
Abstract
Importance
Chronic rhinosinusitis (CRS) significantly impacts patients’ quality of life and incurs substantial healthcare costs. Understanding pathogen trends before, during, and after the COVID-19 pandemic can inform better management and treatment strategies.
Objective
To identify the common pathogens associated with CRS and compare them across pre-pandemic, during-pandemic, and post-pandemic periods.
Design
Retrospective chart review.
Setting
McGill University Health Centre, Montreal, Canada.
Participants
Around 147 patients were 18 years and older, diagnosed with CRS, underwent endoscopic sinus surgery within the specified timeframe (January 2017 to September 2023), and whose charts contained relevant microbiology information. Patients were categorized into 3 groups based on surgery dates: pre- (January 2018 to November 2019), during- (January 2020 to December 2021), and post-pandemic (February 2022 to September 2023).
Main Outcome Measures
Distribution and prevalence of pathogens associated with CRS across the 3 time periods. Microbiology results from nasal cultures were analyzed to identify predominant pathogens.
Results
Among the 147 patients, 46 distinct organisms were identified. Staphylococcus aureus was the most prevalent pathogen, increasing during the COVID-19 period (24.7%) compared to pre-pandemic (17.9%) and post-pandemic (21.5%) periods. Significant increases during the COVID-19 period were noted for Aspergillus fumigatus (6.8%, P < .001), Enterobacter cloacae (6.8%, P = .01), and Cutibacterium acnes (6.8%, P = .03). Post-pandemic, significant rises were observed in Serratia marcescens (P < .001) and Achromobacter denitrificans (P = .03).
Conclusions and Relevance
Significant shifts in CRS-associated pathogens occurred during the COVID-19 pandemic. Notable changes in the prevalence of S. aureus, A. fumigatus, E. cloacae, and C. acnes were observed during the pandemic, with increases in S. marcescens and A. denitrificans post-pandemic. These findings suggest that the pandemic’s impact on healthcare practices and environmental factors influenced the microbial etiologies of CRS. Future research may explore the mechanisms driving these changes and their long-term implications for CRS management.

Introduction
Chronic rhinosinusitis (CRS) stands out as one of the most prevalent chronic conditions globally, boasting a prevalence rate of around 12.3% in the United States alone. This condition significantly diminishes the quality of life for those it afflicts, exerting a substantial impact on both the social functioning of the affected individuals and broader economic implications due to the associated disease burden. 1 The direct healthcare costs linked to the consumption of resources for CRS are estimated to be around USD 10 to 13 billion per year. Moreover, the toll of absenteeism and productivity loss exceeds USD 20 billion annually, compounding the economic impact of CRS. CRS, in particular, incurs elevated indirect costs compared to other chronic diseases, primarily because it predominantly affects individuals in their productive years, typically ranging from 30 to 50 years old. 2 Postoperative success in this patient population has been defined to include both objective findings, such as healthy mucosa, lack of edema and purulent discharge, patency of cavities and ostia, and adequate mucus drainage, as well as patient-reported outcomes, such as improvement in symptoms and quality of life. 3 Studies have shown that patients with CRS have significantly lower rates of depressive symptoms and risk of depression after undergoing treatment. 4 In addition, studies have found that overall, patients with CRS who have a greater wait time before undergoing surgery tend to have a lower quality of life and increased healthcare costs and prescription utilization. 5 Considering the substantial impact that CRS has on affected individuals, the landscape of CRS treatment is being studied to enhance the predictability of its success. For example, biomarker models can be used to improve the allocation of biologic therapy for patients with IgE-high type 2 CRS to minimize costs and unnecessary treatments. 6 For all CRS subtypes in general, a better understanding of underlying infectious causes would enable quicker and more reliable diagnoses. This, in turn, would optimize care and quality of life while minimizing the functional and financial burden of the disease in this patient population. 4
Over the past 3 years, amid the COVID-19 pandemic, there has been rapid and extensive progress in knowledge and development in the field of immunology. We have acquired deeper insights into the function, adaptability, and capabilities of our immune system. The substantial increase in public sanitary measures and mask-wearing has brought about notable changes in the incidence and etiology of other infectious diseases globally, particularly respiratory infections. Global sanitary measures rapidly reduced influenza virus activity by 98% from March to May 2020, with peak season positive test rates dropping from 30% to 3%. Confirmed RSV cases fell by 99.6% during the 2020 to 2021 winter, but after sanitary measures were lifted in 2021, respiratory syncytial virus (RSV) infections and hospital admissions surged past pre-pandemic levels. Similar increases were seen with rhinoviruses, enteroviruses, Streptococcus pneumoniae, and group A streptococcal infections. The resurgence of these infections after the removal of mask mandates and social distancing is suspected to stem from a lack of viral/bacterial exposure, resulting in a dearth of specific immunity during this period. 7 In South Korea, the prevalence of Acinetobacter baumannii and S. pneumoniae in respiratory samples significantly declined post-COVID-19, with Klebsiella pneumoniae rising to prominence. 8 Similarly, a Beijing study on pediatric community-acquired pneumonia revealed a decrease in Mycoplasma pneumoniae infections and an increase in viral causes post-pandemic. 9 Overall, the absence of exposure and the opportunity to develop and strengthen the immune response have created an “immunity debt,” increasing susceptibility and the severity of infection with these pathogens. 10
As demonstrated in previous studies, the epidemiology and etiologies of infectious agents have undergone significant changes during the COVID-19 pandemic. Understanding these shifts is crucial, as it can enhance diagnostic and interventional practices, leading to improved efficiency and quality of patient care. The aim of this study was to identify the current most common pathogens associated with CRS and compare them to the periods before and during the COVID-19 pandemic.
Methodology
Study Design
A retrospective chart review was conducted, assessing patients who underwent endoscopic sinus surgery for CRS between January 2017 and September 2023. The study adhered to the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (2014) and received approval from the McGill University Health Centre Research Institute and the McGill University Health Centre Research Ethics Board. Due to the study’s retrospective nature and its exemption from requiring direct patient contact, permission to access patient charts was granted by the Director of Professional Services at McGill University Health Centre (MUHC), obviating the need for individual informed consent.
Patient Recruitment
The records of patients who underwent endoscopic sinus surgery at the MUHC from January 1, 2017, to September 1, 2023, were systematically reviewed, comprising a total of 340 charts. Inclusion criteria encompassed patients aged 18 years and older diagnosed with CRS, both with and without nasal polyposis, who underwent endoscopic sinus surgery within the specified timeframe, and whose charts contained relevant information on the microbiology of rhinosinusitis. The selected cohorts that underwent endoscopic sinus surgery due to previous failed medial management were categorized based on their surgery dates: patients operated on from January 2018 to November 2019 constituted the pre-pandemic group, those from January 2020 to December 2021 comprised the during-pandemic group, and individuals treated from February 2022 to September 2023 constituted the post-pandemic group.
Data Collection
For each patient, we examined the following data: patient demographics, microbiology results obtained from nasal cultures, and the surgery date. Board-certified otolaryngologists, specializing in rhinology and skull-base surgery at the MUHC, conducted the surgeries for these patients. Culture samples from the nasal mucosa were obtained intraoperatively and subsequently analyzed by laboratory technicians at the same institution. Routine cultures are taken in our hospital system for all cases of rhinosinusitis, including both patients with and without nasal polyposis, to keep an institutional database.
Statistical Analysis
Statistical analysis was conducted using R v 4.3 (version 4.3; R Core Team 2024). The primary objective of the analysis was to assess differences in the predominant pathogens causing CRS before, during, and after the COVID-19 pandemic. Counts and percentages were employed to summarize the distribution of different organisms at various time points. Pairwise comparisons for each organism were executed using the epiR package in R, which contrasts the count of each organism between each pair of time points. The odds ratio (OR) served as a measure of effect size, and the data was normalized to represent the incidence per 100 cases. The statistical significance of the results was determined using the Fisher exact test, with hypothesis testing conducted at a 5% level of significance (α < .05).
Results
Patient Demographics
A total of 147 individuals met the inclusion criteria and were enrolled in our study, comprising 68 males (46.3%) and 79 females (53.7%). The mean age of the population was 49 years, with ages ranging from 17 to 83 years. The distribution across time periods included 56 patients in the pre-COVID-19 period, 45 patients during the COVID period, and 46 patients in the post-COVID period.
Pathogenic Distribution
Among the 147 patients with CRS, cultures identified a total of 46 different organisms. In the pre-COVID and COVID periods, 29 organisms were isolated, while 32 organisms were isolated during the post-COVID period (Figures 1 and 2). The distribution of the most common pathogens during these 3 time periods is outlined below.
Pre-COVID: Staphylococcus aureus (17.9%) > Staphylococcus epidermidis (10.7%) > Pseudomonas aeruginosa (8.3%) > Haemophilus influenzae (7.1%).
COVID: S. aureus (24.7%) > S. epidermidis (6.8%) = Enterobacter cloacae (6.8%) = Cutibacterium acnes (6.8%) = Aspergillus fumigatus (6.8%).
Post-COVID: S. aureus (21.5%) > S. epidermidis (9.2%) > P. aeruginosa (6.2%).

Descriptive statistics for the included organisms. Data normalized per 100 patients.

Total number of organisms normalized per 100 persons.
Figure 3 provides a comprehensive breakdown of the distribution of pathogens across these 3 time periods.

Pathogenic distribution throughout the (a) pre-COVID, (b) COVID, and (c) post-COVID periods.
S. aureus emerged as the most prevalent organism among patients in this study throughout all 3 time periods, with prevalence rates of 17.9%, 24.7%, and 21.5% in the pre-, during, and post-COVID periods, respectively. Following closely in the pre- and post-COVID periods was S. epidermidis, accounting for 10.7% and 9.2%, respectively. However, during the COVID period, S. epidermidis exhibited the same prevalence as E. cloacae, C. acnes, and A. fumigatus, all at 6.8%.
The prevalence of 46 organisms was compared across 3 time periods (Table 1). There was a notably higher prevalence of A. fumigatus during the COVID period compared to both the pre-COVID period (OR = 0.08, P < .001) and the post-COVID period (OR = 6.61, P = .01). Similarly, the prevalence of E. cloacae was significantly elevated during the COVID period compared to both the pre-COVID (OR = 0.17, P = .01) and post-COVID (OR = 3.14, P = .05) periods. C. acnes also exhibited significantly higher prevalence during the COVID period compared to both the pre-COVID period (OR = 0.26, P = .03) and the post-COVID period (OR = 6.61, P = .01).
Comparison of the Prevalence of the Different Organisms Between Time Points.
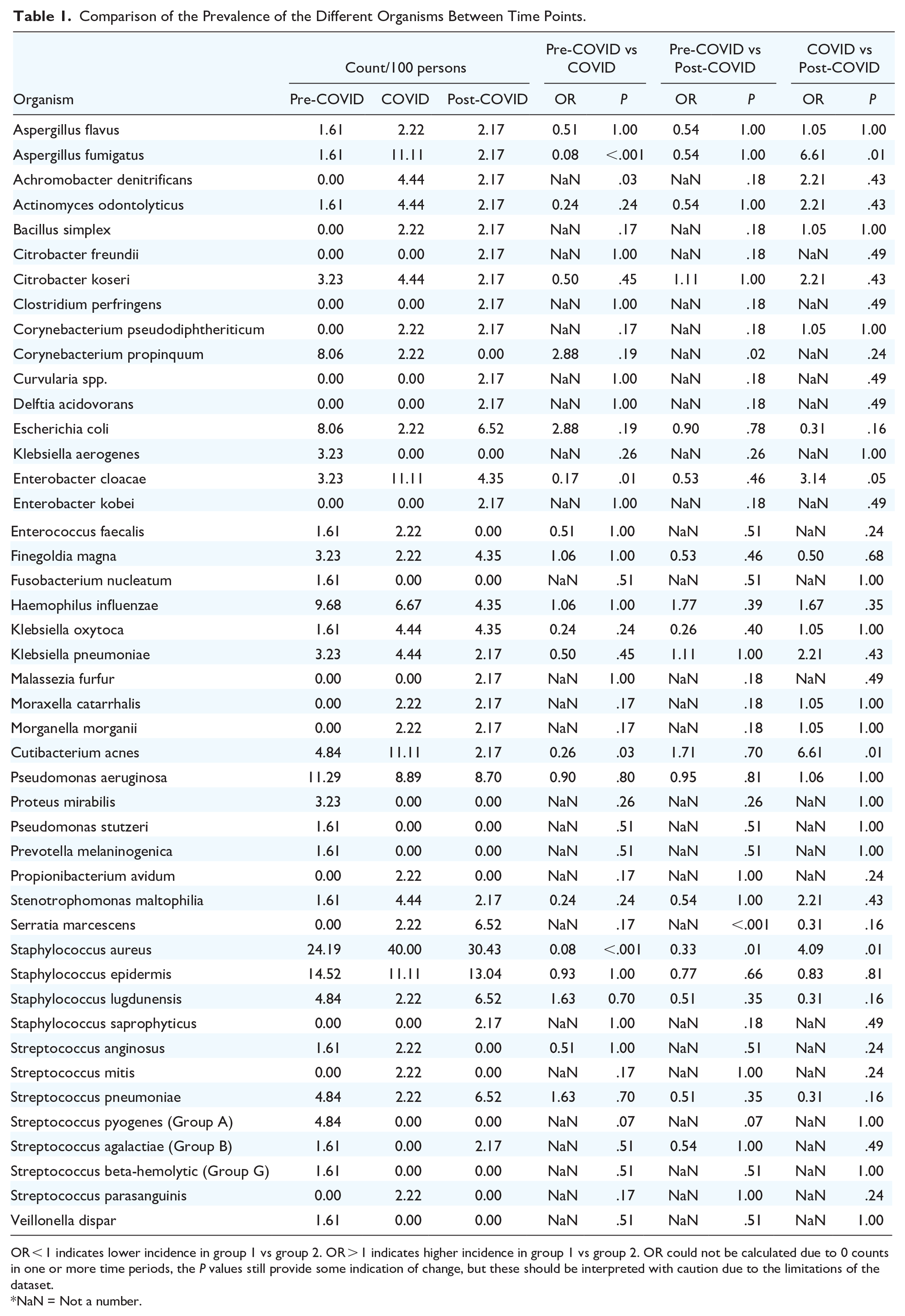
OR < 1 indicates lower incidence in group 1 vs group 2. OR > 1 indicates higher incidence in group 1 vs group 2. OR could not be calculated due to 0 counts in one or more time periods, the P values still provide some indication of change, but these should be interpreted with caution due to the limitations of the dataset.
NaN = Not a number.
A noticeable rise in Achromobacter denitrificans was observed during the COVID period compared to pre-COVID (P = .03). Similarly, Serratia marcescens exhibited a significant increase post-COVID compared to pre-COVID (P < .001). However, for both organisms, the prevalence data in the pre-COVID period is either unavailable or too low to calculate an OR.
While S. aureus remained the most prevalent pathogen throughout all 3 time periods, its overall prevalence exhibited variation, being notably higher during the COVID period compared to both the pre-COVID period (OR = 0.08, P < .001) and the post-COVID period (OR = 4.09, P = .01). Additionally, the prevalence of S. aureus was significantly greater in the post-COVID period compared to the pre-COVID period (OR = 0.33, P = .01). However, other organisms listed in Table 1 either did not show significant changes in prevalence (P ≥ .05) or lacked sufficient data to calculate the OR.
Discussion
The results of this study offer novel insights into the changing landscape of pathogens linked to CRS, especially during the COVID-19 pandemic. Our analysis unveiled substantial shifts in the prevalence of specific organisms, indicating a dynamic interplay among microbial, immunologic, and environmental factors. Notably, 6 organisms exhibited statistically significant differences in prevalence across time periods: S. aureus, A. fumigatus, E. cloacae, C. acnes, S. marcescens, and A. denitrificans.
S. aureus, a common nasal colonizer, exhibited a notable difference in prevalence during the COVID-19 period compared to both before and after, potentially linked to changes in hygiene practices and infection control. This aligns with prior research which has found a higher incidence of S. aureus bacteremia during the COVID-19 period, in particular among patients infected with the virus, suggesting a possibility of increased susceptibility to bacterial super-infections at this time as well as increased risk of nosocomial infection with more time spent in hospital environments. 11 A. fumigatus, an environmental mold, demonstrated significant variations across the studied periods, possibly influenced by environmental factors affected by lockdowns, altered indoor air quality, or changes in outdoor activities. In addition to rhinosinusitis, pulmonary aspergillosis saw a rise in patients infected with COVID-19. This may be due in part to increased admissions to the intensive care unit and use of mechanical ventilation during this period.12,13 These fluctuations extend beyond rhinosinusitis, prompting further investigation into their broader impact on respiratory health during public health crises. E. cloacae, typically a nosocomial bacterium, and C. acnes, a usual part of the skin flora, showed a significant increase during the COVID-19 period, potentially associated with heightened hospital visits and admissions, shifts in antibiotic usage, or other healthcare-related factors. This differs from a study done in Saudi Arabia, which found decreased prevalence of E. cloacae during the pandemic period of 2020 to 2021 in addition to decreased antibiotic resistance of this bacteria, 14 highlighting that different precautions and infection prevention protocols across the world may impact the pathogenic distribution. Additionally, this study identified S. marcescens and A. denitrificans as pathogens with significantly greater prevalence post-COVID compared to pre-COVID. This is in keeping with prior research that found not only increased rates of Serratia bacteremia but also increased antibiotic resistance after the COVID-19 period. 15 These findings may be linked to environmental changes, altered immune responses, or shifts in microbial competition within the sinus and nasal microbiome following the pandemic. Understanding the dynamics of underlying CRS pathogens is crucial for targeted treatment strategies, considering potential implications for disease severity and treatment response. For example, the specific microbiology underlying a particular patient’s disease may be a target for treatment in those who failed endoscopic sinus surgery and have already undergone revision surgery. This may be particularly useful in certain patient populations, such as those with immunodeficiencies, as they are less likely to have success from initial sinus surgery for CRS. 16 Future research may delve into the mechanisms driving these changes, including host factors, environmental influences, and potential long-term implications for CRS management. As well, there are many aerosol-generating procedures performed by otolaryngologists, such as endoscopic exams, sinonasal procedures, head and neck mucosal cancers, and mastoid drilling. 17 Having a better understanding of the common pathogens that colonize this patient population can assist healthcare professionals in ensuring the use of proper personal protective equipment based on the modes of transmission of these pathogens.
We acknowledge several limitations in this present study, with sample bias being a notable concern. Patient selection occurred exclusively within a single medical institution in Montreal, Canada. Given that variations in ecological, environmental, and healthcare factors contribute to the microbial landscape of a region, our reliance on patients from a singular institution may impede the generalizability of our results to a broader population. Additionally, the patients included in this study had undergone endoscopic sinus surgery. Consequently, pathogens associated with acute rhinosinusitis treated conservatively or empirically are not considered in this analysis, potentially yielding different organisms than those included in this study. As well, candidates for surgery during the COVID-19 period differed from the pre- and post-pandemic periods. Patients who tested positive for the virus had their surgeries delayed. Therefore, information on the microbiology of COVID-19-positive patients was generally not collected, and the interplay of various organisms with active SARS-CoV-2 infection is not considered in this study. 18 Furthermore, the study focused on specific time ranges before, during, and after the COVID-19 pandemic. A longitudinal analysis could provide insights into the temporal stability of these changes, assisting in determining whether these alterations are transient fluctuations or sustained shifts in pathogen prevalence.
Conclusion
In summary, our study highlights the dynamic nature of organisms and the markedly different prevalence of several pathogens associated with CRS during the COVID period compared to before and/or after, notably S. aureus, A. fumigatus, E. cloacae, and C. acnes. Additionally, S. marcescens and A. denitrificans exhibited significantly higher prevalence post-COVID compared to pre-COVID. We hypothesize the underlying cause of these differences is multifactorial, such as changes in isolation protocols and altered immune function during the pandemic. These findings are crucial for guiding diagnostic and therapeutic practices, enabling tailored approaches adapted to the current microbial landscape.
Footnotes
Consent to Participate
Due to the study’s retrospective nature and its exemption from requiring direct patient contact, permission to access patient charts was granted by the Director of Professional Services (DPS) at McGill University Health Centre (MUHC), obviating the need for individual consent.
Data Availability Statement
The datasets used and/or analyzed from the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study adhered to the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (2014) and received approval from the McGill University Health Centre Research Institute and the McGill University Health Centre Research Ethics Board on September 28th, 2023.