
Abstract
Objective
The aim of this study was to investigate the psychological distress associated with long-lasting COVID-19 olfactory dysfunction (OD).
Methods
Patients with an OD lasting for more than 6 months were consecutively recruited from the Dour Medical Center (Belgium) from August 2023 to January 2024. The olfaction was investigated with the Olfactory Disorder Questionnaires (ODQ) and the threshold, identification, and discrimination (TDI) testing. General Anxiety Disorder (GAD-7) and Patient Health Questionnaire (PHQ-9) were used to investigate the psychological distress of patients. The olfactory and psychological outcomes of patients were compared with a group of individuals without OD.
Results
A total of 220 patients and 102 asymptomatic individuals completed the evaluations. The mean duration of OD was 31.1 ± 25.1 months. The mean GAD-7 and PHQ-9 scores were significantly higher in OD patients than in asymptomatic individuals (P < 0.008). The OD patient prevalence of mild-to-severe depression (51.2% vs. 44.1%) and mild-to-severe anxiety (39.5% vs. 32.4%) disorders was significantly higher than asymptomatic individuals. Severe anxiety was associated with the presence of anosmia. GAD-7 and PHQ-9 scores were higher in females than in males. The severity of depression (PHQ-9) and anxiety (GAD-7) was significantly associated with the severity of OD (ODQ) and nasal symptoms (SNOT-22).
Conclusion
The presence of a long-lasting OD in patients consulting in otolaryngology is associated with psychological distress. While the causality relationship remains unclear, depression and anxiety symptoms must be investigated in this subgroup of patients with long COVID-19.

Keywords
Introduction
The olfaction plays a crucial role in human social interactions, in transforming eating from a simple vital function to a pleasant activity, and for detecting environmental hazards. 1 The coronavirus disease 2019 (COVID-19) pandemic has highlighted the importance of olfaction according to the large percentage of patients suffering from olfactory dysfunction (OD) at 2 years postinfection (up to 29.8%), including hyposmia, anosmia, phantosmia, or parosmia.2,3 To date, it is estimated that 45 to 90 million of COVID-19-infected individuals still suffer from persistent olfactory or gustatory dysfunctions worldwide. 2 In addition to potential dangers related to the inability to smell, the impairment of olfaction may be associated with psychological distress.4,5
The economic burden related to depression in populations of Western countries and the prevalence of OD may encourage practitioners and researchers to conduct studies tackling psychological symptoms in survivors of COVID-19. 6
To date, most studies investigating the psychological distress related to long-lasting OD have been carried out before the pandemic in patients with long-lasting OD, which was not related to postviral infection.7-11
The aim of this study was to investigate the psychological distress in patients with a long-lasting OD related to COVID-19.
Methods
Setting
This study adhered to the STROBE guidelines for observational studies to ensure transparency and replicability of our findings. Patients with post-COVID-19 long-lasting OD were consecutively recruited from August 2023 to January 2024 in the Dour Medical Center (Belgium). The long-lasting OD consisted of hyposmia, anosmia, parosmia or phantosmia lasting for more than 6 month after the resolution of the COVID-19. Anosmia and hyposmia were defined with the threshold, discrimination, and identification test (TDI). 12 Anosmia was a TDI score ≤16 points and hyposmia was established as a TDI score of less than 30.75. Normosmia consisted of a TDI >30.75. 12 In the present study, patients were included if they had a TDI score below 30.75 or if they reported qualitative OD independently from the TDI score (parosmia or phantosmia). They were interrogated to be classified as anosmic, hyposmic, parosmic/phantosmic depending on the primary complaint and the TDI. If patient with abnormal TDI reported that the most important symptom is parosmia, the patient was classified as parosmic. The exclusion criteria were patients with sinus or olfactory region abnormalities at the nasofibroscopy and imaging (eg, rhinosinusitis, olfactory, or nasal tumor); clinical signs of rhinitis; post-traumatic OD; neurological OD; idiopathic OD; chronic rhinosinusitis with or without nasal polyposis; history of nasal chemo/radiation or functional endoscopic sinus surgery; and severe neurological or psychiatric comorbidities, including depression prior to the occurrence of the OD.
A control group of asymptomatic individuals without reported OD was composed from the University of Mons and the Dour Medical Center communities. Asymptomatic individuals met the same exclusion criteria as COVID-19 patients. In practice, controls were staff of the University of Dour Medical Center. The study protocol was approved by the local ethics committee (ref. 2102028). The electronic informed consent was obtained for all patients.
Demographic, Olfactory, and Psychological Outcomes
The following data were collected: age, gender, comorbidities, allergy, tobacco consumption, previous adherence to an olfactory training protocol, and the medication/dietary supplement intakes.
The subjective evaluation of olfaction was carried out with the French version of the Olfactory Disorder Questionnaire (ODQ), which is a validated patient-reported outcome questionnaire including parosmia (/12), quality of life (/57), and sincerity (/18) scores (Appendix 1). 14 The ODQ score ranges from 0 (no OD) to 87 (severe impact of OD on the quality of life). The psychophysical evaluations consisted of the threshold, discrimination, and identification (TDI) testing (Medisense, Groningen, the Netherlands). 12 Sinonasal symptoms were evaluated with the French version of the Sino-Nasal Outcome Test-22 (SNOT-22). 13
Anxiety levels were evaluated by the French version of the General Anxiety Disorder-7 (GAD-7), which is a validated and standardized patient-reported outcome questionnaire assessing the severity of anxiety of patients from 0 to 21 (Appendix 2). 14 According to large population databases, minimal, mild, moderate, and severe anxiety consisted of 0-4, 5-9, 10-14, and 15-21 scores, respectively.
The French version of the Patient Health Questionnaire-9 (PHQ-9) was used to evaluate the depression symptoms of patients. 15 PHQ-9 is a brief validated and standardized tool used to diagnose and measure severity of depression (Appendix 3). PHQ-9 is adapted from the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV), and suggests minimal, mild, moderate, moderately severe, and severe depression for 1-4, 5-9, 10-14, 15-19, and 20-27 scores, respectively.
Statistical Analyses
Statistical analyses were performed using the Statistical Package for the Social Sciences for Windows (SPSS, v29.0; IBM Corp, Armonk, NY, USA). The descriptive data related to the prevalence of anxiety and depression were reported. The anxiety and depression scores were compared between asymptomatic individuals, and patients with anosmia, hyposmia, and parosmia/phantosmia with Student’s t-test. The proportion of depression and anxiety disorders was compared between groups with a chi-squared test. The associations between demographics, comorbidities, olfactory, and psychological outcomes were investigated with a chi-squared test or the Spearman rho regarding the type of data. A P-value <.05 was considered as significant.
Results
A total of 220 patients and 102 asymptomatic individuals were consecutively recruited from the Dour Medical Center and the University of Mons. Two patients from the OD group did not complete the questionnaires. There were 136 (61.8%) females and 84 (38.2%) males in the study group (Table 1). Asymptomatic individuals included 75 (73.5%) females and 27 (26.5%) males. The mean age of patients was 51.3 ± 14.8 years, and the mean age of asymptomatic individuals was 41.2 ± 16.8 years. The main comorbidities of patients and asymptomatic individuals are described in Table 1. Five (4.9%) asymptomatic individuals and 13 (5.9%) patients reported a history of diagnosed depression in the past 5 years. The olfactory data of patients are available in Table 2. The mean duration of OD was 31.1 ± 25.1 months. The PHQ-9 and GAD-7 data are described in Table 3. The mean PHQ-9 was significantly higher in patients (mean: 6.12; 95%CI: 5.37-6.87) than in asymptomatic individuals (mean: 4.4; 95%CI: 3.7-5.0; Table 3). The mean GAD-7 scores of patients (mean: 4.6; 95%CI: 3.9-5.3) were significantly higher in patients than in asymptomatic individuals (mean: 3.5; 95%CI: 2.8-4.1; Table 3). Note that the olfactory data were completed for 205 patients. Twenty patients had either ODQ or TDI data and were not included in the analysis exploring the influence of the type of the OD on the psychological status. Patients primarily had anosmia, hyposmia, and parosmia in 54 (26.3%), 69 (33.7%), and 82 (40.0%) cases, respectively.
Demographics.

Abbreviations: N, number; NS, nonsignificant; SD, standard deviation.
Vaccination and Olfactory Characteristics of Patients.

Abbreviations: OD, olfactory dysfunction; ODQ, olfactory disorder questionnaire; SNOT-22, Sino-Nasal Outcome Test-22; TDI, threshold, discrimination, identification.
Psychological Outcomes.

Abbreviations: GAD-7, General Anxiety Disorder-7; PHQ-9, Patient Health Questionnaire-9.
Student-t test.
The OD patient prevalence of mild-to-severe depression (51.2% vs. 44.1%) and mild-to-severe anxiety (39.5% vs. 32.4%) disorders was significantly higher than in asymptomatic individuals (Table 4). Precisely, OD patients had a significantly higher proportion of moderate and severe depression, and moderate and severe anxiety than in asymptomatic individuals (Figure 1). The proportion of individuals without depression, minimal depression, minimal anxiety, and mild anxiety did not differ between both groups. When considering subgroups of patients (anosmic, hyposmic, and parosmic patients), anosmia was reported to be associated with a significantly-higher proportion of severe anxiety than in other groups (P = .005; Table 4).
Proportion of Depression and Anxiety in Groups.
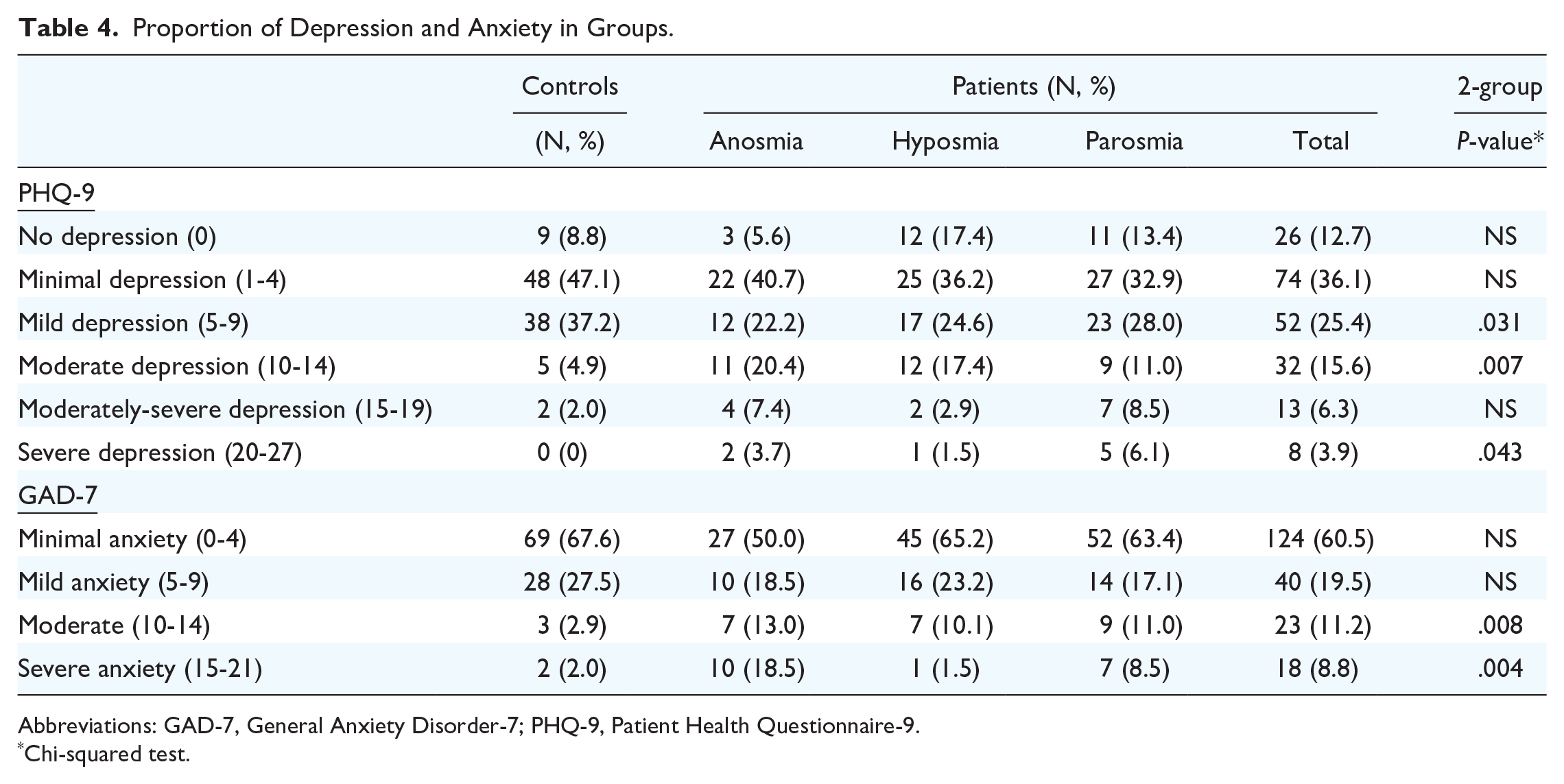
Abbreviations: GAD-7, General Anxiety Disorder-7; PHQ-9, Patient Health Questionnaire-9.
Chi-squared test.
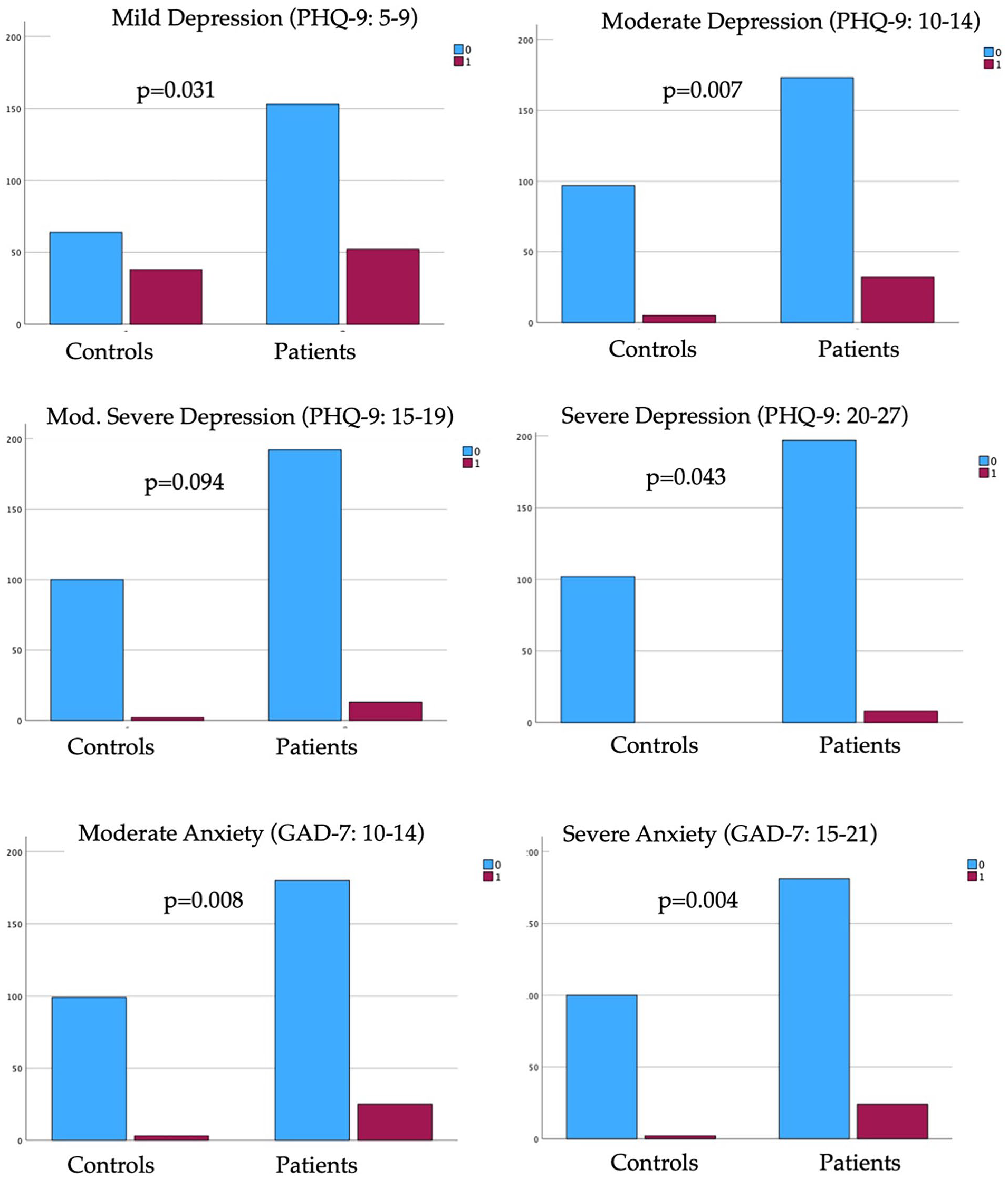
Proportion of mild-to-severe depression and anxiety disorders in patients versus asymptomatic individuals.
Influencing Factors
Gender and vaccine status significantly influenced the depression or olfactory outcomes considering all vaccines as equal. Note that the following vaccines have been used for single, twice, thrice, or fourth vaccination: Pfizer (N = 102, 65.8%), Moderna (N = 26, 16.8%), Astra Zeneca (N = 22, 14.2%), and Johnson & Johnson (N = 5, 3.2%). The others did not remember about the manufacturer. The mean PHQ-9 of females (mean: 6.7; 95%CI: 5.8-7.6) was significantly higher than that of males (mean: 5.2; 95%CI: 4.1-6.3; P = .010). The mean GAD-7 of females (mean: 5.1; 95%CI: 4.3-6.0) was significantly higher than that of males (mean: 3.9; 95%CI: 2.9-4.9; P = .032). There were no other significant differences between females and males in demographics, and olfactory outcomes.
A total of 155 patients declared their pre-OD vaccine status, accounting for 36 unvaccinated and 119 vaccinated patients, respectively. In this group of patients, vaccines were administrated before the occurrence of OD. The mean PHQ-9 of unvaccinated patients (mean: 6.9; 95%CI: 4.8-10.0) was significantly higher than those of vaccinated patients (mean: 5.9; 95%CI: 4.9-6.9; P = .005). The parosmia score was similarly higher in unvaccinated patients than in vaccinated patients (mean: 7.3 [95%CI: 6.3-8.3] versus 5.9 [95%CI: 5.3-6.5]; P = .037).
Association Analyses
The Spearman analysis reported significant negative associations between the duration of the OD and the PHQ-9 (rs = −0.197; P = .014) and the GAD-7 (rs = −0.210; P = .010). The PHQ-9 was positively correlated with the ODQ (rs = 0.633; P = .001) and the SNOT-22 (rs = 0.475; P = .001). The GAD-7 reported significant positive association with the ODQ (rs = 0.531; P = .001) and the SNOT-22 (rs = 0.628; P = .001). PHQ-9 and the GAD-7 were significantly correlated (rs = 0.802; P = .001).
Discussion
To date, only a few studies have investigated the psychological distress in patients with long-lasting OD related to COVID-19.7-11 However, OD is associated with significant detriments to health-related quality of life and has emerged as a public health concern since the COVID-19 pandemic.16,17
The primary findings of this cross-sectional study were the observation of significantly-higher depression and anxiety scores and related prevalence in patients with OD than in individuals without OD history. The association between OD and psychological distress was investigated in COVID-196-8,18.19 and non-COVID-19 studies.20,21
In a cross-sectional survey of 364 patients, Bochicchio et al. found a significant association between psychological distress (Kessler Psychological Distress) and the presence of a long-lasting history of OD in COVID-19 patients. 7 Interestingly, they observed that females are more susceptible to be psychologically affected by the OD than males, which corroborated our observations. 7 In the same vein, Elkholi et al. conducted a cross-sectional study in 487 patients with COVID-19 who were assessed with the Multi-Clinic Smell and Taste Questionnaire and the General Well-being Schedule. 9 Similarly to Bochicchio et al., the authors reported a significant association between the presence of patient-reported OD and the deterioration of mental health. 9 The results of these studies conducted in COVID-19 patients strengthened those of investigations from before the pandemic, which reported significant deterioration of psychological health in patients with long-lasting hyposmia, anosmia, or parosmia.10,21,22 The impact of OD and related retro-olfaction disorder on mental health was similarly supported by Tchekmedyian et al., who reported that patients with diminished smell did not enjoy food and felt unsafe when eating food in 71% and 63% of cases, which contributed to impairing their well-being. 10 The mental health is also important for the recovery process. Sabiniewicz and Hummel showed that patients with OD and high scores on a depressive scale are more willing to adhere to olfactory training protocols due to the depressive symptoms. 11 In 2022, Liu et al. published the results of a prospective study including 192 patients with COVID-19 and non-COVID-19 OD investigating the association between the Questionnaire of Olfactory Dysfunction (QOD), Patient Health Questionnaire-2 (PHQ-2), and demographics. 20 The authors reported a significant association between the severity of QOD, and PHQ-2, which corroborates our findings. In this study, the authors observed an influence of sinonasal symptoms on the PHQ-2, which indirectly corroborates our positive significant association between the SNOT-22 and the psychological tool scores. Because our OD patients did not have chronic rhinosinusitis, this observation may potentially support the existence of continuous inflammation, damage to basal cells, and chronic inflammatory reaction into the nasal mucosa of some patients with long-lasting OD related to COVID-19.8,23 In this way, it is important to note that some recent observations supported a high prevalence of nasal symptoms imitating chronic rhinitis or rhinosinusitis in COVID-19 patients without chronic rhinosinusitis or rhinitis diagnosis.24-27 Thus, the presence of these symptoms may be considered as an aggravating factor of psychological distress in OD patients. Despite these few studies reporting significant associations between OD and psychological distress, the causal link between these conditions remains a mystery. Indeed, it is unclear whether patients with long-lasting OD and a preexisting anxiety or depression disorder more commonly consult in olfaction clinics than others with long-lasting OD without anxiety or depression condition. The potential consultation bias is the primary limitation of the present study, and it is possible that the anxiety and depression symptoms were preexisting in our recruited patients. The controversy is powered by recent studies that have suggested a potential relationship between some symptoms of long COVID-19 and the development of psychological distress. 8 In the USA, Taquet et al. observed in a retrospective study of 62,354 COVID-19 cases that 5.8% of patients had a new psychiatric diagnosis in the 14–90 days after COVID-19 infection. 27 However, the authors specified that the etiological link cannot be demonstrated because there are multifactorial causes of depression and anxiety, and the preexisting psychiatric disorder status of patients was unknown. In another study, Kataoka et al. observed that the presence of a preexisting psychiatric disorder increases the risk of developing long-COVID-19 symptoms. 28 Finally, the observation of a higher prevalence of OD in psychiatric patients than in healthy individuals. 29 is an additional point, which strengthens the complexity of the associations between both conditions. 30
The lack of psychophysical olfactory testing in our control group is a limitation. COVID-19 vaccines demonstrate comparable protection against severe disease outcomes; however, variations in vaccine availability and selection may introduce bias when evaluating subtle immunological differences between vaccine types. Moreover, 46% of patients with long-lasting OD were unvaccinated, which is significantly higher than the national mean rate (10%). 31 To date, the relationship between vaccination status and long-term olfactory dysfunction has not been definitively established. The design (cross-sectional study) can be considered as an additional limitation, while a prospective study evaluating psychological distress before and after the development of OD should be more appropriate. Note that our study reported that controls had a higher proportion of mild depression than patients. The higher proportion of females in the control group might have impacted the comparison between groups because the prevalence of depression is commonly higher in females than in males. Because patients had significantly-higher proportions of moderate and severe depression than controls, the related proportion of mild depression in the patient group was expected.
The originality of this study is its primary strength. Indeed, there are few high-quality studies investigating the psychological distress of patients with long-lasting COVID-19-related olfactory dysfunction (OD) through both validated patient-reported outcome questionnaires (ODQ, PHQ-9, GAD-7) and psychophysical olfactory testing. Moreover, to the best of our knowledge, this study represents one of the largest investigations assessing psychological distress in patients with long-lasting COVID-19-related OD while considering multiple cofactors (eg, comorbidities, vaccination status, previous treatments, nasal symptoms, and olfactory training adherence).
Conclusion
The presence of a long-lasting OD in patients consulting in otolaryngology is associated with psychological distress. While the causality relationship remains unclear, depression and anxiety symptoms must be investigated in this subgroup of patients with long COVID-19.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Ethic committee
Not required.
Informed consent
Not applicable.