
Abstract
Objective
To review the current literature about surgical treatments of pediatric bilateral vocal fold paralysis (PBVFP).
Methods
A systematic review of the current literature in PubMed, Scopus, and Cochrane Library regarding etiologies and management of PBVFP was performed until November 2023 according to PRISMA statements. Quality assessment was assessed with Methodological Index for Non-Randomized Studies (MINORS) tool.
Results
Of the 211 screened articles, 26 were included accounting for 320 patients. The etiologies included idiopathic (42.2%), congenital (19.7%), neurological (16.9%), or post-surgical (9.5%) pediatric bilateral vocal cord paralysis (PBVCP). Patients were decannulated in 76.7% of cases without laryngeal procedure. Decannulation was achieved in 84.6%, 66.6%, 83.3%, 80.0%, and 62.5% of cases of laterofixation of the vocal fold, cricoid split approaches, partial or total arytenoidectomy, uni- or bilateral transverse cordotomy, and selective laryngeal reinnervation, respectively. Dyspnea/stridor relief, swallowing, or voice quality outcomes were used in some studies, which reported conflicting results. Revision and complications varied between studies, with complications mainly involving edema, granuloma, or aspirations. Revision was required in 6.4%, 12.9%, and 40.0% of cases that underwent laterofixation of the vocal fold, arytenoidectomy, and cricoid split procedures, respectively. There was substantial heterogeneity across studies in inclusion criteria, procedures, and outcomes.
Conclusion
The management of PBVFP may involve several temporary or permanent surgical procedures that are associated with overall subjective improvements of symptoms, and laryngeal findings. The retrospective design of studies, the small number of cohorts, the lack of objective outcomes, and the differences between teams regarding procedure timing and features limit drawing reliable conclusions about the superiority of one technique over others.

Keywords
Introduction
Pediatric bilateral vocal fold paralysis (PBVFP) is the second most common congenital laryngeal anomaly in the pediatric population accounting for 15% to 20% of cases. 1 The overall prevalence remains unclear as many cases are not detected early in life. 1 The pediatric bilateral vocal cord paralysis (PBVCP) incidence is estimated to be 0.75 cases per million births per year and represents 30% to 60% of all vocal fold dysfunction in neonates. 2 Most PBVFP cases are idiopathic, while common causes may include congenital malformations, neurological conditions, and iatrogenic surgical injuries. 1 The management of PBVCP is controversial without international expert consensus. Depending on the laryngologist experience, the procedures may substantially vary from one center to another, including laterofixation of the vocal fold, cricoid split, unilateral or bilateral transverse cordotomy, partial or total arytenoidectomy, laryngeal selective reinnervation surgery, and botulinum toxin A injection. 3
The aim of this systematic review was to investigate the etiological, medical, and surgical procedure outcomes of PBVCP.
Material and Methods
The criteria for study inclusion were based on the population, intervention, comparison, outcome, timing, and setting (PICOTS) framework. 4 Two authors (J.R.L. and N.N.) independently reviewed and extracted data according to the PRISMA checklist for systematic reviews. 5
Types of studies: Uncontrolled or controlled prospective or retrospective studies published between 1983 and 2023 were included if they investigated the etiology, and/or the surgical management of PBVCP. The studies had to be published in English, or French peer-reviewed journals. Authors only considered studies reporting data for ≥2 children.
Populations, inclusion/exclusion criteria: Authors should report inclusion/exclusion criteria, definition of PBVFP, diagnostic approach, medical or surgical management, and therapeutic outcomes. Only studies reporting data of patients under 18 years of age were included. Studies including children or infants with unspecified laryngeal immobility or posterior glottic stenosis were excluded. The investigators needed to support the PBVFP diagnostic through the clinical history of patient (eg, neonate, post-infection, or post-surgical paralysis), laryngeal electromyography (EMG), or laryngeal endoscopic findings. The positions of the vocal folds were defined as median, intermediate, or lateral. 6 Paresis and paralysis were both considered. Paresis was diagnosed if movement was sluggish, while paralysis was diagnosed if no volitional movement was observed. 6
Outcomes: The following outcomes were reviewed: study design, number of patients, gender ratio, mean or median age, etiology, duration of follow-up, tracheotomy prior to treatment, therapeutic approaches, number of procedure(s) per patient, decannulation rate, complications, and surgical outcomes (eg, swallowing, voice, or airway assessments). Importantly, unlike previous reviews, 3 this systematic analysis of the literature will be focused on studies reporting outcomes of only 1 procedure, and not multiple procedures in a single cohort.
Intervention and comparison: The following procedures were considered: tracheotomy, unilateral or bilateral laterofixation of the vocal fold, posterior transverse cordotomy, partial and total arytenoidectomy, selective laryngeal reinnervation, botulinum toxin A injection, and laryngeal pacing. 6 Studies including combined surgical approaches (eg, cordotomy with partial arytenoidectomy) or new surgical approach were considered.
Timing and setting: There was no criteria for specific stage or timing in the “disease process” of the study population.
Search Strategy
The literature search was carried out by 2 independent authors (J.R.L. and N.N.) with PubMed, Scopus, and Cochrane Library databases. The databases were screened for abstracts and titles referring to the description of features of pediatric patients diagnosed with bilateral vocal cord paralysis (BVCP). Authors analyzed full texts of the selected papers. Studies were considered if they had database abstracts, available full texts or titles containing the search terms. Results of the search strategy were reviewed for relevance and the reference lists of these articles were examined for additional pertinent studies. Any discrepancies in synthesized data were discussed and resolved by the remaining co-authors. The following keywords were considered: “bilateral,” “vocal fold,” “vocal cord,” “paralysis,” “surgery,” “treatment,” and “outcome.”
Bias Analysis
The bias analysis was conducted with the Methodological Index for Non-Randomized Studies (MINORS) tool, which is a validated instrument designed for assessing the quality of non-randomized surgical studies. 7 The MINORS tool includes 12 items dedicated to methodological points of both comparative and non-comparative studies. The items were scored NP if not provided; 0 if absent; 1 when reported but inadequate; and 2 when reported and adequate. The global ideal score was 16 for non-comparative studies and 24 for comparative studies.
Results
Of the 211 screened articles, 26 studies were included.8-33 Two studies were prospective uncontrolled (EL: III),22,24 while 24 were retrospective chart-reviews (EL: IV).8-21,22,23,25-33 The data of 320 patients were available. The mean or median age of patients was available in 24 studies,8-18,20-28,29,32,33 and ranged from 1 day to 9 years old. Gender characteristics were available for 254 patients.8-11,13-16,20-25,27-29,31-33 There were 155 males (61.0%) and 99 females (39.0%), respectively (Table 1). Heterogeneity among included articles in inclusion/exclusion criteria, decannulation, postoperative functional, and surgical outcomes precluded statistically pooling the data into a formal meta-analysis, thereby limiting the analysis to a qualitative rather than quantitative summary of the available information.
Etiologies.

Seven patients had 2 etiologies supporting their paralysis.
Abbreviation: N, number.
Etiologies
The etiologies were reported in 25 studies accounting for 320 patients.8-24,26-33 According to the pooled data, the main etiologies of BVFP in pediatric population were idiopathic (42.2%), congenital (19.7%), neurological (16.9%), post-surgical (9.5%), or iatrogenic (5.8%; Table 1). Note that the differences between iatrogenic and post-surgical etiologies were unclear in most papers. Tracheotomy was already carried out in 158/260 cases (60.8%) of PBVCP at the time of inclusion.
Surgical Procedures
The surgical procedure findings were reported for 307 cases. The following surgical procedures were performed: tracheotomy (N = 89),8,9,16,31,33 external or endoscopic laterofixation of the vocal fold (N = 53),8,13,15,19,22,25,26,28 bilateral selective laryngeal reinnervation (N = 29),8,10,11,30 anterior–posterior cricoid split (N = 28),23,24,29 posterior cricoid split (N = 2), 18 external total arytenoidectomy (N = 21),12,32 endoscopic laser total/partial arytenoidectomy (N = 16), 12 endoscopic coblation-assisted partial arytenoidectomy (N = 33), 27 endoscopic unilateral (N = 8)20,32 or bilateral transverse cordotomy (N = 26),14,17,20 and botulinum toxin A injections (N = 6). 21 The laryngeal reinnervation included nerve muscle pedicle reinnervation, 30 or anastomosis between thyrohyoid branch of the hypoglossal nerve and the recurrent laryngeal nerve.10,11 In the study of Scatolini et al, 33 several procedures (eg, laryngotracheoplasty, posterior cordotomy) were performed in 9 patients who had PBVCP and subglottic stenosis (Figure 1). The therapeutic approaches regarding patient age are reported in Figure 2.

Flow chart.
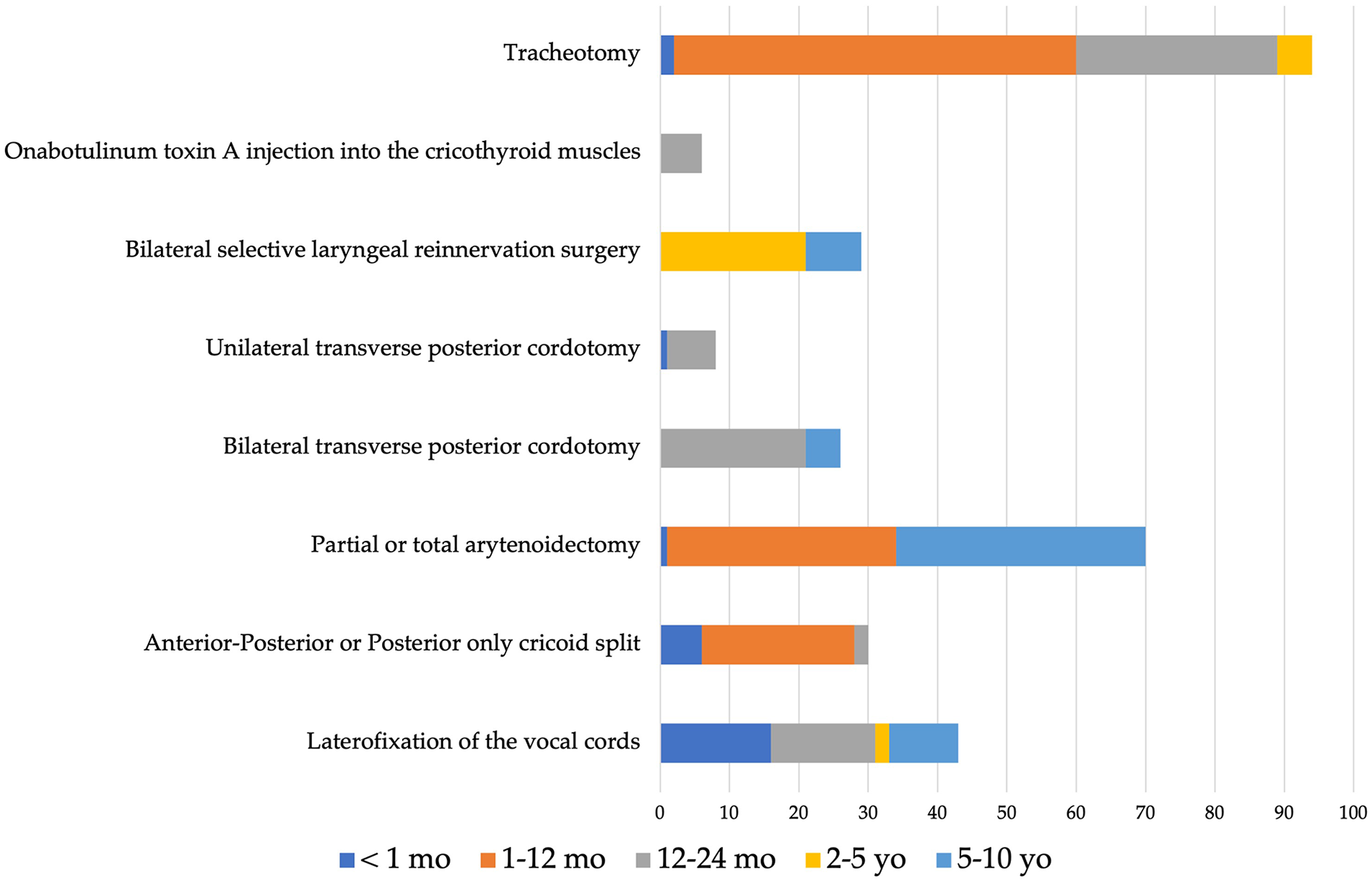
Procedures according to age.
Decannulation
The decannulation data were reported in Table 2. Pediatric patients who underwent tracheotomy until vocal fold motion recovery were decannulated in 76.7% of cases (N = 56/73).8,9,16,26,31,33 Among other studies, the vocal fold motion partly or fully recovered in 54.2% (N = 51/94) of patients who underwent laryngeal surgical procedures.20,27,28 Laterofixation of the vocal fold approaches led to a mean decannulation rate of 84.6% (N = 33/39).8,13,15,19,22,25 Irrespective to the use of costal cartilage, laryngeal framework (cricoid split) procedures were associated with a decannulation rate of 66.6% (N = 14/21).18,23,24 Patients who underwent external or endoscopic arytenoidectomy were successfully decannulated in 83.3% of cases (N = 25/30). 12 Unilateral and bilateral transverse posterior cordotomies led to decannulation rates of 80% (N = 4/5) and 100% (N = 11/11), respectively.14,17,20 Bilateral selective laryngeal reinnervation approaches were associated with a decannulation rate of 62.5% (N = 15/24). In the study of Daniel et al, 21 all children treated with injection of toxin A botulinum into the cricothyroid muscle were decannulated. Note that the follow-up substantially varied from one study to another (Table 2).
Studies.

Age was median or average according to studies.
Abbreviations: A/M, average/mean; M/F, male/female; mo, month; NP, not provided; Tracheot., tracheotomy; Rev, revision rate; VQ, voice quality; yo, year old; d, days; w, weeks.
Surgical and functional outcomes
Primary surgical and functional outcomes substantially varied across studies (Table 2). Dyspnea and stridor were considered as the primary outcomes in 9 studies.19,21,24,25-27,29,30,32 Both dyspnea and stridor were subjectively evaluated by surgeon in all studies. The change of endotracheal tube size was considered as an important outcome in 3 studies where authors commonly reported significant improvements of tube size after laryngopexy.23,24,29 Vocal cord motion was assessed through various subjective approaches in 3 studies, which reported several degrees of recovery, ranging from 36% to 88%.10,11,22,26-28
Voice quality was evaluated from pre- to posttreatment in 7 studies.8,10,11,14,15,17,22,28 Perceptual voice quality (GRBAS) significantly improved after bilateral selective laryngeal reinnervation,10,11 laterofixation of the vocal fold, 28 or bilateral posterior transverse cordotomy. 14 On the other hand, Lagier et al 17 reported significant worsening of perceptual voice quality evaluations (GRB) after bilateral posterior cordotomy. Perceptual voice quality was subjectively considered as acceptable with other composite scores after laterofixation of the vocal fold, 15 or tracheotomy 8 by authors who did not provide statistical analyses. Acoustic parameters were used to assess the posttreatment voice quality in 2 studies.22,25 Sztanó et al 25 reported significant improvements of Shimmer and Jitter post-laterofixation of the vocal fold, while harmonic-to-noise ratio worsened. The pre- to posttreatment comparison of acoustic parameters was not provided in the study of Madani et al 22 who only evaluated the postoperative acoustic measurements. Swallowing function was evaluated by Friedman et al 14 who reported similar subjective endoscopic findings from pre- to post-bilateral transverse posterior cordotomy. The postoperative diet became normal in neonates of the study of Speaker et al 28 who performed endoscopic lateralization of the vocal cords. The weight–height findings of children were normalized after lateropexy in 2 studies.22,25
Complications and revision
A few studies reported complication data.14,15,18,19,22-27,30 Madani et al 22 reported the occurrence of a neck abscess after endoscopic arytenoid abduction lateropexy in a child (N = 1/4), while there were 2 aspirations (N = 2/10) post-laterofixation of the vocal fold in the study of Mathur et al. 15 Aspirations were reported after anterior–posterior cricoid split in 6/25 patients.23,29
Friedman et al 14 observed postoperative symptomatic granuloma in 1/5 patient after transverse posterior cordotomy, which was similarly found by Tan et al 27 after coblation-assisted partial arytenoidectomy in 5/23 patients. Other studies did not report complications.18,19,24,25,26,30-33
Revisions were required in 6.4% (N = 3/47), 12.9% (N = 9/70), and 40.0% (N = 12/30) cases that underwent laterofixation of the vocal fold,13,15,19,22,25,28 arytenoidectomy,12,27,32 and anterior–posterior cricoid split procedures,18,23,29 respectively (Table 2). Uni- or bilateral transverse cordotomy was associated with a revision rate of 30.3% (N = 10/33),14,17,20 while a revision rate of 9.1% (N = 1/11) was found for selective laryngeal reinnervation.10,11,30
Bias Analysis
Two authors used the MINORS score for the bias analysis (Table 3). 7 The MINORS score ranged from 4 to 13/16. The inclusion of patients was not consecutive in most studies, leading to a lower MINORS score for retrospective chart-reviews compared to prospective studies.22,24 Only 1 retrospective study reported data that were collected in all children at similar time-points. 31 The most blatant observation of the bias analysis was the low scores for endpoint assessments (Table 3). In most studies, authors did not use pre- to post-surgical objective assessments, that is, lung evaluations, or laryngeal EMG. Only a few authors used laryngeal EMG for the diagnosis10,11,12,20,30 or for the evaluation of the vocal fold motion recovery.10,11,30 Authors subjectively assessed symptom’s relief, vocal fold motion, perceptual, and acoustic voice quality measurements in most studies. The use of laryngeal EMG is important to confirm the origin of the vocal fold immobility according to the risk to include patients with posterior glottic stenosis, which is a different condition than PBVCP. In that way, 2 teams12,19 included children with a history of post-intubation vocal fold immobility, which was clinically diagnosed as PBVCP. The report of decannulation rates in most studies is a strength because authors can compare the procedures with a similar outcome. The establishment of reliable conclusion about the effectiveness of some procedures was however difficult because some teams included children with multiple laryngotracheal abnormalities or children who underwent several procedures prior the inclusion. Thus, in the study of Scatolini et al, 33 several procedures (eg, laryngotracheoplasty, posterior cordotomy) have been performed in 9 patients who had both subglottic stenosis and BVCP. Similar observations were found in the Tucker’s study, 8 or in the study of Lesnik et al 20 who performed several procedures in children. The follow-up period substantially varied from one study to another (Table 2). Only 8 studies reported adequate data of follow-up,10,11,13-15,20,22,25,30 which is important to evaluate the long-term effectiveness of surgical procedures.
Bias Analysis.
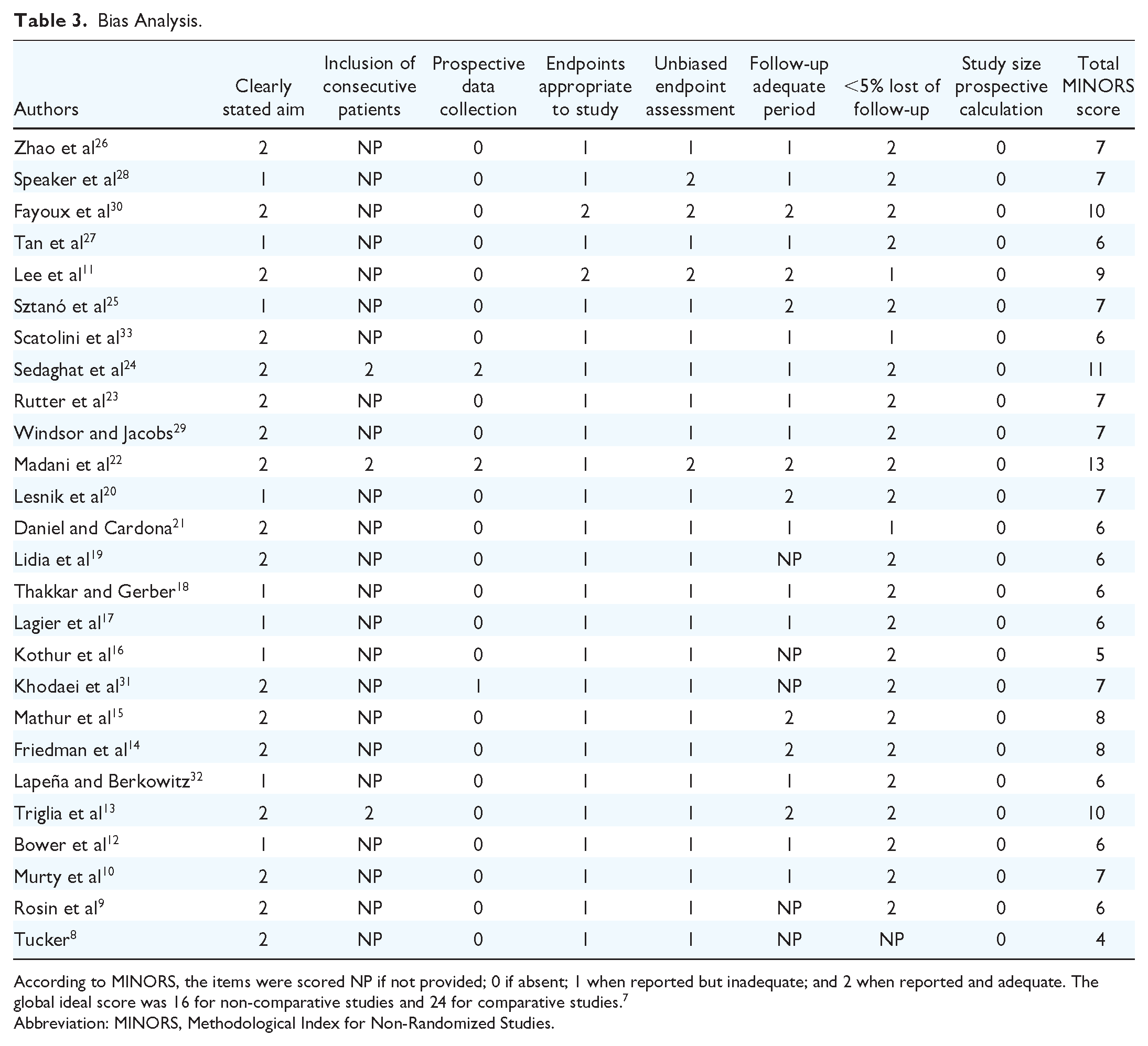
According to MINORS, the items were scored NP if not provided; 0 if absent; 1 when reported but inadequate; and 2 when reported and adequate. The global ideal score was 16 for non-comparative studies and 24 for comparative studies. 7
Abbreviation: MINORS, Methodological Index for Non-Randomized Studies.
Discussion
To date, there is no international consensus about the management of PBVCP, which is probably due to the rarity of the condition and the myriad of procedures performed in small cohort studies. The findings of this systematic review support important heterogeneity across studies for inclusion/exclusion criteria, indication of tracheotomy, types and timing of procedures, and posttreatment outcomes. Note that the present review focused on surgical procedures of PBVCP and significantly differs from other reviews focusing on etiology and management in children, 2 or adults. 6
The diagnosis of PBVCP is still controversial. To date, laryngeal EMG is the gold standard to confirm the PBVCP diagnosis. 34 However, the findings of the present study supported that laryngeal EMG was used in a few studies,10,11,12,20,30 while most authors included children with a clinical diagnosis. The confirmation of the PBVCP diagnosis through EMG is important to exclude posterior glottic stenosis, which may be clinically similar to PBVCP, while reporting therapeutic differences.34,35 In that way, the inclusion of children with PBVCP after intubation trauma in some studies where authors did not objectively support the PBVCP diagnosis may be a confusing factor.12,19
Our review reported that PBVCP was idiopathic, congenital, or neurological in more than three-fourths of cases. The etiologies of PBVCP differ from those of adult patients, which include post-surgical (76.6%), idiopathic (6.9%), and post-trauma etiologies (3.0%). 6 The differences in etiologies between pediatric and adult populations may support the differences found in recovery rates. In the present study, 76.7% of children with tracheotomy achieved partial or total recovery, while the recovery rate is substantially lower in adults who have more commonly post-surgical BVCP (trauma of the laryngeal recurrent nerves). 6
Regarding temporary surgical procedures, studies cited in Table 2 supported that laterofixation of the vocal fold is an effective approach achieving an 84.6% rate of decannulation, which corroborates findings found in the adult literature. 6 Laterofixation of the vocal fold is an alternative and cost-effective approach to tracheotomy, 36 but this procedure needs to be indicated in children who have a possibility of vocal cord motion recovery. Therefore, consideration of the etiology of PBVCP is important. Though vocal fold lateralization procedure is reported to be temporary and reversible, long-term voice outcomes have not been reported. The procedure has the potential to cause scarring of the membranous vocal fold and reduce cricoarytenoid mobility, depending on the length of time the suture is present.
Concerning definitive surgical approaches, it is not straightforward to establish the superiority of one technique over others for many reasons. First, most studies are retrospective case-series including a small number of patients. Second, inclusion criteria and timing for procedures substantially varied from one study to another. Various procedures were indicated by authors in children with BVCP and other conditions (eg, subglottic stenosis), 33 while in other cohorts, authors performed only 1 procedure irrespective to the degree of severity of BVCP. Moreover, because there is no consensus on terminology of BVCP surgeries, some procedures, which can appear similar, may substantially vary across studies. For example, there are significant differences between studies of vocal process directed surgery and the anterior and posterior cricoid split procedures.18,23,24,29 In the same way, the partial arytenoidectomy may concern a varying anterior-to-posterior portion of the vocal process; some authors removing only the anterior and medial part, while others remove anterior and posterior parts. 6 About the timing, a few authors used laryngeal EMG prior to surgery,10,11,20,30 while others rapidly proposed permanent surgery after the discovery of the BVCP without waiting potential recovery of vocal fold motion.18,22,23,25,26,28 However, in some cases, the procedure can be justified, for example, to avoid a tracheotomy in neonates. Third, most authors used subjective surgical outcomes, including the physician assessment of stridor or dyspnea, laryngoscopic findings, or perceptual voice quality evaluations. The lack of use of objective approaches, such as pediatric lung volume and function evaluations, is an important limitation. The decannulation should appear as a reliable surgical outcome. However, the decannulation rate substantially varied from one study to another, which may be due to the heterogeneity across studies in procedure timing, and consequently, vocal cord motion recovery rates. Revision rate and complications are additional useful outcomes to compare surgical procedures. However, revision and complication data were not reported in some studies,8,26 which challenges the comparison of surgical approaches.
Conclusion
The management of pediatric BVCP may involve several temporary or permanent surgical procedures that are associated with overall subjective improvements of symptoms, and laryngeal findings. However, the retrospective design, the small number of patients in studies, the lack of objective outcomes, and the differences between teams regarding the procedure timing and features limit the ability to draw reliable conclusion about the superiority of one technique over others. The establishment of international consensus guidelines considering indications of temporary and permanent surgical procedures according to the etiology and age of patient are needed.
Footnotes
Author Contributions
Availability of Data and Materials
Data are available on request.
Consent for Publication
No consent was required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. IRB was not required for a systematic review.