
Abstract
Importance
Perineural invasion (PNI) is an established prognostic factor in oral squamous cell carcinoma (OSCC), but the impact of its subcategories on survival is not fully understood. This study quantifies the number and diameter of PNI foci to assess their prognostic relevance in OSCC.
Objective
To evaluate the prognostic significance of PNI subcategories, specifically the number and diameter of PNI foci, as predictors of overall survival (OS) and disease-free survival (DFS) in OSCC patients.
Design
Retrospective cohort study, adhering to STROBE guidelines.
Setting
Single-center study at MacKay Memorial Hospital, Taiwan, including patients diagnosed with OSCC from 2005 to 2018.
Participants
Nine hundred twenty-six patients with biopsy-proven OSCC, excluding those with perioperative mortality or incomplete follow-up.
Exposure
Histological evaluation of PNI, including quantifying the number and diameter of invaded nerves, along with clinicopathological features such as tumor stage and lymphovascular invasion (LVI).
Main Outcome Measures
OS and DFS, assessed via Cox proportional hazards models, Kaplan–Meier survival analysis, and receiver operating characteristic curve analysis for PNI foci subcategories.
Results
PNI was present in 138 (14.9%) patients and was significantly associated with adverse histologic features, advanced tumor stage, nodal involvement, metastasis, and LVI. Multivariate analysis revealed that both the number of PNI foci greater than 4 and nerve diameters exceeding 0.21 mm were significantly associated with poorer OS and DFS (P < .05). After adjusting for clinical variables, PNI remained an independent predictor of worse OS [hazard ratio (HR): 1.37] and DFS (HR: 1.46).
Conclusions and Relevance
PNI is a significant independent prognostic factor in OSCC. Patients with more than 4 PNI foci or nerve involvement greater than 0.21 mm in diameter experienced significantly worse survival outcomes. These findings suggest that detailed assessment of PNI subcategories should be incorporated into OSCC management, guiding treatment decisions and potentially informing the need for adjuvant therapies.
Background
Oral squamous cell carcinoma (OSCC) is a prevalent malignancy of the upper aerodigestive tract characterized by poor prognosis and elevated mortality rates, with more than 50% of patients diagnosed at an advanced stage.1,2 Despite advancements in multimodal treatments, including surgery, radiotherapy, and chemotherapy, OSCC continues to pose significant challenges worldwide, marked by high recurrence and mortality rates.3-5 Numerous variables have been scrutinized in the quest to identify prognostic factors in oral carcinoma, falling broadly into 3 categories: tumor-related, patient-related, and treatment-related factors. 6 Among the recognized prognostic factors, the tumor, node, and metastasis (TNM) stage, histological grade, and tumor thickness are nearly universal recognition. However, the prognostic significance of various other clinicopathological factors often remains uncertain and subject to controversy.3,4,6,7 Lymphovascular invasion (LVI) and perineural invasion (PNI) are notably utilized parameters indicative of aggressive behavior and are crucial in predicting the outcome of OSCC.5,6,8-10
PNI is primarily defined by the invasion of nerves by neoplasms, which can occur without involvement of lymphatic or vascular pathways. Instead of spreading through lymphatic dissemination, its progression is guided by molecular mediators that facilitate neural invasion by these cells. This phenomenon is characteristic of specific tumors exhibiting inherent neural tropism, often referred to as “neurotropic malignancies,” and may occur independently of lymphatic or vascular invasion. 8 PNI entails the directional movement of tumor cells toward nerve bundles in the adjacent tissues. It constitutes a distinct form of metastatic tumor spread, differing from both vascular and lymphatic invasion. This unique mode of dissemination poses challenges for achieving local control of malignancies, as neoplastic cells can traverse along nerve pathways, extending well beyond the primary lesion and often eluding detection during surgical procedures. 8 The Royal College of Pathologists in the United Kingdom and the College of American Pathologists have acknowledged the significance of PNI in influencing treatment decisions. To underscore its importance, both institutions have included the documentation of PNI in the standard pathology report for OSCC. 11
While it is widely accepted that PNI tends to indicate a poorer prognosis,10,12-16 there exists contradictory evidence in the literature regarding its correlation with recurrence and overall survival (OS). Several studies have reported that the presence of PNI does not necessarily lead to reduced local control or OS.17-25 At present, PNI is commonly categorized simply as either absent or present, with no unified agreement on delineating its type and extent. However, evidence in the literature indicates that histopathologic subcategories of PNI may offer supplementary prognostic insights.13-15,26 The research conducted by Aivazian et al revealed that the extent of PNI could serve as a predictor for local failure (LF) and disease-specific mortality. 13 In their study, the presence of unifocal PNI and its distance from the tumor did not exert a significant influence on prognosis. However, multifocal PNI emerged as a notable factor, being significantly associated with heightened risks of LF and disease-specific mortality. The presence of PNI as a binary factor alone did not significantly influence the clinical outcomes. The presence of multifocal and ET PNI in OSCC is associated with poor clinical outcomes. Patients with multifocal PNI were associated with worse disease-free survival (DFS) even with adjuvant therapy. 27 Miller et al found in their study that the location of PNI relative to the tumor edge could potentially predict DFS, as extratumoral PNI was significantly linked to a shortened DFS period. 14
To date, there have been relatively few studies investigating the correlation between the histopathologic subcategories of PNI and their prognostic significance in OSCC. The objective of this study was to assess whether the extent of PNI and the size of the nerve involved could predict clinical outcomes in patients with OSCC.
Materials and Methods
Participants and Data Collection
We conducted a retrospective analysis of the medical records of 1024 patients who had not undergone previous treatment and were diagnosed with biopsy-proven squamous cell carcinoma of the oral cavity. This study was approved by the institutional review board of MacKay Memorial Hospital (approval number: 24MMHIS006e). The final study population includes 926 cases after exclusion patients with perioperative mortality (within 30 days of surgery) and incomplete clinical follow-up. Surgeries were performed as the primary treatment method at our hospital between January 2005 and March 2018. Each patient underwent thorough primary tumor excision, elective neck dissection in addition to various types of oral defect reconstruction. Recurrence of the disease was determined either by radiologic evidence with clinical correlation or histologic confirmation through biopsy. Survival follow-up data, including DFS and OS, were gathered from medical records, death certificates, registration offices, and the Clinical Cancer Registry of MacKay Memorial Hospital.
All surgical specimens were fixed in 10% buffered formalin, embedded in paraffin, and sectioned for histopathological examination, stained with hematoxylin and eosin. A senior oral pathologist reviewed the samples using a microscope (BX43; Olympus, Hachioji, Tokyo, Japan) with 10× ocular lenses, scanning for PNI foci. Sections were examined first with a 4× objective lens (40× total magnification), and then rechecked with 10× or 20× lenses (100× to 200×). Practically, PNI foci was determined when tumor cells invaded the total or near total nerve circumference. 28 In cases of equivocal conditions, immunohistochemical studies with S-100 protein and cytokeratin AE1/AE3 were used for confirmation. To prevent duplicate counting of PNI foci within each section, consistent criteria for identifying PNI foci were applied to all sections. A mark is labeled next to each counted focus. Total number of PNI foci in the entire sampled sections was counted. The extent of PNI was determined by classifying the number of PNI foci when PNI was present. The number of distinct sites of PNI was generated after counting and summing the PNI foci from all tumor sections.29,30 This included the presence of distinct foci of PNI situated at various locations within the tumor, engagement of multiple nerve twigs converging onto a substantial nerve bundle within the same tissue block, and involvement of multiple nerve twigs in a specific area not readily attributed to the convoluted course of the nerve or tangential sectioning alone. An eyepiece micrometer was used to measure the diameter of the invaded nerve during microscopic examination. Other evaluated pathological variables included LVI, histological grade, and surgical resection margin. Clinical, demographic, and histopathological data were collected from the medical records of the patients. Demographic data, including age, sex, clinical stage, and final status (survived or expired), were obtained from the patient’s medical records death certificates, registration offices, and the Clinical Cancer Registry of Mackay Memorial Hospital. The TNM classification of the American Joint Committee on Cancer (eighth edition) was used for clinicopathological staging. 31
Statistical Analysis
Data are presented as the mean ± standard deviation of the mean. General linear model analyses were used to examine the effects of clinicopathological variables, either categories or continuous variables, and logistic regression models were utilized for adjusted comparisons of independent effects analysis. Follow-up time was the interval between the date of surgery and the event or last contact. OS was the duration from the time of first diagnosis to death or the last date of follow-up. DFS was the time from random assignment to cancer recurrence or death from any cause. Receiver operating characteristic (ROC) curve analysis using the Youden Index was conducted to determine the optimal diameter and number cut-off points for dividing PNI cases into binary variables. The highest Youden Index indicated the cut point that balances sensitivity and specificity, which was then used for regression model classification. 32 The Kaplan–Meier method was used to establish survival curves, and the log-rank test was employed to evaluate the statistical significance of differences. A Cox proportional hazards model was used to test independent significance in survival analysis. Only significant variables in the univariate analyses were selected for the multivariate regression models. The proportional hazards assumption for the Cox model was tested using Schoenfeld residuals. Multicollinearity in the logistic regression models was assessed using variance inflation factors, and the linearity of logit for continuous variables was verified through graphical methods. The Statistical Package for Social Sciences software (SPSS for Windows version 26.0; IBM Corp., Armonk, NY, USA) was used for all statistical analyses. All statistics were 2-sided, and a P-value of <.05 was considered statistically significant.
Results
Characterization of the Patients
The study population comprised 926 cases of OSCC. The majority of patients were male (90.1%), including 834 males and 92 females, with a median age of 54.6 years (range: 24-86 years). All included patients underwent resection of the primary lesion to negative margins based on clinical and radiologic examination. The predominant tumor localizations were in the buccal region (38.8%) and tongue (24.7%). Most tumors were late staged as pT3-4 (66.2%); however, 282 (30.4%) patients had already presented with cervical lymph node metastasis during tumor resection (Table 1).
Clinical Characteristic of OSCC Patients.
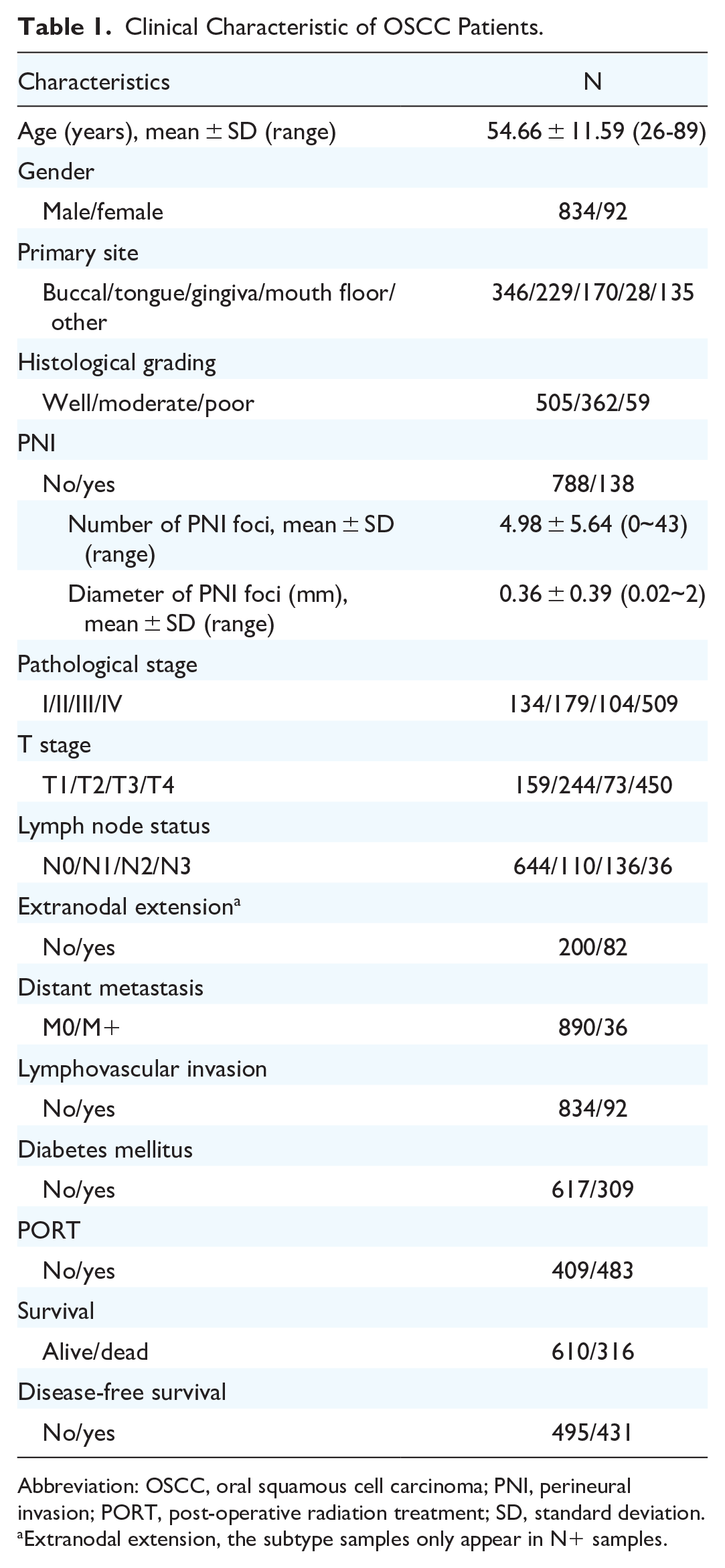
Abbreviation: OSCC, oral squamous cell carcinoma; PNI, perineural invasion; PORT, post-operative radiation treatment; SD, standard deviation.
Extranodal extension, the subtype samples only appear in N+ samples.
Correlation of Histological Subcategories of PNI with Clinicopathological Parameters
PNI was identified in 138 (14.9% of the total) patients. Its presence demonstrated significant associations with various clinicohistopathologic features, including tumor site (specifically the tongue), advanced pathological T and N categories, and LVI (Table 2). Logic regression analysis revealed increased odd ratios for these parameters except the N stage.
Characteristics of Patients with OSCC in Relation to Perineural Invasion (n = 926).

Abbreviations: CI, confidence interval; OR, odds ratio; OSCC, oral squamous cell carcinoma.
Adjust by above univariate significant factors.
Statistically significant (P < .05).
Impact of PNI on Survival in All Patients
Follow-up information was accessible for 926 patients, with a median follow-up of 9.6 years. The OS rates were 52.9% at 9.6 years and 68.1% among patients with and those without PNI, respectively (Table 3). Moreover, A Cox regression model analysis indicated PNI was recognized as an independent prognostic indicator of OS, with a hazard ratio (HR) of 2.19. Upon adjustment for other clinical variables, HR shifted to 1.37, indicating that even after adjustment, PNI remained a significant independent OS predictor. As anticipated, older age, positive nodal status (pN+), advanced pathological stages, LVI, diabetes mellitus (DM), extranodal extension (ENE), and distant metastasis were all significantly associated with poorer OS. PNI, older age, pN+, DM, LVI, ENE, and distant metastasis continued to be independent statistical associations for OS, with adjusted HRs, after adjustment for clinical factors (Table 3). Additionally, PNI was associated with DFS, and it remained an independent statistical association for DFS even after adjustment, with an HR of 1.46. Positive nodal metastasis, poor differentiation, LVI, DM, ENE, advanced stage, and distant metastasis were independent statistical associations significantly associated with poor DFS, even after adjustment (Table 3). The Kaplan–Meier method was used to investigate the correlation between OS and DFS and PNI, revealing that PNI was associated with unfavorable clinical outcomes (Supplemental Figure 1).
Univariate and Multivariate Analysis of Overall Survival and Disease-Free Survival in OSCC Patients (n = 926).

Abbreviations: CI, confidence interval; HR, hazard ratio; OSCC, oral squamous cell carcinoma.
Statistically significant (P < .05).
Adjust by above univariate significant factors.
Extranodal extension adjust by above univariate significant factors.
PNI Numbers and Diameter as Potential Survival Markers
In 138 patients with OSCC, the number of PNI foci ranges from 1 to 43, with an average of 4.9 foci. ROC curve analysis with the Youden Index was conducted to determine the optimal cut-off values for predicting OS based on the number and diameter of nerves involved in PNI. The cut-off values determined were 4 for the number of invaded nerves in PNI [area under the curve (AUC): 0.621; P = .014] and 0.21 mm for the diameter of invaded nerves in PNI (AUC: 0.607; P = .03) (Supplemental Figure 2). The linear regression model revealed an association between the number of invaded nerves and nerve diameter (Supplemental Figure 3).
Various primary tumor sites, late tumor stage and ENE were significantly correlated with the number of PNI foci (Table 4 and Supplemental Table 1). Only tumor stage was significantly associated with PNI nerve diameter (Table 4).
Characteristics of Patients with Perineural Invasion OSCC in Relation to Perineural Invasion Subcategory (n = 138).

Abbreviations: CI, confidence interval; OR, odds ratio; OSCC, oral squamous cell carcinoma.
Adjust by above univariate significant factors.
Extranodal extension adjust by above univariate significant factors.
Statistically significant (P < .05).
Logic regression analysis was calculated to identify the association between tumor location on the tongue, larger tumor size, and ENE in patients with more PNI foci (Table 4). Additionally, odds ratios were computed to assess the association between late tumor stage and patients with an increased diameter of PNI foci (Table 4). These factors retained statistical significance after adjustment for clinical parameters.
Impact of Subcategory Perineural Invasion on the Survival of Patients with OSCC
Escalation in both the number and diameter of PNI foci was associated with OS and DFS. After adjusting for clinical parameters, a PNI foci number exceeding 4 emerged as an independent statistical associations for OS, with an adjusted HR of 2.04. Similarly, a diameter of >0.21 mm was identified as an independent statistical associations for OS, with an adjusted HR of 1.94. As anticipated, the PNI foci number persisted as an independent prognostic factor for DFS after adjusting for clinical parameters, and the diameter exhibited significance as an independent statistical associations for DFS (Table 5). Intriguingly, PNI foci invaded nerves of ≤4 and maximum diameter of ≤0.21 mm the involved nerve demonstrated no significant changes compared with cases with no PNI after adjusted by other parameters. This indicates that the effect of PNI on clinical outcomes may not be pronounced or detectable below these thresholds.
Univariate and Multivariate Analysis Overall Survival and Disease-Free Survival in Perineural Invasion Subcategory OSCC Patients (n = 926).

Abbreviations: CI, confidence interval; HR, hazard ratio; OSCC, oral squamous cell carcinoma.
Statistically significant (P < .05).
Adjust by Table 3 univariate significant factors.
The Kaplan–Meier method was used to investigate the correlation between OS and DFS with the number and diameter of PNI foci. An increase in both the number and diameter of PNI foci was strongly associated with poorer clinical outcomes (Figure 1).

(A, C, and E) Kaplan–Meier analysis for overall survival according to quality and involved diameter of nerve in OSCC patients. (B, D, and F) Kaplan–Meier analysis of disease-free survival in OSCC patients. P-values were calculated by the log-rank test. OSCC, oral squamous cell carcinoma.
Impact of Postoperative Radiotherapy on PNI in OSCC
In patients with a small number of PNI foci (≤4) and small diameter nerves (≤0.21 mm), post-operative radiation treatment (PORT) shows no significant difference in survival outcomes (Table 6 and Supplemental Figure 4). However, for patients with greater number of PNI foci or larger diameter nerves, there is a survival benefit from receiving PORT. Specifically, these patients exhibit a significant improvement in both OS (HR: 2.14, 95% CI: 1.33-3.44, P = .002) and disease-free survival (HR: 1.64, 95% CI: 1.00-2.69, P = .048), highlighting the importance of considering nerve involvement extent in treatment planning.
Univariate and Multivariate Analysis Overall Survival and Disease-Free Survival in Perineural Invasion Subcategory OSCC Patients (n).
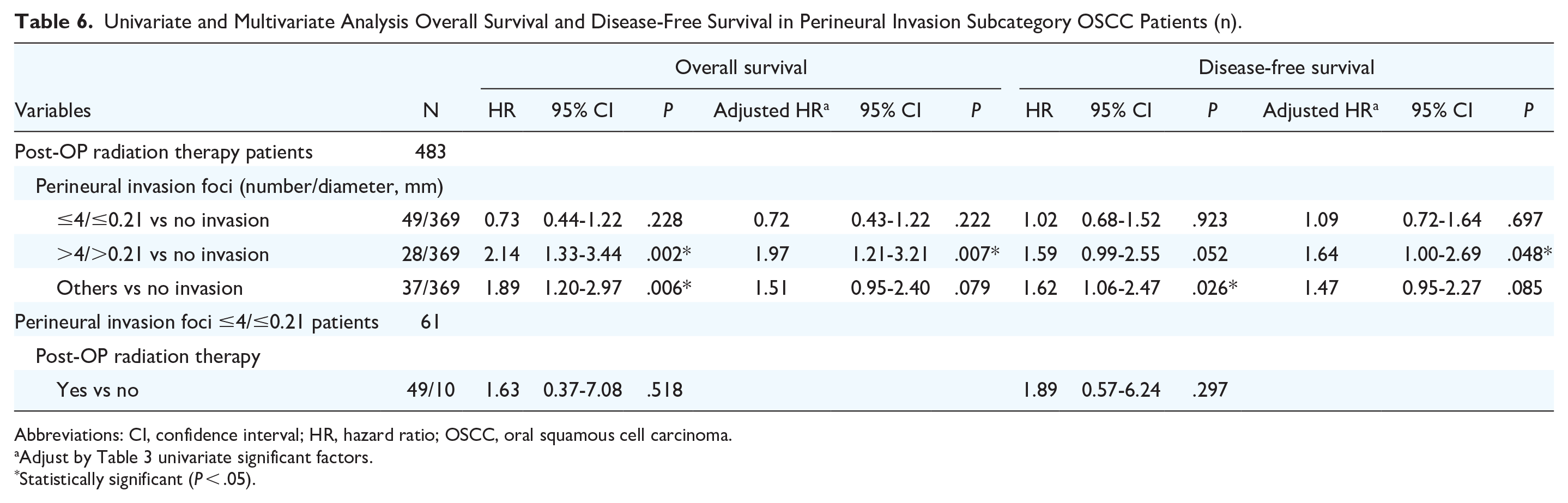
Abbreviations: CI, confidence interval; HR, hazard ratio; OSCC, oral squamous cell carcinoma.
Adjust by Table 3 univariate significant factors.
Statistically significant (P < .05).
Discussion
PNI occurs when tumor cells penetrate the perineural space, facilitated by a complex interplay among tumor cells, neural tissue, and the tumor microenvironment. 33 Various histological growth patterns have been utilized to define PNI. In this study, we tried to adopt the more strict standard for evaluation of PNI foci with the assistance of immunohistochemical studies in equivocal cases, hoping to make a reproducible and reliable results. 28 PNI isn’t merely the migration of tumor cells through a low-resistance plane; rather, it results from a reciprocal growth interaction between the nerve and tumor, allowing the tumor to spread along the nerve pathway. Hasmat et al also established a correlation between PNI and elevated T and N categories, LVI, ENE, as well as depth of invasion (DOI). 34 Tai et al and Nair et al have demonstrated similar findings, indicating that PNI is linked to higher T and N categories, as well as tumor thickness or DOI.25,35 This study on OSCC revealed significant associations between PNI and tumor occurrence site, advanced pathological T and N categories, TNM stages, and LVI. Further analysis of the quantity and size of nerve invasion was conducted. Multivariate analysis revealed that the involvement of multiple nerves compared with the single focus was associated with occurrences on the tongue, larger primary tumor size, and ENE. Moreover, a correlation was found with larger primary tumor size as the diameter of the invaded nerves increased. This study is the first to quantify the quantity and size of PNI foci in OSCC and analyze it in conjunction with histopathological factors, holding significant clinical relevance.
Nair et al demonstrated in their comprehensive study that PNI predicted decreased disease-specific survival and OS in patients with T1-T4 OSCC through multivariate analysis. 35 However, contrary to these findings, several other studies 17,18,20,36 did not observe a significant effect on survival. Our findings suggest that the discrepancies observed in the literature may arise from the inclusion of single invaded PNI, which could potentially diminish its impact on survival. The concept is reinforced by Hasmat et al 34 who conducted a recent re-evaluation of their OSCC cases. They discovered that multifocal PNI was linked to a greater risk of OS and DFS compared to DOI. However, they did not provide specific information regarding the actual number of multifocal PNI occurrences. A similar study by Wei et al 30 involved a recent reevaluation of T1-T2 OSCC cases. They categorized patients into low- and high-risk groups based on the number of PNI (≥5 foci = high risk). Their analysis revealed that the number of PNI independently predicted survival in multivariate analysis, even after adjusting for T classification, LVI, differentiation, margin status, and tumor thickness. However, noteworthy, their study included only 10 patients with OSCC whose PNI was >5. In contrast, our study includes a significantly larger number of cases, enabling a more robust statistical analysis.
A potential confounding factor regarding PNI multifocality is the possibility that 2 foci of PNI may actually represent 2 segments of 1 involved nerve bundle. This scenario means that the PNI does not genuinely involve multiple nerves, and this issue has not been addressed in previous studies. Furthermore, standardized histopathologic criteria that facilitate optimal identification of PNI involving multiple nerves are lacking. Unfortunately, routine histologic sections do not allow for the assessment of the connectivity of PNI foci. However, if a nerve bundle is involved to such an extent that it is identified in more than 1 location, it is reasonable to assume that this represents a biologically more significant form of PNI compared to a single small focus. Moreover, the distance between foci of PNI may be useful in evaluating the likelihood of such a situation. Necropsy studies of nerve propagation in SCC have indicated that linear involvement of more than 1 cm is uncommon, suggesting that PNI foci separated by more than 1 cm are likely to be truly multifocal. 37
Previous findings regarding the size of the involved nerve have shown variability. Similar to the results of this study, Brandwein-Gensler et al 5 demonstrated that involvement of nerves larger than 1 mm in size was linked to an increased risk of LF. Conversely, Fagan et al 38 did not observe an association between the diameter of the nerve involved and tumor recurrence, although they did not encounter nerve sizes greater than 0.99 mm in their cohort. While the size of the involved nerve emerged as a significant predictor of LF in univariable analysis, it did not attain statistical significance in multivariable analysis in the study by Aivazian et al 13 However, it’s important to note that the study included only 16 cases with involvement of nerves larger than 1 mm in size. Due to the limited number of events and statistical power, errors may occur. Therefore, we calculated the diameter of the involved nerves and conducted ROC analysis with Youden Index to determine the optimal cut-off point. The estimated cut-off point of 0.21 mm was utilized to evaluate OS and DFS. We found that OS and DFS were not influenced by the involvement of nerves with a small size, but when the nerve diameter exceeded 0.21 mm, both OS and DFS decreased. Our study’s findings suggest that when PNI is present, quantifying and assessing its size may assist in risk stratification and facilitate decisions regarding adjuvant therapy. This suggests the need for a scientific statistical approach to determine whether the diameter of nerve invasion affects clinical prognosis.
The presence of PNI is considered an intermediate prognostic factor, and there is debate in the literature regarding whether PNI should warrant adjuvant radiotherapy.15,18,20 Aivazian et al revealed that patients with unifocal PNI do not demonstrate an increased risk of recurrence or disease-specific mortality in the absence of PORT. 13 These results need to be interpreted with caution, but they raise the possibility of safety in withholding PORT in patients with unifocal PNI as the only indication for adjuvant therapy. Our study revealed that the prognosis is similar to that of patients without PNI if the nerve diameter of PNI is 0.21 mm, and the number of affected nerves is 4. Therefore, recording the size and quantity of nerves affected when PNI occurs is important in addition to documenting the presence or absence of PNI. This approach provided a more accurate assessment of the need for postoperative adjuvant therapy.
Different observers may have variations in assessing PNI in OSCC. Although board-certified oral and/or surgical pathologists generally have fair interobserver agreement when evaluating selected microscopic images of OSCC, differences still exist due to various proposed definitions of PNI.39,40 Single senior board-certified oral pathologist can provide consistent diagnostic results and a straightforward, coherent conclusion. 41 However, this approach introduces some limitations, such as subjectivity and bias, with personal experiences potentially affecting results. 42 Despite these limitations, a single pathologist ensures consistency in the diagnostic process. Nevertheless, there is a need for more widely accepted, objective, and reproducible criteria for evaluating PNI in OSCC.
Conclusions
In OSCC, PNI presents prognostic challenges. Our study elucidates multifocal PNI foci significance, indicating its association with poor outcomes. Additionally, diameter of PNI foci emerges as a crucial predictor, with larger sizes correlating with worse prognosis. These findings underscore the importance of precise PNI foci assessment for risk stratification and treatment decisions. Moreover, our study suggests reevaluating adjuvant radiotherapy strategies, considering nuanced factors like nerve size and quantity to optimize patient care and outcomes.
Supplemental Material
sj-docx-2-ohn-10.1177_19160216251316219 – Supplemental material for Perineural Invasion Unveiled: Deciphering the Prognostic Impact of Diameter and Quantity Subcategories in Oral Cancer
Supplemental material, sj-docx-2-ohn-10.1177_19160216251316219 for Perineural Invasion Unveiled: Deciphering the Prognostic Impact of Diameter and Quantity Subcategories in Oral Cancer by Hui-Wen Cheng, Li-Han Lin, Hung-Pin Lin and Chung-Ji Liu in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-pptx-1-ohn-10.1177_19160216251316219 – Supplemental material for Perineural Invasion Unveiled: Deciphering the Prognostic Impact of Diameter and Quantity Subcategories in Oral Cancer
Supplemental material, sj-pptx-1-ohn-10.1177_19160216251316219 for Perineural Invasion Unveiled: Deciphering the Prognostic Impact of Diameter and Quantity Subcategories in Oral Cancer by Hui-Wen Cheng, Li-Han Lin, Hung-Pin Lin and Chung-Ji Liu in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
None.
Consent for Publication
Not applicable.
Data Availability Statement
All data will be made available by the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This study was supported by grants from MacKay Memorial Hospital (MMH-E-108-12) and the National Science and Technology Council (NSTC), Taiwan: (110-2314-B-195-015-MY3)
Ethics Approval and Consent to Participate
This study was approved by the institutional review board of MacKay Memorial Hospital (approval numbers: 24MMHIS006e). All procedures involving human participants were in accordance with the ethical standards of the national research committee and with the 1964 Helsinki declaration and its later amendments. Consent to participate is not applicable due of the retrospective design of the study.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.