
Abstract
Background
Minimally invasive cochlear implant surgery by using a microstereotactic frame demands solid connection to the bone. We aimed to determine the stability of commercially available orthodontic miniscrews to evaluate their feasibility for frame’s fixation. In addition, which substitute material most closely resembles the mechanical properties of the human temporal bone was evaluated.
Methods
Pull-out tests were carried out with five different types of orthodontic miniscrews in human temporal bone specimens. Furthermore, short fiber filled epoxy (SFFE), solid rigid polyurethane (SRPU50), bovine femur, and porcine iliac bone were evaluated as substitute materials. In total, 57 tests in human specimens and 180 tests in the substitute materials were performed.
Results
In human temporal bone, average pull-out forces ranged from 220 N to 285 N between screws. Joint stiffness in human temporal bone ranged between 14 N/mm and 358 N/mm. Statistically significant differences between the tested screws were measured in terms of stiffness and elastic energy. One screw type failed insertion due to tip breakage. No significant differences occurred between screws in maximum pull-out force. The average pull-out values of SFFE were 14.1 N higher compared to human specimen.
Conclusion
Orthodontic miniscrews provided rigid fixation when partially inserted in human temporal bone, as evidenced by pull-out forces and joint stiffness. Average values exceeded requirements despite variations between screws. Differences in stiffness and elastic energy indicate screw-specific interface mechanics. With proper insertion, orthodontic miniscrews appear suitable for microstereotactic frame anchoring during minimally invasive cochlear implant surgery. However, testing under more complex loading is needed to better predict clinical performance. For further pull-out tests, the most suitable substitute material is SFFE.

Keywords
Introduction
For patients suffering from sensory deafness or profound hearing loss, a cochlear implant (CI) is the current treatment of choice. 1 Due to extensive research over the past years, indication criteria have been expanded to include patients with higher residual hearing,2-4 unilateral deafness, 5 and asymmetric hearing loss, 6 as well as atypical causes of hearing loss (eg, vestibular schwannoma, 7 Meniere’s disease, 8 and tinnitus 9 ). Especially, patients with residual hearing, mostly elderly patients with underlying diseases and associated higher risk of surgery-related complications, could benefit from a less invasive technique of CI surgery.
The standard procedure for implanting the CI, mastoidectomy posterior tympanotomy approach, is a traumatic and time-consuming surgery that requires extensive removal of the skull bone.10,11 During the surgery, an array of stimulating electrodes is inserted into the cochlea, which ensures the transmission of the electrical pulses to the hearing nerve. In an effort to reduce both intraoperative trauma as well as the duration of surgery, and to increase patient’s safety, minimally invasive approaches of cochlear implantation have been investigated for more than 10 years. However, this approach is still experimental and has not been commonly performed yet.
The main idea of all procedures is to place the electrode array via a single bore-hole directly into the patient’s cochlea, avoiding extensive removal of the skull bone. Since important structures, for example, the facial nerve or chorda tympani, cannot be identified during surgery without resection of the temporal bone; unassisted manual drilling is no option. Several approaches to provide surgeons with the required accuracy in the submillimetric area with a maximum deviation of 0.3 mm 12 have been published: head-mounted systems, 13 stationary robot systems, 14 and microstereotactic frames (MSFs).15-19
The workflow of the last-mentioned frame-based approach includes a bone-anchored fixation with three miniscrews onto the patient’s temporal bone (Figure 1), a segmentation of the patient’s individual anatomy and afterward the customization of an individual jig, that defines the drilling path to the basal turn of the cochlea.20,21 In fact, the fixation of the frame to the skull plays a crucial role in the accuracy of the drilling process. If a rigid fixation is not ensured, the drilling can deviate from the calculated trajectory and hamper electrode insertion or, in the worst case, result in injury of nerval structures.
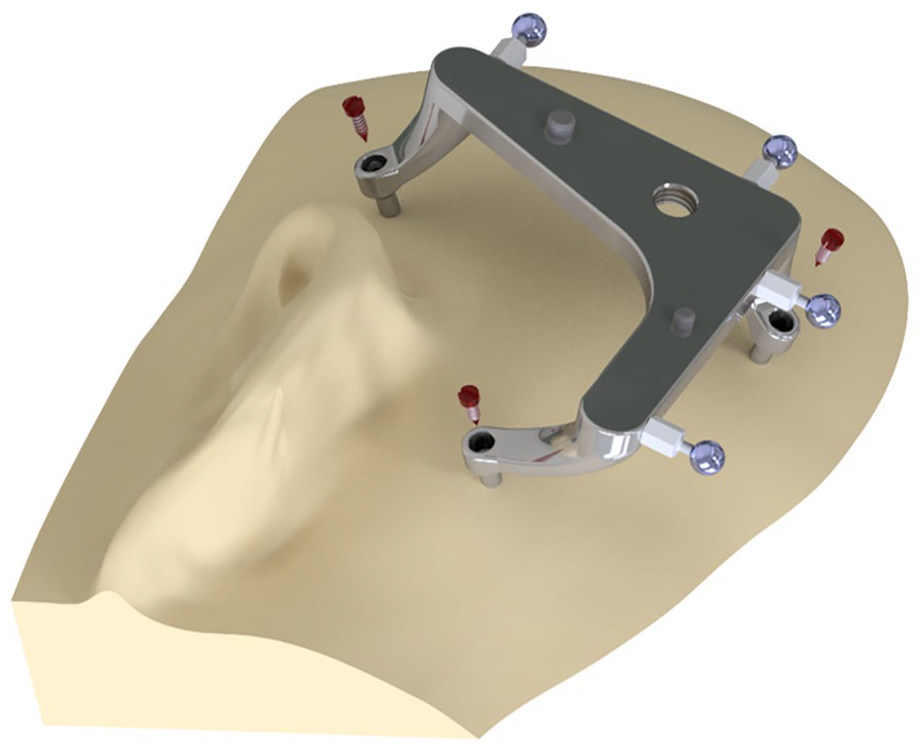
Illustration of the reference frame and fixation with miniscrews.
For this specific application, Labadie et al demonstrated already in 2009 that bone anchors ensure adequate stability, 22 these results were confirmed by Kobler et al. 23 However, experiments with miniscrews from orthodontics have not yet been published.
In this study, we investigated whether sufficient stability for the fixation of MSFs can also be ensured by orthodontic miniscrews which are commercially available and well-established medical products. These miniscrews are widely used in orthodontics as temporary fixation of midface trauma, mandibular fractures, or for the fixation of bone grafts due to their easy surgical insertion and their performance in establishing a solid and rigid connection to the bone.24,25 They were mechanically characterized in several investigations demonstrating a high primary stability26,27 which is important also for minimally invasive CI surgery. However, these miniscrews have never been tested in the mastoid bone and this study aims for filling this lack of knowledge.
Gracco et al showed a high stability at pull-out trails with miniscrews with a mean force of 183.4 N for all tested screws and with a comparable design to those screws investigated in this study. 28 In contrast, Yashwant et al showed lower forces in their pull-out trials with mini-implants ranged from 13.45 N to 61 N tested in sawbone samples 29 but with a significantly lower density than the samples tested in this study. These publications described considerable differences with regard to the stability of mini bone screws. Furthermore, in the aforementioned investigations, the bone screws were placed with their full length of 9 mm to 12 mm into the bone, which deviates from the fixation of the MSF. While it has been experimentally confirmed that a higher insertion depth also leads to greater stability, 30 screw-in depth at the lateral skull base is limited to 3.6 mm to 5 mm due to the limited thickness of the bone as shown in previous measurements with a custom-made software. 31 The insertion depth of the screw for this special purpose is therefore only one-third of the whole screw and a review of literature could not show any experiments in which the miniscrews were only partially inserted into the bone or substitute material. Furthermore, the bone screws for the fixation frame will be placed in the temporal and the parietal bone, which mechanical characterizations differ from the jaw bone.32-34
Due to the aforementioned limitations, a mechanical characterization of the fixation using mini bone screws for this special purpose needs to be performed. In this study, we present the results of the experiments, which aimed to show that a stable and reliable attachment to the lateral skull base is also feasible with mini bone screws.
In addition to the tests in the human temporal bone, pull-out tests were also performed in four different substitute materials. While experiments in human bone specimens provide the most reliable results for the clinical use, suitable substitutes for phantoms or training are also required. In this case, the limited availability of human bone samples is the major problem, as these specimens can only be obtained from body donors. Moreover, human specimens are more difficult to store and prepare. Polyurethan foams, for example, Sawbone®, approximate the biomechanical properties of human bones with little limitations. 35 Studies to replace the human temporal bone have not been performed before. Based on studies related to the miniscrews, in which porcine iliac bone was frequently used as substitute material for the mandibula, this material was also tested. Moreover, bovine femur was included in our experiments, as it is characterized by comparable biomechanical characteristics to the human temporal bone. 36 The main advantage in these cases is the better availability compared to human bone. Storage and preparation require the same effort.
Materials and Methods
Pull-Out Test Setup
The mechanical pull-out testing was performed using a material testing machine (Zwick 1445; ZwickRoell GmbH & Co. KG), equipped with a 10 kN load cell. Recordings of deflection of the screw, applied force, and duration of the test were made with one measuring point per 0.01 mm deflection by the program Zwick PC-Software, V5.72 (ZwickRoell GmbH & Co. KG). The specimens were fixed on a base plate whereupon the screws were inserted 3.6 mm into the respective test material. The correct insertion depth was ensured by a spacer made individually for each screw tested. The spacer was also used to connect the construction to the test machine with a tension ring (Figure 2). Drilling a pilot hole was not required, as all screws are self-drilling. During the mounting of the specimens, attention was paid to a proper alignment of the longitudinal screw axis with the vertical pulling direction of the testing machine. First, a preload in tensile direction of 5 N was applied and held for five seconds. Then the pull-out test was performed at a velocity of 10 mm/min. The primary end point was the complete pull-out of the tested screw. The force-displacement curves were recorded by the software and the maximum force encountered was used for evaluation. The maximum displacement of a screw was defined at 5 mm, if this threshold was exceeded, the pull-out test was stopped. To compensate for the elongation of the steel cable, 19 tests were performed with a fixed screw up to a force of 300 N. Raw data of these trials were averaged and approximated by a fourth degree polynomial regression. In this manner, the elongation of the steel cable during the application of the force was mathematically subtracted. The calibrated displacement only refers to the screw-bone interface. The screws were inserted manually perpendicularly to the bone or sawbone surface up to the limit of the spacer. All screws were tightened to the predetermined depth until a solid connection to the bone was established. A total of 237 pull-out tests were performed in all described materials. In summary, all miniscrews were tested in human temporal bone; however, S1 did not yield interpretable results. S1 was tested in all substitute materials, while S2, S3, S4, and S5 were tested in SFFE and bovine femur as substitute materials. Table 1 summarizes the number of each pull-out test with regard to screw type and material.
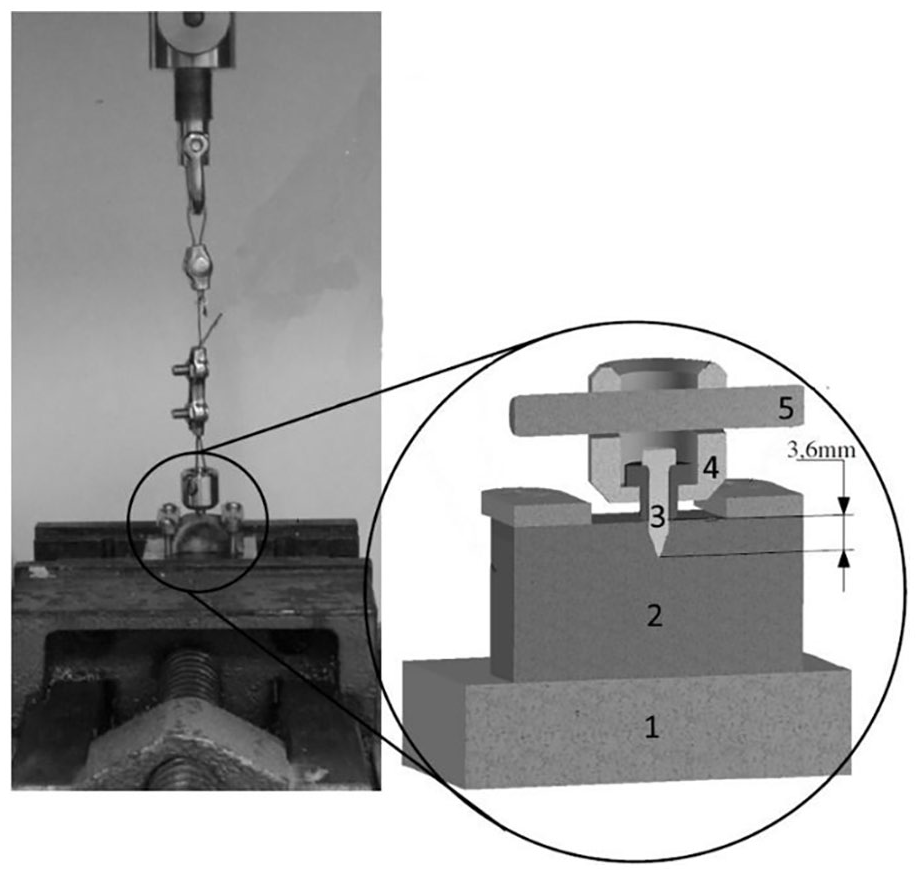
Illustration of the pull-out test setup: 1: baseplate; 2: specimen; 3: screw; 4: spacer; 5: tension ring.
Overview of Number of Performed Pull-Out Tests Per Screw in Each Investigated Material.

Abbreviations: S1: PSM quattro standard; S2: Promedia LeForte; S3: KLS maxdrive drill-free; S4: General Implants mini bone screw; S5: Promedia dual top; SFFE: short fiber filled epoxy; SRPU50: solid rigid polyurethane.
Specification of the Tested Materials
Human temporal bone was tested as reference material since the proposed fixation requires bone anchorage in this part of the skull. After receiving institutional review board approval (Ethics Committee of Hannover Medical School; 3512-2017), all human bone specimens were obtained from anonymized body donors. In addition, 2 artificial bone substitutes materials have been used: “solid rigid polyurethane” (SRPU50; Sawbones Europe) and SRPU with a 1.54 mm layer of short fiber filled epoxy (SFFE; Sawbones Europe). The SFFE was utilized for a realistic simulation of the cortical layer of the temporal bone. 37 In addition, two animal substitute materials were tested, porcine iliac bone and bovine femur. Only the plateau of the distal femur of the bovine femur was used as this part most closely resembles the structure of human bone. 38 All non-synthetic specimens were separated from soft tissue and stored frozen prior to the experiments. The samples were then thawed prior to the experiments which is known to have minor effect on the mechanical properties. 39 The mechanical properties of the materials, as available, are given in Table 2. For the testing of the sawbone specimens, a block measuring 15 mm × 15 mm × 30 mm was used for each pull-out test. Human bone samples and animal substitute materials were also trimmed to fit in the test setup. The distance between two drill holes in non-synthetic materials was at least 1.5 cm in each test. After each of the first five trials, a microscopic check was carried out to detect any damage to the bone. Afterwards, only macroscopic controls were carried out after each pull-out.
Overview of Mechanical Properties of the Investigated Substitute Materials and Human Temporal Bone. SFFE/SRPU50: Sawbones Europe.

Abbreviations: SFFE: short fiber filled epoxy; SRPU50: solid rigid polyurethane.
Specification of the Tested Screws
Five types of orthodontic miniscrews were tested (Figure 3 and Table 3).

(a) Illustration of investigated bone screws. S1: PSM quattro standard (PSM Medical Solutions). S2: Promedia LeForte (Promedia Medizintechnik). S3: KLS maxdrive drill-free (Gebrüder Martin GmbH & Co KG). S4: General implants mini bone screw (General implants Germany GmbH). S5: Promedia dual top (Promedia Medizintechnik). (b) Detailed photograph of the flank at the tip of S3.
Overview of Miniscrews Investigated in This Study.

PSM: PSM Medical Solutions; Promedia: Promedia Medizintechnik; KLS: Gebrüder Martin GmbH & Co KG; General implants: General Implants Germany GmbH.
All miniscrews were selected in advance as self-tapping and self-drilling, and all are distributed as such according to the manufacturer’s specifications. In contrast to previous tests, 23 all screws were commercially available with an original intended use in dental surgery or for craniofacial and maxillofacial osteosynthesis. The length of the screws ranged between 9 and 11 mm; however, all screws were only inserted into the material to a predetermined depth of 3.6 mm. The length of the miniscrews was chosen to ensure visibility of the screw heads above the skin level 19 after insertion into the bone, which facilitates intraoperative anchoring of the frame. The screw diameter was 2 mm in all screws. The screwdrivers recommended by the manufacturers were used. All screws featured a cross-drive head, while all manufacturers recommended a classic screwdriver, only Promedia’s screwdriver could hold the entire screw head. Thread Design was the comparable for all screws. S2 to S5 were equipped with a flank at the tip (Figure 3b), whereas S1 was not equipped with such flank although it is also distributed as “self-drilling”.
Analysis
Graphical visualization and evaluation of the calibrated displacement was performed with Spyder, Version 4.1.5, with a customized protocol. The captured data was transferred to an Excel sheet (Microsoft Excel® 2019). Means and standard deviations for peak load provide the descriptive statistics. Using Kruskal-Wallis test, each screw type’s measurements from independent samples were compared for significant differences. A significance level of p = .05 was set. All statistical analysis was performed with SSPS® Version (28) (IBM Inc). Each force-displacement curve was analyzed individually to determine the joint stiffness, since the course of the pull-out was not linear over the entire test. A linear region was determined with a customized protocol in which the linear region was approximated using linear regression (least squares method) over at least 25 measurements. We iterated through different threshold values (from 0.05 to 10 N/mm) to find a suitable threshold. The threshold was used to determine if the linear regression line fitted for a segment of the data. Along with these measurements, the slope in the respective area was determined using the formula

Example of a force-displacement curve. Y-axis: force in N; X-axis: displacement in mm. Between the two crosses, a linear regression was applied.
With the given measurement data, the elastic energy was then determined using the formula:
k represents the stiffness determined before, measured in N/mm. Δd represents the change in displacement within the linear region and is measured in mm.
Results
The results of all pull-out tests divided by average force, standard deviation, range of the results, and calibrated displacement in human temporal bone as well as bovine femur and SFFE are given in Table 4.
Results of Pull-Out Tests Divided by Screw and Investigated Material.

All forces are given in N. Calibrated displacement is given in mm.
Abbreviation: SFFE: short fiber filled epoxy.
Bone Replacement Materials
S1 was evaluated in SRPU and bovine femur and also in pull-out tests with porcine iliac bone and pure sawbone. In 15 successful pull-out tests with porcine iliac bone, the average pull-out force was 127.7 N ± 80.7 N. In 15 successful pull-out tests with pure sawbone (SRPU50), the required average pull-out force was 187.1 N ± 59.2 N.
S2, S3, and S4 were tested in bovine femur and SFFE (Figure 5). In S2, one pull-out test had to be excluded from analysis due to an overtightening of the screw.

Overview of results of pull-out tests displayed in boxplots regarding different materials. X-axis: tested material; Y-axis: pull-out forces in N; left: pull-out forces in human temporal bone; middle: pull-out forces in bovine femur; right: pull-out forces in SFFE; S2: red boxplots; S3: green boxplots; S4: blue boxplots; S5: yellow boxplots; SFFE: short fiber filled epoxy. Asterisk brackets show statistic significant difference.
Comparisons in bovine femur regarding pull-out force with the Kruskal-Wallis test were statistically insignificant. A statistical significance was found in the pull-out-test of laminated sawbone between S1 and S5 (P = .008). Comparisons between all other screws were statistically insignificant. In bovine femur, S3 demonstrated significantly higher joint stiffness compared to S2 (P = .08), S4 (P = .02), and S5 (P < .01). No statistically significant differences in joint stiffness were found between screws in the SFFE material (Figure 6).

Overview of results of joint stiffness displayed in boxplots regarding different materials. X-axis: tested material; Y-axis: joint stiffness in N/mm; left: joint stiffness in human temporal bone; middle: joint stiffness in bovine femur; right: joint stiffness in SFFE; S2: red boxplots; S3: green boxplots; S4: blue boxplots; S5: yellow boxplots; SFFE: short fiber filled epoxy. Asterisk brackets show statistic significant difference.
In bovine femur, S3 demonstrated significantly lower elastic energy absorption than S4 (P = .05) and S5 (P < .05). In the SFFE material, significant differences were observed between S2 and S4 (P < .01), S3 and S4 (P < .01), and S3 and S5 (P = .03; Figure 7).
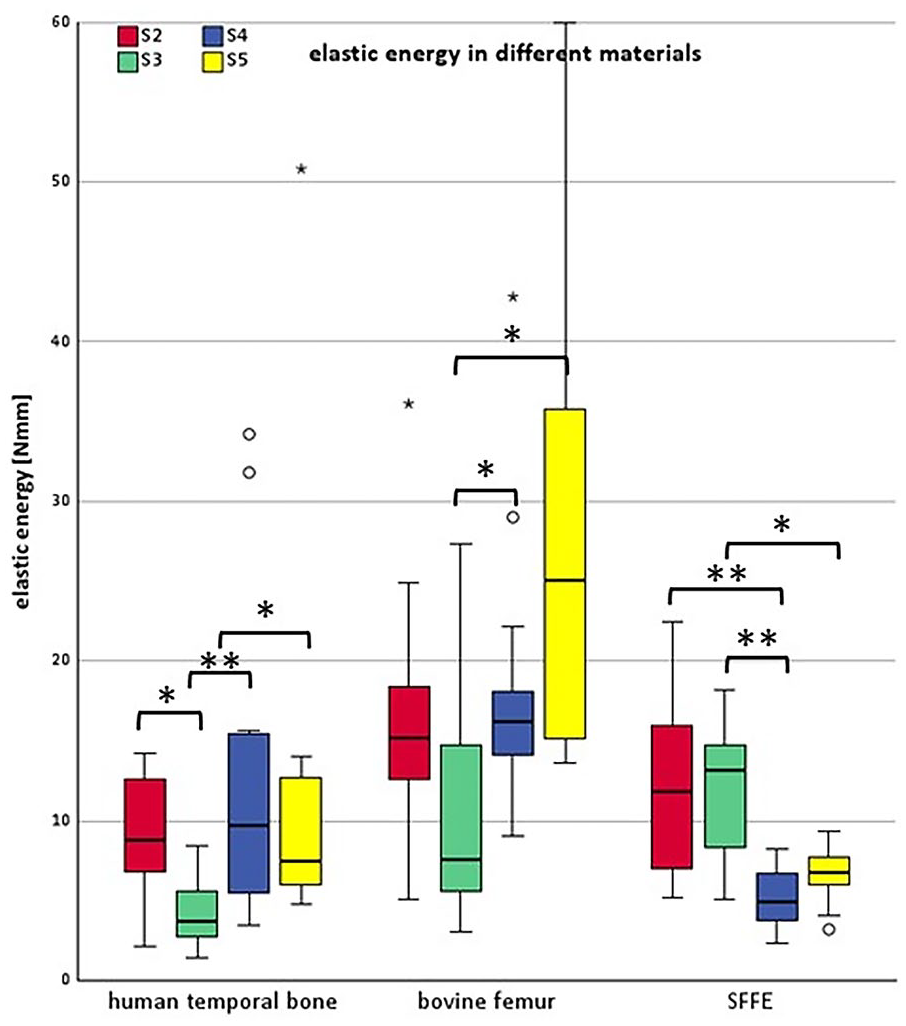
Overview of results of elastic energy displayed in boxplots. X-axis: tested material; Y-axis: elastic energy in Nmm; left: elastic energy in human temporal bone; middle: elastic energy in bovine femur; right: elastic energy in SFFE; S2: red boxplots; S3: green boxplots; S4: blue boxplots; S5: yellow boxplots; SFFE: short fiber filled epoxy. Asterisk brackets show statistic significant difference.
Generally, in each test, the investigated material failed. No damage or failure of a screw, except for S1, was observed.
Human Temporal Bone
S1 could unexpectedly not be placed into the human temporal bone samples as, in most cases, a small piece of the screw-tip already broke off during insertion and could no longer be used to cut into the bone. A total of 15 attempts were performed to insert S1 correctly. However, this was only successful twice. In both following pull-out tests, a piece of the screw-tip remained in the bore hole (Figure 8).

Comparison between S1 before drilling into the bone (left) and after the pull-out test (right).
In S3, in one case, the screw was overtightened and no pull-out was performed. One pull-out test was excluded from the analysis, as the pull-out force was less than 1 N so that it was evaluated as unnoticed overtightening of the miniscrew.
In S4, one test was excluded from the analysis, as the pull-out force was less than 1 N. In one case, a displacement of 5.0 mm was recorded, which was the predefined maximum of displacement. The test was stopped and the maximum force included into the evaluation.
In S5, in the pull-out tests in human temporal bone two screws and in bovine femur one screw was overtightened and no pull-out was performed.
All comparisons between the different screws types regarding pull-out strength (P > .05) in human temporal bone were statistically insignificant. The joint stiffness showed statistically significant differences between S3 and S4 (P = .01) as well as between S3 and S5 (P = .03) in human temporal bone. No significant differences were observed between the other screws (Figure 6). The elastic energy showed statistically significant differences between S3 and all other screws (S2, S4, S5) in human temporal bone, with P-values ranging from .01 to .04 (Figure 7).
Discussion
According to the recommendations of the Biometric Institute of our clinic, it was required to conduct 12 pull-out tests for each screw type in each material to demonstrate statistical significance. To ensure the attainment of this number even in the case of unsuccessful tests, the planned number of pull-out tests was increased to 15 for each screw type and substitute material.
Substitute Material
Regarding the investigation of a suitable substitute material, four different materials were tested. Laminated and non-laminated Sawbones were selected as artificial materials, as described. The natural materials evaluated included porcine iliac bone and bovine femur. No animal temporal bones were investigated because information regarding mechanical characterization was not available in literature at the time of the experiments. Porcine bone is often used as a replacement material for the mandible, representing one of the original applications of the reviewed miniscrews.25,43,44 However, it exhibited significantly lower values in comparison to the human temporal bone, with an average pull-out force of 128 N ± 80.7 N, also in comparison to the bovine femur. The differences were statistically significant (P = .03), leading to the decision not to pursue this approach. These findings align with the results of Kobler et al. 23
A similar result was observed in the unlaminated Sawbone (SRPU50). With an average pull-out force of 187 N ± 59 N, this material showed a statistically significantly lower pull-out force than the laminated Sawbone (P = .01). Consequently, no further pull-out tests were conducted using this substitute material.
Bovine femur and laminated Sawbone were tested in this study with all screws. The bovine femur exhibited a larger standard deviation, attributed, as with the human temporal bone, to variations in bone-diploe interface. In all tested screws, bovine femur showed significant lower joint stiffness than the human temporal bone, while elastic energy was higher than in human temporal bone for all screws.
The mechanical behavior of SFFE with regard to joint stiffness and elastic energy, most closely resembling the human temporal bone among all tested replacement materials. The average pull-out values of the laminated Sawbone were only 14.1 N higher compared to the human specimen. This difference is considered acceptable, making it suitable for use as a substitute material for the human temporal bone in further pull-out experiments.
Pull-Out force in Human Temporal Bone
The initial study design involved testing all types of screws in each material, with S1 randomly selected to serve as a reference. Unfortunately, the experiments were started with pull-out tests in the substitute materials due to a lack of knowledge about the performance of S1 in human temporal bone specimens. Subsequently, as mentioned earlier, we discovered that none of the intended pull-out tests in human temporal bone specimens could be performed. As a result, S1 had to be excluded from further experiments.
This unexpected finding necessitated a modification of the original study protocol. Now all other screws were first evaluated in human temporal bone samples, as it is the most relevant and critical material. In contrast to S1, this was possible without remarkable problems for all other screw types.
Although S1 was also described as self-cutting and self-drilling, it differs from the rest of the miniscrews in a special feature: it does not have a flank at the tip (Figure 3b). In retrospect, we consider this design detail to be an important aspect of the screw that contributes to its ability to drill and to cut the temporal bone, and therefore, its stability.
The biomechanical behavior of the individual screws displayed some significant differences. S4 showed the smallest standard deviation (101.7 N), while the other screws showed larger variations, with standard deviations ranging from 112 N to 135 N. Notably, SFFE shows an exactly inverse trend.
During drilling, compressive forces primarily occur along the drilling axis. Pull-out forces may arise during inserting or removing the drill, but in the study by Kobler et al,23,45 these forces amounted to a maximum of 26 N in untrained users. The mean forces were likely lower, but were not reported. The transverse interaction forces during drilling were consistently low, averaging between 1.0 N and 2.0 N, with a maximum reported value of 11.9 N.
Converting these transverse forces, which act roughly perpendicular to the skull surface, forces into tensile forces along the main axis of the miniscrews used for bone anchorage is highly speculative. It depends strongly on the geometry of the specific microstereotactic frame, including design details such as distances between bone screws, direction of force application, and its height above the skull surface. Therefore, a direct comparison of the values mentioned by Kobler et al 23 with the pull-out forces determined in this study is not feasible.
However, for a rough placement of the determined values in the context of expected drilling forces, we made the following assumptions: during drilling, compression forces primarily in axial direction are transferred to the bone screws via the ministereotactic frame. This is not critical for the stability of the bone anchoring. Transverse forces are on average negligibly small (≤2 N), and even the maximal transverse forces in a worst-case scenario described in of 12 N 23 does not seem to be crucial in case of a flat frame design, such as the one used in our group (which might differ in systems with longer legs and a more distal force transmission point, as in Kratchman et al 46 ). Therefore, assuming the strongest additive effects, it is unlikely that the forces in pull out direction would exceed 50 N.
Considering comprehensive safety margins are already included in these assumptions, further multiplication with additional safety factors does not seem justified. Therefore, we regard 50 N as an upper limit for reference forces. Furthermore, it is mentionable that the planned intraoperative setup (Figure 1) will distribute the applied forces among three miniscrews.19,47 In another scenario with just one screw, the screw-in depth is increased to 6 mm 17 which contributes to additional pull-out stability.
All the miniscrews tested23,45 force successfully withstood the upper limit force, except for a single test by S2, which held only 36 N. Average pull-out forces in human temporal bone ranged between 220 N and 284 N. For comparison: in the mentioned study by Kobler et al, bone anchors showed a median pull-out strength of 392.9 N in the human specimens. However, the bone anchors were inserted 5 mm into the bone, which is 1.4 mm (28%) deeper than in this study.
There were also variations in the displacement of the miniscrews under load. While S4 exhibited a displacement of up to 3.34 mm, in some cases, the top layer of the bone was detached from the rest of the specimen during the experiment before the miniscrew was pulled out. The other types of screws showed calibrated displacements between 1.4 mm and 2.2 mm.
Based on the visual observation of the pull-out tests, we exclude that the screws were elongated by the reported values in the experiments. It is impossible to ascertain if and to what degree this displacement affects the stability of the bone-screw interface and thus the bone-screw interface. This relatively large deviation could indicate a slow failure with a detachment of the upper layer of the bone before the miniscrew pull-out rather than a pull-out from the bone material, potentially limiting accuracy. Furthermore, it could be a deformation resulting from the experimental setup that was not captured by the mathematical correction.
However, Rau et al have performed investigations regarding accuracy using three screws of type S3 to mount the reference frame of a surgical targeting system. 15 The result was a high drilling accuracy with a mean position error of 0.41 mm. Therefore, we assume that a comparable large displacement does not occur in the clinical setting or has only minor effect on accuracy.
The joint stiffness in human temporal bone results align with the findings from the pull-out force testing, where S3 showed the highest average pull-out force compared to other screws. The significant differences observed between S3 and other screws in human bone suggested that S3 achieves a very rigid connection to the temporal bone. This could be attributed to subtle differences in thread pattern, shape, or material when compared to S2, S4, and S5. However, joint stiffness alone may not fully predict anchorage performance, as no significant differences were observed between screws in SFFE despite variations in pull-out force. Further mechanical testing could provide insights into the factors contributing to the higher joint stiffness observed for S3. Overall, these findings provide additional insights into the strength of the bone-implant interface achieved with different orthodontic miniscrews.
While S3 demonstrated the highest joint stiffness and maximum pull-out force, it showed significantly less elastic energy prior to failure compared to all other screws. As S3 achieves rigidity and resistance to pull-out, the low elastic energy value could point to only small deformation of the joint under load. In contrast, screws S2 and S4 exhibit more ductile interfaces, with lower maximum stiffness yet greater energy absorption before failure. Material factors likely also contribute, as differences in elastic energy were not observed between screws in SFFE. These findings highlight interrelated factors governing interface stability. Overall, S3 provides the strongest connection to bone, informing miniscrew selection for applications requiring enhanced anchorage strength and resistance to failure. Further testing under varied loading conditions is required to elucidate the mechanisms conferring high stiffness yet low ductility to the S3 bone-screw interface. However, the lack of significant differences between the miniscrews in SFFE in terms of joint stiffness emphasizes the influence of material properties on anchorage performance.
In terms of intraoperative handling, we found S5 to be the most convenient to use, as it was the only screwdriver that could hold the entire screw head, making the screwing more stable and easier to insert.
It might pose a clinical concern that one unnoticed overtightening of S3 and S4 was observed in one experiment with human material, although a manual check of the correct placement of the screw was performed after each screwing-in before the pull-out. If this issue arises during surgery, it could lead to a deviation of the trajectory due to the complete failure of the joint. In a similar setup for minimally invasive access to the cochlea, in which the frame was fixed with only one miniscrew onto the skull, the screw is tightened with a torque wrench to a predefined force to prevent overtightening. 17
Human bone showed the highest variation of results compared to the tested substitute materials, possibly attributed to the variation of the cortical bone-diploe interface. Although age, gender, and ear side have only minor effects on temporal bone thickness and bone density, 48 their influence on pull-out force remains unclear. Given the bone structure, preoperative bone density measurements in imaging could be performed, followed by the use of preoperative indices (Screw Implantation Safety Index and Column Density Index) to identify optimal areas for screw placement.
An additional limitation of the presented tests is the exclusive use of experiments with bone specimens in an optimized configuration. In further investigations, the miniscrews should also be tested with the complete reference frame (Figure 1) including three bone screws, rather than examining an isolated, single screw, as the loading conditions are more complex in such a case. Moreover, in this study, only a load case of 90° along the screw axis was tested. While the longitudinal pull-out test provides valuable insights into bone-screw interface stability, this loading condition is simplified compared to clinical scenarios. In vivo, more complex forces arising from drilling and handling would act on the screws. Although sufficient for comparing basic interface rigidity, additional testing methods are warranted to replicate surgical conditions.
Transverse and oblique pull-out tests could determine strength against shear loads. Axial fatigue and cyclic loading tests would elucidate performance under repetitive forces and micromotions. Finally, experiments with the complete intraoperative setup using multiple screws could evaluate stability under combined multidirectional forces. While practical constraints often limit testing complexity, these techniques could better characterize construct strength for survival under intraoperative loads.
Our results provide preliminary data to guide miniscrew selection, but further verification is needed under diverse loading modalities. These experiments should also be conducted with the miniscrews only partially inserted into the bone, as their tapered design may make them more susceptible to lateral forces.
The investigated orthodontic miniscrews have proven excellent primary stability in orthodontic studies, resulting from the mechanical connection and the relationship between the miniscrew thread and the surrounding bone immediately after installation. 25 The higher loss rate described in several publications is a long-term complication that does not play a crucial role in cochlear implantation surgery, as the miniscrews are removed at the end of the procedure and do not have a sustainable load-bearing function.
Overall, none of the successfully tested miniscrews showed a statistically significant difference in withstanding forces in the pull-out test. S3 displayed significant higher stiffness, indicating a solid connection to the bone. However, the smallest elastic energy absorption also suggests a solid connection with only little deformation. Overall, all tested miniscrews seem suitable for fixation of a stereotactic frame at the lateral skull base due to sufficient stiffness and the ability to withstand the expected force.
S1 had to be excluded from the tests because no solid connection to the skull could be established. Due to the high displacement, S4 would not be our first choice, and we recommend conduction further tests before utilizing it for fixation.
Conclusion
This study is the first evaluation of the stability of orthodontic miniscrews at the lateral skull base and their feasibility for frame fixation in minimally invasive cochlear implantation surgery. Different substitute materials were compared for further experiments. Our findings demonstrate that laminated sawbone specimens, with an average pull-out force 14.1 N higher compared to the human specimens and comparable mechanical performance in terms of joint stiffness and elastic energy, are suitable as substitute material for the human temporal bone.
Our experiments revealed that all miniscrews withstood an adequate pull-out force in tests with human temporal bone specimens. The measured joint stiffness indicates that a solid bone connection can be established. Therefore, the investigated orthodontic miniscrews are suitable for fixation of a stereotactic frame at the lateral skull base.
Footnotes
Correction (June 2024):
This article has been updated with Figure 4 since its original publication.
Author Contributions
CM performed the experiments, drafted the manuscript, and designed the figures. CM, MK, BW, and TR were involved in planning, and TR, OM, and TL supervised the work. CM, BW, MK, and TR processed the experimental data, performed the analysis, CM and MK performed the statistics. TR, TL, and OM aided in interpreting the results and worked on the manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
The datasets during and/or analyzed during the current study available from the corresponding author on reasonable request.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany’s Excellence Strategy—EXC 2177/1—Project ID 390895286, project RA2751/4-1 and in part by the Federal Ministry of Education and Research of Germany (BMBF, grant number 13GW0367B).
Ethics Approval and Consent to Participate
Via institutional review board approval (Ethics Committee of Hannover Medical School; 3512-2017).