
Abstract
Background
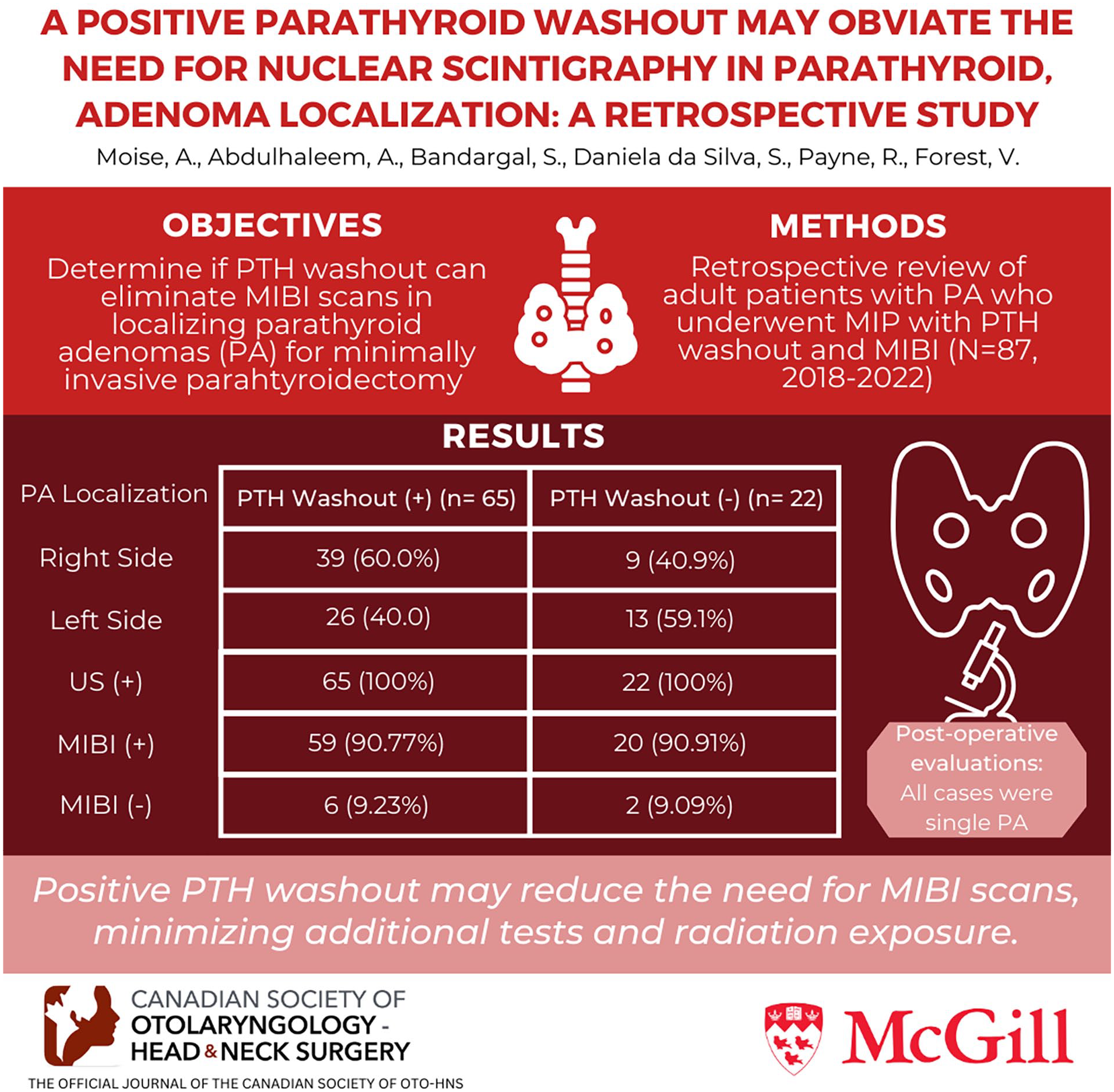
Minimally invasive parathyroidectomy (MIP) in patients with a parathyroid adenoma (PA) requires imaging modalities for precise localization. Parathyroid hormone assay on ultrasound-guided fine-needle aspiration washout, or PTH washout, can be used for this purpose. It is unclear whether PTH washout complements traditional PA localization techniques such as a sestamibi (MIBI) scan or diminishes its need. This study aims to determine whether a positive PTH washout obviates the need for an MIBI scan in the preoperative localization of a PA.
Method
A multi-center retrospective, comparative review comprised adult patients who underwent MIP at 2 McGill University teaching hospitals between 2018 and 2022. Patients who had both PTH washout and MIBI scan for preoperative localization of PA, final histopathology reports available, and preoperative/postoperative results recorded were included in the final analysis.
Results
Of the 193 patients’ charts reviewed, 87 were included in this study. Of these 87 patients, 74.7% (65/87) had a positive PTH washout result. Among those, MIBI correctly detected 90.8% (59/65) of the PAs. The MIBI scan did not contribute meaningful information for any of the 65 patients who had positive PTH washout results.
Conclusion
These findings strongly support the use of preoperative dedicated ultrasound as the initial standard procedure. When a PA candidate on ultrasound is found, a PTH washout should be performed. If positive, it could suffice as the sole localization method for MIP surgery. When a PA was identified on ultrasound and confirmed with PTH washout, the MIBI scan did not add more information. Benefits include fewer patient tests, less exposure to ionizing radiation, and reduced healthcare expenses.
Keywords
Introduction
Parathyroid adenoma (PA) is the most common cause of primary hyperparathyroidism. 1 Typically, it is diagnosed through laboratory testing and clinical symptoms, and localized by imaging prior to surgical resection. Previously, bilateral neck exploration was the gold standard to localize parathyroid adenoma in primary hyperparathyroidism but advances in radiology made minimally invasive parathyroidectomy (MIP), the procedure of choice in patients with a PA, reducing operation time and complications. 2
The success of an MIP is dependent upon the precision of imaging modalities necessary for PA localization. Various imaging modalities are available for the identification of PA including technetium 99m sestamibi scintigraphy (MIBI), ultrasound (US), contrast-enhanced computed tomography (CT), magnetic resonance imaging (MRI), four-dimensional parathyroid CT (4D-CT), and more recently, 18 -fuorocholine PET/CT and 11 C-choline PET/CT. In rare cases where imaging is equivocal or fails to localize the parathyroid adenoma, venous sampling can be used. All of these modalities have their respective sensitivity and specificity and advantages and disadvantages which can vary significantly. Moreover, considerations such as the local expertise, availability, and costs effectiveness associated with these methods could influence the clinician’ choice of the optimal imaging strategy.3-6
Current guidelines recommend the use of at least 2 modalities for a precise preoperative localization of a PA.7,8 MIBI and US are considered first-line imaging modalities.9,10 MIBI is the most widely used imaging modality for accurate localization of PA, due to its high sensitivity and specificity. When technetium-99-sestamibi scanning is paired with SPECT (single photon emission computed tomography), it has the highest positive predictive value among the imaging techniques. Notwithstanding these significant strengths, MIBI also has some disadvantages, including the patient’s exposure to ionizing radiation and its higher cost compared to US. US is a widely available, noninvasive, and inexpensive adenoma localizing procedure, but localization of the adenoma is very dependent on the experience of the ultrasonographer. It can be indeed highly sensitive in experienced hands and US can provide high-resolution anatomical details of PA without radiation exposure.11,12
A preferred approach among traditional techniques for many institutions involves utilizing MIBI and US as complementary imaging studies providing highly reliable results in preoperative localization of PA.7,12,13 However, due to several factors such as the presence of concomitant thyroid disease and small parathyroid adenoma size, discordant findings between these 2 imaging studies can occur. In these cases, additional ancillary tests, such as MRI, CT, and 4D-CT, may be needed to achieve a precise preoperative localization of the PAs. 11 4 D-MRI and 4D-CT are newer imaging modalities that have shown to be more sensitive than US and MIBI, particularly, when they show discordant, equivocal, or negative results.14-16
As mentioned, most of these ancillary tests are resource-intensive and costly, most involve radiation exposure, and may not always be easily accessible in all areas or institutions.12,14,16 In this context, parathyroid hormone assay on a US-guided fine-needle aspiration washout, also known as PTH washout, emerged as a valuable, simple, accessible, quick additional procedure without radiation exposure for preoperative localization of PA, especially in patients with a suspected parathyroid adenoma detected on US.17-22
Although there are a few studies that have investigated, documented, and reported the benefits of using this US-guided procedure (PTH washout) as a PA localization method in a clinical setting, it is unclear whether PTH washout is an adjunct or an alternative for the conventional imaging modalities such as MIBI scan.20-22 This study aims to determine whether a positive US-PTH washout obviates the need for an MIBI scan in the preoperative localization of a parathyroid adenoma and if it could be used as a first-line localization modality.
Methods
This study protocol conforms to the principles of the Declaration of Helsinki and was approved by the Medical-Bioethics Research Ethics Board of the Integrated Health and Social Services Network for West-Central, Montreal.
Study Population and Data Collection
We performed a retrospective, multi-center comparative review of PTH washout versus MIBI scan for patients who underwent PA excision at 2 McGill University teaching hospitals from January 2018 until December 2022.
This study population consisted of adult patients who had undergone MIP and had received both US-guided PTH washout and MIBI scans as part of their preoperative workup.
As stated in the Summary Statement and Guidelines from the Fifth International Workshop on Primary Hyperparathyroidism, although parathyroidectomy is an option for all patients if there are no contraindications, in this cohort common indications include hypercalcemia, osteoporosis, nephrolithiasis, reduced renal function, or younger age. 23
For patients who consented to both preoperative PTH washout and sestamibi (MIBI) scans, demographic data, imaging findings, PTH assay results, as well as preoperative and postoperative serum levels, pathological outcomes, and follow-up information were reviewed and included in the statistical analysis.
The localizations of parathyroid adenomas were divided into right superior, right inferior, left superior, and left inferior. Serum levels of PTH and corrected calcium were collected, with 1 reading taken preoperatively and 3 independent postoperative readings at 1-, 6-, and 24-hour intervals after surgery.
All patients included in the study underwent preoperative workup protocol at our hospitals. Preoperative imaging prior to the PTH washout attempt included neck US performed by radiologists or 1 of the 2 endocrine surgeons and an MIBI scan performed by nuclear medicine specialists. A US was always performed before the PTH washout. However, given the retrospective nature of the study, the timing of the MIBI scan varied (pre- or post-PTH washout) depending on several factors. PTH washout procedure was done under US guidance for all cases by 2 experienced ENT surgeons who specialized in thyroid and parathyroid surgeries and trained in thyroid US as well as US-guided fine-needle aspiration biopsy.
PTH Washout Procedure
Parathyroid hormone assay on a US-guided fine-needle aspiration washout (PTH washout) of the suspected adenoma was performed using a 10-mL standard syringe with a sterile 21-gauge needle under real-time US scan (LOGIG P9 from General Electric, 12 MHz frequency, linear probe 12L SMP).
Prior to proceeding, the neck skin was cleaned with either chlorhexidine or isopropyl alcohol swabs and marked, and then local anesthesia was performed with 1 cc of xylocaine 1% with epinephrine.
After needle insertion, negative pressure was quickly applied with a back-and-forth oscillation into the targeted mass with 2 or 3 passes. The needle was then rinsed into 1 cc isotonic saline solution that had been poured into the appropriate blood test tube for PTH levels. The blood test tube containing the solution of the PTH washout was immediately sent to the laboratory for PTH level measurement.
The cutoff value for defining a positive PTH washout following a US-guided fine-needle aspiration of a suspected PA lesion was established based on our institutional experience. Patients with a PTH level greater than 400 pmol/L were classified as PTH washout positive, those with a PTH washout level less than 100 pmol/L were defined as PTH washout negative, and the values in between were considered as intermediate PTH washout. The cutoff for PTH levels in washout samples went beyond the most stringent criteria in the literature, being at least 3 times the level of the serum PTH and greater than 400 pmol/L. Each of our patients with positive PTH washout results satisfied both essential criteria: their PTH washout values were above 400 and at least 3 times higher than their serum values. Setting a high cutoff value in the PTH washout test likely minimized the occurrence of false positives ensuring that positive results are highly indicative of true PA presence. On the other hand, such stringent thresholds could also decrease the test’s sensitivity by missing true positive cases with lower PTH levels.
Statistical Analysis
Data were presented as number percentage (%) for the categorical variables, while the continuous variables were expressed as mean ± standard deviation (±SD) or median range (min-max). For frequency analysis in contingency tables, statistical analyses of associations between variables were performed using the chi-square test or Fisher’s exact test (with significance set at P < .05). For continuous variables, the nonparametric Mann–Whitney U test was used. Statistical analyses were performed using STATA® (STATA Corp., College Station, TX, USA).
Results
Of 193 adult patients who underwent MIP during the study period, 87 consented to have preoperative PTH washout in addition to an MIBI scan. Preoperative workup was performed in all cases in our institutions. All patients were successfully operated on, and pathological evaluation of the surgical specimen confirmed that all cases (100%) were single parathyroid adenomas. None of the patients in our sample were found to have any additional adenomas on MIBI. Theoretically, identifying a parathyroid adenoma candidate with US could miss a second adenoma, but this has not been a scenario that we have encountered in our series. According to follow-up evaluations conducted post-treatment, no patient required additional surgical intervention for the subsequent identification of a double adenoma.
Study Group
The baseline demographical and lesion characteristics of our study group are summarized in Table 1. Of the 87 patients, 69 (79.31%) were females and 18 were males (20.69%). The median age of the patients was 61.6 years (range 25-89 years). The mean preoperative serum PTH level was 167.15 pg/mL, while postoperative first and second readings were 45.01 and 36.73 pg/mL, respectively. According to the histopathology reports, the right inferior and the left inferior sites were identified as the most frequent locations for a PA, comprising 44.83% (39/87) and 32.18% (28/87) of cases. The left superior and right superior sites accounted for 12.64% (11/87) and 10.34% (9/87) of occurrences. The size of suspected PA in US was smaller than 1 cm for 62.06% (54/87) of patients, between 1 and 1.5 cm, and superior to 1.5 cm in 21.84% and 16.09% of instances.
Baseline Demographical and Lesion Characteristics of the Study Group.

Categorical variables are presented as number percentage (%) and continuous variables as mean ± standard deviation (±SD).
Abbreviations: LT-Inf, left inferior; LT-Sup, left superior; PA, parathyroid adenoma; PTH, parathyroid hormone; RT-Inf, right inferior; RT-Sup, right superior; US, ultrasound.
PTH Washout Groups—Positive Versus Negative
PTH washout was negative and did not identify the PA in 22 (25.3%) cases. It was positive and identified the PA in 65 (74.7%) patients. Table 2 provides a comparison of baseline characteristics between patients exhibiting positive and negative results in PTH washout tests. The analysis of demographics and other lesion characteristics revealed no statistically significant differences between the groups, with all P-values exceeding .05. Notably, the size of PA approached statistical significance with a P-value of .074, suggesting a trend where smaller adenomas (<1 cm) were more likely to yield negative PTH washout results. This finding is coherent, as it is technically more challenging to accurately target very small lesions located deep in the thyroid using fine-needle aspiration, compared to larger lesions. It is important to consider that the relatively small sample of lesions analyzed in the present study may have attenuated the statistical power of our test, and with a larger sample, the results could potentially achieve statistical significance. There was no correlation between PTH washout concentrations and serum PTH and serum calcium levels. Of the 87 lesions suspected in US, MIBI had localized 59/65 (90.8%) in the positive group and 20/22 (90.9%) in the negative group.
Comparison Between PTH Washout Positive and Negative Groups.
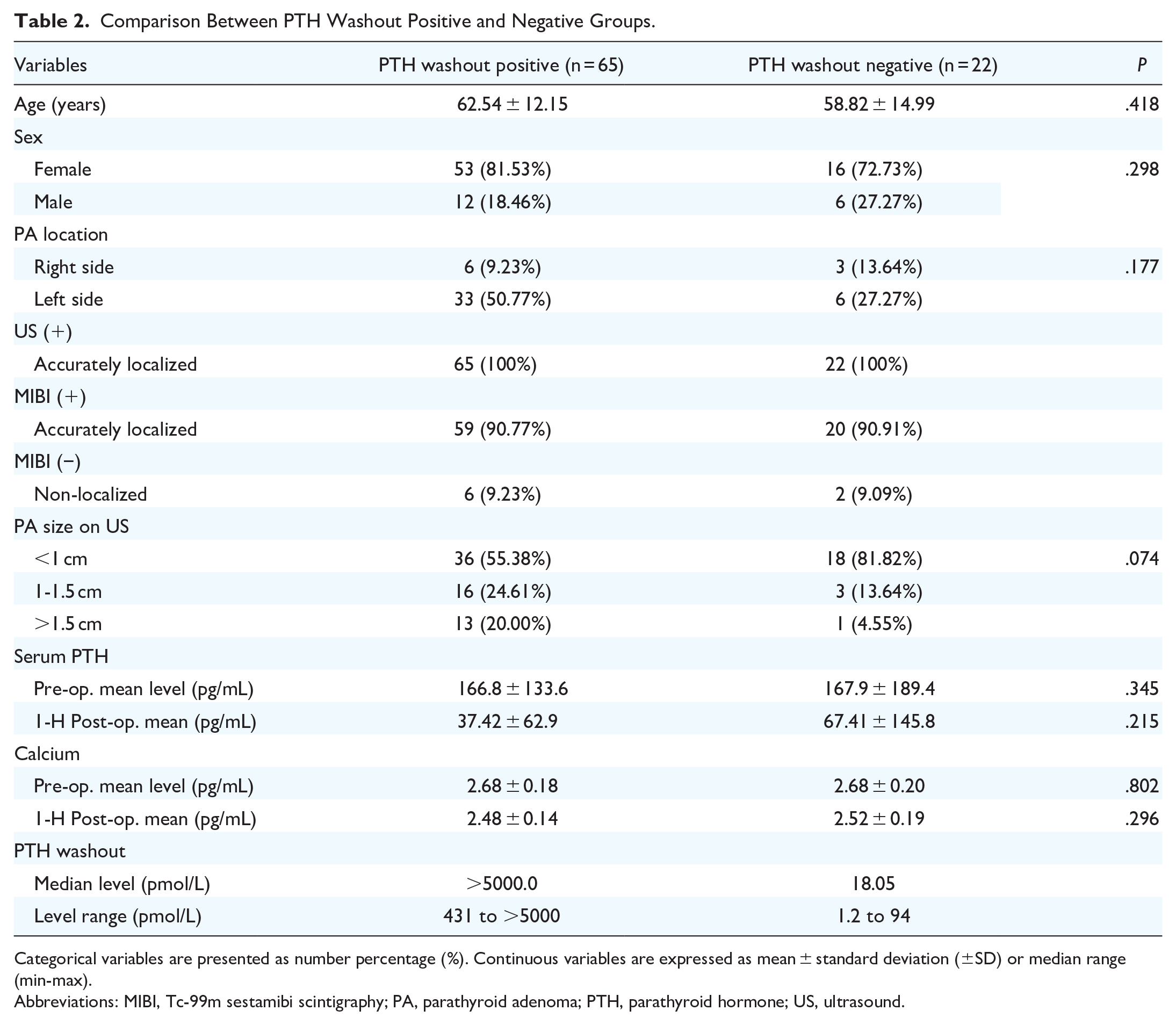
Categorical variables are presented as number percentage (%). Continuous variables are expressed as mean ± standard deviation (±SD) or median range (min-max).
Abbreviations: MIBI, Tc-99m sestamibi scintigraphy; PA, parathyroid adenoma; PTH, parathyroid hormone; US, ultrasound.
PA Localization in Positive PTH Washout Group
PTH washout levels of the aspirate samples were markedly elevated (>5000 pmol/L) in 92.3% (12/13) of lesions bigger than 1.5 cm, 81.3% (13/16) of the lesions between 1 and 1.5 cm, and 77.8% (28/36) of the lesions smaller than 1 cm (Figure 1).

PA size and PTH washout result in a positive group (n = 65). PTH washout results exceed 5000 pmol/L (in blue) in parathyroid lesions measuring less than 1 cm in size, 1 to 1.5 cm, and more than 1.5 cm, respectively. Parathyroid adenomas were suspected on ultrasound with PTH washout levels of the aspirate samples 400 to 5000 pmol/L (in orange).
A substantial decrease of 50% or more in serum PTH level, measured preoperatively and at 1-, 6, 24-hour, and 5-day intervals postoperatively, was present in 89.2 (58/65), 93.9% (61/65), 98.5% (64/65), and 100% (65/65) of cases, respectively (Figure 2). We found that when a lesion was identified as a PA candidate on US, a positive PTH washout test result was proven to be highly effective, detecting, and confirming appropriate localization of true parathyroid tissue in all 65 (100%) cases. Figure 3 illustrates these results in comparison with those of the MIBI scan. It is important to consider that the PTH washout performance may have been enhanced by preliminary imaging that identified potential parathyroid adenoma. This initial identification not only selected optimal candidates for the procedure but also aided surgeons in navigating more effectively. On the other hand, the combination of a US helping to localize and a PTH washout confirming the parathyroid adenoma could provide the 2 preoperative localizing modalities needed to assist in MIP.

Decrease in serum PTH levels ≥50% in a positive group (n = 65). Mean serum PTH levels (in blue) were measured preoperatively and postoperatively at 1-, 6-, 24-hour, and 5-day intervals, with the respective number of patients (in orange) for which a substantial decrease of 50% or more was present.

PA localization: MIBI scan versus US-PTH washout in positive group (n = 65). Comparison between MIBI and US + PTH washout localization: accurate PA localization (in green), non-localizing PA (in red).
In the positive PTH washout group, MIBI localized the PA in 90.77% (59/65) of the patients (Figure 3). The remaining 6/65 (9.23%) cases for which MIBI had a negative result but a positive PTH washout of a candidate lesion found on US, were mainly located on the right side (66.7%; 4/6) and smaller than 1 cm (66.7%; 4/6) in size. In the 6/65 (9.23%) instances where MIBI failed to localize a candidate lesion, the presence of a PTH washout level of greater than 5000 pmol/L of a suspected PA in US was a reliable indicator of a PA. This is significant as they were corroborated with an appropriate decrease in postoperative serum PTH. Notably, out of all of the patients who had positive PTH washout results, none (0/65) had an MIBI scan that showed a double adenoma or contributed meaningful information in guiding clinical management. Identification of true parathyroid lesions in the positive PTH washout group, MIBI showed a sensitivity of 90.77% (Figure 3).
Discussion
MIP in patients with a parathyroid adenoma is dependent on the precision of imaging modalities used in the localization of the adenoma. The primary objective of our study was to investigate whether a US-guided positive PTH washout could avoid the need for an MIBI scan in the preoperative localization of PA. To the best of our knowledge, this paper is among the first to address this question.
The majority of studies examining the efficacy of PTH washout as a localization technique have primarily emphasized its ancillary role with an MIBI scan.19-22 However, a limited number of comparative studies have documented their institutional experience to evaluate the viability of this method as the preferred approach. Notably, various studies have proposed distinct positive cutoff values for PTH washout, all contributing to correct PA localization.18-22,24-30 Kiblud et al reported a sensitivity of 70% for a positive PTH washout of 1000 pg/mL, while Gokcay et al found a sensitivity of 90% for a value of 436.5 pg/mL.20-22,24-27 Certain investigations that accepted a positive cutoff value greater than 45 pg/mL or a PTH washout/serum PTH ratio above 1 had a higher sensitivity of up to 95%.19-22
In our study, patients exhibiting a PTH washout level exceeding 400 pmol/L (3772 pg/mL) and a PTH washout value 3 times the serum levels were categorized as having a positive PTH washout, exceeding the cutoff values outlined in existing literature. This preoperative localization of a PA with an elevated PTH washout level allows our specialists to promptly assess the characteristics of the suspicious lesion and identify patients who would benefit from an MIP. This targeted approach ensures timely surgical intervention for confirmed PA cases.
Nonetheless, a predominant preference among nuclear medicine physicians and surgeons involves the utilization of multiple imaging modalities to enhance preoperative localization accuracy. Certain studies have suggested that the size and volume of the parathyroid lesion can influence sestamibi uptake and the likelihood of achieving a positive PTH washout result. It has been documented that smaller candidate lesions are more challenging to localize.19,20,31 Conversely, Gokçay et al reported that the success of the procedure is independent of lesion size and more closely linked to the operator’s expertise and experience. 20 In our study population, we did not observe any correlation between tumor size or serum PTH and the PTH levels. Although there was a difference between positive and negative groups in the percentage of lesions smaller than 1 cm, this correlation did not reach statistical significance. This could be attributed to 2 main factors. First, the relatively small sample size of lesions analyzed might have limited the probability of statistical significance in our results. Second, the high level of proficiency of experienced surgeons coupled with the standardized biopsy protocol they employed, potentially reduced variability and impacted the statistical outcomes.
By contrast, there appears to be a relationship between the size of the parathyroid adenoma and the effectiveness of the MIBI scan in localizing parathyroid lesions in patients with a positive PTH washout result. These MIBI results align with findings from other studies, which have reported sensitivity of 68% to 90%, depending on the protocol (ie, combined or not with SPECT), and a negative rate of 12% to 25% for suspected lesions smaller than 1.5 cm. Furthermore, some investigations have noted lower sensitivity and accuracy for MIBI when compared to PTH washout.18-22,28-30 In our cohort of 87 patients, the sensitivity of PTH washout was found to be 74.7%, compared to 90.8% for MIBI scans. Importantly, 100% of PTH washout-positive lesions were proven to be true-positive parathyroid tissue, confirmed by final pathology after surgery. It is noteworthy that in 75% of the cases where MIBI results were negative, PTH washout successfully detected parathyroid lesions. In addition, no false positives with PTH washouts were recorded in our study.
Our results show that a positive PTH washout result of a PA candidate on US is a reliable localizing modality and it could potentially suffice as the sole localization method for MIP. A prospective study is underway to evaluate this approach. This would obviate the need for these patients to undergo the MIBI procedure and consequently avoid exposure to ionizing radiation. Studies have suggested that a single-positive imaging modality may be a sufficient indication for surgeons performing focused or MIP. 29 Moreover, the US PTH washout is safe and quick and can be an office-based procedure that does not cause parathyromatosis or has no major complications.12,19,22,28,32,33 When performed by experienced endocrine surgeons or specialists, it is an extremely valuable tool for parathyroid localization in simple and more complex cases.20,28 In this study population, the experience and the standardized protocol used are likely contributing factors to the absence of procedure-related complications.
The benefits of this approach extend beyond its clinical advantages, as it also provides cost-effective solutions to address challenges such as limited accessibility to imaging platforms and specialized expertise needed for conducting and interpreting imaging studies, as well as sparing higher costs on healthcare systems and ionizing radiation exposure for the patient.12,34 Although PTH washout is considered to be cost-effective, this paper does not aim to quantify the savings (financial, resources, and time) that may result if an imaging procedure such as MIBI scan can be avoided for most patients candidate for MIP. 35 However, further studies with a greater number of cases in whom a PA was detected and confirmed by a positive PTH washout test are needed to get conclusive proof of the range of these savings. In the context of increasingly constrained healthcare, we believe that the PTH washout procedure represents a cheaper and viable alternative.
Our study has some limitations. It is a retrospective study. While our study provides valuable information regarding the performance of PTH washout, prospective studies are requisite to validate its clinical utility. Our study harbors geographic selection bias as the McGill University teaching hospitals are located in the urban city of Montreal, Canada. Our establishments may not accurately represent the reality of many other non-quaternary hospitals and community care centers. An important limitation of our study is the potential source of positive bias arising from the pre-selection of patients with localized adenomas identified through imaging, who were then candidates for targeted PTH washout procedures. Due to the existing imaging workup, it was not feasible to avoid or accurately assess this inherent bias. It is important to mention that all patients included in our study had a single adenoma detected in US (either done by a radiologist or by endocrine surgeons trained in US and US-guided biopsy), which was confirmed by US-guided PTH washout. Considering the high pretest probability of a single adenoma, these patients could potentially be candidates for successful MIP even without MIBI imaging. It should be noted that none of the patients in our sample were found to have any additional adenomas on MIBI. While, in theory, US may fail to detect a second adenoma, this was not observed in our series. Given the demonstrated reliability of PTH washout as a confirmatory tool, there is a compelling case for revisiting and potentially revising these standard indications to reduce reliance on MIBI, thereby optimizing diagnostic protocols in a cost-effective and resource-efficient manner. Lastly, we did not use the Perrier classification for PA localization due to the inconsistent availability of US data retrospectively. This limitation may affect the precision in describing the anatomical location of parathyroid adenomas, which is valuable for surgical planning. The use of real-time US imaging combined with the surgical team’s expertise allowed for reliable localization, reducing the necessity for a formal classification system like Perrier in this context.
Conclusion
Our findings support the use of preoperative dedicated US as the initial standard procedure as it provides quick information on a candidate lesion. When a parathyroid adenoma is suspected in US, a PTH washout test may be carried out, and if positive, maybe eventually it could be considered as the second localizing modality for surgeons performing MIP. While sestamibi scans and other imaging modalities continue to have their place, in specific circumstances, their use may be minimized. When a single parathyroid lesion was identified in US and confirmed with PTH washout, the MIBI scan did not seem to be necessary as it did not contribute additional information for performing. This streamlined approach can reduce the need for further diagnostic tests, limit patient exposure to ionizing radiation, and decrease healthcare costs without compromising the success of the surgical intervention.
Footnotes
Author Contributions
Conceptualization: AM, MA, RP, and VF (lead); Collection of data: AM; Analysis: AM, SDS, RP, and VF; Writing – original draft preparation: AM; Writing – review and editing: AM, MA, SB, SDS, RP, and VF (lead). All authors participated in revising the manuscript as well as for final approval of the version to be submitted for publication.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Research Ethics Board (REB) of the integrated Health and Social Services Network for West-Central, Montreal (#MP-2023-3584).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.