
Abstract
Background:
Lingual thyroglossal duct cysts (LTGDCs) are rare, and there is no clinical consensus on the use of transoral endoscopic resection assisted by radiofrequency plasma ablation for their treatment.
Objective:
To evaluate the feasibility, safety, and perioperative outcomes of transoral endoscopic assisted by radiofrequency plasma ablation resection for LTGDCs.
Materials and Methods:
We reviewed 17 patients aged 34 ± 12 years (range 12-61) who underwent transoral endoscopic resection assisted by radiofrequency plasma ablation for LTGDCs over 5 years. The procedure involved endoscopic exposure, circumferential dissection, cyst dome resection, fluid evacuation, multi-angle ablation, and cervical compression-aided ablation. Operative time, blood loss, complications, feeding recovery, and recurrence rates were analyzed.
Results:
All procedures were completed endoscopically, without conversions to open surgery or tracheostomy. The mean operative time was 75.0 ± 31.2 minutes, and the average intraoperative blood loss was 28.0 ± 9.2 mL. All patients resumed liquid diets on postoperative day 3 and semiliquid diets by day 5. No severe complications occurred. Over a 2 to 40 months follow-up, the recurrence rate was 29.4% (5/17).
Conclusions and Significance:
Transoral endoscopic resection assisted by radiofrequency plasma ablation is a feasible and safe option for LTGDCs, with favorable cosmetic outcomes. However, the higher recurrence rate may limit its broader clinical applicability.
Keywords
Introduction
Thyroglossal duct cyst (TGDC) is a common congenital disorder of the midline cervical region. Lingual thyroglossal duct cyst (LTGDC) is a rare subtype, accounting for approximately 0.5% to 2.0% of all cases.1,2 Due to its location at the base of the tongue, the lesion is typically asymptomatic in the early stages. However, as it enlarges, it may obstruct the airway.
The classic surgical approach to TGDC is the traditional external cervical route, exemplified by the Sistrunk procedure. 3 This involves resection of the cyst, the residual thyroglossal duct, and a portion of the hyoid bone, along with adjacent tissues, to achieve maximal completeness of excision. However, this approach involves a long surgical path, and rare airway injuries or severe airway compromise have been reported and may require temporary airway protection in exceptional cases. 4 Therefore, it is not well-suited for LTGDC—particularly in those with aesthetic concerns. Consequently, identifying minimally invasive methods for resecting LTGDC has become a key focus of both domestic and international research.
Previous studies have demonstrated that transoral endoscopic resection for LTGDC is safe and effective. 5 However, a high recurrence rate of LTGDC has been reported in the literature. 6 Due to the low incidence of LTGDC and the absence of large-sample studies, there is currently no clinical consensus regarding the optimal surgical approach, specifically whether to adopt a transoral endoscopic technique or the traditional open Sistrunk procedure. In this study, we retrospectively analyzed the clinical data of 17 patients who underwent transoral endoscopic low-temperature plasma resection of LTGDC at our institution. This investigation represents an initial exploration of the safety of the technique and aims to provide practical experience and a reference for selecting surgical approaches to manage LTGDC.
Materials and Methods
General Information
Patients diagnosed with LTGDC between 2019 and 2023 were enrolled. The inclusion criteria were as follows: a cyst at the tongue base confirmed by laryngoscopy, with computed tomography (CT) demonstrating close anatomical proximity to the hyoid bone; voluntary selection of transoral endoscopic surgery after provision of fully informed consent; adequate preoperative assessment indicating satisfactory transoral exposure, defined as an interincisal distance ≥30 mm; and sufficient baseline physical status to tolerate general anesthesia. Patients with spinal disorders resulting in restricted neck extension were excluded. All patients were fully informed of the potential risks associated with the surgical procedure and voluntarily chose to undergo endoscopic-assisted low-temperature plasma excision of the lingual lesions, performed under supportive laryngoscopic guidance. This study was conducted in accordance with the Declaration of Helsinki and approved by the local Institutional Review Board (Number 2025-1162-15).
Surgical Methods
All patients underwent tracheal intubation under general anesthesia. A high-definition rigid endoscopy platform (XION MATRIX HD; XION GmbH, Berlin, Germany) with a 0° laryngoscope (XION; XION GmbH, Berlin, Germany) was used together with a standard cotter device (Karl Storz SE & Co. KG, Tuttlingen, Germany). The laryngeal plasma device employed was the model 8872 (PROcise XP Plasma Wand; Smith & Nephew, Watford, UK). Following full exposure of the lesion via laryngoscopy, surrounding secretions were meticulously cleared. The plasma device was then used to dissect and excise the cyst, starting from the cyst dome and progressing to the lingual muscle layer. This step involved actively resecting the cyst dome to facilitate the evacuation of cystic fluid. The cyst wall and its peripheral boundaries were exposed in a bowl-shaped configuration.
Subsequently, the cyst was retracted and dissected from multiple angles and positions. This process was repeated until the lesion was entirely excised. Additionally, plasma ablation was applied to the tissue on the inner surface of the hyoid bone at its midpoint (the cyst root), extending to the hyoid bone periosteum. This was achieved by applying external cervical compression to the hyoid bone, thereby enhancing access and ensuring thorough ablation.
Before each procedure, a new suction canister was used, and the volume of intraoperative plasma irrigation fluid was recorded. At the end of the surgery, intraoperative blood loss was estimated by subtracting the volume of irrigation fluid from the total volume collected in the suction canister.
Perioperative Treatment
Following surgical intervention, patients were closely monitored for respiratory status, bleeding, and other potential complications. Antibiotics and glucocorticosteroids were administered in calculated doses via nebulization or intravenous infusion. Postoperative fasting and intravenous nutritional support were initiated. To minimize the risk of postoperative bleeding, infection, and other wound-related complications, oral intake of cold fluids commenced on postoperative day 3, followed by semiliquid foods on day 5, with transition to a regular diet within 2 to 3 weeks.
Follow-up evaluations included endoscopic laryngoscopy at 1 week, 1 month, and 3 to 6 months postoperatively. In addition, a CT re-examination was conducted between 1 and 2 years after surgery.
Outcomes and Assessment
The primary outcome was disease recurrence, defined as the reappearance of a TGDC during postoperative follow-up, confirmed by clinical examination and imaging when indicated. Secondary outcomes included surgical feasibility and safety, perioperative parameters, and postoperative complications. Surgical feasibility was assessed by successful completion of the endoscopic procedure without conversion to open surgery or the need for tracheotomy. Safety outcomes included the occurrence of major perioperative complications, such as operative-site hemorrhage, dyspnea, or secondary infection. Additional secondary outcomes comprised operative time, intraoperative blood loss, and postoperative symptoms, including throat pain and swallowing discomfort. Operative time and blood loss were recorded intraoperatively as continuous variables. Postoperative follow-up duration was recorded for all patients, and management strategies for recurrent cases were documented.
Results
Seventeen patients with LTGDC were included. Of these, 11 were male, and 6 were female, with ages ranging from 12 to 61 years and a mean age of 34.0 ± 12.0 years. In the cohort, 12 of 17 patients presented with symptoms of pharyngeal foreign body sensation; 2 reported intermittent pharyngeal pain, while one 12-year-old female presented with increased pharyngeal secretions as the primary symptom. Notably, 2 cases were asymptomatic and identified incidentally during routine physical examinations.
Postoperative pathological examination confirmed the diagnosis of TGDCs. All 17 patients successfully underwent the surgical procedure without intraoperative conversion to open surgery or tracheotomy. No major complications, such as operative-site hemorrhage or dyspnea, were observed. Additionally, no cases of secondary infection occurred. Postoperative symptoms included mild throat pain and some degree of swallowing discomfort.
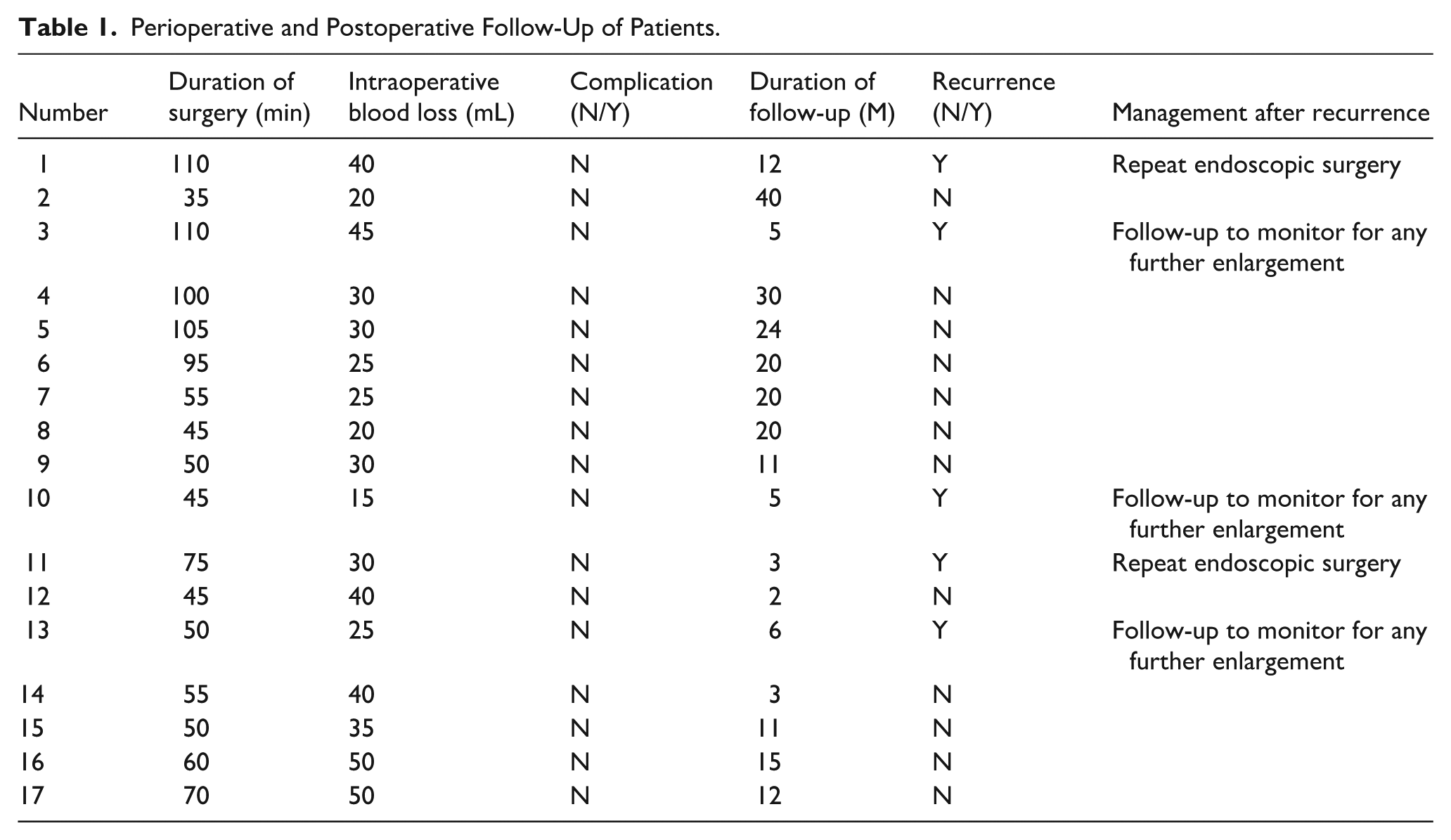
The mean operative time was (75.0 ± 31.2) minutes, and the average intraoperative blood loss was (28.0 ± 9.2) mL (Table 1). Postoperative follow-up was conducted over a period ranging from 2 to 40 months. Recurrence occurred in 5 of the 17 cases, all at the original tongue-base site, resulting in a recurrence rate of 29.4%. Two cases underwent repeat endoscopic surgery, and 3 cases were followed up to monitor for any further enlargement (Table 1).
Perioperative and Postoperative Follow-Up of Patients.
The following 2 cases highlight variable clinical presentations and postoperative outcomes.
A 19-year-old female patient was admitted with a newly identified mass at the base of the tongue, which had been present for over 1 month. Endoscopic laryngoscopy revealed a sizable cyst located in the midline at the root of the tongue, exerting pressure on the epiglottis (Figure 1A). A cervical CT scan demonstrated a round, low-density lesion at the base of the tongue, with a longitudinal diameter of approximately 1.8 cm. No significant enhancement was observed in contrast-enhanced imaging (Figure 1B-C). Endoscopic plasma excision of the tongue root lesion was subsequently performed (Figure 2). Postoperative pathological examination demonstrated fibrous cyst wall tissue without an identifiable epithelial lining. The cyst wall contained dilated and congested blood vessels, stromal edema, and hemorrhage, accompanied by a dense infiltrate of lymphocytes and plasma cells. Focal salivary gland tissue was also identified (Figure 1D-E). Postoperative pathological findings, combined with clinical features, confirmed the diagnosis of a TGDC. Follow-up endoscopic laryngoscopy was conducted at 1 week, 1 month, and 3 months postoperatively, with a repeat CT scan performed at 16 months (Figure 3A-C). These evaluations indicated a good postoperative recovery, with no evidence of recurrence (Figure 3D-E).
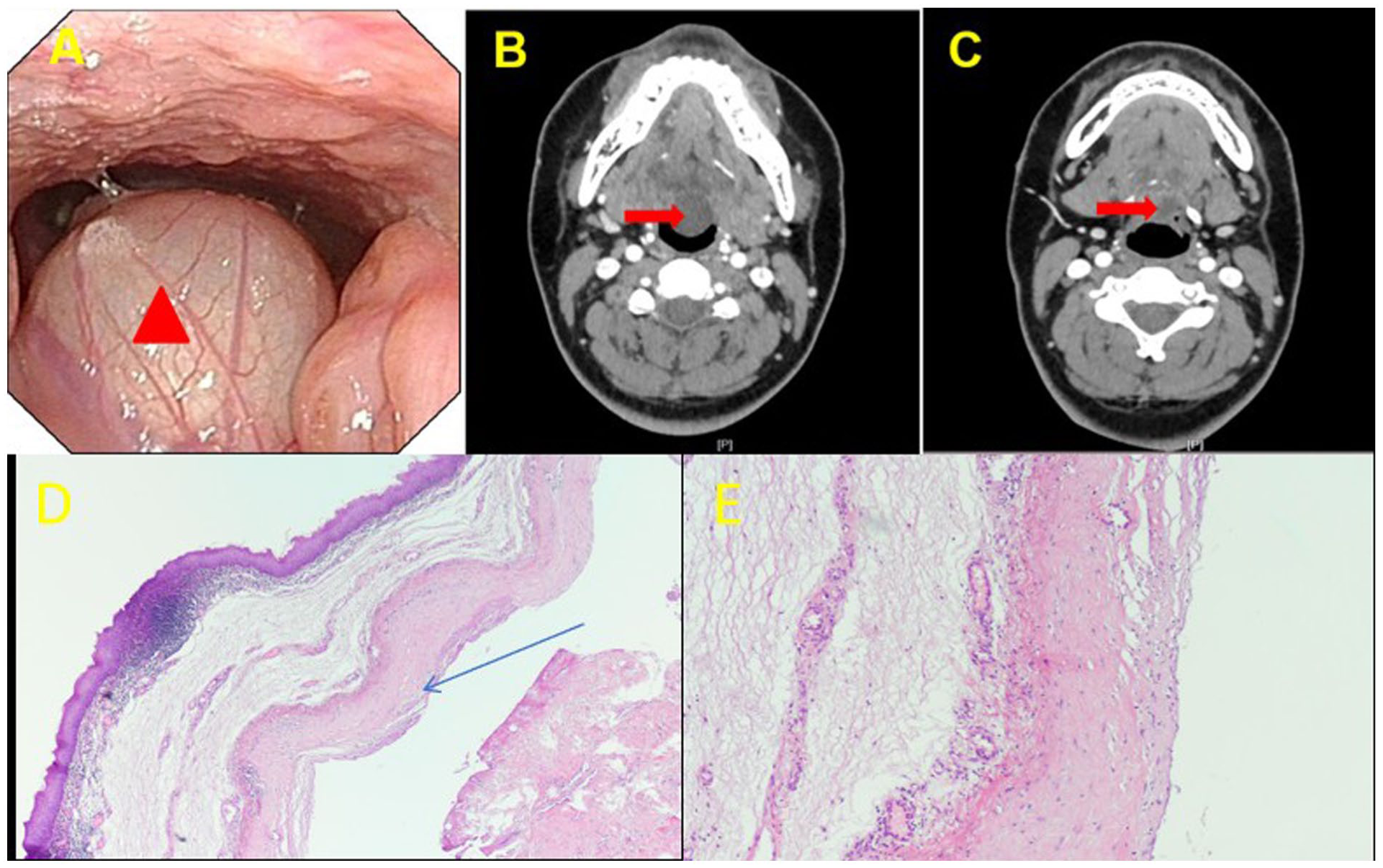
Case example 1. (A) Lesions (red triangles) seen under direct visual vision with an endoscopic laryngoscope; (B, C) CT of the neck showing the lesion was closely related to the base of the tongue (red arrows). (D, E), Histopathological findings on H&E-stained sections (D, ×40; E, ×100). The submucosa beneath the overlying squamous epithelium showed cyst formation. The cyst wall consisted of dense fibrous connective tissue without a definitive epithelial lining and showed collagenization and hyaline degeneration, accompanied by scattered lymphocytes and plasma cells. Focal salivary gland tissue was also observed (blue arrows). CT, Computed tomography.
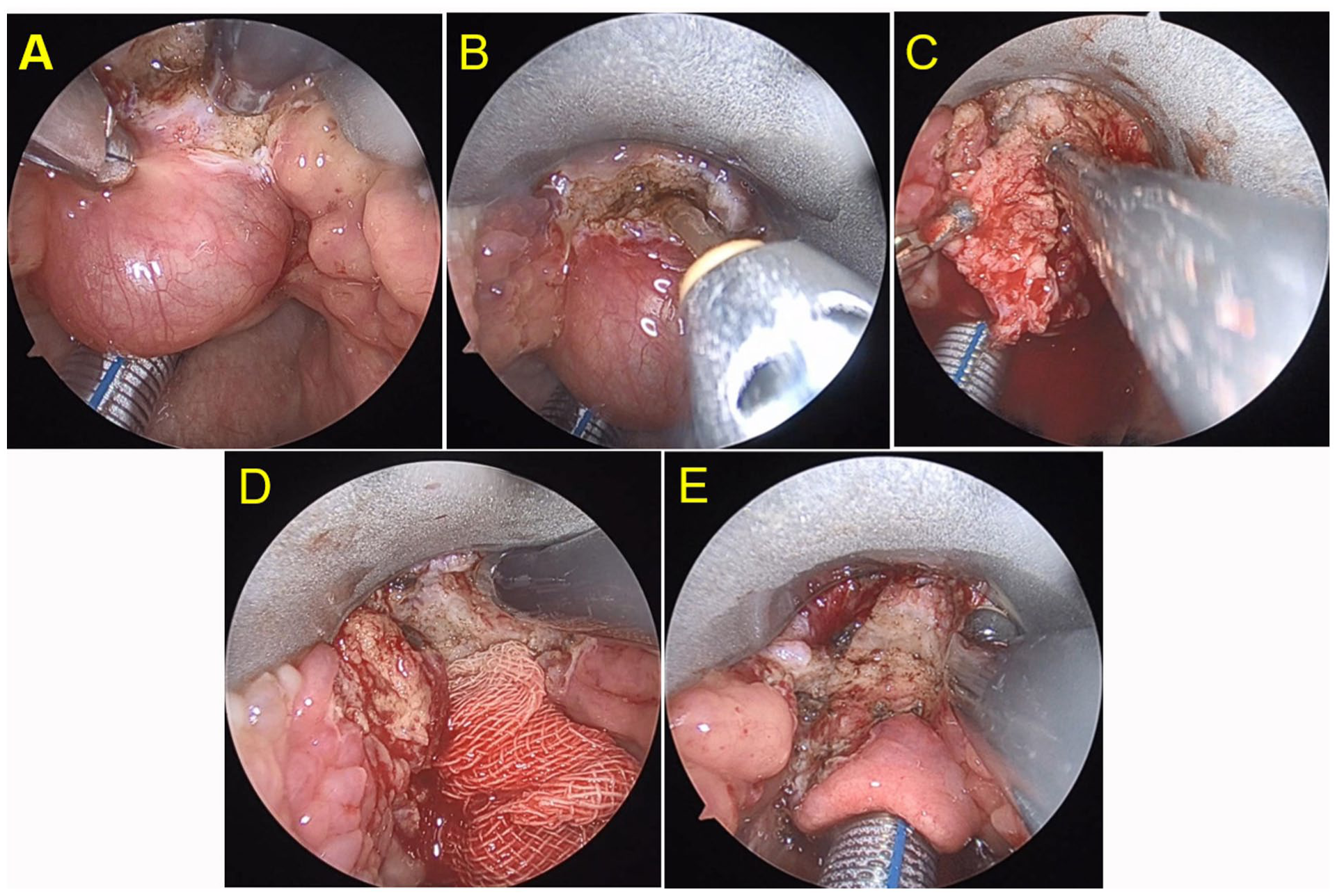
Procedures for endoscopic plasma excision of the tongue root lesion. (A) excised the “head” of the cyst to the tongue muscle layer; (B) Removal of the cyst “head”; (C) Multi-angle traction; (D) Ablation of the medial surface of the hyoid bone; (E) Surgery is complete.
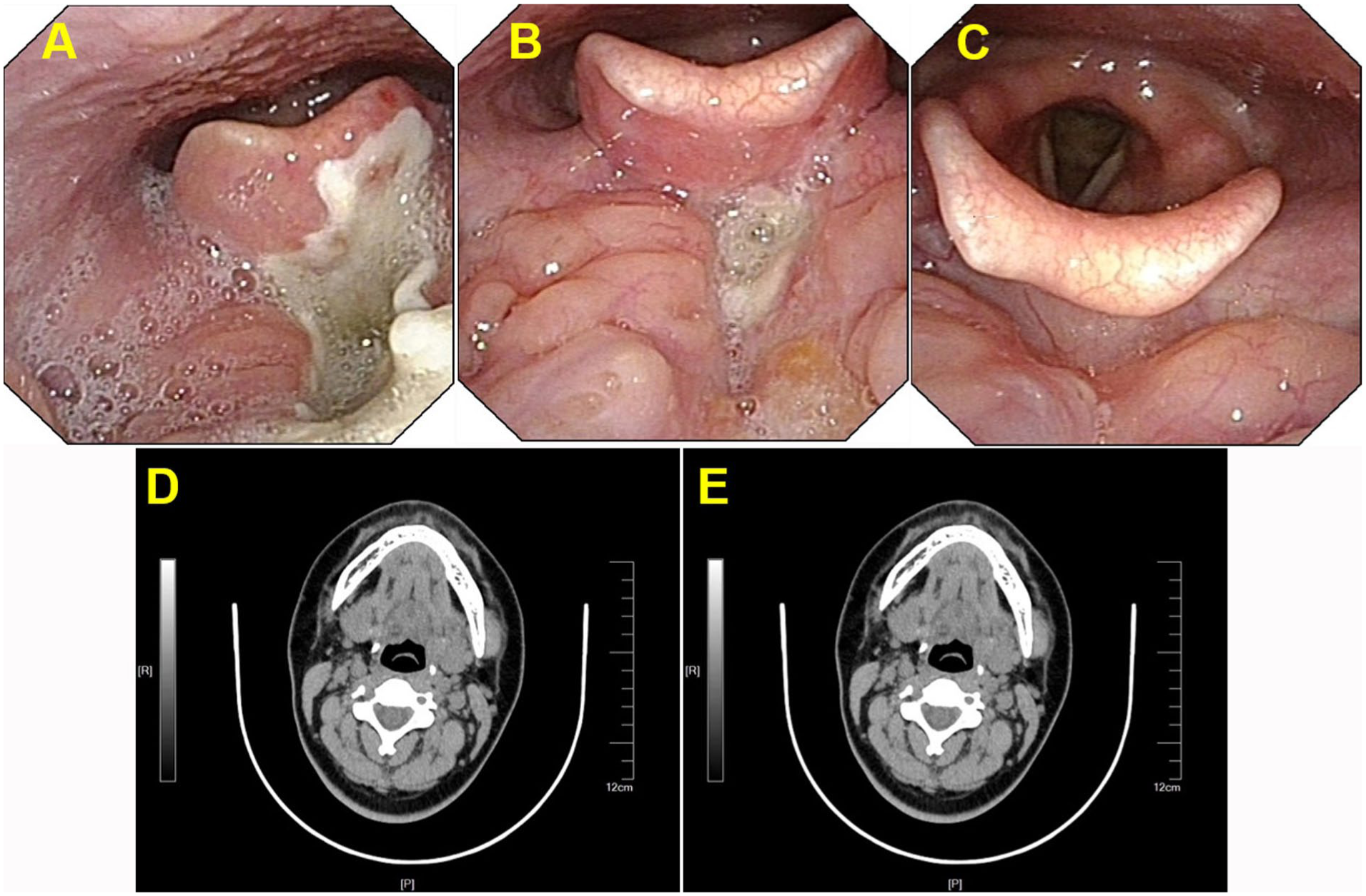
Endoscopic laryngoscopy and CT after surgery for typical case 1. (A) 1 week after surgery, the endoscopic laryngoscope was re-examined; (B) Endoscopic laryngoscopy was re-examined 1 month after surgery; (C) Endoscopic laryngoscopy was re-examined 6 months after surgery; (D, E) There was no recurrence in neck CT 16 months after surgery. CT, Computed tomography.
In the second case, a 12-year-old female patient was admitted with a 10-month history of persistent pharyngeal discomfort (Figure 4). On examination, a palpable mass was identified at the base of the tongue. After admission, an endoscopic laryngoscopy revealed a rounded mass at the posterior aspect of the tongue root (Figure 4A). CT subsequently identified a round lesion in the epiglottic region, consistent with a cystic structure (Figure 4B-C). Surgical excision was performed under laryngoscopic guidance. Histopathological examination revealed fibrous cyst wall tissue without a definitive epithelial lining. The wall demonstrated vascular dilation and congestion, stromal edema, and hemorrhage, accompanied by dense lymphoplasmacytic infiltration. Scattered follicle-like structures were observed at the periphery of the lesion. These findings confirmed the diagnosis of a TGDC (Figure 4D-E). At 3 months postoperatively, follow-up endoscopic laryngoscopy suggested a potential recurrence, and the lesion (Figure 4F). However, the patient currently exhibits no significant symptoms. Routine follow-up visits are ongoing to monitor for recurrence and ensure optimal clinical outcomes (Figure 4G-H). If deemed necessary, surgical intervention will be performed through an open surgical procedure.
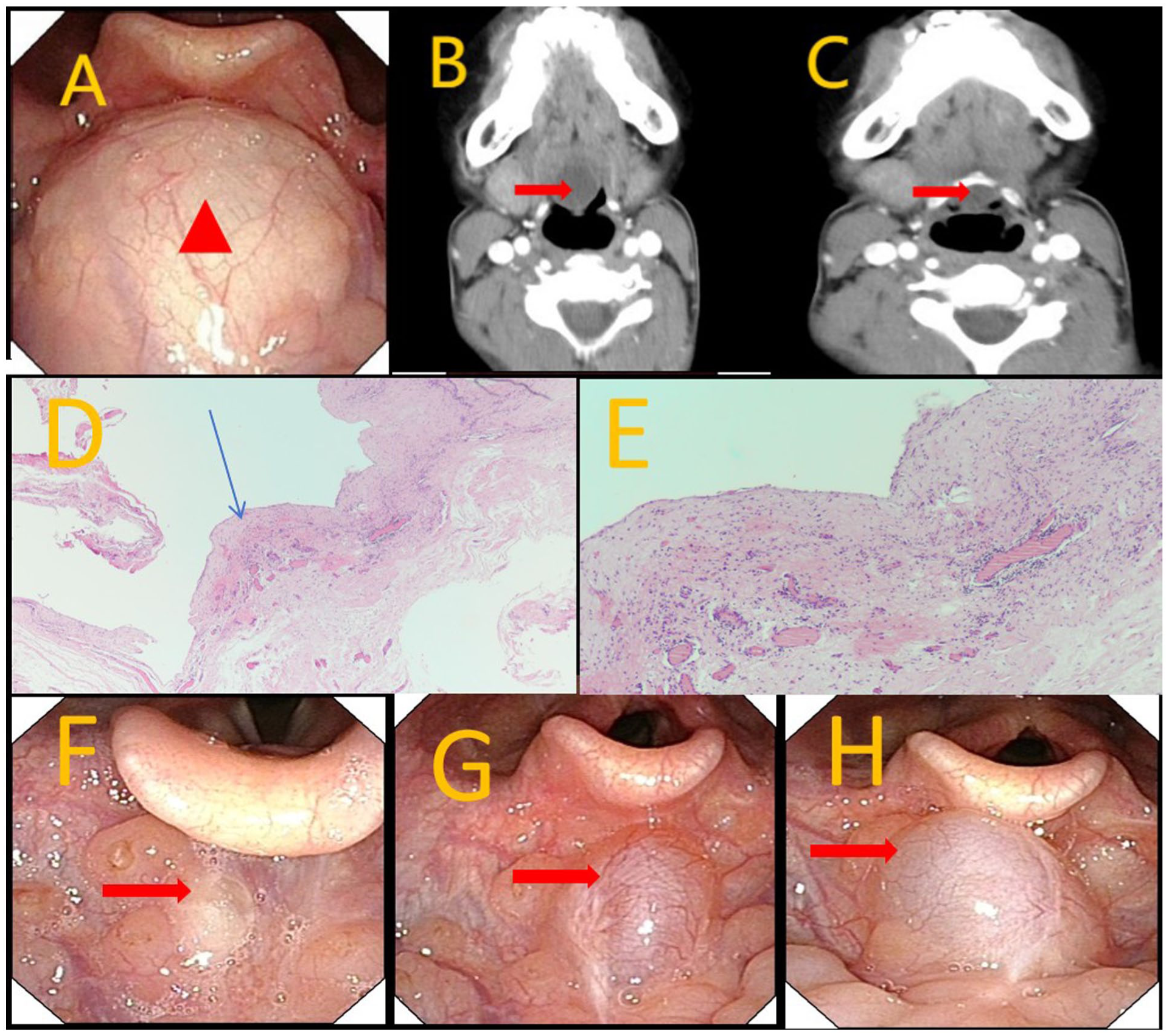
Case example 2. (A) Lesions (red triangles) seen under direct visual vision with an endoscopic laryngoscope; (B, C) CT of the neck showed that the lesion was closely related to the base of the tongue (red arrow). (D, E) Histopathological findings on H&E-stained sections (D, ×40; E, ×100). The submucosa beneath the overlying squamous epithelium demonstrated cyst formation. The cyst wall consisted of dense fibrous connective tissue without a definitive epithelial lining and showed collagenization and hyaline degeneration, with scattered lymphocyte and plasma cell infiltration. Focal follicle-like structures were present, confirming thyroid tissue (blue arrows). (F) The re-examination of the laryngoscope at 3 months postoperatively showing suspected cyst recurrence at the surgical site; (G) The re-examination of the laryngoscope at 6 months postoperatively showing enlarged cyst. (H) The re-examination of the laryngoscope 1 year after the operation showing the cyst enlargement. CT, Computed tomography.
Discussion
In the present study, 17 patients with LTGDC successfully underwent endoscopic excision without conversion to open surgery, tracheotomy, or major complications. Intraoperative blood loss was minimal, and there were no major operative complications. During 2 to 40 months of follow-up, recurrence occurred in 5 patients (29.4%), highlighting that long-term disease control remains the key challenge of this approach.
Normal thyroid development begins in the fourth week of embryogenesis with the formation of the thyroid primordium and reaches its final anatomical position by the 7th week. Failure of the thyroglossal duct to regress may lead to the formation of a TGDC. 7 TGDCs may occur anywhere along the duct’s course—from the foramen cecum at the tongue base to the suprasternal notch. They are most commonly located in the cervical region at the level of the hyoid bone (60%), followed by locations below (24%)8,9 and above (13%) the thyroid. A small proportion (0.5%-2%) arises from the tongue base and is referred to as LTGDCs. The clinical manifestations of LTGDCs are often atypical and vary substantially among patients, influenced by the lesion’s location, size, and the individual’s overall condition. Notably, the predominant symptoms reported in international cohorts differ from those observed in China. Studies from other countries indicate that upper respiratory discomfort is the most common presentation, whereas approximately 15% of patients are asymptomatic, with cysts detected incidentally.2,10 This discrepancy may reflect differences in healthcare referral pathways, as patients in some regions are screened and referred early to primary care facilities. As a result, clinical presentations may be less specific, and disease severity may vary at the time of diagnosis.
LTGDCs are frequently misdiagnosed as epiglottic cysts due to overlapping clinical features. However, compared to LTGDC, an epiglottic cyst is typically located on the epiglottic surface and is characterized by a thinner, more translucent cyst wall. A key distinguishing feature of LTGDC is the presence of a thickened submucosal capsule located at the midline base of the tongue, posterior to the foramen cecum.5,11 Although CT and MRI findings may appear similar, these entities can be differentiated by the structural characteristics at the base of the epiglottic region. Additionally, LTGDCs exhibit distinct epithelial histology, most commonly composed of non-keratinized stratified squamous epithelium. In some cases, pseudostratified or ciliated columnar epithelium may also be observed.6,12,13
The Sistrunk procedure is the standard treatment for TGDC. Since its introduction in 1920, it has significantly reduced the recurrence rate associated with simple cyst excision—from approximately 50% to 2% to 6%. 14 However, for LTGDCs, complete resection as required by the Sistrunk procedure involves a neck incision, hyoid bone resection, removal of the cyst from the lingual root to the foramen cecum, and subsequent placement of a surgical drain.
Transoral endoscopic surgery offers a scarless route that avoids an external cervical incision. The question of how to achieve complete resection of LTGDC via a transoral endoscopic approach remains a topic of ongoing interest among global experts. As early as 1996, Urao proposed an intraoral surgical approach for the management of LTGDC. 15 In this technique, the cyst was incised and sutured during the procedure; however, the cyst base was not adequately addressed.
With advancements in endoscopic technology, the limitations of traditional transoral approaches—such as restricted visualization—have been substantially mitigated. An increasing number of surgeons are now employing endoscopically assisted transoral techniques for the management of LTGDC. In 2009, Burkart performed transoral endoscopic excision in 16 patients with LTGDC using an electrosurgical knife combined with instrumental stripping. None of the patients experienced recurrence during postoperative follow-up, demonstrating the safety and efficacy of endoscopically-assisted transoral surgery. 5 Pereira et al 10 later conducted a systematic evaluation of endoscopic transoral surgery for LTGDC and reported an overall recurrence rate of approximately 1.9%.
Some surgeons recommend endoscopic transoral surgery as the primary treatment for LTGDC. However, others argue that this approach carries a risk of recurrence and maintain that the Sistrunk procedure remains the preferred treatment modality. 16 Nevertheless, for newly diagnosed LTGDC, transoral endoscopic management has gradually gained consensus as a viable and effective approach. 17 In the present study, 17 patients underwent successful and complete transoral endoscopic surgery without postoperative complications such as respiratory distress or bleeding, further supporting the safety of this technique.
For patients with recurrent disease, treatment via a transcervical external approach remains an option. 18 In addition, some researchers have explored the use of the da Vinci robotic system for transoral treatment of LTGDC. This technique offers advantages such as a three-dimensional field of view and a highly flexible robotic arm, allowing for precise lesion excision, and has yielded favorable outcomes.19,20 This approach provides a new surgical option, which warrants further investigation in future studies.
The 29.4% recurrence rate observed in this study may be attributed to several factors, including variations in lesion morphology, the coarse nature of plasma cutting, and a relatively short surgical learning curve, all of which may have impeded complete removal of the LTGDC capsule wall and the residual thyroglossal duct tract. Moreover, previous studies reporting lower recurrence rates for endoscopic approaches may underestimate the actual risk. In the study by Zhang et al, 18 7 patients ultimately required Sistrunk’s procedure as a salvage treatment following multiple failed endoscopic excisions, suggesting that initial endoscopic management may not consistently achieve a definitive cure. This may partially explain the low recurrence rate reported by Perreira et al. 10 Therefore, our findings, although based on a small cohort, may better reflect the actual recurrence risk associated with transoral endoscopic excision. With ongoing accumulation of cases, increased surgical experience, and refinement of operative techniques, the recurrence rate of this procedure is expected to decline.
Endoscopic plasma resection of LTGDC is considered a highly safe procedure. The endoscopic system’s high-definition magnification meets surgical visualization requirements, whereas the low-temperature plasma device enables both cutting and coagulation, with adjustable angles that allow for flexible lesion resection and adequate hemostasis. Nevertheless, this technique has certain limitations. It requires one-handed operation, and even with an assistant holding the endoscope, interference between the scope and instruments can hinder maneuverability. Continuous adjustment of the angle and depth of the plasma electrode is necessary to ensure full exposure of the lesion, which can prolong operative time and increase the risk of bleeding from potential trauma to the tongue base. All 17 procedures in this study were completed successfully. The longer operative times observed in some cases, particularly in early-stage patients, may be attributed to the time required for hemostasis and repeated intraoperative observation.
Multiple transoral strategies have been reported for LTGDC, including suspension-laryngoscopic/endoscopic or microscopic excision using cold instruments with electrocautery (and sometimes microdebrider assistance), marsupialization/decapping in selected cases, and energy-based refinements such as CO2 laser–assisted excision with adjunctive treatment of the presumed “root” region. 5 More recently, transoral robotic surgery has also been described to improve exposure and instrument dexterity for tongue-base excision. 21 Across these approaches, recurrence appears closely related to completeness of cyst-wall removal and, critically, how the root/hyoid–foramen cecum-associated tract is managed. 22
A key component of our procedure is adjunctive radiofrequency plasma ablation at the cyst root on the inner surface of the midline hyoid region, facilitated by external cervical compression to improve access. Conceptually, this step is intended to address potential epithelial remnants along the tract insertion/attachment near the hyoid–foramen cecum axis, analogous to the rationale of tract management in Sistrunk surgery. Because the transoral approach does not remove the hyoid bone, targeted periosteal ablation may help reduce residual epithelial tissue at the root. Nevertheless, ablation should be viewed as an adjunct rather than a substitute for meticulous cyst-wall excision: inadequate exposure, incomplete capsule dissection, or insufficient treatment of the root region can still result in recurrence. In addition, energy delivery at the tongue base requires careful depth control to balance thoroughness against risks of thermal injury, edema, odynophagia, and postoperative bleeding.
Although the transoral approach avoids an external cervical incision and provides a scarless cosmetic advantage, it does not necessarily translate into faster postoperative recovery. In our series, oral intake was initiated on postoperative day 3 as part of a conservative airway-safety pathway after tongue-base mucosal intervention, when postoperative edema, odynophagia, and concerns about bleeding or aspiration may be more prominent. By contrast, Sistrunk procedures are often managed with early oral intake. 23
In this study, 2 adult patients underwent surgery despite being asymptomatic at presentation because of concerns about disease progression, which could entail additional time, effort, and potential impact on their work. Moreover, they are familiar with transoral surgical approaches and elected to proceed with surgical treatment. However, for the 12-year-old patient who experienced recurrence detected during follow-up after the initial surgery, concerned about the potential risks of a second operation, the family opted for close monitoring and chose to defer further surgery until adulthood, if necessary.
Several operative principles may help optimize outcomes. First, adequate exposure to the lesion is essential. Intraoperatively, active decompression of the lesion is recommended to reduce mass effect and facilitate retraction of the cyst wall. Multi-angle retraction improves visualization and supports more efficient surgical manipulation. Second, applying external cervical pressure over the hyoid and ablating its central medial tissue with a plasma device enables thorough management of the cystic tract at its root. Third, surgical dissection should be centered along the midline. The plasma tip should be directed toward the lesion, with maximal stripping of the surrounding tissue to minimize linear incisions and reduce the risk of injury to the lingual artery.
This study has several limitations. The main limitation is the relatively high recurrence rate, suggesting that the transoral endoscopic approach as applied in this cohort may not achieve disease control comparable to Sistrunk surgery; therefore, Sistrunk remains the treatment of choice for most patients when feasible, and transoral surgery should be reserved for carefully selected cases with appropriate counseling regarding recurrence risk. Second, postoperative diet advancement was relatively conservative, which may reflect a functional recovery disadvantage relative to typical Sistrunk management. Third, intraoperative blood loss was estimated by subtracting recorded irrigation volume from suction canister volume; this method may underestimate actual blood loss because blood can be retained in gauzes, adhere to instruments, be swallowed, or not be thoroughly suctioned, and measurements may be affected by unrecorded fluids.
In conclusion, transoral endoscopic surgery for lingual root-type thyroglossal cysts is still in the exploratory stage, but its feasibility and safety suggest it is a viable alternative to a traditional Sistrunk procedure. The relatively high recurrence rate, however, indicates the necessity for further in-depth exploration and enhancement of related studies, including prospective multicenter trials.
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of Affiliated Drum Tower Hospital of Nanjing University Medical School and conducted in accordance with the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all individual participants included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are accessible and sharing can be made available when requested.*