
Abstract
Objective
To compare hearing preservation outcomes between lateral wall and perimodiolar electrode arrays for cochlear implant patients.
Study Design
Retrospective cohort study.
Setting
A large Western Australian cochlear implant clinic
Methods
A total of 311 adult cochlear implant recipients (321 ears) implanted between 2017 and 2022 were included. Of these, 174 presented with postlingual hearing loss and preoperative functional low-frequency hearing. The change in low-frequency pure-tone average was assessed as the difference between preoperative to 3-, 6-, and 12-months postoperative measurements. Data were analyzed through linear mixed-effects modeling and one-way ANOVA.
Results
Preoperative low-frequency, pure-tone average was higher for those implanted with perimodiolar compared with lateral wall electrodes (P < .05). The linear mixed-effects model revealed that change in low-frequency pure-tone average at all postoperative timepoints was similar between lateral wall and perimodiolar electrodes (P > .05).
Conclusion
There were similar changes in residual postoperative hearing between all electrode types when controlling for preoperative low-frequency hearing and age implanted. These data suggest that newer, thinner perimodiolar and lateral wall electrodes could be considered for individuals with greater levels of preoperative low-frequency hearing.
Keywords
Introduction
Cochlear implants are considered the standard of care for treatment of severe-to-profound sensorineural hearing loss.1,2 The purpose of a cochlear implant is to provide improved access to sound, thus improving hearing outcomes that, in-turn, can improve quality of life. 1 Cochlear implants can also improve speech outcomes (in quiet and noise), which are strong indicators of real-world hearing experience. 3 As cochlear implant candidates typically have little to no hearing in the higher frequencies, every attempt is made to preserve the remaining hearing in the lower frequencies after cochlear implantation. 4 These attempts are made, as individuals with preserved low-frequency hearing post implantation have the potential to achieve better sound quality, music perception, and speech outcomes than those with no preserved hearing.5,6 Furthermore, evidence indicates that lateral wall (LW) electrodes can improve hearing preservation when compared to perimodiolar (PM) electrodes.7,8 Therefore, it has been routinely recommended to implant LW electrode arrays where there is substantial residual preoperative hearing and PM electrodes where there is limited residual preoperative hearing. 9 However, recent research with newer electrode models indicates that low-frequency hearing preservation may be achieved with both LW and PM electrode arrays.10,11 This is likely due to enhanced surgical techniques, as well as improvements in electrode array design and flexibility that have led to improved hearing preservation outcomes regardless of array type.12,13
The 2 abovementioned designs for cochlear implant electrode arrays can be defined as LW, which are positioned along the LW of the scala tympani; and PM, which are designed to be either adjacent to the modiolus or in a mid-scala position within the scala tympani.14,15 Typically, LW electrodes demonstrate a lower incidence of scalar translocation and tip fold-over and are associated with better hearing preservation outcomes than PM arrays.10,16-18 However, more recent slim PM array designs are thinner and surgically inserted with a sheath-based surgical approach (as opposed to stylet), which reduces damage to internal structures within the cochlea. 19 Because of this, newer PM models are believed to reduce the incidence of traumatic insertion; improve modiolar proximity; improve hearing preservation; and produce better speech perception when compared with an older PM model.18-22 Moreover, PM arrays have been designed to provide more localized stimulation of auditory neurons, reduced power consumption, and less channel interaction.9,10,23 Recent studies comparing LW and PM arrays, produced by a single manufacturer, showed contradictory findings for preservation of residual hearing.11,24 Thus, further comparisons of hearing preservation outcomes between different electrode array designs will provide the much-needed insight.
To add further complexity, electrode designs of the various manufacturers differ significantly in length, diameter, flexibility, and number of active electrodes (between 12 and 22).11,24 Given the various benefits and limitations of each electrode style, it can be difficult for surgeons and clinicians to identify which electrode type will provide the best patient outcomes.
Therefore, the aim of the current study was to compare hearing preservation outcomes between LW and PM electrode arrays commercially available in Australia since 2017. We hypothesized that the change in low-frequency hearing would be significantly less for LW electrode arrays.
Methods
Participants
This study was a retrospective analysis of clinical data collected from individuals implanted between January 2017 and April 2022 from a large Western Australian cochlear implant clinic. Ethics approval was granted by the University of Western Australia (2021/ET000265). Data were collected from 311 cochlear implant recipients, 10 of which had an implant in both ears, resulting in a total of 321 ears. Surgery was carried out by 10 cochlear implant surgeons using similar but not identical protocols; surgery consisted of a transmastoid facial recess with round window or extended round window approaches. Implanted devices consisted of cochlear implant electrode arrays manufactured by either Cochlear Ltd. or Med-El. Based on the electrode design, the various electrode models were divided into 3 groups: LW(c), consisting of CI522 (n = 8) or CI622 (n = 27) devices; PM, consisting of CI532 (n = 81) or CI632 (n = 113) devices; and LW(m), consisting of Synchrony Flex 24 (n = 18), 26 (n = 15), 28 (n = 47), Synchrony2 Flex 24 (n = 4), 26 (n = 3), 28 (n = 1), Synchrony Medium (n = 1), or Synchrony Soft (n = 3) devices.
Hearing Frequency
Retrospective data from routine clinical pure-tone audiometry were collected at 4 timepoints (preoperatively, 3-, 6-, 12-months postoperatively) using the standard 10 down, 5 up threshold-seeking procedure (modified Hughson Westlake procedure), 25 performed in a sound-treated booth using TD39 headphones. Air conduction thresholds were obtained at all octave frequencies between 250 to 8000 Hz, with interoctave frequencies measured where the difference between adjacent octave frequencies was 20 dB or greater. Narrow-band noise was used to mask the better hearing ear where interaural attenuation levels were 40 dB or more. While bone conduction was obtained, they were not included in the analysis. Where no response was recorded at maximum levels, the hearing threshold recorded was 5 dB above the nonresponse level (115 dB hearing level; HL at 250 and 8000 Hz; 125 dB HL for all other frequencies). Low-frequency, pure-tone average (LFPTA) was calculated from the average of hearing threshold levels at 250 and 500 Hz. Functional low-frequency hearing was classified as a preoperative LFPTA of ≤80 dB HL. 26 Change in LFPTA was used as the primary outcome measure. This was determined as the difference between preoperative LFPTA and the LFPTA at each postoperative timepoint. If an audiogram was not recorded at a particular timepoint and was preceded by an audiogram indicating no measurable hearing, then the maximal score for low-frequency hearing (115 dB HL at 250 and 8000 Hz; 125 dB HL for all other frequencies) was imputed at all subsequent timepoints.
Hearing preservation was calculated using the method proposed by Skarzynski et al 27 :

Recipients were then categorized into 1 of 4 groups based on the classification system for hearing preservation: Complete ≥75%, Partial = 25% to 75%, Minimal = 0% to 25%, and Loss of Hearing = No measurable hearing.
Statistical Analysis
One-way between-subjects ANOVAs were used to compare hearing preservation and change in LFPTA between groups at each timepoint. Subsequently, linear mixed-effects models were used to compare the change in LFPTA over time between electrode types. A random intercept was included (participant ID); timepoint and electrode type were included as predictors, and age at implant and pre-op LFPTA were included as covariates in all models. An additional model was used to assess if variability in electrode length within the LW(m) group influenced LFPTA. A mixed-design ANOVA was used to identify the main effects and interactions, then the estimated marginal means were used for follow-up pairwise comparisons. An alpha level of <.05 was used to indicate statistical significance. Linear mixed-effects models were used as they are robust for longitudinal data and account for baseline differences and missing data.28-30 To further support linear mixed-effects model analyses, additional repeated-measures ANOVAs across all timepoints, and each timepoint separately, were conducted for LFPTA outcomes through matching pairs based off pre-op LFPTA and age at implant between electrode types from the same surgeon. Analyses were conducted using R V4.2.2 (RStudio, PBC, Boston, MA).
Results
Out of a total of 311 individuals (321 ears), there were 174 males and 137 females, 161 implanted in the left ear and 160 implanted in the right ear, and 25 were prelingually deaf. Mean age at implant was 67.3 ± 13.7 years. Pure-tone thresholds (250, 500, 1000, 2000, 4000 Hz) for the entire cohort across all timepoints are shown in Figure 1. Cochlear implant recipients with only preoperative data (ie, no 3-, 6- or 12-month data), and those who did not have functional low-frequency hearing preoperatively were excluded from the analysis of LFPTA, leaving a total of 171 individuals (174 ears).
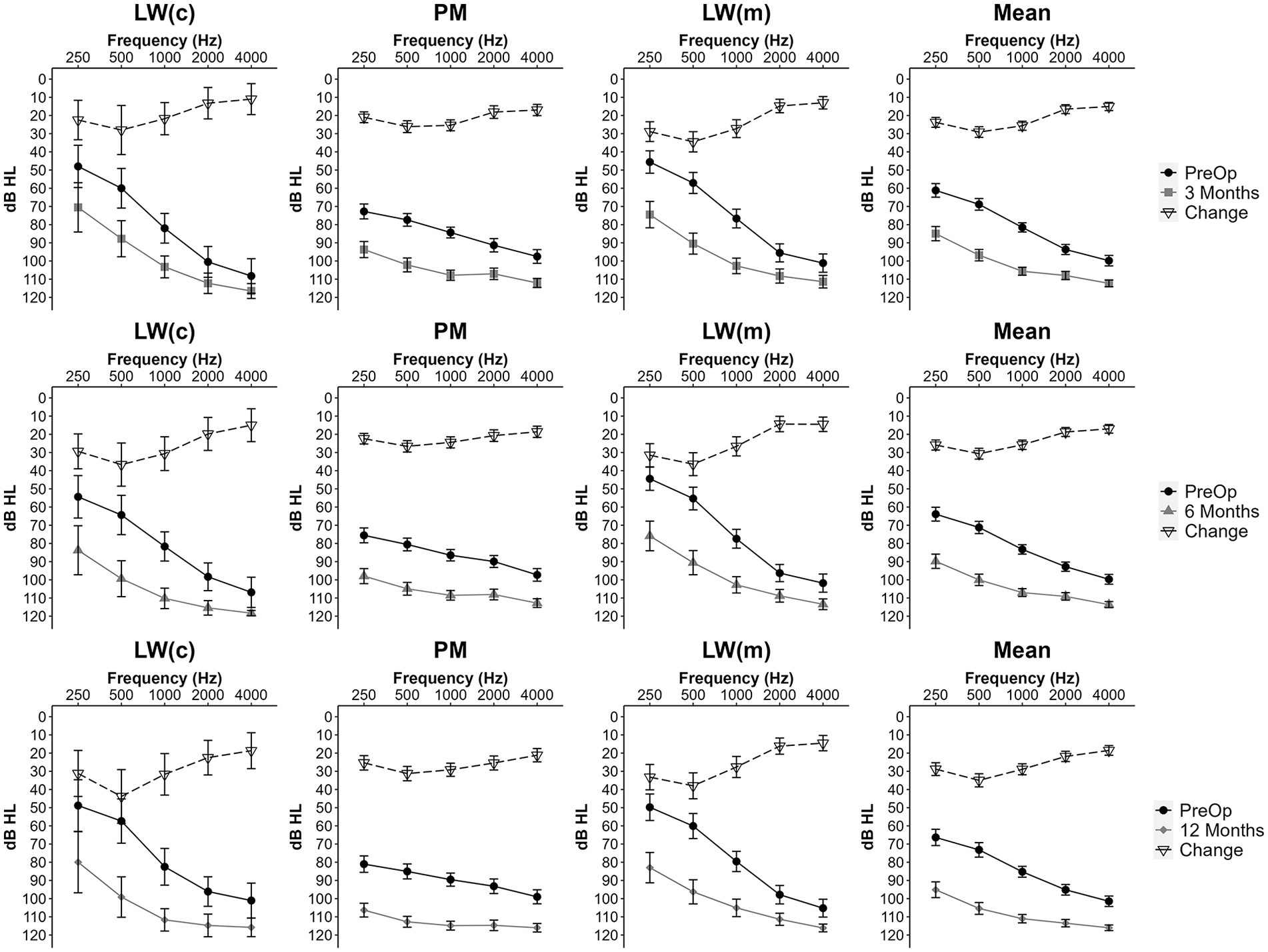
Pure-tone thresholds (mean ± 95% CI) for the entire cohort (n = 321) at Pre-Op (•), 3 months (■), 6 months (▲), and 12 months (♦), along with the change from preoperative values (▽). PM, perimodiolar; LW(m), lateral wall (MED-EL); LW(c), lateral wall (cochlear).
Preoperative LFPTA was lower (indicating better/more residual hearing) for LW(c) and LW(m) compared with PM (P < .05) (Table 1). The one-way between-subjects ANOVAs revealed that, at all postoperative timepoints, mean LFPTA was higher (poorer hearing) in the PM group compared with the LW(m) group (P < .05). However, when the change in LFPTA, rather than overall mean, was compared between preoperative values and all postoperative timepoints, the degree of change was similar between LW(c), LW(m), and PM (P > .05) (Table 1). Age at implant was also similar between all 3 electrode types (P < .05) (Table 1).
Comparison of Raw LFPTA and Change in LFPTA Between PM, LW(c), and LW(m). Individuals Included Were Postlingually Deaf with FLFH (≤80 dB HL) Preoperatively.

Data represented as mean ± SD.
Abbreviations: FLFH, functional low-frequency hearing; LFPTA, low-frequency pure-tone average; LW(c), lateral wall (cochlear); LW(m), lateral wall (MED-EL); PM, perimodiolar.
Indicates significantly different to PM (P < .05).
The linear mixed-effects model indicated that the degree of change in LFPTA increased over time in LW(c), LW(m), and PM (P < .05). That is, over time, all electrode designs showed an increasing drop in hearing. Additionally, older age at implant and lower (ie, better) preoperative LFPTA were associated with greater change in LFPTA (P < .05) (Table 2). The mixed-design ANOVA revealed a main effect of time (P < .05), but not electrode type (P > .05); however, there was a significant interaction between time and electrode type (P < .05) (Table 3). Nevertheless, posthoc comparisons did not reveal any differences for predicted change in LFPTA between LW(c), PM, and LW(m) electrodes at any timepoint (P > .05) (Figure 2). Within-group posthoc comparisons over time indicated an increase in change in LFPTA between 3- to 6-months (P < .05) and 6- to 12-months (P < .05) for PM, but not LW(c) or LW(m). Electrode length did not significantly impact change in LFPTA within the LW(m) group (P > .05) (Supplemental Material 1).
Linear Mixed-Effects Model Evaluating the Effect of Electrode Type [Lateral Wall (Cochlear) = Reference Variable, PM, LW(m)] on Low-Frequency Hearing (LFPTA) at Each Timepoint (3-, 6-, 12-Months Postop). Preop LFPTA and Age at Implant were Included as Fixed Effects, Participant ID was Included as a Random Effect.

Abbreviations: CI, confidence interval; LFPTA, low-frequency pure-tone average; LW(m), lateral wall (MED-EL); PM, perimodiolar; β: Beta weight (estimate).
Main Effects for Measurement Time (Time), Electrode Manufacturer/Type (Type), Preop LFPTA, and Age at Implant from the Mixed-Design ANOVA on Change in LFPTA.

Abbreviation: LFPTA, low-frequency pure-tone average.

Change in low-frequency pure-tone average (LFPTA) for each group at 3-, 6-, and 12-months postoperation based on the estimated marginal means from the linear mixed-effects model. Data represented as predicted score (95% CI). PM, perimodiolar; LW(m), lateral wall (MED-EL); LW(c), lateral wall (cochlear).
Hearing preservation at 3-months [LW(c): 58.2 ± 32.8%; LW(m): 54.9 ± 26.6%; PM: 49.1 ± 28.6%], 6-months [LW(c): 50.3 ± 32.1%; LW(m): 53.7 ± 28.4%; PM: 46.5 ± 29.5%], and 12-months [LW(c): 43.1 ± 30.3%; LW(m): 48.6 ± 30.5%; PM: 37.4 ± 28.7%] was similar between groups (P > .05). Proportions of recipients within each category of hearing preservation (complete, partial, minimal, loss of hearing) are shown in Table 4.
Hearing Preservation Group Frequencies (%) at Each Timepoint for Recipients with PM, LW(c), and LW(m) (Complete = >75%, Partial = >25%-75%, Minimal = 0%-25%, Loss of Hearing = No measurable hearing).

Abbreviations: LW(c), lateral wall (cochlear); LW(m), lateral wall (MED-EL); PM, perimodiolar.
Discussion
This study showed that, despite having poorer low-frequency hearing preoperatively, those who received a PM electrode array had similar changes in LFPTA at all timepoints postoperatively compared to those receiving LW electrode arrays. These results do not support our hypothesis that there would be less change in low-frequency hearing with LW electrodes.
Previous studies have noted better preoperative hearing in individuals implanted with LW electrodes,3,6,9,31,32 supporting a common clinical practice of implanting LW electrodes in patients with greater residual hearing. However, research suggests PM and LW electrodes are both necessary, as each type suits certain individuals depending on the characteristics of their hearing loss and their hearing goals. 9 Those with severe-to-profound hearing loss (or “traditional” cochlear implant candidates) are believed to benefit most from PM electrodes as they provide optimal electrical stimulation, but with less residual hearing to lose at implanation. 9 Conversely, LW electrodes are seen as more beneficial to those with functional residual hearing, since they are less traumatic to the fine inner-ear structures; thus, preserving residual hearing more effectively and retaining the option of electric-acoustic stimulation. 9 The practice of preferentially implanting LW electrodes in individuals with significant levels of residual hearing is demonstrated in the current study, as those implanted with LW(c) and LW(m) electrodes had significantly better LFPTA preoperatively than the PM group. However, change in LFPTA postoperatively was similar between groups across all timepoints for our cohort, suggesting that PM and LW electrodes result in similar postoperative changes to LFPTA regardless of preoperative LFPTA. This is further supported by our hearing preservation results (calculated via the method proposed by Skarzynski et al 27 ), as no differences were observed between groups at any postoperative timepoint. This supports the notion that 1 electrode type does not show superior hearing preservation over the other.10,11
In the current study, hearing preservation at 3-months (49%-58%), 6-months (47%-50%), and 12-months (37%-43%) for both LW(c) and PM electrodes were slightly better than a recent study utilizing the same electrodes (3-month: ~45%, 6-month: ~37.5%, 12-month: ~37.5%). 10 Furthermore, 3-, 6-, and 12-month hearing preservation rates (percentage of those with some degree of preserved hearing) for LW(m), LW(c) and PM were 70%, 67%, and 51%, respectively. These are lower hearing preservation rates than the 84% and 93% observed when analyzing those implanted with Synchrony Flex 28/Soft and Synchrony 24 electrodes in a systematic review. 33 However, in the current study, 23% of those implanted with a LW(m) had complete hearing preservation 12-months postoperatively (Table 4), which is lower than the 39% seen in those implanted with a Synchrony Flex 24 electrode in the systematic review, but similar to the 24% observed in those implanted with a Synchrony Flex 28 electrode. 33 Regarding LFPTA, the comparable average change in postoperative LFPTA between PM and LW electrodes over the 12-month testing period has been reported previously (~25-35 dB change).10,11 However, some studies have noted larger changes at 12-months (~45-50 dB)24,31 and smaller changes at 6-months (~14 dB). 21 For example, Ludwig et al 24 noted less change in LFPTA for individuals with LW (~15-30 dB) compared with PM (~40-50 dB) electrodes across the same timepoints. Conversely, Holder et al 21 noted less change in LFPTA 6-months postoperatively for individuals with PM (11 dB) compared with LW (18 dB).
Across these aforementioned studies, age at implant varies greatly from an average of 32-35 years, 10 to 51 years, 24 to 67-70 years,11,21,31 with average age in the current study (mean age 66 years) being similar to that of the latter cited studies. This suggests that variations in outcomes occur regardless of the age a recipient is implanted. This is further supported in the current study, as change in LFPTA was similar at 3-, 6-, and 12-months when controlling for age at implant and preop LFPTA (Figure 2). Furthermore, the definition of functional low-frequency hearing in the inclusion criteria is relatively similar across all studies (current study included) (≤80-85 dB at 125-500 Hz).10,11,21,24,31 Differences in LFPTA outcomes may, therefore, be related to surgical methods, such as technique (round window, extended round window, cochleostomy) 4 ; angular depth of insertion34,35; speed of insertion 36 ; use of corticosteroids 36 ; or surgical experience with a particular electrode type. 12 However, these data are unavailable in the current study. Another potential cause for varied results between electrode types is the design of recent PM models. Older PM electrodes have a thicker electrode array and are more likely to cause trauma, as the increased stiffness of the electrodes tip increases the likelihood of scalar translocation.37,38 The thinner, more flexible design of LW arrays may partly explain why better hearing preservation with LW electrodes has been seen previously. 31 Furthermore, thinner LW electrodes designed for hearing preservation have shown a greater likelihood of preserving hearing in both the short- and long-term when compared with older PM models from different manufacturers. 39 Currently, newer, thinner, more flexible PM models demonstrate similar short- and long-term hearing preservation when compared with LW models from the same manufacturer.10,11,13 Therefore, improvements in surgical protocols and PM electrode model design may explain why similar changes in residual hearing from pre- to postoperatively are being reported between electrode types in recent research.
Limitations
This study has several limitations. First, the lack of access to surgical factors that may influence data meant that this could not be included in the analysis. Inclusion of surgical outcomes/procedures within a regression model has shown to improve model fit (increase R 2 ) in hearing preservation outcomes,4,40 and different surgical outcomes have been shown to influence results depending on the electrode type. 41 Furthermore, PM electrodes have shown a higher incidence of tip fold-over compared with LW electrodes, 17 which can subsequently result in poorer hearing outcomes. However, newer, slim PM models have indicated reduced tip fold-over incidence compared with older models.18,20 Second, surgeon experience and preference with each type of electrode were unaccounted for; this may have led to potential bias in both selection of, and proficiency in, surgical insertion of the different electrode arrays, as surgeons have noted preferences toward a particular electrode type, 42 which could impact hearing preservation results. Third, the preference in our cohort to use LW(m) and LW(c) electrodes in individuals with better residual hearing may have resulted in overrepresentation of particular hearing loss mechanisms more prone to poorer outcomes (eg, some forms of genetic hearing loss). Fourth, variations in electrode length within the LW(m) group may have influenced hearing preservation results; however, the separate analysis of electrode length we conducted within the LW(m) found no differences in hearing preservation outcomes (Supplemental Material 1). Lastly, this study did not utilize a randomized design with matched groups, which would provide stronger evidence to support the conclusions made.
Conclusion
For this cohort, PM and LW electrodes preserved hearing to a similar extent, despite those with LW electrodes having significantly better preoperative low-frequency hearing. These data suggest that the use of newer, thinner PM electrodes could be considered regardless of the level of residual low-frequency hearing. In addition, the use of newer, thinner electrode designs (LW or PM) could be considered for individuals with greater levels of residual low-frequency hearing.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216251316217 – Supplemental material for The Effect of Cochlear Implant Electrode Array Type on Hearing Preservation
Supplemental material, sj-docx-1-ohn-10.1177_19160216251316217 for The Effect of Cochlear Implant Electrode Array Type on Hearing Preservation by Matthew Zimmermann and Cathy Sucher in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
The authors would like to acknowledge the clinicians from the Ear Science implant clinic involved in collection of the retrospective clinical data collated for this article (Ronel Chester-Browne, Elle Statham, Steffanie Cohen, Courtney McMahen, Jerimiah Soo, Liz Clarke) and research assistant Denise Howting for their contribution to the data organization process. Additionally, we would like to acknowledge Marcus Atlas, Rob Eikelboom, Ronel Chester-Browne, and Paul Mcllhiney for their assistance in the review of the article.
Author Contributions
M.Z.: data organization and analysis, writing of the manuscript, review and editing of manuscript. C.S.: study design, implementation and data collection, editing of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Internal funding from the Ear Science Institute Australia.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.