
Abstract
Objectives
A risk-adjusted analysis was completed using data from the National Surgical Quality Improvement Program (NSQIP) to compare the rates of recurrent laryngeal nerve injury in thyroid surgery using traditional versus alternative sources of cautery (defined as Harmonic Scalpel© and LigaSure©).
Methods
A retrospective cohort study was completed using the NSQIP database on adult patients who underwent total thyroidectomy, subtotal thyroidectomy, or completion thyroidectomy between 2016 and 2018. The primary outcome measure was recurrent laryngeal nerve injury. The exposure variable was use of conventional or alternative sources of cautery. Multivariable linear and logistic regression analyses were performed to control for potentially confounding variables.
Results
A total of 13,961 cases were analyzed; 9450 used alternative sources of cautery compared to 4511 where traditional cautery was used. There was no significant difference in rates of postoperative recurrent laryngeal nerve injury between the 2 sources of cautery compared.
Conclusions
Risk of recurrent laryngeal nerve injury should not be a factor when choosing method of cautery for thyroid surgery. Therefore, other factors like cost-effectiveness can be considered.

Introduction
Thyroid surgery is one of the most commonly performed surgeries in Otolaryngology—Head and Neck Surgery. Hemostasis is paramount to avoid life-threatening complications. A known but dreaded complication of thyroid surgery is damage to the recurrent laryngeal nerve (RLN), with a cited risk of permanent RLN injury in 0.3% to 3% of cases, and transient RNL palsies in 5% to 8%. 1 Adequate hemostasis is required for safe thyroid surgery. Poor intraoperative hemostasis can lead to poor visibility, therefore putting the RLN at higher risk of injury. In addition, poor hemostasis can lead to postoperative hematoma, therefore putting the RNL at further risk when take back surgery is required in an emergency setting.
The optimal source of cautery for hemostasis in thyroid surgery is still up for debate. Conventional hemostatic techniques include conventional bipolar and monopolar cautery, vascular ligation, and hemostatic clips. These techniques are considered the gold standard for thyroid surgery. 2 Alternative sources of cautery including the Harmonic Scalpel© and the LigaSure Vessel Sealing System© are gaining popularity. These devices are marketed to achieve fast and safe hemostasis with less thermal spread, with the overall goal of reducing operative time and complications. 3
Over the years, research has been conducted comparing these alternative sources of cautery to conventional cautery. The research to date has assessed operative efficiency, intraoperative blood loss, postoperative complications, surgical completeness in oncologic surgery, and cost-effectiveness.4-6 There has not yet been a retrospective, risk-adjusted analysis using a large database conducted to compare the rates of RLN injury between conventional cautery and the alternative sources.
The primary objective of this study was to use a large, multi-institutional database with a risk-adjusted analysis to compare post-thyroidectomy RLN injury as a clinically significant outcome between conventional hemostasis and alternative sources of cautery (operationally defined as the Harmonic Scalpel© and LigaSure Vessel Sealing System©). The secondary objective was to measure other factors contributing to RLN injury.
Materials and Methods
Study Design
A retrospective cohort study of patients undergoing total thyroidectomy, subtotal thyroidectomy, and completion thyroidectomy was conducted. The primary outcome variable was RLN injury. The exposure variables were traditional or alternative sources of cautery. The use of “alternative” sources of cautery was defined as use of either of the Harmonic Scalpel© or the LigaSure Vessel Sealing System© device.
Data were collected using the the ACS National Surgical Quality Improvement Program (ACS NSQIP®) from the years 2016 to 2018. NSQIP is a nationally validated, risk-adjusted, outcomes-based program to measure and improve the quality of surgical care. A number of 713 centers contribute to the ACS-NSQIP database in the United States, Canada, Australia, and within Europe and Asia. The information contained within the ACS-NSQIP database, including procedure-targeted data, is described in detail in the Participant Use Data File user guides. For our study objective, access was granted to the ACS-NSQIP database through a contractual Data Use Agreement. All data were stripped of personal identifiers. This study did not require institution ethical approval as NSQIP data are exempt from the Ottawa Hospital REB as it uses deidentified data.
Population
All patients included were older than 18 years and were selected for inclusion on the basis of current procedural technology (CPT) codes. Patients undergoing the following procedures (CPT codes) were included in our analysis: partial thyroid lobectomy, unilateral, with or without isthmusectomy (60240); partial thyroid lobectomy, unilateral, with contralateral subtotal lobectomy, including isthmusectomy (60212); total thyroid lobectomy, unilateral, with or without isthmusectomy (60220); total thyroid lobectomy, unilateral, with contralateral subtotal lobectomy, including isthmusectomy (60225); thyroidectomy, total or complete (60240); thyroidectomy, including substernal thyroid, cervical approach (60271). We excluded the following CPT codes: thyroidectomy, removal of all remaining thyroid tissue following previous removal of a portion of thyroid (completion or redo; 60260); thyroidectomy, total or subtotal for malignancy with radical neck dissection (60254); thyroidectomy, including substernal thyroid sternal split or transthoracic approach (60270); thyroidectomy, total or subtotal for malignancy with limited neck dissection (60252). We also excluded patients who underwent thyroidectomy for reasons other than thyroid disease (eg, laryngeal or hypopharyngeal cancer, or parathyroid disease). The International Statistical Classification of Disease and Related Health Problems, ICD-10 (ICD-9) codes for the variable postoperative diagnosis included C16.0 (1510), C32.2 (1613), C32.9 (1619), C75.0 (1914), C77.0 (1960), D35.1 (2271), E21.0 (25201), E21.2 (25208), E21.3 (25200).
Data Collection
The primary outcome variable was RLN injury. The exposure variable was use of alternative sources of cautery, either the Harmonic Scalpel© or LigaSure Vessel Sealing System©, as indicated in the operative report.
The following variables were included based on previous literature and subject knowledge: age, gender, race, and potential confounding variables including body mass index, history of bleeding disorder, platelet count, American Society of Anesthesiologists Classification (ASA) classification, smoking, antihypertensive medications, drain use, nerve monitor use, and development of postoperative hematoma.
Statistical Analysis
Patients with missing data or incomplete follow-up were excluded from the analysis. Descriptive statistics were used to report baseline patient characteristics, including proportions, means, and standard deviations (SDs). The χ2 statistics were used to compare RLN injury proportions between cautery groups. Univariable and multivariable logistic regression modeling were used to assess the predictors of postoperative RLN injury. Effects estimates were reported as odds ratios (ORs) and 95% confidence intervals (CIs), comparing conventional and alternative sources of cautery. Multivariable models were constructed using explanatory variables chosen a priori based on clinical importance, and those that were observed to be highly significant in univariable models (P < .001). Otherwise, a P value of <.05 was used as the cutoff for statistical significance. All analyses were performed using SAS version 9.4 (SAS Institute).
Results
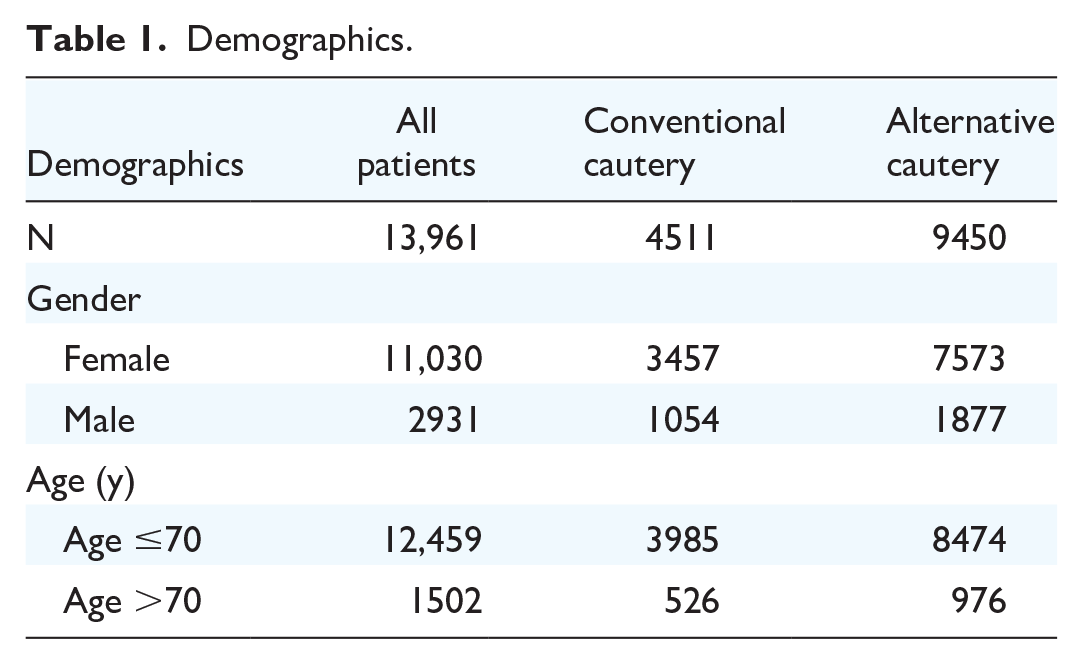
A total of 13,961 patients who underwent thyroidectomy between 2016 and 2018 were identified in the ACS-NSQIP database. Of these, 9450 patients (67.7%) underwent a total or subtotal thyroidectomy with the use of alternative sources of cautery, and 4511 patients (32.3%) underwent surgery using traditional cautery. Descriptive statistics are summarized in Table 1.
Demographics.
The overall percentage of patients with postoperative RLN injury was 5.88% (821/13,961). The percentage patients who suffered RLN when alternative sources of cautery were used was 6% (567/9450). The percentage of patients who suffered RLN injury when traditional cautery was used was 5.63% (254/4511). The crude RLN injury rate among operations using alternative sources of cautery was not significantly different than that in operations using conventional cautery (P = .3857). See Table 2.
Rate of Recurrent Laryngeal Nerve Injury in All Patients and by Type of Cautery Used.

Univariable analysis demonstrated the following risk factors to be associated with a significantly increased rate of RLN injury: age, body mass index, history of bleeding disorder, use of antihypertensive medications, ASA score over 2, drain use, use of nerve monitor, and incidence of hematoma (Table 3).
Results of All Variables by Univariate Analysis.

Abbreviation: ASA, American Society of Anesthesiologists Classification; BMI, body mass index.
Multivariable analysis for RLN injury demonstrated that there was no statistically significant difference in RLN injury when conventional cautery was compared with alternative sources of cautery, OR 1.13 (95% CI 0.97-1.33; P = .1251).
On further multivariable analysis, there was a significantly higher rate of RLN injury in patients with a bleeding disorder OR 1.88 (95% CI 1.15-3.09; P = .012), when a drain was used OR 1.30 (95% CI 1.12-1.53; P = .0008) and in patients with a postoperative hematoma OR 2.48 (95% CI 1.7-3.6; P < .0001). There was a significantly lower rate of RLN injury when the nerve monitor was used OR 0.83 (95% CI 0.71-0.97; P = .016). See Table 4 for full results for multivariable analysis.
Results of Multivariate Analysis for Risk Factors for Recurrent Laryngeal Nerve Injury.

Abbreviation: ASA, American Society of Anesthesiologists Classification; BMI, body mass index.
Discussion
This retrospective risk-adjusted analysis using the NSQIP was completed to compare postoperative RNL injury between thyroid surgery using conventional cautery and alternative energy devices.
Within our data set, there was no significant difference in RLN injury when conventional and alternative sources of cautery were compared. On multivariable analysis, there was a significantly higher rate of RLN injury in patients with a bleeding disorder, in cases where a drain was used, and in patients with postoperative hematoma. The authors hypothesize that these factors may reflect cases with more bleeding—whether it be in a patient with a history of a bleeding disorder, reflected by a postoperative hematoma, or by a surgeon’s choice to place a drain. Increased bleeding in the field can lead to poorer visualization and inadvertent injury of critical structures like the RLN. We hypothesize this may be the reason these cases had higher reported rates of RLN injury. The choice to place a drain may also reflect cases where the thyroid gland was larger therefore leaving more dead space in the wound after thyroidectomy, leading the surgeon to place a drain before closing. A larger gland can distort anatomy, and typically requires more extensive dissection to allow for mobilization. These factors may lead to challenging anatomy, increased traction on the nerve, or more extensive dissection along the length of nerve increasing the chance of damage to the RLN.
On multivariable analysis, there was a significantly lower rate of RLN injury when a nerve monitor was used. This was an interesting finding. Until recently, the data on use of a nerve monitor and RLN injury have been fairly equivocal. There was a recently published article analyzing 17,510 patients using the AC NSQIP database that found that nerve monitoring was used in nearly two-thirds of thyroid surgeries between 2016 and 2018, and the use of a nerve monitor was associated with a lower risk of RLN injury. 7
Other research groups have compared various sources of cautery with aim to find the optimal source for thyroid surgery. Injury to the RLN has been collected within the category of postoperative complications, however has never been assessed as the primary outcome measure. A systematic review and meta-analysis of 9 clinical trials compared LigaSure© with conventional cautery and found no advantage to LigaSure© in terms of postoperative complications rates, including hypocalcemia, nerve lesions, hematoma, and infection. 5 The authors reported no significant difference in the overall incidence of postoperative complications, OR 0.91 (0.61-1.36; P = .65). 5 They reported transient nerve lesions, OR 1.05 (0.53-2.08; P = .88), and combined all permanent postoperative complications, OR 0.49 (0.12-2.00; P = .32), however did not report on permanent nerve damage. 5 Another systematic review and meta-analysis analyzed 12 randomized control trials (RCTs) comparing Harmonic Scalpel© and traditional cautery also found that complications were similar in both groups. 4 Postoperative complications included transient and/or permanent RLN palsy or paresis, transient and/or permanent hypocalcemia or hypothyroidism, hematoma, seroma, dysphonia, with OR 1.20 (0.20-7.22), P = .84. 4 They did not report on the risk of RNL injury separately. A RCT conducted in 2009 compared the LigaSure© to Harmonic© and conventional cautery, and found the operative safety was similar for all 3 methods of cautery. 8 Overall, 2 cases of transient vocal cord palsies were observed in this study with no significant differences between groups. 8 Another RCT conducted in 2012 assessed LigaSure© versus conventional suture ligation and also found no significant differences in complications. 9 Two patients in the LigaSure© group suffered a transient RLN palsy that was not significant. 9
There are other factors that can be considered when choosing the optimal type of cautery for thyroid surgery. Cost-effectiveness of alternative sources of cautery compared to traditional cautery should be a priority in our current healthcare system climate. A systematic review published in 2016 reported that compared to conventional techniques, Harmonic devices reduced total reported costs by 10% (P = .007), with a large portion of the overall savings derived from a reduction in operative costs (in part as a function of decreased operative time). 10 Another systematic review and meta-analysis published in 2010 concluded that there was no difference in total cost in hospital (P = 0.08) between ultrasonic coagulator and conventional techniques. 11 Availability of hospital resources and surgeon comfort and preference should also factor into choice of optimal cautery source.
Limitations
This study was based off of the NSQIP database, which is associated with inherent limitations. The main limitation of this study is potential confounding effects of variables not captured in the NSQIP database. The NSQIP database has no identifiers. Therefore, we are unable to determine the location the data have come from, the volume of cases performed at centers submitting data, or the duration of time the centers submitting data have been using these alternative sources of cautery. Other limitations include information bias from reliance on retrospective data, and the relatively recent addition of thyroid-specific data to the database, limiting collection years to 2016 to 2018. Using this database, we were also unable to decipher whether or not the RLN injury reported was transient or permanent.
Strengths
The large sample size derived from the NSQIP database which receives data from centers worldwide is a key strength to this article.
Conclusion
In summary, this retrospective risk-adjusted analysis using NSQIP did not find a statistically significant difference in RLN injury in thyroid surgery performed using alternative sources of cautery when compared to traditional sources. According to our dataset, the risk of RLN injury should not be factored in when deciding what source of cautery to use. It is possible that sites performing higher volume of cases have lower complication rates; however, this information is not extractable from our database. There is typically a learning curve with new devices and this may not be captured in these data. Other factors including operating room resources, cost-effectiveness, and surgeon comfort may be more applicable.
Footnotes
Acknowledgements
Ranjeeta Mallick, BSc, MSc, MSc, PhD, Senior Statistician, the Ottawa Method Center, the Ottawa Hospital Research Institute.
Author Contributions
Dr Corliss A. E. Best was first author and wrote the majority of the manuscript; Dr Jumana Hussain helped with project design, data interpretation, and writing the methods portion of the manuscript; Dr Stephanie Johnson-Obaseki was the senior author and was responsibility for concept creation and significant editing to the manuscript.
Availability of Data and Materials
Data were gathered using the National Surgical Quality Improvement Program (NSQIP) database.
Consent for Publication
Consent was given by all authors to submit this article for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study did not require institution ethical approval as National Surgical Quality Improvement Program (NSQIP) data is exempt from the Ottawa Hospital REB as it uses deidentified data.