
Abstract
Background
The aim of this study is to describe the management and associated follow-up strategies adopted by thyroid surgeons with different surgical volumes when loss of signal (LOS) occurred on the first side of planned bilateral thyroid surgery, and to further define the consensus on intraoperative neuromonitoring (IONM) applications.
Methods
The International Neural Monitoring Study Group (INMSG) web-based survey was sent to 950 thyroid surgeons worldwide. The survey included information on the participants, IONM team/equipment/procedure, intraoperative/postoperative management of LOS, and management of LOS on the first side of thyroidectomy for benign and malignant disease.
Results
Out of 950, 318 (33.5%) respondents completed the survey. Subgroup analyses were performed based on thyroid surgery volume: <50 cases/year (n = 108, 34%); 50 to 100 cases/year (n = 69, 22%); and >100 cases/year (n = 141, 44.3%). High-volume surgeons were significantly (P < .05) more likely to perform the standard procedures (L1-V1-R1-S1-S2-R2-V2-L2), to differentiate true/false LOS, and to verify the LOS lesion/injury type. When LOS occurs, most surgeons arrange otolaryngologists or speech consultation. When first-side LOS occurs, not all respondents decided to perform stage contralateral surgery, especially for malignant patients with severe disease (eg, extrathyroid invasion and poorly differentiated thyroid cancer).
Conclusions
Respondents felt that IONM was optimized when conducted under a collaborative team-based approach, and completed IONM standard procedures and management algorithm for LOS, especially those with high volume. In cases of first-site LOS, surgeons can determine the optimal management of disease-related, patient-related, and surgical factors. Surgeons need additional education on LOS management standards and guidelines to master their decision-making process involving the application of IONM.

Keywords
Background
Intraoperative neuromonitoring (IONM) is one of several important technological advances for thyroid and parathyroid surgery1-7 and is gaining acceptance and increasing use by thyroid surgeons.8-10 In a survey published in 2020, Feng et al 11 investigated the use of IONM among 1015 thyroid surgeons, and 83% of respondents reported using IONM. The use of IONM by surgeons is gradually increasing compared to previous studies12,13 due to increased surgeon confidence, improved safety, and improved ability to determine the functional status of the recurrent laryngeal nerve (RLN).14-16
During IONM of the RLN in thyroid surgery, measures of laryngeal electromyography (EMG) amplitude can correlate with RLN function and be helpful in predicting the outcome of vocal cord movement.17,18 According to the 2011 and 2018 International Neural Monitoring Study Group (INMSG) guidelines,1,19,20 the basic criteria for loss of signal (LOS) are (1) an EMG change from an initially satisfactory EMG (the optimal normative baseline, more than 500 µV), (2) absence of response or low response (ie, 100 µV or less) to 1 to 2 mA stimulation on a dry field, and (3) loss of laryngeal twitch and/or glottis movement (Supplemental Table 1). All these INMSG guidelines recommend consideration of staging contralateral surgery in setting the levels of signal. However, there is still obvious heterogeneity among thyroid surgeons in the use of IONM and its efficacy in preventing RLN dysfunction and interpreting EMG signals.21-23 Regarding surgeons’ attitude toward contralateral surgery in cases of LOS after completion of thyroidectomy on the first side, most surgeons (up to 58%) continue with contralateral side surgery in some studies.11,13 It has been suggested that the level of experience with IONM may be related to the choice of surgical staging. 11
Factors influencing adherence to the INMSG guidelines may include familiarity with IONM in the service institution and region and the adequacy of training resources. Studies have shown that thyroid surgeons aged ≤45 years or who have performed thyroid surgery for ≤15 years are more likely to use IONM routinely, including some young high-volume thyroid surgeons in academic centers. 11 The purpose of this study was to describe the treatment and follow-up strategies used by thyroid surgeons worldwide when LOS occurs on the first side during planned bilateral thyroid surgery.
Methods
The survey was piloted by the INMSG Board between September 2020 and December 2020. The online survey (Google Form; https://docs.google.com/forms/d/e/1FAIpQLSfZVuJyeQE1XhjxkyGFzt4Cww029hJdpo-DAhHuVZnvd-aGVw/viewform?usp=sf_link) was administered by sending an email request from January 2021 to June 2021. The survey was designed in English to avoid the complexity of translating the questionnaire for all communities. The participant (one email address) can only submit one survey report. The online questionnaire was also distributed via a link through social networks such as Line group, LinkedIn, Facebook, and WhatsApp. The survey could be accessed by computer, laptop, or smartphone. If necessary, interested individuals who responded to calls for participants were given instructions on how to complete and submit the questionnaire online. Participant confidentiality was maintained throughout the research process.
The content of this survey is shown in Supplemental Figures 1 and 2. The questionnaire was divided into 7 sections and took approximately 15 minutes to complete. The sections were as follows: (1) background information of participants, (2) IONM team and equipment, (3) frequency of performing IONM procedures for total thyroidectomy patients, (4) consequences of intraoperative loss of EMG signal, (5) postoperative follow-up and management after intraoperative LOS, and (6-7) LOS management on the first side of thyroid resection during thyroid surgery for (6) benign and (7) malignant disease.
Subgroup analyses of the survey results were performed based on thyroid surgery volume: <50 cases/year; 50 to 100 cases/year; and >100 cases/year. Chi-square tests of independence were used to compare nominal qualitative variables. Significance was attributed to P values <.05. The statistical analysis was performed using SPSS Statistics version 26.0 (IBM).
Results
Background Information of Participants
A total of 318/950 (33.5%) respondents from around the world completed the survey. Background information including the location and specialty of the respondents is shown in Supplemental Table 2, and a detailed list and distribution of the respondents’ country of practice are shown in Supplemental Figure 3.
Demographic Information of Respondents and the Experience of Using IONM
The results are shown in Supplemental Table 3. Among the 318 respondents, 80.5% were male, the mean age was 47.7 ± 9.6 years, and 70.4% had >10 years of surgical experience. The 318 respondents were divided into 3 subgroups according to their annual thyroid surgery volume: <50 cases/year (108 respondents, 34.0%); 50 to 100 cases/year (69 respondents, 21.7%); and >100 cases/year (141 respondents, 44.3%). In the high surgical volume group, there were more respondents who were male (P = .004), older (P < .001), and had more than 10 years of surgical experience (P < .001). Ninety-three (29.2%) respondents had used IONM for 10 years or more, with the high surgical volume group significantly more likely to have used IONM (P < .001). All respondents used IONM to some extent, while 231 (72.6%) respondents used IONM in selected cases and 87 (27.4%) respondents used IONM routinely in all cases.
The IONM Team and the Respondent Equipment
The results are shown in Table 1. A total of 77.4%, 25.5%, and 7.5% of respondents used monopolar probes, bipolar probes, and stimulating dissection instruments as intermittent IONM (I-IONM) stimulation methods, respectively. The choice of high-volume surgeons was not significantly different from other groups. A total of 149 (46.9%) respondents used continuous monitoring (C-IONM) clinically, of which 137 (91.9%), 19 (12.8%), and 3 (2.0%) respondents used vagus nerve (VN) electrode, stimulating dissection instruments, and laryngeal adductor reflex (LAR) stimulation method, respectively. High-volume surgeons had a significantly higher proportion of patients using vagal nerve electrode (P < .001). A total of 63.8%, 36.8%, 8.8%, 1.9%, and 6.0% of respondents used prefabricated EMG endotracheal tubes (ETTs), regular ETTs with EMG adhesive electrodes, palpation of laryngeal twitch responses, intramuscular electrodes in vocalis muscles, and needles or adhesive electrodes on thyroid cartilage, respectively. The choice of high-volume surgeons was not significantly different from other groups.
Respondent’s IONM Team and Equipment.

Abbreviations: AITD, autoimmune thyroid disease; EMG, electromyography; ETT, endotracheal tube; IONM, intraoperative neuromonitoring; LAR, laryngeal adductor reflex.
Multiple choice is available.
Frequency of Performing IONM Procedures for Total Thyroidectomy Patients
The results are shown in Table 2. The proportions of respondents who always performed the IONM procedures L1, V1, R1, S1, S2, R2, V2, and L2 were 61.0%, 57.5%, 81.1%, 25.5%, 23.3%, 76.4%, 65.1%, and 43.1%, respectively. The proportion of high-volume surgeons performing V1 and V2 was not significantly different from the other groups. High-volume surgeons performed significantly more L1 (P = .005), R1 (P < .001), S1 (P < .001), S2 (P = .001), R2 (P < .001), and L2 (P = .046) procedures.
Frequency of Performing IONM Procedures for Total Thyroidectomy Patients.
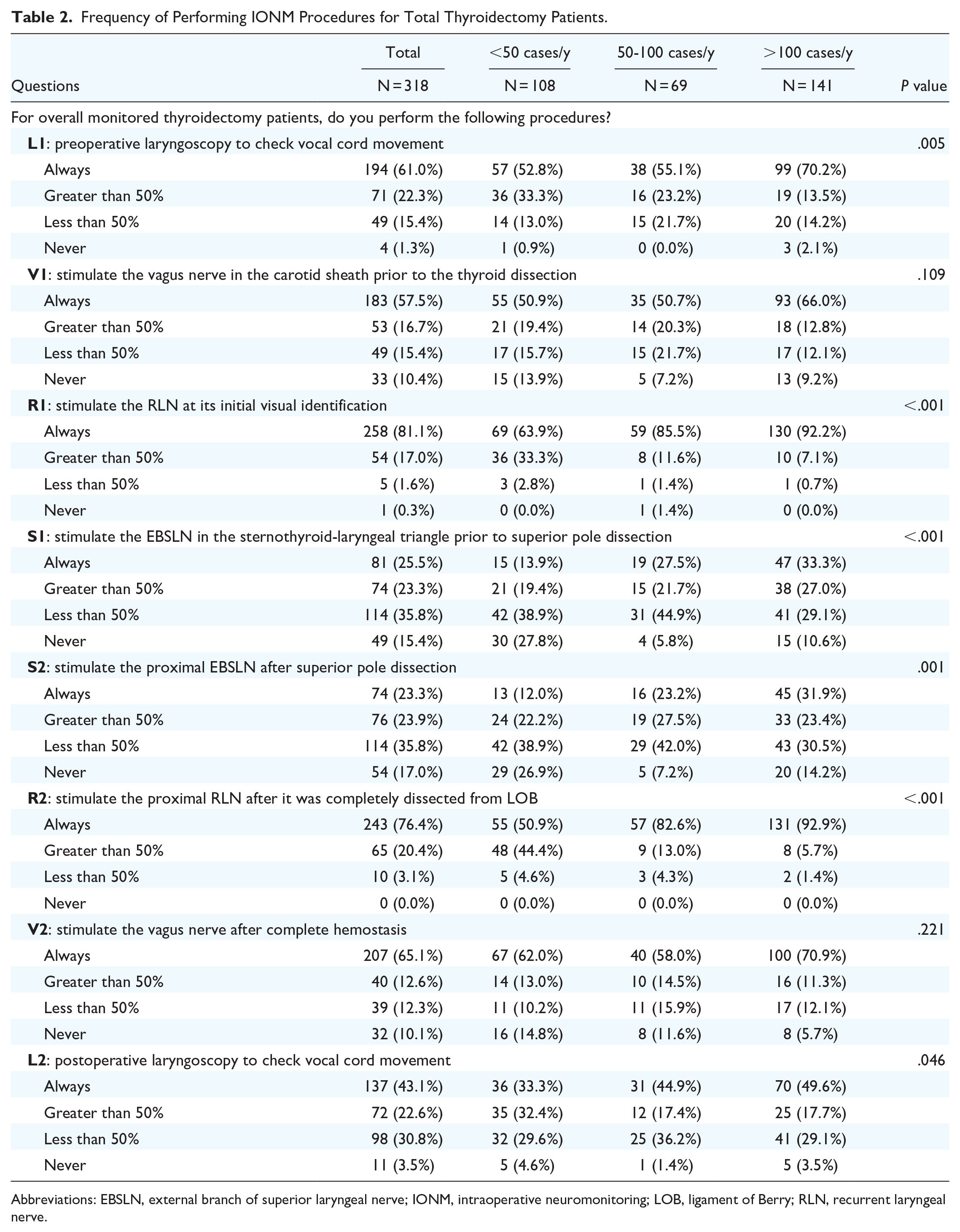
Abbreviations: EBSLN, external branch of superior laryngeal nerve; IONM, intraoperative neuromonitoring; LOB, ligament of Berry; RLN, recurrent laryngeal nerve.
Consequences From Intraoperative LOS
The results are shown in Table 3. When total thyroidectomy was performed, LOS occurred on the first surgical side, and the proportion of surgeons who would perform the following procedures to differentiate true/false LOS was as follows: presence of a laryngeal twitch (71.4%), EMG response from contralateral VN stimulation (71.7%), evaluation for monitoring equipment dysfunction (interface-connector box; 98.1%), evaluation for incorrect use of neuromuscular blocking agents (88.1%), and malposition of recording electrodes (ie, EMG tube; 97.2%).
Consequences From Intraoperative Loss of EMG Signal.
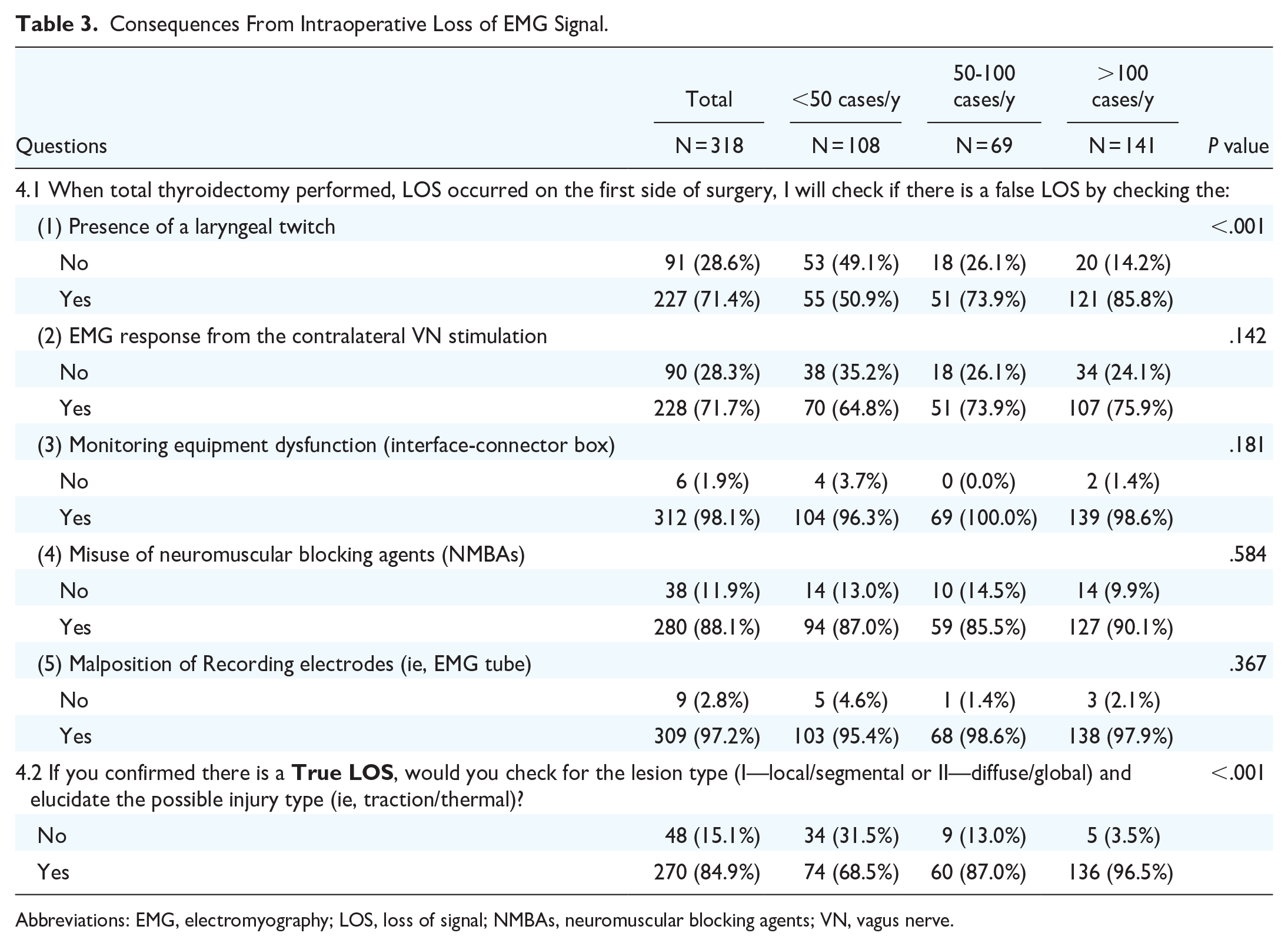
Abbreviations: EMG, electromyography; LOS, loss of signal; NMBAs, neuromuscular blocking agents; VN, vagus nerve.
In total, 84.9% of respondents checked the lesion type (I—local/segmental or II—diffuse/global) and elucidated the possible injury type (ie, traction/thermal) when a true LOS occurred, and the rate was significantly higher in the high surgical volume group (P < .001).
Postoperative Follow-Up and Management After Intraoperative LOS
The results are shown in Table 4. In the question “What treatment do you give the patient with intraoperative LOS?” the respondents tended to refer to speech-language pathologists (SLPs): 53.5% only referred patients with confirmed vocal cord paralysis (VCP), 36.2% referred patients with subjective voice change (with/without VCP), and 15.1% referred all patients (with/without voice change or VCP). The respondents tended to give steroids to affected patients: 37.7% only gave steroids to patients with confirmed VCP, 24.5% gave steroids to patients with subjective voice change (with/without VCP), and 22.6% gave steroids to all patients (with/without voice change or VCP). The choice of high-volume surgeons was not significantly different from other groups.
Postoperative Follow-Up and Management After Intraoperative LOS.
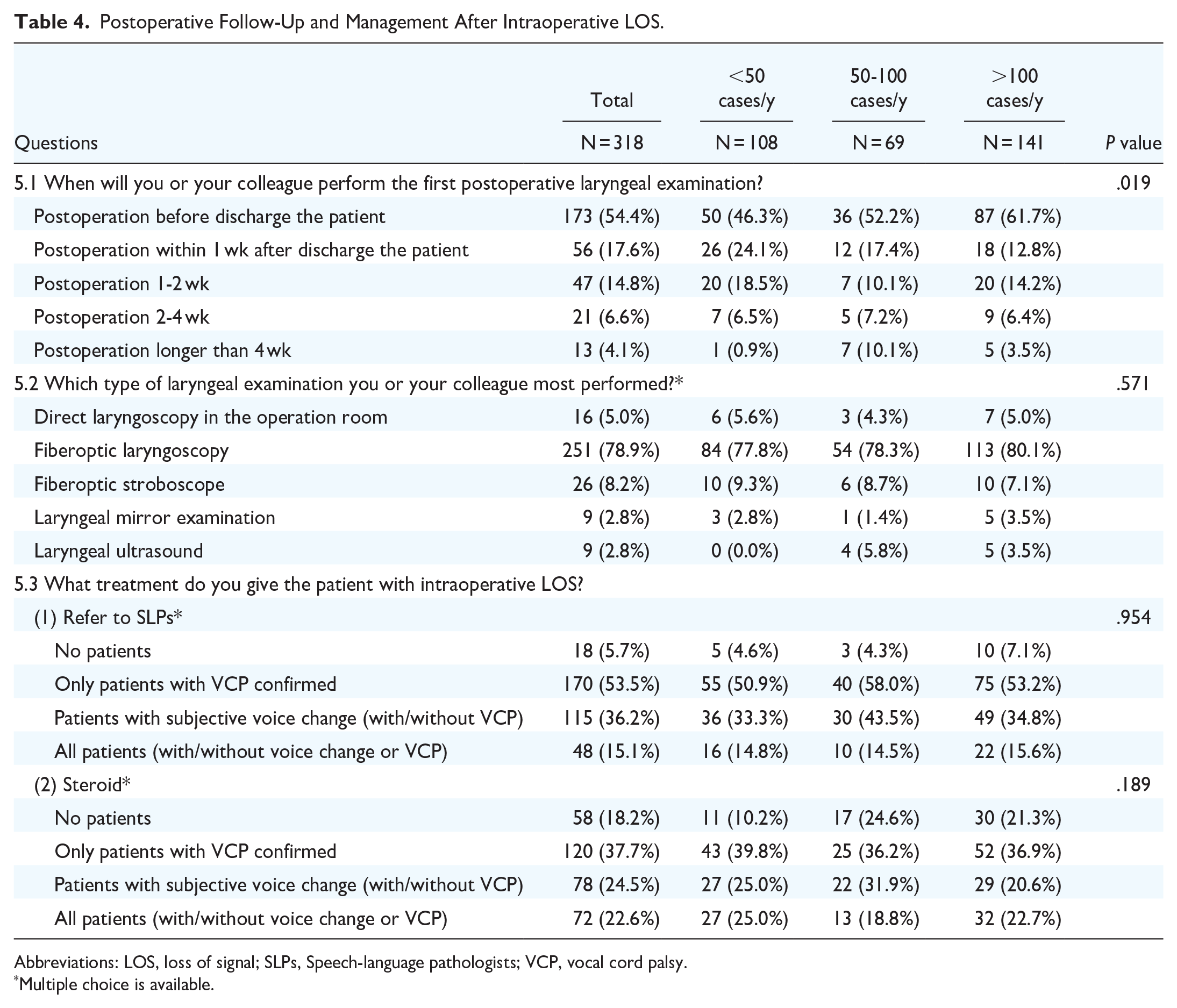
Abbreviations: LOS, loss of signal; SLPs, Speech-language pathologists; VCP, vocal cord palsy.
Multiple choice is available.
LOS Management on the First Side of Thyroid Resection During Thyroid Surgery for “Benign” Disease
If LOS persisted after hemithyroidectomy on the first side in benign cases, the main strategy choice for all respondents is presented in Figure 1A and Supplemental Figure 4A. Surgeons tended to perform stage contralateral surgery (55%-81%) when LOS persisted after hemithyroidectomy on the first side in all scenarios. In addition, small proportion of respondents did not choose stage contralateral surgery as a management strategy.
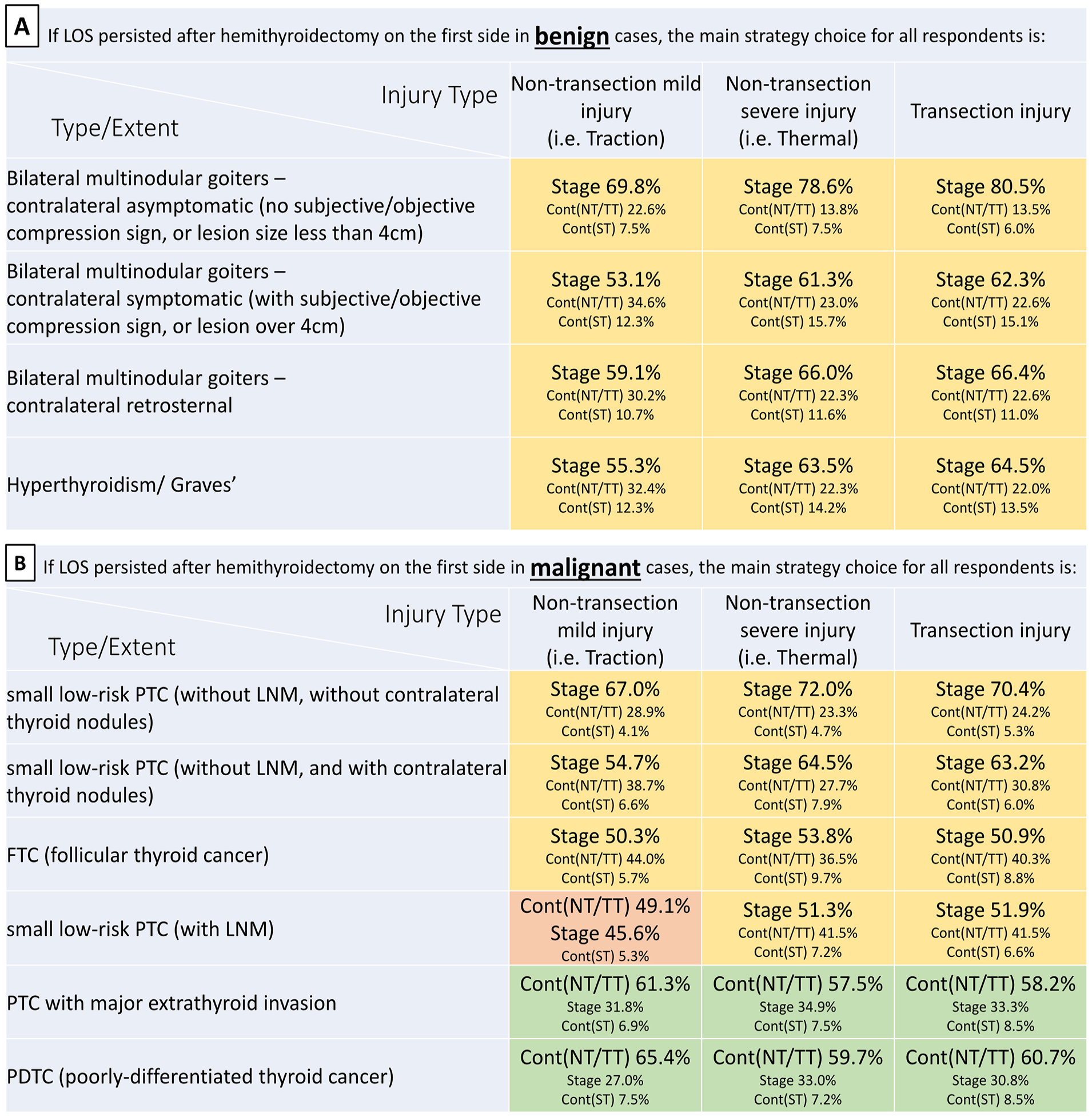
The main strategy choice for all respondents for LOS management on the first side of thyroidectomy for (A) benign and (B) malignant disease. Stage, stage contralateral surgery; Cont (NT/TT), continue carefully with total or near-total thyroidectomy on the second side; Cont (ST), continue carefully with subtotal thyroid resection on the second side; LOS, loss of signal.
The results of questions 6.1 to 6.4 are shown in Table 5. A total of 87.4% of respondents routinely started the surgery from the dominant site. To evaluate the need for completion thyroidectomy, 91.2%, 72.6%, and 56.0% of respondents considered disease-related factors, patient-related factors, and surgical factors, respectively. A total of 61.9% of respondents would perform the planned completion thyroidectomy as soon as possible when there was laryngeal recovery before patient discharge. In the aforementioned questions, the choice of a high-volume surgeon was not significantly different from the other groups.
LOS Management on the First Side of Thyroid Resection During Thyroid Surgery for “Benign” Disease.
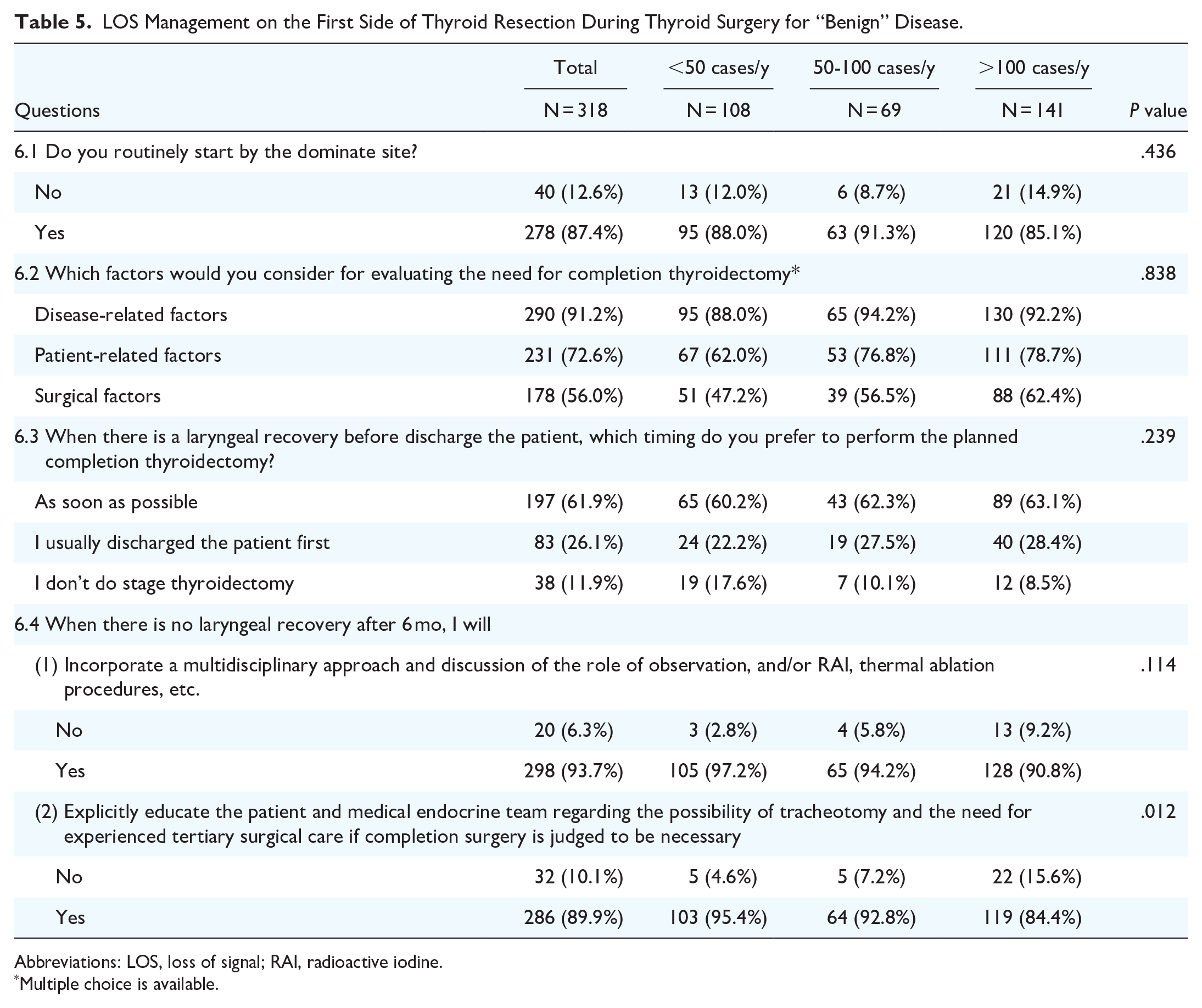
Abbreviations: LOS, loss of signal; RAI, radioactive iodine.
Multiple choice is available.
When there was no laryngeal recovery after 6 months, 93.7% of respondents would incorporate a multidisciplinary approach and discuss the role of observation and/or radioactive iodine (RAI), thermal ablation procedures, etc. A total of 89.9% of respondents explicitly educated the patient and medical endocrine team regarding the possibility of tracheotomy and the need for experienced tertiary surgical care if completion surgery was judged to be necessary.
LOS Management on the First Side of Thyroid Resection During Thyroid Surgery for “Malignant” Disease
If LOS persisted after hemithyroidectomy on the first side in malignant cases, the main strategy choice for all respondents is presented in Figure 1B and Supplemental Figure 4B. When the malignancy is small low-risk papillary thyroid cancer (PTC) or follicular thyroid carcinoma (FTC), respondents tend to perform stage contralateral surgery (50%-70%) when the LOS persists after hemithyroidectomy on the first side. However, a large proportion of respondents do not choose stage contralateral surgery as management strategy when the malignant disease is PTC with major extrathyroidal extension or poorly differentiated thyroid cancer (PDTC). Carefully continuing with total/near-total thyroidectomy on the second side is the main choice when respondents do not perform stage contralateral surgery.
The results of questions 7.1 to 7.4 are shown in Table 6. A total of 89.3% of respondents routinely started surgery from the dominant site. To evaluate the need for completion thyroidectomy, 97.5%, 66.4%, and 51.6% of respondents considered disease-related factors, patient-related factors, and surgical factors, respectively. A total of 61.9% of respondents would perform the planned completion thyroidectomy as soon as possible when there was laryngeal recovery before patient discharge. In the aforementioned questions, the choice of a high-volume surgeon was not significantly different from the other groups.
LOS Management on the First Side of Thyroid Resection During Thyroid Surgery for “Malignant” Disease.

Abbreviations: LOS, loss of signal; RAI, radioactive iodine.
Multiple choice is available.
When there is no laryngeal recovery after 6 months, 89.6% of respondents would incorporate a multidisciplinary approach and discussion of the role of observation, RAI, and/or external beam radiation, and 95.0% of respondents would explicitly educate the patient and medical endocrine team regarding the possibility of tracheotomy and the need for experienced tertiary surgical care if completion surgery is judged to be necessary.
Discussion
The application of IONM in thyroid surgery is well established and increasingly accepted around the world.1,19,20,24 The use of IONM for anatomical identification of the RLN and assessment of RLN injury and to reduce the risk of temporary and permanent RLN paralysis are common motivations for surgeons to use IONM. Standardized IONM procedures were advocated to eliminate false IONM results and elucidate the mechanism of RLN injury.9,25,26 By ascertaining surgical pitfalls and changing the nerve approach, IONM can contribute to the improvement of surgical techniques. The aim of this study is to describe and analyze the differences in surgical practices among surgeons with different surgical volumes and to further define the consensus on IONM applications and LOS management. Several issues are worth discussing:
1. IONM equipment: In I-IONM stimulation, a monopolar probe (used by 77.4% of respondents) is used to provide diffuse current spread, promoting mapping of a larger area; a bipolar probe is used to provide greater sensitivity through focal nerve stimulation; stimulating and dissection instruments27,28 are an emerging real-time I-IONM (used by 7.5% of respondents), reduce the need for tool changes and increase the monitoring frequency, approximating continuous stimulation. C-IONM stimulation29,30 often requires the use of a vagal nerve probe (used by 43.1% of respondents), which allows rapid detection of nerve injury by monitoring second-by-second signal changes to adjust surgical steps. LAR 31 is a novel and promising monitoring method (used by 0.9% of respondents) that requires the use of an ETT electrode to stimulate the laryngeal mucosa to evoke a brainstem reflex, which eliminates the need for probe implantation except for the EMG ETT. The most common recording methods are commercialized prefabricated EMG ETTs or regular ETTs with EMG adhesive, where the EMG signal is recorded by ETT-based electrode in contact with the vocalis muscle. Alternatively, palpation of the laryngeal twitch response and intramuscular electrodes in the vocalis muscle are still used by some surgeons in selected situations. Needles or adhesive electrodes on the thyroid cartilage (used by 6.0% of respondents) offer the advantage of high signal stability and no need to check the ETT position,32-35 which is a newly added cost-effective and stable option for EMG recording.
2. Confirmation of true/false LOS: For LOS patients, the surgeon should consider the optimal timing of contralateral surgery for total thyroidectomy patients with planned bilateral thyroid operations to avoid bilateral VCP.24,36 However, LOS recovery and false LOS may occur and may lead to an unnecessary second operation. Several studies have developed a management algorithm for neural monitoring troubleshooting,1,37,38 which provides a reliable modality for intraoperative LOS evaluation and management that would provide the surgeon with real-time information that could help guide surgical procedures and planning. After years of advocacy, surgeons would choose more than one method to differentiate true/false LOS, and high-volume surgeons were more likely to perform each differentiation method (Table 3).
3. Confirmation of RLN injury lesion and type: During thyroid surgery, transection, clamping, ligature, thermal, compression, and traction can cause RLN injury. Chiang et al 7 first described the possible mechanisms of RLN injury during monitored thyroidectomy in 2008 and classified traction/stretch injury into type I (local/segmental) and II (diffuse/global) injuries. In the current study, 84.9% of the respondents checked the mechanism and type of RLN injury, and even more, 96.5% of the high-volume surgeons did so (Table 3).
4. Postoperative LOS management: Post-thyroidectomy voice evaluations and intervention are gradually being emphasized, and some studies have suggested routine voice analysis and early voice intervention with a multidisciplinary approach (including SLP).39-41
5. The incorporation of true LOS into the surgical strategy of a planned bilateral thyroidectomy: This is one of the cornerstones of several INMSG guidelines as it is considered a benefit of neural monitoring in that it helps circumvent the need for a bilateral procedure and possible tracheotomy.
IONM improves the identification of intraoperative RLN injury, especially in normal-appearing but nonfunctioning nerves after surgery on the first side. 42 In many studies, researchers agree that IONM can have a significant impact on decision-making for contralateral surgery after unilateral paralysis, with the avoidance of bilateral VCP being the primary consideration.4,36,42-44 In our study, we were surprised to identify that, for both benign and most malignant cases despite LOS survey, respondents would proceed with contralateral surgery, a surgical strategy that does not incorporate the ipsilateral LOS according to the INMSG guidelines. In the current study, the effect of surgical volume and surgical strategy was not significant. However, disease factors have a prominent impact on surgical strategy, particularly with surgeons tending to continue carefully with total/near-total thyroidectomy on the second side in cases of more severe malignant disease (eg, major extrathyroid extension and PDTC) and tending to undertake stage surgery for benign cases or small low-risk PTC or FTC. Benign/malignant disease factors have been reported in the literature to influence surgical decisions. 4 Barczyński et al 45 also reported that 48% and 77% of surgeons recommend staging or changing contralateral surgical extent in malignant and benign cases, respectively. Wu et al 43 conducted a study that analyzed the surgical data of 803 thyroid procedures. Staged surgery was recommended for bilateral goiter, Graves’ disease, or low-risk thyroid carcinoma (differentiated and medullary thyroid carcinomas) and was performed on 85% of patients with first-sided LOS. Total thyroidectomy was recommended for advanced thyroid carcinoma (including undifferentiated thyroid carcinoma) and was performed on 15% of patients with first-side LOS.
Standardized IONM procedures, discrimination of true LOS, and assessment of injury severity and mechanism allow surgeons to better understand the potential nature of neural recovery and make appropriate treatment decisions.1,19,20 Dralle et al 36 reported that in IONM-assisted thyroid surgery with first-sided LOS, 84.7% of surgeons would choose unilateral surgery and 8.8% would intentionally reduce the surgical extent on the contralateral side to avoid dissection near the RLN. Contralateral subtotal thyroidectomy is considered a treatment strategy to avoid increasing the risks of disease recurrence and revision surgery; however, none of the thyroid procedures performed in this particular strategy in the study by Wu et al. 43 This strategy was not used in any of the thyroid procedures nor was it preferred in our current study in depending on the different scenarios of benign or malignant disease (Supplemental Figure 4A and B). The RLN injury mechanism is related to postoperative neural function (transient/permanent paralysis), permitting consideration of whether it is important and in the best interest of the patient to perform surgery on the contralateral side on the same day.4,42 In the current study, in the case of non-transection mild injury (ie, traction) in patients with small low-risk PTC with lymph node metastasis, 49.1% of surgeons chose carefully to continue with total/near-total thyroidectomy on the second side, and the decision was based on the injury mechanism and comprehensive consideration of disease pathology. Surgeons tend to take into account all factors (disease/patient/surgical) and choose the most suitable strategy for the patient, with disease factors being the highest priority among them.
Considering the natural course of nerve recovery and the importance of not delaying cancer treatment, 61.9% of surgeons in this study would perform the planned thyroidectomy as soon as possible after the larynx has recovered. Completion surgery on the contralateral side in patients with ongoing ipsilateral nerve injury can still be recommended but should be performed by a surgeon with sufficient experience,36,46 and informed consent must be obtained from the patients. 15 If the RLN injury has not recovered within 6 months, a multidisciplinary team approach is suggested,43,44 including the role of observation, RAI, and/or external beam radiation. For these patients with permanent unilateral VCP (>6 months), referral to an experienced surgeon is recommended if contralateral surgery is indicated,4,42 and 95.0% of surgeons in the current study supported this management recommendation.
Since 2015, according to the American Thyroid Association Management Guidelines, 47 intrathyroidal PTC or low-risk FTC may be amendable to total lobectomy or total thyroidectomy, and completion thyroidectomy is not always needed. In the 2018 INMSG guidelines, 19 stage contralateral surgery is optimal for patients with benign thyroid disease and low-risk thyroid cancer who are medically suitable for second anesthesia. 48 Continued contralateral surgery should rarely be considered, and is largely reserved for patients with high-risk disease requiring urgent surgical treatment and those for whom second anesthesia poses a significantly higher medical risk, and a complete lobectomy is mostly performed. 19 In the 2018 INMSG guidelines, there are 2 recommendations for staging bilateral thyroid surgery with LOS monitoring. First, IONM information should be obtained and utilized in the strategy of a planned bilateral procedure by staging the surgery in the setting of ipsilateral LOS. It should be shared and discussed with the patient during the preoperative informed consent process.15,19 Second, a surgeon should prioritize concern for the obvious significant medical and psychological morbidity of bilateral VCP and possible tracheotomy (even temporary) over perceived surgical convenience, the routine of performing the “planned procedure,” or the potential perceived impact on surgical reputation by openly acknowledging the surgical complication of ipsilateral LOS. The full benefit of neural monitoring information in this surgical setting is appreciated by both optimizing patient quality of life and decreasing surgical costs. Specific training on IONM devices and procedures can significantly shorten the learning curve for surgeons considering introducing IONM into their practice. The INMSG has issued a consensus statement on training courses for IONM applications in thyroid and parathyroid surgery. 9 In the current study, when first-side LOS is occurred, not all respondents were inclined to stage contralateral surgery even for benign disease. Surgeons need additional education on LOS management standards and guidelines to master their decision-making process involving the application of IONM.
There are several limitations of the current study. One limitation of this study is the occurrence of nonresponder bias. We utilized several large organizations with their extensive membership lists and sent out the survey. As with all survey studies, it is subject to responder bias. There is still heterogeneity due to experience and the institutional environment among high-volume surgeons. Furthermore, due to the format of the questionnaire, using surgical volume as the primary parameter to differentiate surgeons’ experience inevitably has limitations. Surgeons with different surgical volumes may make the same choices for completely different reasons, leading to biases that make differences between groups less noticeable. In addition, regardless of surgical volume, confidence in the technique could influence the surgeon’s intraoperative decision. This is an important factor in the intraoperative decision to complete a planned total thyroidectomy or to perform staged completion surgery, in addition to patient and disease-related factors.
Conclusions
The teamwork, IONM standard procedures, and management algorithm of LOS were admired by most surgeons, especially the high-volume surgeons. In addition, when first-sided LOS is performed, most surgeons can make the optimal management decisions based on disease-related factors, patient-related factors, and surgical factors. Surgeons need additional education on LOS management standards and guidelines to master their decision-making process involving the application of IONM.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216241265684 – Supplemental material for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery
Supplemental material, sj-docx-1-ohn-10.1177_19160216241265684 for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery by Tzu-Yen Huang, Hsin-Yi Tseng, Francesco Frattini, Marika D. Russell, Amr H. Abdelhamid Ahmed, Frank Weber, Paulina Wierzbicka, I-Cheng Lu, Kwang Yoon Jung, Özer Makay, Young Jun Chai, Feng-Yu Chiang, Rick Schneider, Marcin Barczyński, Henning Dralle, Gregory W. Randolph, Che-Wei Wu and Gianlorenzo Dionigi in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-tif-2-ohn-10.1177_19160216241265684 – Supplemental material for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery
Supplemental material, sj-tif-2-ohn-10.1177_19160216241265684 for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery by Tzu-Yen Huang, Hsin-Yi Tseng, Francesco Frattini, Marika D. Russell, Amr H. Abdelhamid Ahmed, Frank Weber, Paulina Wierzbicka, I-Cheng Lu, Kwang Yoon Jung, Özer Makay, Young Jun Chai, Feng-Yu Chiang, Rick Schneider, Marcin Barczyński, Henning Dralle, Gregory W. Randolph, Che-Wei Wu and Gianlorenzo Dionigi in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-tif-3-ohn-10.1177_19160216241265684 – Supplemental material for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery
Supplemental material, sj-tif-3-ohn-10.1177_19160216241265684 for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery by Tzu-Yen Huang, Hsin-Yi Tseng, Francesco Frattini, Marika D. Russell, Amr H. Abdelhamid Ahmed, Frank Weber, Paulina Wierzbicka, I-Cheng Lu, Kwang Yoon Jung, Özer Makay, Young Jun Chai, Feng-Yu Chiang, Rick Schneider, Marcin Barczyński, Henning Dralle, Gregory W. Randolph, Che-Wei Wu and Gianlorenzo Dionigi in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-tif-4-ohn-10.1177_19160216241265684 – Supplemental material for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery
Supplemental material, sj-tif-4-ohn-10.1177_19160216241265684 for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery by Tzu-Yen Huang, Hsin-Yi Tseng, Francesco Frattini, Marika D. Russell, Amr H. Abdelhamid Ahmed, Frank Weber, Paulina Wierzbicka, I-Cheng Lu, Kwang Yoon Jung, Özer Makay, Young Jun Chai, Feng-Yu Chiang, Rick Schneider, Marcin Barczyński, Henning Dralle, Gregory W. Randolph, Che-Wei Wu and Gianlorenzo Dionigi in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-tif-5-ohn-10.1177_19160216241265684 – Supplemental material for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery
Supplemental material, sj-tif-5-ohn-10.1177_19160216241265684 for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery by Tzu-Yen Huang, Hsin-Yi Tseng, Francesco Frattini, Marika D. Russell, Amr H. Abdelhamid Ahmed, Frank Weber, Paulina Wierzbicka, I-Cheng Lu, Kwang Yoon Jung, Özer Makay, Young Jun Chai, Feng-Yu Chiang, Rick Schneider, Marcin Barczyński, Henning Dralle, Gregory W. Randolph, Che-Wei Wu and Gianlorenzo Dionigi in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-tif-6-ohn-10.1177_19160216241265684 – Supplemental material for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery
Supplemental material, sj-tif-6-ohn-10.1177_19160216241265684 for The INMSG Survey on the Loss of Signal Management on the First Side During Planned Bilateral Thyroid Surgery by Tzu-Yen Huang, Hsin-Yi Tseng, Francesco Frattini, Marika D. Russell, Amr H. Abdelhamid Ahmed, Frank Weber, Paulina Wierzbicka, I-Cheng Lu, Kwang Yoon Jung, Özer Makay, Young Jun Chai, Feng-Yu Chiang, Rick Schneider, Marcin Barczyński, Henning Dralle, Gregory W. Randolph, Che-Wei Wu and Gianlorenzo Dionigi in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
The authors would like to thank all respondents for their participation (list alphabetically by the last name): Orhan Agcaoglu, Aslan Ahmadi, Aysegul Aktas, Pier Francesco Alesina, Mohammad AlFalasi, Miguel Allen, Fadi Almahameed, Rajab Alzahrani, Iñaki Amunategui Prats, Eleni Anastasiou, Matteo Annoni, Gian Luca Ansaldo, Cumhur Arici, Akif Enes Arikan, Lia Assumpcao, Andrea Attard, Husnu Aydin, Nurcihan Aygün, Jasung Bae, Seung-Kuk Baek, Marcin Barczynski, Giancarlo Basili, Sylvia Batista, Katrin Bauer, Hans-Guenter Becker, Carlo Bellotti, Nikola Besic, Andrea Borasi, Maurizio Bossotti, Emre Bozkurt, Katrin Brauckhoff, Laurent Brunaud, Carnaille Bruno, Yusuf Bukey, Guldeniz Karadeniz Çakmak, Pietro Giorgio Calò, Jorge A. Calvo, Henrique Candeias, Felipe Capdeville, Patrizio Capelli, Claudio Casella, Maurílio Chagas, Leong-Perng Chan, Tseng Cheng Chen, Yu-Hsien Chen, Kai-Yean Cheng, Maria Grazia Chiofalo, Yi-Fan Chou, Christos Chouliaras, Christos Christoforides, Cheng Hsun Chuang, Calogero Cipolla, Wilhelmina Conradie, Federico Cozzani, Natalia Cuello, Titus Cvasciuc, Aitor De la Quintana, Loredana De Pasquale, Marek Dedecjus, Paolo Del Rio, Rosen Dimov, Maite Domínguez Ayala, Luis Omar Domínguez-Palomera, Gianluca Donatini, Guilherme Duque, Ahmet Cem Dural, Manuel Duran-Poveda, Mete Düren, Enrico Erdas, Varlık Erol, Fausto Famà, Manuel Felices, Dimitrios Gialvalis, Marie-Laure Matthey Giè, Marc Goebel, Erick Gonzales Laguado, Peter E. Goretzki, Giuseppa Graceffa, Pierre Guarino, Tufan Gumus, Angela Gurrado, Deniz Güzey, Mehmet Haciyanli, Jeong Hun Hah, Lutz Hausser, Avi Khafif Hefetz, Hyun Jun Hong, Isabelle Honigman, Li-Jen Hsin, Cheng Hsin Liu, Maurizio Iacobone, Gokhan Icoz, Ahmet Ömer İkiz, William B. Inabnet III, Waldmann Jens, Yong Bae Ji, Milan Jovanovic, Young Ho Jung, Stylianos A. Kapiris, Stavros Karakozis, Hakan Kaya, Dahee Kim, Soo Young Kim, Reinhold Klug, Wolfram Trudo Knoefel, How-Yun Ko, Aleksander Konturek, Ioannis Koutelidakis, Bojan Kovacevic, Robert Králik, Gerasimos Kritikos, Akshay Kudpaje, Marco Kulcsar, Sophocles Lanitis, Kang-Dae Lee, Byung-Joo Lee, Yong Sang Lee, Tsung-Lun Lee, Ennio Leopaldi, Yi-Shing Leu, Jean-Christophe Lifante, Pierre Lindas, Davide Lombardi, Kerstin Lorenz, Patricia Luengo Pierrard, Achilles Alves De Levy Machado, Özer Makay, Alessandro Marchesi, Theodora Margariti, Testini Mario, Jesús Martínez-Salazar, Cristina Martínez-Santos, Juan Manuel Martos-Martinez, Maurice Matter, Fabio Medas, Michael Meier, Giuseppe Mercante, Nickos Michalopoulos, Radu Mihai, Michele Minuto, Akira Miyauchi, Alberto Mobiglia, George Mochloulis, Martina T. Mogl, Dieter Morales-Garcia, Uwe Mueller, José Luis Muñoz de Nova, Rafael Nagato, Konstantinos Nastos, Müller Nicole, Josef Obermeier, Peter O’Leary, Ana Oliveira, İbrahim Özata, Serdar Ozbas, Beyza Ozcinar, Murat Ozdemir, Emre Özoran, Rumen Pandev, Theodosios Papavramidis, Constantinos Parpounas, Alessandro Pasculli, Antonella Pino, Giulia Pinto, Ioannis Pliakos, Andrea Polistena, Alessandro Pontin, Marco Raffaelli, Levan Ramishvili, Greg Randolph, Leonardo Rangel, Tomas Ratia, John Ridge, Serenella Ristagno, Leonardo Rossi, Navin Rudolph, Pavel Rumyantsev, Nuri Alper Sahbaz, Jorge Rosa Santos, Serkan Sarı, Jochen Schabram, Abbey Schepers, Rick Schneider, David Scott-Coombes, Yasemin Şenyürek, Carlos Serra, Atakan Sezer, Mohammad Feras Shalabi, Patrick Sheahan, Yotam Shkedy, Eveline Slotema, Constantin Smaxwil, Samuel K Snyder, Carlos Soares, Ra-Yeong Song, Ismail Cem Sormaz, Juan Soto, Selen Soylu, Stefano Spiezia, Michas Spiros, Jose Higino Steck, Kyung Tae, Alberto Tatti, Hin Ngan Tay, Serkan Teksöz, Serdar Tezelman, Serdar Tezelman, Alfio J. Tincani, Frederic Triponez, Tsung-Yih Tsai, Hsin-Yi Tseng, Yiğit Türk, Mehmet Uludag, Julio Andrés Valencia, Kyriakos Vamvakidis, Klaas Van Den Heede, Sam Van Slycke, Evandro Vasconcelos, Acklei Viana, Oscar Vidal, Jesús Villar-del-Moral, Shih Wei Wang, Chen-Chi Wang, Frank Weber, Theresia Weber, Corinna Wicke, Kai-Pun Wong, Alejandro Yanzon, Hakan Yigitbas, Ali Cihat Yildirim, Petr Ziegler, Andreas Zielke.
Author Contributions
The original idea was conceived, and the study was designed by C.W.W., G.D., F.Y.C., and G.W.R. H.Y.T., F.F., M.D.R., A.H.A.A., I.C.L., and Y.J.C. were responsible for creating and completing the database. F.W., P.W., K.Y.J., Ö.M., R.S., M.B., and H.D. all made valuable contributions and changes to the manuscript leading to its completion. The original manuscript was created by T.Y.H. and C.W.W., and was reviewed and approved by all authors. All authors read and approved the final manuscript.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article (and its supplementary information files).
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from Kaohsiung Medical University Hospital, Kaohsiung Medical University (KMUH111-1R48, KMUH111-1R49, KMUH112-2R50, KMUH112-2R51), and National Science and Technology Council (NSTC112-2314-B-037-033, NSTC 112-2314-B-037-034), Taiwan.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board (IRB) of Kaohsiung Medical University Hospital, Taiwan (KMUHIRB-E(II)-20220196).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.