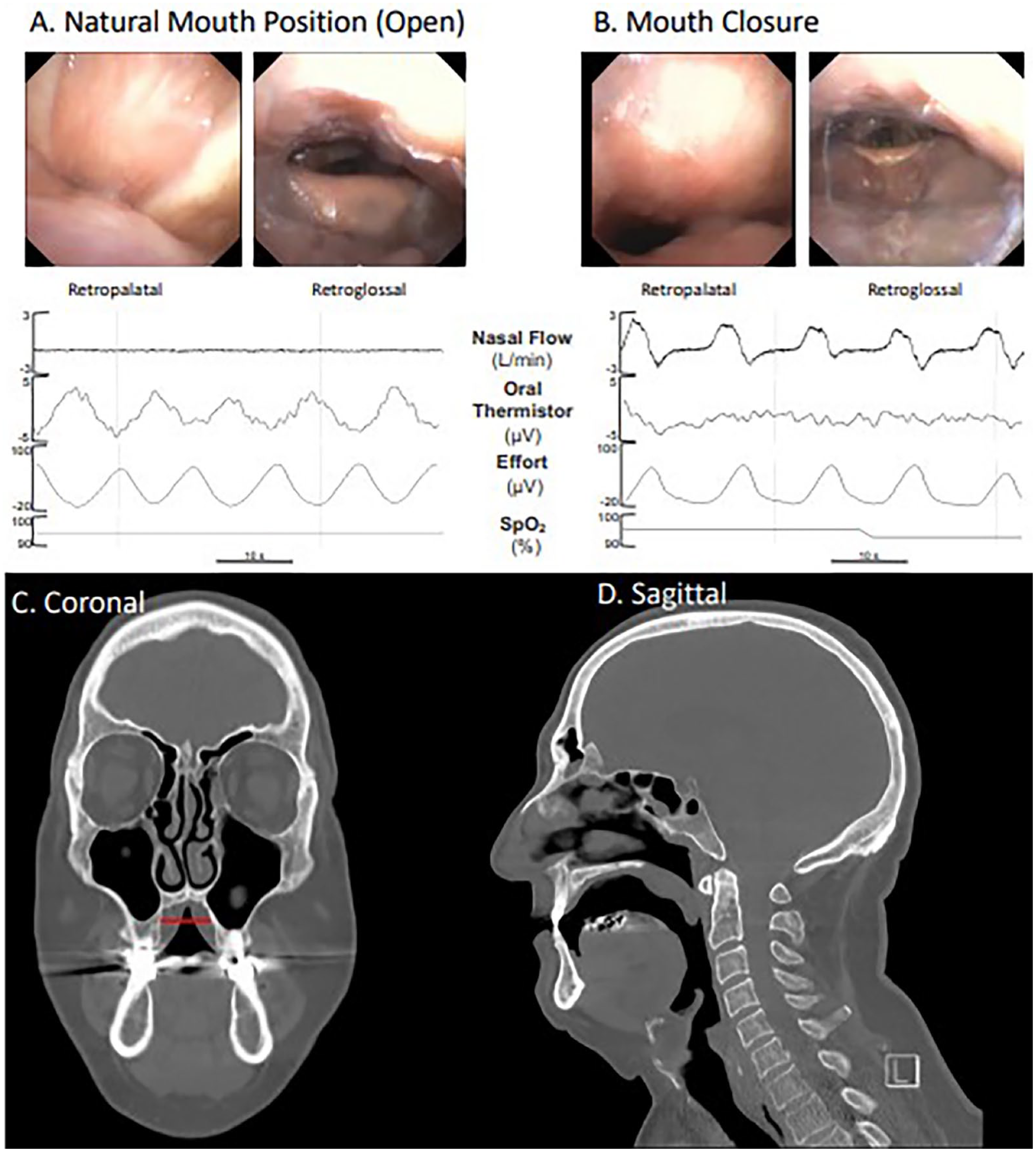
DISE and physiologic data. (A) Nasoendoscopy shows a complete collapse of the velum; however, an oral thermistor confirms the presence of mouth breathing. (B) Mouth closure opens the retropalatal and retroglossal airways increasing nasal airflow. (C) The patient’s coronal CT image shows a narrow, high-arched palate with an intermolar distance of 23 mm (red bar) consistent with transverse maxillary deficiency. (D) The sagittal CT image displays a complete collapse of the velum, and a patent oropharyngeal airway.
Discussion
This illustrative case report underscores the importance of monitoring the route of breathing during DISE. Nasoendoscopy and CT scans both showed a complete collapse of the velum in the anterior-posterior direction, possibly implicating it as a surgical target. However, physiologic data obtained from a nasal canula, oral thermistor, respiratory effort belt, and pulse oximetry demonstrated that the patient was breathing orally, and the complete collapse of the velum did not abolish inspiratory airflow. Furthermore, when a mouth closure maneuver was performed, the collapse of the velum was mitigated (Figure 1B).
Prior studies have demonstrated that monitoring the preferred breathing route is crucial in selecting the appropriate CPAP interface. Nasal CPAP is generally more effective than oronasal CPAP due to its focused pressure application, which projects the tongue and velum anteriorly, thereby maintaining airway patency. 4 Oronasal masks, however, allow pressure dissipation through the mouth, often necessitating higher CPAP levels to achieve the same therapeutic effect.5,6 Furthermore, patients who predominantly breathe through their mouths during sleep require even higher CPAP levels with oronasal masks, leading to issues with treatment efficacy and adherence. 7 Integrating assessments of breathing patterns with mask interface choice could significantly improve CPAP efficacy.
The velum functions as a physiologic gatekeeper, directing airflow based on the patient’s primary route of breathing. 8 During nasal breathing, the velum is pulled toward the tongue, allowing airflow through the nasal passage. 9 When breathing orally, the soft palate elevates and moves posteriorly against the posterior pharyngeal wall, thereby closing the nasopharyngeal airway. 8 Therefore, isolated collapse of the velum in a primary nasal breather is pathologic and could prompt a sleep surgeon to consider anatomic modification of this structure. 10 However, in patients who predominantly breathe through their mouth, such as the patient in this case report, the collapse of the velum does not impede inspiratory airflow (Figure 2). In some patients, mouth breathing may be a protective adaptation to maintain adequate ventilation in the setting of high nasal airway resistance. 11 Nonetheless, mouth breathing has been shown to associate with worse oxygen desaturation and increased degree of upper airway collapse during sleep.12,13 In short, surgical consideration of the soft palate requires an understanding of the patient’s predominate route of breathing for successful outcomes.
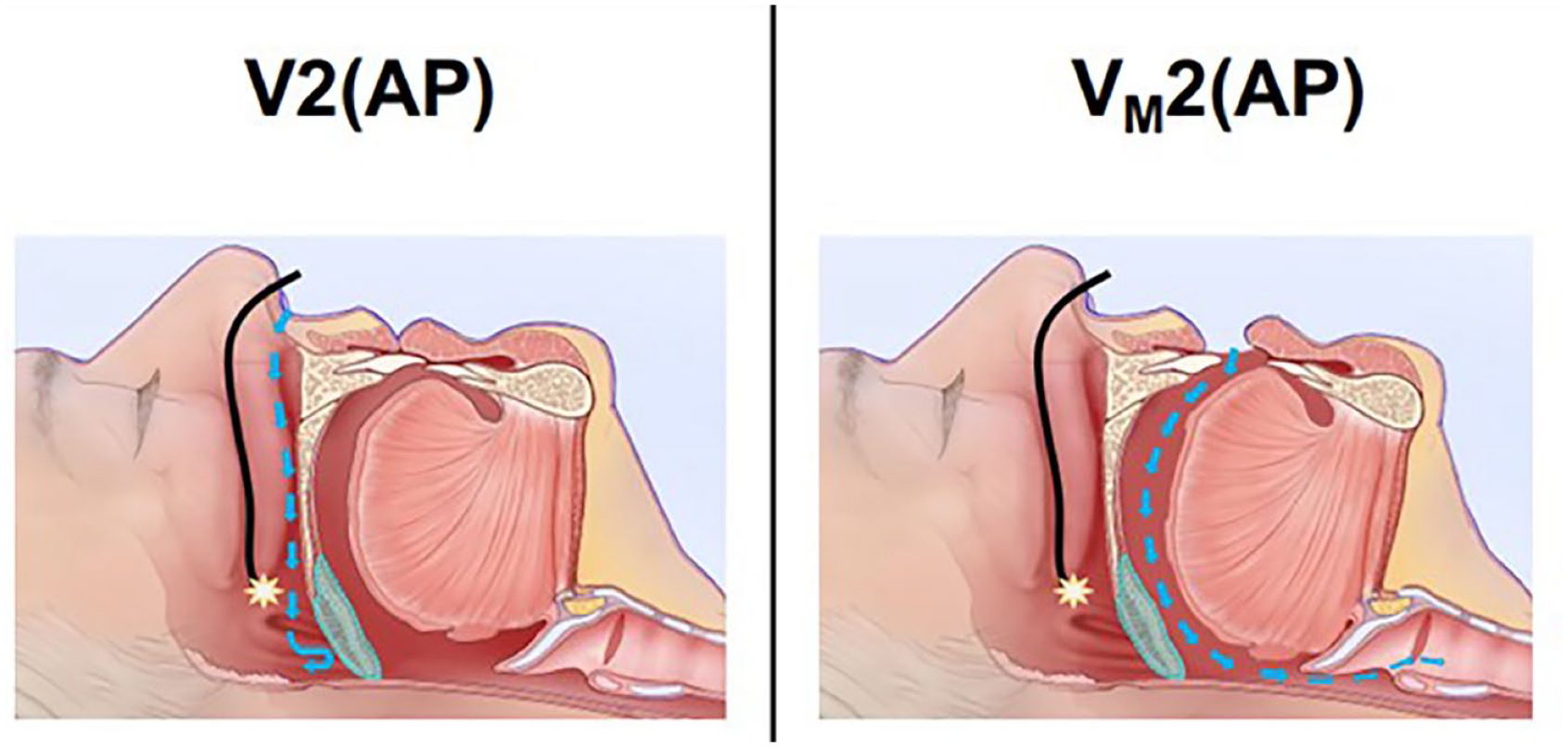
When breathing nasally (left panel), a collapsed velum is pathologic and leads to arterial oxygen desaturation. Oral breathing (right panel) bypasses the collapsed velum and maintains adequate ventilation.
Of note, in our patient's case, no obstructive events were observed during a 10 minute DISE examination. His stable breathing during DISE was consistent with the respiratory findings of his polysomnogram during non-rapid eye movement (NREM) sleep. This is not surprising considering that the electroencephalogram patterns observed during propofol anesthesia (eg, DISE) has previously been shown to resemble that of NREM sleep. 14 However, DISE does not replicate the characteristics of REM sleep, where loss of neuromuscular tone can cause obstructive events in some patients with OSA. 15 In this patient, several factors may synergistically contribute to the worsening of OSA during REM sleep. First, transverse maxillary deficiency could predispose the patient to posterior displacement of the genioglossus muscle. 16 Second, it is well-established that genioglossal muscle tone decreases significantly during REM sleep, further compromising the stability of the airway and increasing the risk of obstruction. 17 Third, the act of mouth opening has been shown to displace the mandible in a posterior and inferior direction, exacerbating tongue base collapse and narrowing the airway. 18 The combination of these anatomical and physiological factors may thus create an environment conducive to more pronounced obstructive events during REM sleep.
Mouth breathing has been shown to have increased prevalence among patients with OSA compared with primary snorers and is perhaps even more common in those who seek PAP alternative treatments. 7 In our DISE examination, we do not apply medications in the nose such as topical decongestants nor anesthesia to preserve the patient’s natural route of breathing. Additionally, before DISE we ask each patient to fill out a questionnaire regarding signs of nocturnal mouth breathing including morning dry mouth, nighttime nasal congestion, or bedpartner-noticing open mouth. In the senior author’s experience, results of the clinical questionnaire often correlate with the route of breathing observed during DISE.
This case provides new evidence, indicating that the route of breathing should be a consideration in the overall management strategy for OSA. Mouth breathing can increase airway collapsibility leading to higher AHIs, which can affect patient outcomes of surgical therapy. 19 Personalized approaches that consider whether the patient primarily breathes nasally or orally during sleep could significantly improve treatment adherence and success rates. As the route of breathing can dynamically change due to various factors, including positional changes and environmental influences, it is critical for clinicians to consider these variations when designing a treatment plan.
Conclusion
Noting the route of breathing is critical to correctly interpret DISE, particularly at the level of the velum. If an oral thermistor is not available to confirm route of breathing, arterial oxygen saturation, and visual approximation of respiratory effort can be used to differentiate obstructive apneas from stable mouth breathing. The VOTE classification provides measures of collapse severity (0/1/2) and pattern (AP, lateral, concentric) but fails to classify route of breathing. We propose “VM” to denote the collapse of the velum in the context of mouth breathing to characterize this common phenotype seen in a sleep otolaryngology practice (Figure 2).
Footnotes
Acknowledgements
Kendra Troske, BA, and Erica Kent, BS, assisted with data organization.
Authors’ Note
This case was presented at the International Surgical Sleep Society 2023 Educational Update in Nashville, TN, September 29, 2023.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.C.D.: Grant research funding by NIH, Inspire, Nyxoah Medical. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institutes of Health (1R01HL144859-05)