
Abstract
Objective
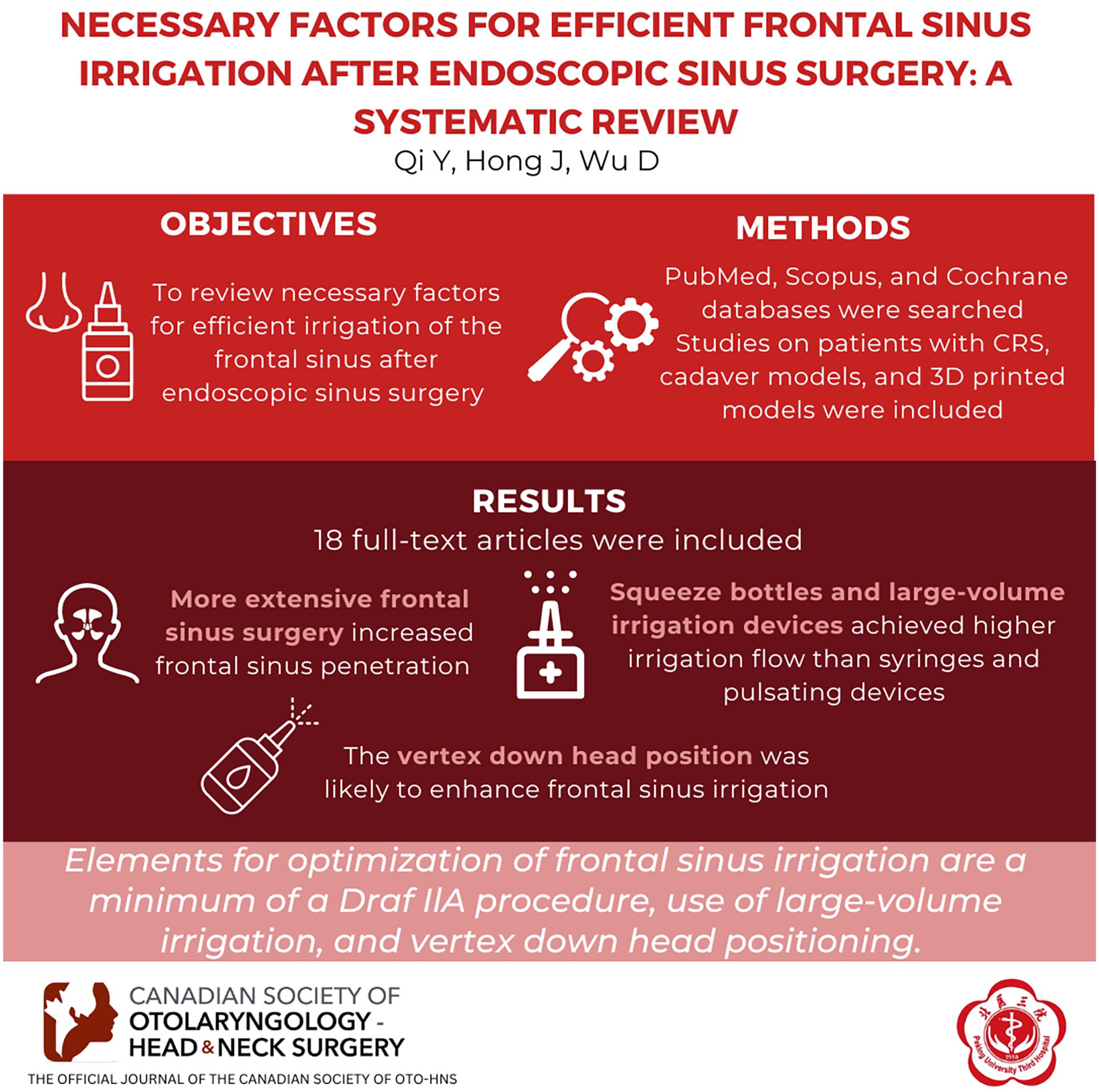
The frontal sinus remains a challenging site for irrigation due to its position relative to the nostril and ethmoid sinus. This study aims to summarize the necessary factors for efficient irrigation of the frontal sinus after endoscopic sinus surgery (ESS) among patients with chronic rhinosinusitis (CRS).
Methods
Using Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines, a systematic literature review was conducted on PubMed, Scopus, and Cochrane databases to identify studies assessing the effect of frontal sinus irrigation in patients with CRS, cadaver models, or 3D-printed models of the sinonasal cavity after ESS.
Results
Of the initial 206 abstracts reviewed, 18 full-text articles were included. The degree of the frontal sinus ostium opening after ESS was found to be associated with the efficacy of frontal sinus irrigation. More extensive frontal sinus surgeries tended to increase frontal sinus penetration. A Draf IIA procedure was identified as the minimum standard to achieve sufficient irrigation in the frontal sinus. Due to decreased backpressure in the nasal passage, increasing septectomy in Draf III did not significantly improve irrigation delivery. Squeeze bottles achieved significantly higher irrigation flow in the frontal sinus than syringes and pulsating devices. Large-volume irrigation devices provided better irrigation for the frontal sinus by entering or flushing the entire frontal sinus. The head position influenced the frontal sinus irrigation by altering the ostia position relative to fluid flow and vertical height of the frontal sinus during irrigation. While the vertex down head position was likely to enhance frontal sinus irrigation, the comfort of the head position and patient compliance should be considered.
Conclusion
Elements for optimization of frontal sinus irrigation are a minimum of a Draf IlA procedure for frontal sinus dissection, use of large-volume irrigation, and vertex down head positioning. Developing comfortable head positions with high frontal sinus irrigation efficiency would increase patient compliance and improve outcomes.
Level of Evidence:
NA.
Introduction
Chronic rhinosinusitis (CRS) is a chronic inflammatory condition of the nasal cavity and sinuses, affecting 15% of the Western population and contributing to increased healthcare costs.1,2 Endoscopic sinus surgery (ESS) is often a more effective and reliable treatment for patients with CRS who have not responded to conservative medication. The primary goal of the ESS procedure is to widen the natural outflow tract of the sinuses, thereby enhancing the contact between nasal mucosa and medications. 3 However, long-term revision rates for ESS were estimated to be as high as 14% to 24%.4,5 Sinonasal irrigation after ESS is essential to effectively treat patients with CRS in the long term.6,7 Nasal irrigation has been demonstrated to flush excess mucus secretions and debris, promoting nasal cleansing and wound healing. 8 In CRS patients treated with ESS, sinonasal irrigation reduced the sinonasal cavity’s inflammatory load by reducing eosinophil infiltration and inhibiting chemokine secretion.9,10
The frontal sinus region has a complex anatomy with critical neighboring structures, including various frontal recess chambers adjacent to the orbit and skull base, which increase the difficulty of the surgery. 11 Different surgical treatment modalities are utilized to address frontal sinus lesions, ranging from balloon dilatation to wide-open ESS techniques.12,13 The operated frontal sinus with an enlargement of the sinus ostia provides access for sufficient water flow. The effectiveness of frontal sinus irrigation may be affected by several factors. Previous studies have shown that the Draf III procedure has advantages over Draf IIA regarding irrigation for the frontal sinus.14-16 However, the optimal extent of frontal sinusotomy for efficient irrigation has not been reported. Besides, the type of irrigation device can affect irrigation efficiency through its delivery volume and intensity. Large-volume devices have been found to offer superior irrigation of the nasal cavity and sinuses compared to low-volume devices.16,17 Furthermore, head position is closely related to the efficiency of frontal sinus irrigation.16,18,19 This emerging evidence has enhanced our understanding of frontal sinus irrigation.
This study aims to conduct a systematic review of the literature, summarize the necessary factors for sufficient irrigation of the frontal sinus after ESS, and provide a theoretical basis for future clinical practice.
Materials and Methods
Literature Search Strategy
An evidence-based systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 20 The study protocol was registered in the PROSPERO database on April 10, 2024 (registration number: CRD42024530555). A comprehensive systematic literature review was performed using the PubMed, Embase, Web of Science, and Google Scholar databases from inception to June 8, 2024. To maximize the likelihood of identifying all relevant publications, a combination of keywords was used: nasal irrigation, nasal rinse, nasal douche, CRS, rhinosinusitis, chronic sinusitis, nasal polyps, polyposis, frontal sinus, and ESS.
Study Selection
Two investigators (Y.Q. and D.W.) independently reviewed the titles and abstracts of all identified studies. The included studies focused on frontal sinus irrigation after ESS in patients with CRS. Studies involving cadaveric and 3D-printed models of the sinonasal cavity post-ESS were also included. Studies without results on frontal sinus irrigation were excluded, as were case reports, letters, abstracts, meeting proceedings, and pediatric studies. Figure 1 outlines the search strategy and inclusion process used to identify relevant studies.

Article selection process for systematic literature review.
Data Extraction and Analysis
The collected data included details such as the first author, the year of publication, study design, subject, surgical procedure, nasal irrigation, assessment, results, and conclusions. We categorized the studies based on the type of research subject, including human studies, cadaver studies, and 3D-printed model studies. The summary of surgery mainly included different surgery procedures and their extents. Description of nasal irrigation encompassed the device used, volume, irrigation reagent, and head positions. Head positions were classified according to the angle of the nose relative to the vertical cranio-caudal axis. The primary outcomes were the effect of surgery, irrigation device, and head position on frontal irrigation after ESS. Following the extraction of studies, summary tables were formulated, and the quality of each article was evaluated using the categorization system provided by the Oxford Center for Evidence-Based Medicine Levels of Evidence. 21
Quality Assessment
The Methodological Index for Non-randomized Studies (MIN-ORS) was used to assess the risk of bias in the included non-randomized clinical trials. The checklist comprised a set of questions (8 for noncomparative and 12 for comparative studies) to evaluate important aspects of each study. 22 Studies were classified into 4 levels based on the total score, 0 to 4 was “very low,” 5 to 8 was “low,” 9 to 12 was “good,” and 13 to 16 was “excellent.” 23 The quality of cadaveric studies was assessed using the Quality Appraisal for Cadaveric Studies (QUACS) scale, 24 which consists of a 13-item checklist addressing the design, conduct, and report of cadaveric dissection studies. Each item was scored 0 (no/not stated) or 1 (yes/present), with points awarded only if the criteria were fully met. The overall score was expressed as a percentage, with the first quartile considered “very low,” the second “low,” the third “good,” and the fourth “excellent.” 23 The Medical Education Research Study Quality Instrument (MERSQI) was also used to assess the risk of bias in model studies, including 10 items clustered in 6 domains. 25
Results
Characteristics of Studies
A total of 206 articles were identified through the initial database search (Figure 1). After screening, 90 articles were selected for full-text review and 72 articles were excluded because they did not contain results on the effect of frontal sinus irrigation. Finally, 18 articles met the final inclusion criteria for the systematic review. Among the included studies, 3 were human studies, all of which were nonrandomized clinical trials.26-28 Eleven studies were cadaveric assessments,16-19,29-35 2 were 3D-printed model studies,36,37 and 2 were studies of computational fluid dynamics.15,38
The main features of the study are presented in Table 1. In human trials, 29 patients with CRS and 7 healthy volunteers were included. In the cadaver assessment, 86 fresh-frozen human cadaver heads were used for ESS and nasal irrigation. Six techniques were used to assess frontal sinus distribution: endoscopic, MRI, CT, nuclear medicine imaging, watering indicating paste, and computational fluid dynamics. In endoscopic assessment, 8 studies used various scales to evaluate flushing fluid entry into the sinuses during irrigation.16-19,29,32,34,35 Among these, 3 studies16,19,32 used a 4-point scale (0—nasal cavity only; 1—distribution to frontal recess; 2—distribution to medial one-half of frontal sinus; 3—distribution to lateral one-half of frontal sinus; 4—lavage) for the assessment of frontal sinus irrigation, while 1 study used a 3-point scale (0—restricted to nasal cavity; 1—distribution to frontal recess; 2—distribution to frontal sinus proper; 3—filling of entire sinus). 35 Two studies graded the staining intensity and area of irrigated sinuses using different scales, 1 on a 3-point scale (0—absent: no dye visualized; 1—minimal: only trace dye visualized on parts of mucosa; 2—moderate: dye clearly visible on most or all parts of mucosa; 3—heavy: dye heavily stained on mucosa or pooling of dye within site), 31 and the other on a 4-point scale (0—no staining; 1—light staining; 2—medium staining; 3—intense staining; 4—extreme staining). 30 A study involving a 3D-printed model utilized a responsive gel that changes color on contact with liquids on internal surfaces, allowing for a more intuitive observation of liquid distribution within the frontal sinus. 36 Two studies employed computational fluid dynamics simulation to generate video files and static images for each sinus irrigation.15,38
Frontal Sinus Irrigation in CRS After ESS.

Abbreviations: CRS, chronic rhinosinusitis; CT, computed tomography; ESS, endoscopic sinus surgery; LOE, level of evidence; MRI, magnetic resonance imaging.
Risk of Bias
Three studies were nonrandomized clinical trials, assessed by the MINORS criteria26-28 (Table 2). The overall scores of 2 comparative studies were deemed “excellent” (13-16 points),26,27 while 1 noncomparative study received a sum score at the “low” level (5-8 points). 28 Eleven cadaveric studies were assessed with the QUACS scale, with the overall quality being relatively high16-19,29-35 (Table 3). The mean QUACS score was 74.1% (range 53.8%-84.6%), with 5 studies rated as “excellent”17,18,31,32,35 and 5 studies rated as “good.”16,19,29,30,33 Two 3D-printed model studies36,37 and two computational fluid dynamics studies15,38 were assessed with the MERSQI (Table 4). The average score was 10, which was only about half of the maximum possible score of 19.5. This relatively low score may be attributed to the limited robustness of the study design and insufficient evidence of validity.
Assessment of 3 Nonrandomized Clinical Trials by Methodological Index for Non-Randomized Studies (MINORS).
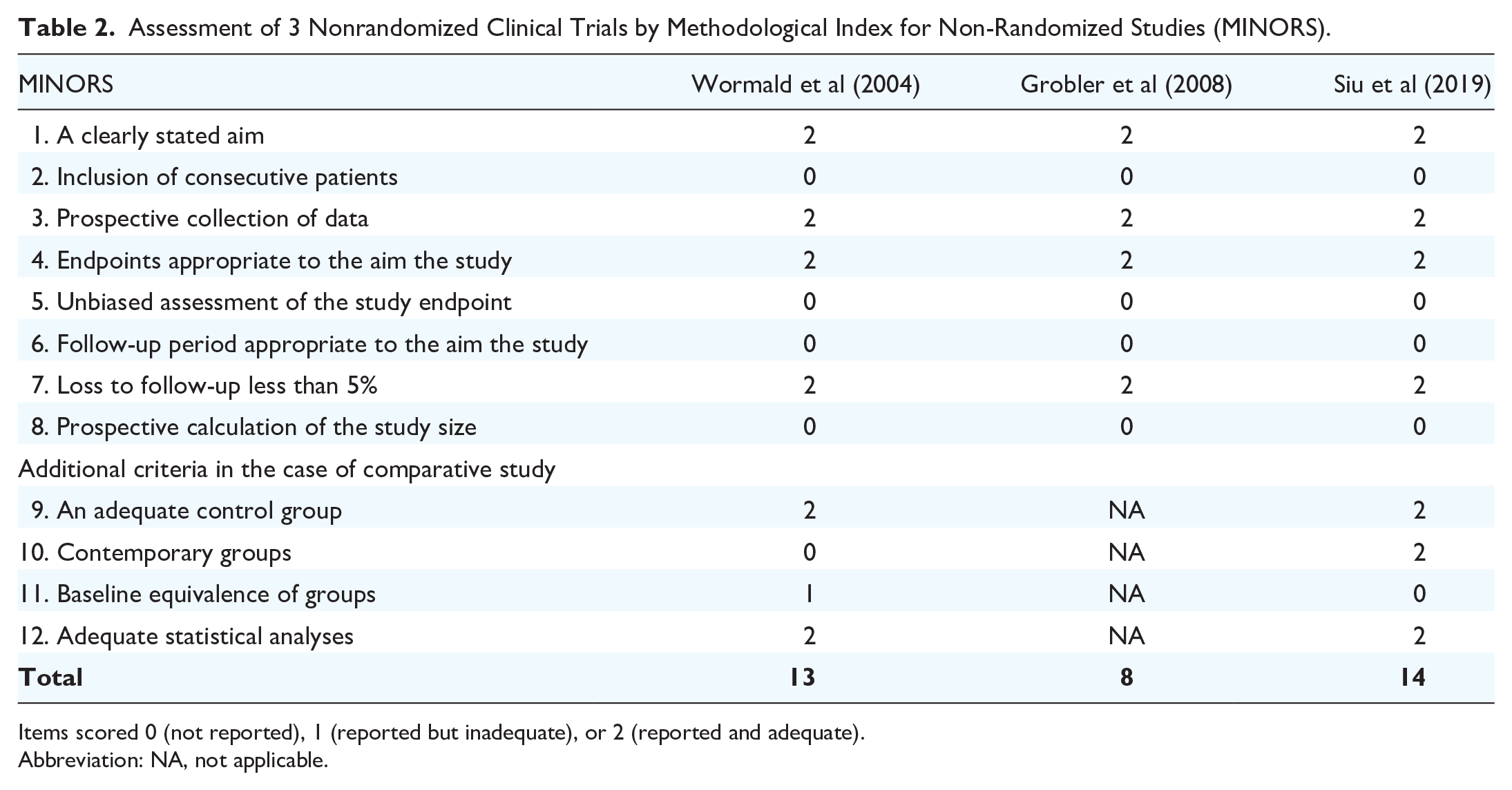
Items scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate).
Abbreviation: NA, not applicable.
Assessment of 11 Cadaveric Studies by QUality Appraisal for Cadaveric Studies (QUACS).

Numbers Q1 to Q13 in heading signified: Q1, a clearly stated aim; Q2, sufficient information about the sample; Q3, thorough description of methodology; Q4, state and type of embalmment of the specimens; Q5, state of the education of dissecting researchers; Q6, number of researchers; Q7, unambiguous description of the results; Q8, statistical methodology; Q9, consistency of the findings; Q10, photographs of the observations; Q11, discussion within the context of current evidence; Q12, clinical implications; Q13, limitations of the study. Items scored 0 (not reported or inadequate) and 1 (reported and adequate).
Values are total (relative to maximum) %.
Assessment of 2 Model Studies by Medical Education Research Study Quality Instrument (MERSQI).
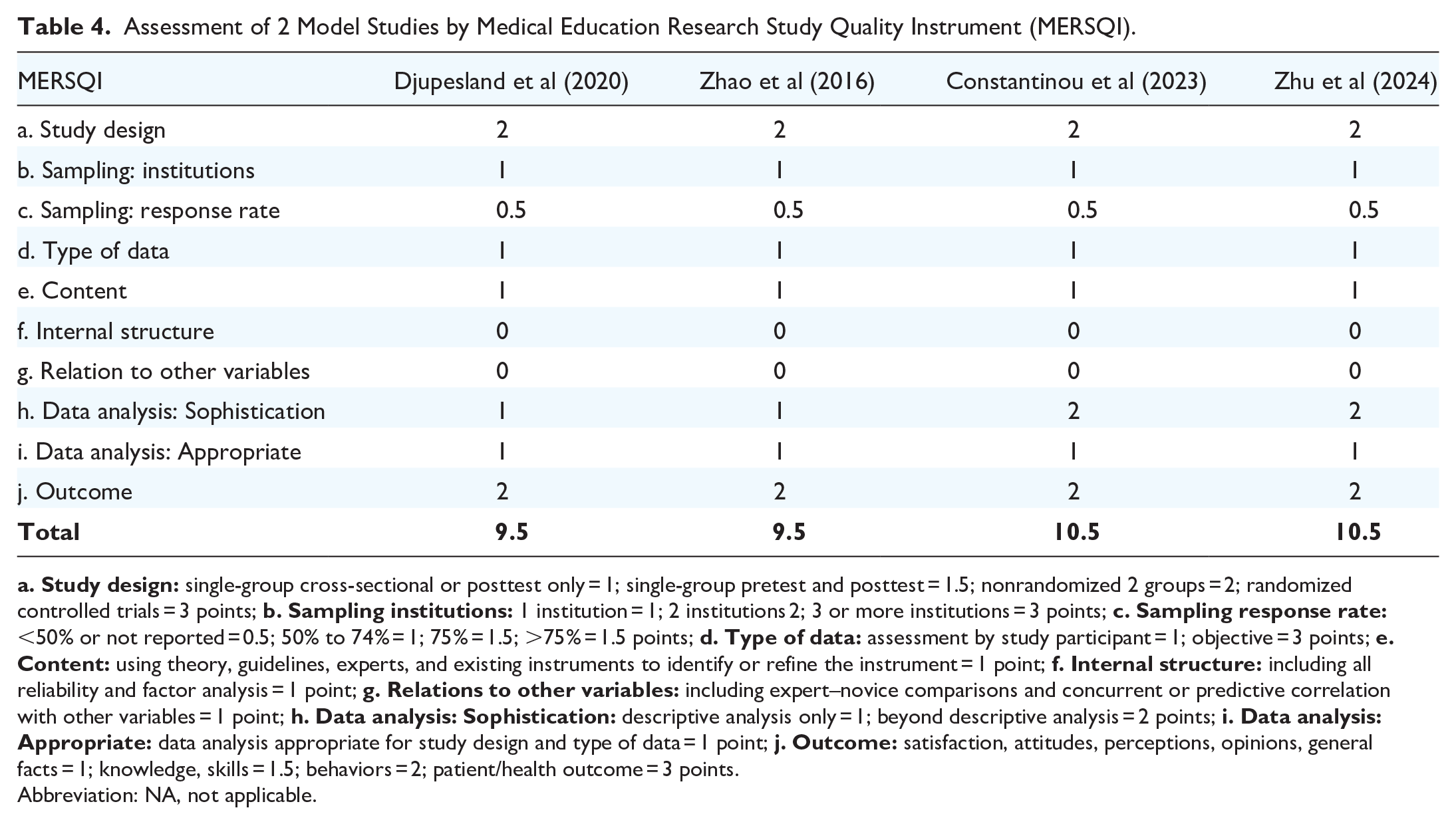
Abbreviation: NA, not applicable.
Endoscopic sinus surgery
Fifteen studies explored the impact of ESS on frontal sinus irrigation, including two human trials,27,28 nine cadaver assessments,16-19,31-35 two 3D-printed model studies,36,37 and two computational fluid dynamics studies.15,38 We synthesized the findings regarding the influence of ESS on frontal sinus irrigation, considering various surgical types and Draf grading of frontal sinus surgery.
In the cadaver assessment, 3 studies conducted stepwise endoscopic dissections on fresh-frozen human cadaver heads, utilizing a scoring table to evaluate the amount of irrigation entering the frontal sinus after each step.17,18,34 Among these, 2 studies segmented the operation of the maxillary sinus, frontal sinus, and sphenoid sinus into 4 steps.18,34 Step 0 represented the undissected state, Step 1 involved Draf I+ superior turbinectomy, Step 2 comprised Draf IIA+ 5 mm ostium in maxillary and sphenoid, and Step 3 entailed Draf III+ widest dissection in maxillary + removal of the sphenoid face. One study found that frontal sinus penetration remained unchanged in Step 1 compared to the undissected status. The highest frontal sinus irrigation penetration was observed in Step 2, with no variation in irrigation distribution within the sinus between Step 2 and Step 3, irrespective of head position and delivery device. 18 Another study revealed a general trend of frontal sinus improvement throughout each dissection stage with the nose facing 45° downward, although no significant statistical difference was noted. 34 Besides, Chen et al 17 performed dissections from undissected to maxillary antrostomy with total ethmoidectomy to Draf III and removal of intersinus septum. As the extent of surgery increased, they observed a decline in nasal irrigation fluid’s ability to access the frontal sinus, likely due to reduced backpressure in the nasal passage following sinus cavity opening.
Another study by Gantz et al 31 performed balloon sinuplasty followed by ESS on 4 human cadaver heads. In this study, balloon sinuplasty involved inserting a catheter into the maxillary and frontal sinus cavities, inflating the balloon to 12 cm H2O for 10 seconds, followed by deflation and device withdrawal. ESS involved uncinectomy, maxillary antrostomy, total ethmoidectomy, sphenoidotomy, and Draf IIA frontal sinusotomy. Using a 3-point scale, the staining score of the frontal sinus increased significantly from 1.29 to 2.04 after balloon sinuplasty (P = .006), whereas no statistically significant increase was observed following ESS compared to the balloon procedure (P = .96).
A total of 12 studies reported the impact of Draf classification in frontal sinus surgery on nasal irrigation distribution.15-19,31,32,34-38 Among these, 4 studies focused solely on frontal sinus surgery,16,19,32,38 while 8 studies included concomitant surgery on the maxillary sinus, sphenoid sinus, and ethmoid sinus.15,17,18,31,34-37 Three studies indicated that Draf III demonstrated superior efficacy to Draf IIA in achieving frontal sinus irrigation distribution.16,19,38 Similarly, Gantz et al exclusively performing surgery up to the Draf IIA degree found no disparity in frontal sinus irrigation between Draf IIA procedure and balloon sinuplasty, resulting in moderate irrigation levels. 31 However, 3 studies showed no difference between Draf IIA and Draf III in irrigation distribution within the frontal sinus,18,34,36 with one study even indicating a decrease in frontal sinus irrigation with Draf III. 17 Moreover, Spielman et al reported enhanced irrigant penetration following standard Draf IIA frontal sinusotomy after resecting the axilla-agger nasi complex to achieve a 0° endoscopic view. 35 Three studies exclusively examined the impact of Draf III surgery on frontal sinus irrigation. Constantinou et al reported that squeeze bottles provided superior coverage at the frontal site following Draf III. 37 However, Zhao et al 15 found that, while Draf III achieved effective penetration of irrigation into the frontal sinus, it unexpectedly resulted in premature spillage of irrigation fluid across the resected septum, leading to reduced irrigation in other sinuses. Roxbury et al 32 reported that increasing septectomy in Draf III surgery did not enhance lavage delivery to the frontal sinus and suggested a limited septectomy for access to ensure effective postoperative drug delivery.
In 2 human studies, frontal sinuses were surgically opened, although no specific classification of frontal sinus surgery was provided.27,28 One study indicated that surgically treated sinuses were more likely to achieve penetration compared to nonoperated sinuses (P = .0016) and obstructed sinuses (P = .0325), 28 whereas the other study found no significant difference in the frontal sinuses even after ESS. 27 Moreover, Grobler et al 28 reported that the irrigation penetration into the frontal sinus measured 3.6 mm [95% confidence interval (CI) 2.504-4.496], while the unpenetrated dimension was 0.7 mm (95% CI 0.650-1.650; P < .0001). Similarly, in a cadaveric assessment, data on sinus penetration for all sinuses were amalgamated, revealing the most substantial enhancement in sinus penetration at an ostial size of 4.7 mm, albeit not specifically for the frontal sinus alone. 34 In addition, this study noted that the frontal sinus irrigation did not improve with the enlargement of the sinus ostium.
Compared to nonoperative sinonasal cavities, Draf IIA procedures facilitated the opening of the frontal sinus ostium, leading to enhanced irrigation entry into the sinus. A procedure of Draf IIA could achieve sufficient irrigation for the frontal sinus. However, the benefits of more extensive procedures, such as Draf III, for frontal sinus irrigation remained uncertain.
Irrigation Devices
All included studies detailed various devices utilized for nasal irrigation. Based on different volumes and power, irrigation devices could be divided into syringes, squeeze bottles, irrigation pots, low-pressure gravity-dependent douching devices, and pulsation devices. Syringes were used in 3 studies,18,26,37 involving gently pushing the solution into the nostril. Irrigation pots, with volumes of 120 mL or 240 mL, were utilized in 2 studies.29,33 The irrigation pot was shaped like a teapot and was used with the head turned to the side so that the solution entered the upper nostril and exited the lower nostril. One study used a low-pressure gravity-dependent douching device, 18 which required no mechanical or electrical assistance for irrigation. Pulsating devices were utilized in 3 studies,15,17,29 facilitating liquid flow under constant volume and pressure independent of patients’ efforts. Squeeze bottles were the most commonly used devices, employed in 16 studies,15-19,27-37 relying on hand squeezing to deliver the solution into the nostril.
A total of 8 studies compared the effects of different devices on frontal sinus irrigation.15-18,26,29,33,37 Wormald et al 26 compared the distribution of nasal irrigation with syringes and nasal spray in the frontal sinuses, finding that the douching method was notably more successful in penetrating the frontal recess than the nebulizer. However, neither the douche nor the nebulizer achieved penetration into the frontal sinus, potentially due to the smaller syringe volume used. Eight studies compared squeeze bottles and other devices.15-18,29,30,33,37 Constantinou et al reported squeeze bottles provided better distribution than nasal drops. 37 Three studies compared the irrigation effect of the squeeze bottle with the pulsation device.15,17,29 Two studies adopted the nose-to-sink position and consistently found that the squeeze bottle provided more significant irrigation in the frontal sinus.17,29 However, a computational fluid dynamics study revealed that both the pulsating device (12 mL/s) and the squeeze bottle (60 mL/s) effectively penetrated the frontal sinus at the vertex down position. In addition, Mozzanica et al 18 reported no difference in the irrigation distribution between the squeeze bottle and the gravity-dependent device in all surgical steps. Harvey et al 33 reported that the irrigation pot offered broader distribution in all sinuses than the squeeze bottle after any surgery, except for the frontal sinus alone. Furthermore, 2 studies reported that the large-volume squeeze bottle provided better irrigation in the frontal sinus than the low-volume one.16,30
Head Position
All studies included reported the head position during nasal irrigation. According to the angle of the nose and the vertical standing craniocaudal axis, head positions could be divided into 3 types: the neutral, upright position, the nose-to-sink position, and the vertex down position. The neutral upright position was used in 5 studies,16,19,27,34,37 where the head was slightly forward, maintaining a natural upright position. The nose-to-sink position was employed in 13 studies,15,17,18,28-31,33-38 with the head positioned such that the nose faced 45° downward. Nine studies used the vertex down position,15,16,18,19,26,30,32,34,36 wherein the head was oriented with the nose facing 90° downward.
A total of 7 studies compared the effect of frontal sinus irrigation at different head positions.15,16,18,19,30,34,36 Five studies demonstrated that the vertex-down position during the irrigation resulted in superior delivery to the frontal sinus compared to the other 2 positions.16,18,19,30,36 Among them, 3 studies18,19,30 reported that when considering the combined impact of head position, irrigation device, and surgical extent on frontal sinus irrigation, the vertex-down position exhibited a notable enhancement compared to the nose-to-sink position. Barham, et al 16 reported that the vertex head position resulted in enhanced distribution (90.6% vs 50.1%, P < .001), and its effect was synergistic with Draf III (100% with 87.5% lavage, P < .001), although it did not surpass the efficacy of Draf IIA (81.2% with 25% lavage, P < .001). A similar study found that the distribution of Draf II and Draf III at the vertex down position covered most of the frontal sinuses, unlike at the nose-to-sink position. 36 However, 2 studies found that frontal sinus irrigation was worse at the neutral upright position, while there was no difference between the nose-to-sink and the vertex down position.15,34
Discussion
Sinonasal cavity irrigation after surgery is a recognized and effective method for the long-term treatment of CRS. It has been proposed that factors influencing sinonasal irrigation include surgery, irrigation devices, and head position. 39 However, it is important to acknowledge that despite advancements, accessing the frontal sinus through irrigation remains challenging due to its intricate surrounding anatomy. 11 Situated adjacent to the orbit and skull base, the frontal sinus necessitates specific irrigation devices and head positions to ensure adequate delivery of irrigation, factors that significantly affect post-ESS irrigation efficacy.40,41 Moreover, residual air cells in the frontal recess post-surgery may result in incomplete surgical clearance, thereby heightening the challenge of achieving effective frontal sinus irrigation and topical drug therapy.27,42 This scenario can contribute to CRS recurrence, particularly in patients with eosinophilia, asthma, and aspirin intolerance.43-45 Therefore, comprehending the essential factors for efficient frontal sinus irrigation among CRS patients is pivotal for maintaining disease control post-ESS. To our knowledge, it is the first systematic review summarizing the evidence for efficient frontal sinus irrigation after ESS for patients with CRS.
We first summarized the impact of ESS on frontal sinus irrigation. The distribution of nasal irrigation fluid in unoperated sinuses, particularly in the frontal sinus, was limited, regardless of the irrigation device and head position.15,18,26,46 The extent of surgical treatment for the frontal sinus varied, ranging from straightforward balloon ostial dilation to comprehensive frontal surgery. 41 Balloon ostial dilatation of the frontal sinus aimed to expand the narrow passage without removing tissue. In the study by Gantz et al, both balloon dilation and Draf IIA significantly increased frontal sinus permeability, with similar improvements in frontal sinus irrigation. 31 However, the study was performed on only 4 cadaver heads, and the small sample size may have contributed to the lack of a statistical difference in frontal sinus penetration between balloon sinuplasty and ESS. In addition, the study measured staining after irrigation rather than using real-time video, which might have underestimated the amount of flushing fluid entering the frontal sinus after ESS. Balloon sinuplasty is commonly indicated for patients with chronic sinusitis who do not have nasal polyps. This is because the procedure only dilates the sinus opening without removing tissue, potentially limiting the effectiveness of postoperative irrigation. However, few studies have compared the effects of these 2 procedures on postoperative irrigation. Therefore, further research is needed to determine if balloon dilation has the same effect as Draf IIA in improving frontal sinus permeability. Four other studies demonstrated that the Draf III procedure provided better frontal sinus irrigation than Draf II, regardless of the device and head position.16,19,31,38 Removing the middle turbinate and septum left the frontal sinus optimally open, allowing for better irrigation distribution.47,48 However, the effect of surgical expansion on frontal sinus irrigation remains controversial. The distribution of irrigation in the frontal sinus may not be directly proportional to the size of the sinus opening. The increased frontal sinusotomy from Draf IIA to Draf III did not significantly improve the frontal sinus permeability. After surgical removal of the tissue, the volume of the nasal passages increased, reducing the back pressure required for the rinses to reach the frontal sinus. 17 Consequently, the irrigation fluid may cross the excised nasal septum prematurely, reducing penetration into the frontal sinus.15,18,32 Notably, Zhu et al proposed that Draf I to III surgeries had varying effects on postoperative irrigation, contingent on frontal sinus development. 38 They observed that the impact of Draf procedures was more pronounced in the well-developed group than the moderately developed group. This suggests that it may be feasible to determine the optimal surgical scope in the future based on the degree of frontal sinus development. Based on the aforementioned evidence, Draf IIA appeared to be the minimum surgical procedure necessary to achieve sufficient irrigation in the frontal sinus. More studies are required to verify these findings.
The choice of irrigation device also played a crucial role in the effectiveness of frontal sinus irrigation. Low-volume devices, such as nasal drops and nebulizers, can successfully deliver drugs into the nasal cavity but show minimal irrigation into the frontal sinus. 49 In contrast, large-volume devices provided better frontal sinus irrigation.16,26,30 One possible explanation is that large volumes of water could easily fill the sinonasal cavity and provide a higher fluid flow level, which is crucial for reaching the relatively lower ostia of the frontal sinus. Furthermore, a previous study demonstrated that the irrigation efficiency was volume-dependent.50,51 The present study showed that squeeze bottles likely provided the best irrigation for the frontal sinus.15,17,18,30 This advantage was related to high flow momentum during the effective squeeze, increasing penetration into the frontal sinus. However, some human studies suggested that the squeeze bottle may have some side effects, including Eustachian tube dysfunction.50,51 It should be noted that the squeeze pressure of the squeeze bottle was adjustable. Appropriate squeeze pressure and patient selection can reduce the side effects. In addition to the device itself, the design of the nozzles significantly affects the distribution of the fluid flow within the sinonasal cavity and the irrigation efficiency. Wu et al reported that a squeeze bottle with an extended nozzle improved the flushing efficiency compared to a classic rinse bottle. 52 In the future, more suitable devices should be invented to improve the efficiency of frontal sinus irrigation. Overall, the choice of irrigation device should be based on each patient’s specific needs and conditions. Large-volume devices, like squeeze bottles, offer adequate irrigation for the frontal sinus, but physicians should carefully assess patients’ suitability for these devices to avoid potential side effects. Proper patient education and guidance on using irrigation devices can enhance the benefits of nasal irrigation in managing sinus conditions effectively.
We next summarized the findings related to the head position during nasal irrigation and its impact on frontal sinus delivery. Wu et al evaluated 6 head positions, including head tilting 10°, 45°, and 60° forward with or without leaning 30° to the right and found that the head position of tilting 45° forward with leaning 30° was the most suitable for nasal irrigation. 53 In our study, we categorized the head position into 3 types according to the angle of the nose and the vertical line: the neutral upright position, the nose-to-sink position, and the vertex down position. Due to its anatomical arrangement and the effect of gravity, the frontal sinus, which is positioned anteriorly and superiorly to the ethmoid sinus, exhibited a less favorable irrigation effect in the neutral upright position. In the nose-to-sink position and the vertex down position, the frontal sinus was kept lower than the site of surgical resection, suggesting similar effects on frontal sinus irrigation in both positions.15,34 However, more studies reported that the vertex down position improved distribution and synergistically enhanced the effect of specific surgical techniques on frontal sinus irrigation.16,18,19,36 The vertex down position maximized the irrigation path into the frontal sinus to coincide with the direction of gravity, allowing direct, unimpeded irrigation flow into the frontal sinus. Moreover, the vertex down position improved fluid flow distribution within the frontal sinus following Draf IIA (50.1%) and Draf IIB (81.3%) procedures, with the most synergistic effect observed with the Draf III procedure (90.7%).16,19 For large-volume irrigation devices, head position may not significantly affect frontal sinus irrigation as it did for low-volume devices.29,42 It should be noted that the vertex down position often requires patients to kneel during irrigation, which can be challenging for elderly patients and those with arthritis. The goal of selecting a suitable head position is to promote the fluid flow efficiently entering or flushing the entire frontal sinus by adjusting the vertical height of the frontal sinus and the ostia position relative to the fluid flow. With advancements in irrigation device design, achieving a comfortable head position with high irrigation efficiency could enhance patient compliance and treatment outcomes.
Our study has several limitations. First, there was significant heterogeneity in the methodologies of the included studies. Different scoring scales were used to assess the distribution of flushing within the frontal sinus. Adopting a more uniform evaluation method would improve consistency across studies. Second, most of the included studies were cadaver studies, which raised questions about the reproducibility of these results in patients with CRS. Cadaver studies and 3D-printed model studies did not account for the effects of edema, discharge, and ciliary movement on the distribution of frontal sinus irrigation and, therefore, cannot fully simulate the pathological state of CRS. In addition, large-volume irrigation in living subjects might result in poor subjective experiences due to the natural breathing rhythm. Consequently, more high-quality human trials are needed to determine the optimal method for frontal sinus irrigation in patients with CRS after ESS.
Conclusion
Existing studies demonstrated a lack of uniformity regarding frontal sinus irrigation after ESS. However, certain approaches have shown promise. Elements for optimization of frontal sinus irrigation are a minimum of a Draf IIA procedure for frontal sinus dissection, use of large-volume irrigation, and vertex down head positioning. The opening degree of the frontal sinus ostium after ESS, ostia position relative to the fluid flow during the irrigation, and the volume of irrigation devices are determining factors for achieving sufficient frontal sinus irrigation.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
D.W. and Y.Q. analyzed the data and drafted the manuscript. J.H. revised the manuscript. D.W. designed the study and revised the manuscript. All authors have read, edited, and approved the final manuscript.
Availability of Data and Materials
All data gathered for the systematic review were gathered from articles cited in this article and listed in the reference section.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Natural Science Foundation of China (82000954), Beijing Science and Technology Nova Program (Z201100006820086), Beijing Hospitals Authority Youth Program (QML20190617), Beijing Hospitals Authority Clinical Medicine Development of Special Funding (XMLX202136), and the Key clinical projects of Peking University Third Hospital (BYSYZD2023029).
Ethics Approval and Consent to Participate
Not applicable.