
Abstract
Background
End-of-life (EOL) conversations offer individuals opportunities for consideration of future treatment options with accordance to their values and wishes, helping maintain autonomy and dignity in the eventual dying process. While there exists multiple reports in the international literature focusing on community-based interventions for initiating early advanced care planning (ACP) conversations and EOL planning behaviors in non-terminally ill adults, the effects of these interventions are poorly understood.
Objectives
We conducted a systematic review and meta-analysis to provide a comprehensive summary of community-based interventions for the initiation of early ACP conversations and EOL planning behaviors that may aid other countries and societies in adopting such implementations.
Search Methods
A total of 30,869 abstracts were identified from CINAHL, Cochrane Central Register of Controlled Trials, Embase, PsycINFO and PubMed from their respective dates of inception to 20 July 2025, of which 71 articles were included in the final analysis.
Selection Criteria
The population of interest were non-terminally ill adults above the age of 18 who were residing in the community at the time of study. The intervention of interest was any community-based intervention with the objective of promoting or educating on EOL and ACP related topics. The comparator was any ongoing education or outreach on EOL and ACP in the community or no intervention at all. The outcome was (1) rate of completion of EOL and ACP-related behaviors and (2) self-reported scores of knowledge, attitudes and perceptions of EOL and ACP.
Data Collection and Analysis
Two investigators independently extracted data for each study, pertaining to the study design, intervention design, baseline characteristics, EOL and ACP-related knowledge, attitude. The quality of studies was appraised in reference to the National Institute for Health and Care Excellence checklist. A meta-analysis of standardized mean difference (SMD) was conducted to assess the effectiveness of interventions in improving (1) uptake of EOL and ACP-related behaviors and (2) knowledge, attitudes and perceptions (KAP) towards EOL and ACP.
Main Results
83 studies consisting of interventions using workshops, 1-to-1 counselling, discussion groups, modified AD, complex methods, distribution of printed or online materials, were included in this study. Community-based EOL interventions were significantly associated with carrying out EOL or ACP-related behaviors (n = 71,489 participants in 19 studies, RR = 2.24, 95% CI: 1.42 to 3.53, I2 = 97%) and more positive perceptions towards EOL and ACP (n = 1,766 participants across 12 studies, SMD = 1.24, 95% CI: 0.42 to 2.06, I2 = 87%) as compared to usual care. Similar findings were reported for single-arm studies and remained robust on sensitivity analysis of studies with low risk-of-bias only. Subgroup and meta-regression analyses showed that discussion group and workshop-based interventions were relatively more effective in promoting EOL and ACP compared to other interventions.
Authors’ Conclusions
Community-based interventions were shown to be effective in improving uptake of EOL and ACP-related behaviors and perceptions towards EOL and ACP amongst the nonterminally ill. Further studies investigating interventions for promotion of EOL and ACP should consider appropriate right-siting in the community and co-creation with key community figures to improve contextualization and generalizabilty.
Plain Language Summary
There is moderate evidence for community-based evidence in promoting end-of-life (EOL) and advanced care planning (ACP)-related behaviors and attitudes amongst a non-terminally ill population.
Keywords
Background
The Problem, Condition or Issue
Quality end-of-life (EOL) care is emerging as an important public health issue globally. EOL care refers to care in the last 6–12 months of life (Goh, 2016). This is usually at the onset of a life-limiting illness such as advanced cancer or end-stage organ failure. EOL care aims to optimize quality of life through the provision of psychological, social, spiritual, and physical support for patients and their loved ones (Department of Health, nd). Insufficient EOL care conversations and preparation have resulted in unwanted admissions and treatments for patients with advanced diseases when it would not have altered their disease trajectory (Prince-Paul & DiFranco, 2017) With an aging population and an increasing proportion of chronic illnesses with prolonged terminal phases (e.g., dementia), there is a pressing need to improve early EOL care preparation across the globe. For the purposes of this review, we define early EOL planning as planning for EOL care prior to the EOL (life expectancy of 12 months or less).
Early EOL planning has been shown to increase the quality of EOL care received (Brinkman-Stoppelenburg et al., 2014), reduce admissions in the last 30 days of life (Prater et al., 2019), and increase quality of care near the EOL (Ankuda & Meier, 2018). Planning for EOL care requires conversations that are iterative and center around the values of the person, encompassing topics such as care plans, medical plans, legal issues, and funeral planning (Sorrell, 2018). Currently, EOL conversations tend to be initiated by healthcare professionals, and usually only towards the last phase of a serious illness. As these tend to be medico-centric, there is a tendency to neglect physical and psychosocial concerns (Balaban, 2000). Moreover, people with newly diagnosed life-limiting illness often find it difficult to have EOL conversations at this time (Larson & Tobin, 2000).
Advance care planning (ACP) is a form of EOL communication process through which adults of any age or stage of health deliberate and share about their values, wishes and preferences regarding future medical care (Sudore et al., 2017a; Sudore et al., 2017b). ACP involves EOL care preparation and has been shown to improve not only EOL care in patients but also psychological outcomes in family members (Detering et al., 2010). According to the Centers for Disease Control and Prevention, improving community education of ACP addresses the public health issue of unwanted and expensive treatments (Prince-Paul & DiFranco, 2017) and therefore, delivers quality EOL care. By having early ACP conversations in the community before the last phase of a serious illness, family members and loved ones have sufficient time to explore EOL care as a holistic concept that addresses not just the medical decisions, but also the social, legal and financial dimensions (Banner et al., 2018). Care plans that the family believe in and support may be made in advance, and can be instituted should the patient lose mental capacity due to illness.
Currently, early ACP conversations in the community are generally avoided by the public (especially in Asian societies), as ACP conversations may be considered taboo (Lin Goh, 2018). A survey conducted in Singapore showed that only 36% of respondents from the general public expressed feeling comfortable having ACP conversations (Blackbox Foundation, 2014). Similar results have been reported in the UK with 72% of respondents agreeing with the statement “People in Britain are uncomfortable discussing dying, death, and bereavement” while they are healthy (Dying Matters, 2024), and in the United States, where 69% of respondents say that death is a subject that is generally avoided in their society (Hamel et al., 2017).
Barriers to early ACP conversations include perceptions that ACP conversations are not relevant to individuals given their health or age (McLennan et al., 2015), concerns about relationships with loved ones and “burdening” them with such discussions (Schickedanz et al., 2009), lack of knowledge of EOL issues and options for EOL care (McCarthy et al., 2010), lack of accessibility to information for facilitating early ACP conversations (Banner et al., 2018), religious and cultural factors (Granek et al., 2013; Periyakoil et al., 2016), as well as a fear of dying (Tay et al., 2012).
While there exists multiple reports in the international literature focusing on community-based interventions for initiating early ACP conversations and EOL planning behaviors, the effects of these interventions are poorly understood (Abba et al., 2013). Thus, in order to better understand the initiation of ACP conversations in nonterminally ill adults in the community, this review aims to summarise the existing international literature on community-based interventions, and evaluate the effects of these interventions on the initiation of early ACP conversations and EOL planning in the community through a meta-analysis. Specifically, we aim to meta-analyze changes in self-reported knowledge, attitudes and perception scores towards EOL/ACP and rates of uptake of EOL/ACP-related behaviors to evaluate the impact of community interventions on these two outcomes.
The Intervention
This review included all types of community-based interventions targeted at initiating early ACP conversations and EOL planning behaviors in non-terminally ill adults. ACP conversations are defined as two-way communications between a person and one’s care practitioner regarding their goals and preferences for future medical care, with review and recording of such conversations where appropriate (Rietjens et al., 2017). ACP conversations may include one or more of the following elements of early EOL care: reflection and discussion of personal values; preferences for medical care and/or treatment towards the EOL; preferences related to supportive, cultural, or spiritual care towards the EOL; concerns associated with personal finance and administrative documentation; concerns associated with the dying process; funeral planning; or death (Rietjens et al., 2017). Hence, EOL planning behaviors can be defined as any tangible goal-directed steps taken by an individual to establish a record of preferences for future medical care (Mullick et al., 2013). Examples of EOL planning behaviors may include one or more of the following: completing an advanced directive document; making early funeral arrangements; making or updating a will; appointing a Lasting Power of Attorney (LPA) (Mullick et al., 2013; Rietjens et al., 2017).
Community-based interventions are the focus of this review. These are complex interventions, which may be described as “non-standard, having different forms in different contexts, while still conforming to specific, theory driven processes” (Petticrew, 2011). They have multiple interacting components and often do not have simple linear pathways linking the intervention and outcome. Thus, randomization may not always be feasible and appropriate, and systematic reviews of complex health interventions will need to include data from a broader range of study designs (Shepperd et al., 2009).
An example of a randomized community-based intervention for early EOL planning is the PREPARE randomized clinical trial (Sudore et al., 2018). In the PREPARE trial, older patients (55 years and above), with 2 or more chronic illnesses were recruited from primary care clinics in a public-health delivery system. Participants were exposed to either an easy-to-read version of an advance directive in addition to an online, patient-directed ACP program (PREPARE arm); or just the advance directive alone. A subsequent increase in ACP documentation was reported in the PREPARE arm, compared to those exposed to the advance directive alone (43.0% vs. 33.1%, p < .001). Furthermore, there was higher patient-reported engagement (98.1% vs. 89.5%, p < .001) in the PREPARE arm. Another randomized trial assessed the effect of a tripartite educational intervention (involving face-to-face discussion, educational forms and reminder cards) on the use and discussion of advanced directives (Sachs et al., 1992).
Examples of nonexperimental studies for early EOL community-based interventions include lectures delivered by a physician to members of the general public who had responded to an open advertisement (Miyashita et al., 2008), roadshows held in busy town centers in collaboration with a local “Dying Matters” campaign aimed to educate and engage the public in discussing EOL issues (Hickey & Quinn, 2012), and the development of an information booklet and education program for other elders by peer volunteers (Sanders et al., 2006).
How the Intervention Might Work
These community-based interventions aim to change the health behaviors of nonterminally ill adults in the community in order to nudge them towards early ACP conversations and EOL planning. As these community-based interventions are complex behavior-change interventions that may impact multiple interacting components of a person’s psychology and environment to change intention and behavior (McLeroy et al., 2003), theoretical models on health behavior change might provide us with greater insight on how these interventions might work. As these are a mixed-bag of community-based interventions, it is unlikely that a single theoretical model would be able to comprehensively explain the underpinnings of how such interventions could result in behavior change in ACP conversations (Angeles et al., 2014). However, it may be useful to understand different concepts of behavior change theory, and how these may explain the effects of these community-based interventions in increasing early ACP conversations and EOL planning behaviors in the community.
For example, the Health Belief Model (HBM) describes six concepts to health behavior change: risk susceptibility, risk severity, benefits to action, barriers to action, self-efficacy, and cues to action (Jones et al., 2015). The HBM proposes that individuals with greater perceived benefits, fewer perceived barriers, and good self-efficacy who are provided cues to action are more likely to be motivated towards a health behavior. In the context of EOL discussions, this was supported by a study which showed that the likelihood of EOL communication increased as perceived barriers decreased (Ko & Lee, 2009). For example, a public lecture series conducted in Japan addressed the misconception that dying at home was not possible. Prior to the lecture, 9% of participants stated that home death was possible. This increased to 34% after the lecture (Miyashita et al., 2008).
Another model on health behavior change, the Theory of Planned Behavior (TPB), described the concepts of an individual’s attitudes, subjective norms, and perceived behavioral control on the intention to perform a particular health behavior (Ajzen, 1985). The TPB was used in understanding healthy older adults’ intention to use hospice care should they face terminal illness (Nahapetyan et al., 2017). Nahapetyan et al. showed that higher perceived control to use hospice care, and preferences for EOL care that favor comfort and quality of life over living as long as possible were significant predictors of intention to use hospice care. Another example was an education program developed for 121 older adults in West Japan. This included a video, a lecture with handouts, and a session for discussion among participants. By offering them an opportunity to learn more about EOL care and demystify the dying process, this improved attitudes amongst the participants towards advance directives (Matsui, 2010).
Hence, by utilizing theoretical models on health behavior change such as the HBM and the TPB, we gain an insight into how these community-based interventions can influence nonterminally ill adults to initiate early ACP conversations and adopt EOL planning in the community. In addition, we developed a logic model a priori (Figure 1) to better illustrate the inputs, processes, and outputs that in general, may be involved in such community-based interventions, as well as how these may lead towards the short-term and long-term outcomes of the interventions (Bravo et al., 2016; Glasgow et al., 2019; Green & Levi, 2009; McMahan et al., 2021; Sudore et al., 2014; Van Scoy, Green, et al., 2017; Van Scoy, Reading, et al., 2017). Logic Model on the Inputs, Processes and Outcomes of Community-Based Interventions for Initiating Advance Care Planning Conversations in Nonterminally Ill Adults
A limitation of these community-based interventions are that these studies aim to increase outcomes of early ACP conversations and EOL planning in the community but are unable to evaluate if these interventions change actual behavior in future circumstances of approaching death or terminal illness. It is likely to be impractical and resource intensive to conduct such a study to evaluate if actual behavior in the future has been impacted by the community-based interventions that we are reviewing, and we acknowledge this as a limitation of our study.
Why It Is Important to Do This Review
While there exists multiple reports in the international literature focusing on community-based interventions for initiating early ACP conversations and EOL planning behaviors in nonterminally ill adults, the effects of these interventions are poorly understood. Furthermore, these community-based interventions may be costly and resource intensive, or difficult to implement in other countries and cultural contexts. Hence, it is important to summarize the reported interventions and investigate their effects in the community.
To our knowledge, there is only one systematic review examining interventions to encourage discussion of EOL preferences between members of the general population and their loved ones (Abba et al., 2013). However, this review was conducted in 2013, included only five unique studies, and only examined the effects of discussions between participants and people close to them, or barriers to such a discussion. Thus, our systematic review will provide a comprehensive and up-to-date summary of complex community-based interventions for the initiation of early ACP conversations and EOL planning behaviors that may aid other countries and societies in adopting such implementations.
Objectives
This systematic review aims to answer the following research questions: 1. What are the existing community-based interventions for initiating ACP conversations and EOL planning behaviors in nonterminally ill adults internationally? 2. What are the effects of community-based interventions on the initiation of ACP conversations and EOL planning behaviors of nonterminally ill adults in the community, specifically in terms of attitudes towards EOL and ACP and subsequent uptake of related behaviors
Methods
The systematic review protocol was published on 24th May 2021 and is accessible via: https://doi.org/10.1002/cl2.1168.
Criteria for Considering Studies for This Review
Types of Studies
We included randomized controlled trials (RCTs), quasi-experimental studies such as non-randomized controlled trials and observational studies such as cross-sectional studies that evaluated the effectiveness of community interventions to promote end-of-life care conversations. Evaluation reports commissioned by governments, public health institutions and private companies such as health technology assessments (HTAs) are also included. We excluded studies that solely report qualitative data without quantitative outcomes.
Types of Participants
Studies that recruited nonterminally ill participants aged 18 years and above from the community will be included. Patients with chronic illness will also be included as long as they do not fulfil the criteria for terminal illness, namely life-limiting illness with a life expectancy of 12 months or less. We excluded studies that recruited participants from hospitals or other similar inpatient settings as such participants are more likely to be terminally ill and exposed to initiating EOL conversations. Studies targeting terminally ill patients in the community or family members and carers of terminally ill patients are excluded as well.
Types of Interventions
All studies describing community-based interventions for initiating early ACP conversations and EOL planning behaviors were included. Interventions include a range of approaches, including workshops, lectures, forums, roadshows, communication through brochures, or targeted one-to-one communication. These interventions may be conducted by government-affiliated, private, or social organizations, or may be community-based interventions that were initiated by members of the community. As these are complex interventions, a control group may not always be included in these interventions and the lack of such is not an exclusion criteria. The minimum requirements for an intervention to be included in this review are that it involves the topic of early ACP conversations and EOL planning in the community, and generates at least one outcome of early EOL planning behavior.
Study Setting
All community-based interventions will be included in this review. Individuals in the community may be recruited from participants’ homes, community centers, common spaces in the community, malls, schools, business compounds, religious spaces, and community healthcare facilities such as the outpatient clinic, primary care, day care centers, senior care or activity centers. As the focus of this review is on community-based interventions, studies that were conducted on hospitalized participants or participants institutionalized in a healthcare facility will not be included in this review. This includes participants who are residing in nursing homes, mental institutions, community hospitals, inpatient hospice, or shelters and senior group homes.
Types of Outcome Measures
Studies evaluating the following primary or secondary outcomes using quantitative data (e.g., uptake rates, self-reported scores on intention to initiate EOL planning behaviors, self-reported scores on perceptions and attitudes to ACP) were included. Studies that reported qualitative information (e.g., description of in-depth interviews questions and methods of administering questions; focus group discussions; unstructured written narratives or responses from questionnaires) without quantitative data were excluded from this review. In addition, outcomes evaluated by government-affiliated, private, social organizations, or health institutions were included in this study.
Primary Outcomes
The primary outcomes of this review are the. 1. Rate of uptake of early EOL planning behaviors including one or more of the following: early ACP conversations conducted or initiated, completing an advanced directive document; making early funeral arrangements; making or updating a will; or appointing a LPA. 2. Changes in knowledge, perceptions and attitudes towards early ACP conversations and early EOL planning behaviors. These changes are measured quantitatively using previously validated questionnaires such as the Advanced Care Planning Engagement Survey (Sudore et al., 2013), or self-designed instruments.
Duration of Follow-up
No restrictions were placed on the duration of follow-up. In general, most community-based interventions for early EOL planning may have a cross-sectional or pre-post design and may not have a follow-up evaluation of the intervention as it may be difficult to recontact participants of such a community-based intervention. However, some studies may include a follow-up evaluation of the intervention at a later time frame (e.g., 6 months post-intervention) (Sato et al., 2009). This review described the presence of follow-up and its respective duration if the included studies have explicitly stated so.
Search Methods for Identification of Studies
We searched the following electronic databases from inception to the 20 July 2025: Medline (via PubMed) Embase (via Embase. com) Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library PsycINFO (OvidSP) Cumulative Index to Nursing and Allied Health Literature (CINAHL) (via EBSCO)
The search strategy consisted of medical subject headings (MeSH) terms and keywords involving the concepts of (1) the outcome of the study includes early ACP conversations or early EOL planning, (2) types of interventions, and (3) studies conducted in the community. We have presented the electronic search strategy in Appendix A. The search strategy was produced with the consultation of a medical information specialist, and piloted on PubMed. Modifications were made to optimize the search before translation over to other databases as befitting the syntax. No language nor date restrictions were applied during our electronic search.
Searching Other Resources
In order to further extend the search, the bibliographic references of relevant systematic reviews and all included articles were searched for relevant articles to be included in the review. Relevant individuals and organizations will be contacted for information regarding unpublished or ongoing studies. We also performed a search of the grey literature using Web of Science, Google Scholar, and the Worldwide Hospice Palliative Care Alliance.
Data Collection and Analysis
Selection of Studies
Two reviewers independently (2 amongst YYT, SNF, KYF) screened the titles and abstracts of the retrieved records against the predefined inclusion criteria based on (a) the population of nonterminally ill adults in the community; and (b) interventions on early EOL planning behaviors using the Covidence tool (Covidence 2024). Any discrepancies in records included will be resolved by discussion with the senior author (LJRM).
Summary of Characteristics of Included Studies

Legend: ACP = advanced care planning; AD = advanced directive, KAP = knowledge, attitudes and perceptions; NA = not applicable; NR = not reported; SD = standard deviation.
Data Extraction and Management
For studies that were subsequently included in this review, two review authors independently conducted the data extraction on the Covidence platform with the following data fields: sample size, methodological issues (study design, sampling method, randomization methods (if applicable), study setting, country, time frame, method used for data collection), demographic information (age, gender, race, education, income, marital status), interventions (type of intervention, platform of delivery, message of the intervention, time required to administer the intervention, frequency of administration of the intervention, follow up methods and time points of interest, comparison group if there is one, and cost of the intervention), and outcome data (initiation of early ACP conversations or EOL planning behaviors, changes in knowledge, perceptions and attitudes to early ACP conversations and EOL planning). Any discrepancies in data collection were resolved by discussion with the senior author (MLJR) until a common consensus has been reached. Corresponding authors of included articles were contacted by email to request further data on methods or results where necessary.
Assessment of Risk of Bias in Included Studies
Risk of bias assessment of selected studies was conducted by two review authors independently using the National Institute for Health and Care Excellence (NICE) quality appraisal checklists for quantitative intervention studies and quantitative association studies (Schlander, 2007). Studies were rated as “Low”, “Moderate” or “High” risk-of-bias based on these quality appraisal checklists. Specifically, as no guidance was given on how to summate the scoring for individual domains towards an overall grading, it was prospectively determined that (1) ratings of significant bias were scored −1 and domains which studies failed to report were scored −0.5, and (2) studies receiving a total score no less than −1 were rated overall “Low” risk-of-bias, studies receiving ratings of significant bias for one to four, inclusive, domains were rated overall “Moderate” risk-of-bias, while studies receiving ratings of significant bias for five or more domains were rated “High” risk-of-bias. Additionally, if a study did not report data where applicable for a high number of domains, the overall bias was downgraded by a level as well.
For visualization purposes, the individual domains were categorized into themes of “Population”, “Allocation to Intervention”, “Outcomes”, “Analyses”, and “Summary”, following the categorization found in the NICE checklists as well. Themes with no ratings of significant bias were visualized as “Low” risk-of-bias, themes with at least one but less than half of its total domains rated as having significant bias were visualized as “Moderate” risk-of-bias while the remaining themes with half or more domains rated as having significant bias were visualized as “High” risk-of-bias. Risk-of-bias assessment was then visualized as traffic-light plots using the robvis tool (McGuinness & Higgins, 2021).
Discrepancies in the risk of bias assessment were resolved by discussion with the senior author until a common consensus was reached.
Measures of Treatment Effect
For all studies with a control group, dichotomous data were analyzed based on the number of events and the number of people assessed in the intervention and comparison groups. These numbers were used to calculate the risk ratio (RR) or odds ratio (OR) and the 95% confidence interval (CI). In the instance that observational studies do not report the number of events and the number of people assessed in the intervention, adjusted and unadjusted ORs or RRs and their respective 95% CIs will be extracted.
For continuous measures, we will analyze data based on the mean, the standard deviation, and the number of people assessed for both intervention and comparison groups to calculate the mean difference (MD) and 95% CI. If more than one study measures the same outcome using different tools, we calculated the standardized mean difference (SMD) and the 95% CI with inverse variance weighting. In cases of missing standard deviation values, we will recalculate them from the reported statistics provided in these studies, such as t-statistic values, 95% CIs.
For quasi-experimental studies where outcome measures are recorded pre- and postintervention, measures obtained before the intervention will be treated as the control group and measures obtained after the intervention as the treatment group (Reeves et al., 2019).
Further descriptive synthesis of various aspects of the community-based interventions (e.g., the cost of the intervention, type of intervention, platform of delivery, message of the intervention, or time required for the intervention) were extracted where possible. Using the data collected, a comprehensive summary of all community-based interventions for initiating early EOL planning was provided and the range of interventions was categorized into broad groups based on the nature of such interventions.
Unit of Analysis Issues
For each included study, the unit of analysis was assessed for appropriateness for the unit of randomization and the design of each study (i.e., whether the number of observations matches the number of “units” that were randomized) (Higgins et al., 2021). The preferred method for unit of randomization was prospectively determined to be the individual participant.
If a cluster-randomized trial was included, the intraclass correlation coefficient (ICC) was extracted and used to convert trials to their effective sample size before incorporating them into the meta-analysis, as recommended by the Cochrane Handbook for Systematic Review of Interventions (Higgins et al., 2021).
Where insufficient data are available from cross-over studies to incorporate paired data in a meta-analysis, the measurements from each arm would be considered separately, as if from a parallel group trial. As this can result in a unit of analysis error, the results were only included if they are demonstrably similar to the results of a paired analysis (Higgins et al., 2021).
Studies including within-subject comparisons (pre- and post-) were included in the meta-analysis if they analyzed the data using paired sample t-test and present the mean of the difference as well as its standard error. Then, such a result will be pooled with other studies presenting the mean differences and standard errors in meta-analysis of standardized mean difference.
Criteria for Determination of Independent Findings
It was a priori determined that the unit of study in this review should correspond to a unique trial or cohort study. Hence, each study was assessed such that secondary or subgroup analyses of the same cohort reported in a different paper would be excluded.
Dealing With Missing Data
In the event of any missing data, the review team attempted to contact study authors via email to obtain the original data pertaining to the study. Missing data was handled by listwise deletion of the affected observations in the meta-analysis and subsequently discussing its impact on findings after.
Assessment of Heterogeneity
Clinical and methodological heterogeneity was assessed qualitatively by comparing the distribution of important participant factors between studies, and study design factors, intervention types and loss to follow-up and discussed amongst key authors of the review.
As the heterogeneity in study methodology and outcomes was not significant enough to adversely impact comparability, a meta-analysis was conducted. Statistical heterogeneity was assessed (1) by visual inspection of the forest plots and (2) using the chi-squared test with a significance level of 0.10. Statistical heterogeneity in each meta-analysis was measured using the I2 statistic as described in the Cochrane Handbook for Systematic Reviews of Interventions recommendations (Higgins et al., 2021). The I2 statistic was calculated using the restricted maximum likelihood estimation, as it has the least bias compared to other estimators regardless of sample size (Langan et al., 2019). Overall heterogeneity was rated using the following categories: <25%, no heterogeneity; 25%–40%, low heterogeneity; 50%–74%, moderate heterogeneity; and 75% or greater, high heterogeneity. High heterogeneity (≥75%), where identified, was explored for sources of heterogeneity using subgroup analyses and meta-regression. Clinical variation across studies was assessed by comparing the distribution of important participant factors in the study (e.g., age), and other study factors.
In addition to the I2 value (Higgins et al., 2021), Cochran’s Q-statistic value, p value from the chi-squared test, and the tau-squared value were presented to provide a more comprehensive view of the direction and magnitude of the treatment effects. As in meta-analyses with few studies (Higgins et al., 2021), the chi-squared test is underpowered to detect heterogeneity should it exist; a p value of .10 will be used as a threshold of statistical significance.
Assessment of Reporting Biases
Publication bias was assessed through funnel plots to investigate any relationship between effect estimates and study size or precision, as recommended in the Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (Higgins et al., 2021). Egger’s regression test was performed to assess funnel plots for asymmetry. In the case of an asymmetrical funnel plot for any meta-analysis outcome, potential causes of reporting biases would be explored and its potential impact on findings would be discussed.
Data Synthesis
Results for randomized trials, quasi-experimental designs, and observational studies would be synthesized and reported separately. All relevant variables for each meta-analysis were compiled as a data table and analyzed in R version 4.3.3 (R Core Team & others, 2013) using the metafor package (Viechtbauer, 2010). It was previously determined that data analysis would be done on Review Manager but this did not come to fruition due to the retirement of Review Manager from both Campbell’s workflows and the public domain. As two or more studies were found to report adequate data, a meta-analysis of the available data for each outcome (e.g., uptake rate of ACP completion) would be conducted. Variability in populations and interventions, setting, and possibly other factors, of included studies was anticipated. Therefore, RRs/ORs or SMDs were pooled using a random effects model to account for study variability and forest plots were generated to visualize results.
Contour-enhanced funnel plots were constructed and statistical tests of funnel plot asymmetry were performed using Egger’s test. Heterogeneity would be assessed using both Cochran’s Q test and the I2 statistic calculated using restricted maximum likelihood estimation method (Higgins et al., 2021).
As mentioned previously, if the extracted data cannot be pooled quantitatively in a meta-analysis, it was prospectively determined that the data would be narratively synthesized. This is to provide readers with a broad overview and clear summary of the effects of community-based interventions, the associated design elements and respective changes in knowledge, attitudes and perceptions towards EOL or ACP topics.
Subgroup Analysis and Investigation of Heterogeneity
Subgroup analyses will be performed in order to assess if there is variation in the effects of the intervention depending on the following factors: 1. Study design, specifically if the study was two-arm or one-arm 2. Type of intervention and design elements of the intervention 3. Risk-of-bias of included studies
Sensitivity Analysis
Sensitivity analysis was done by repeating the meta-analysis and excluding (1) studies of low methodological quality and (2) studies that were not randomized controlled trials. Further sensitivity analysis was done through (1) identifying studies which disproportionately contributed to the effect size via visualization using Baujat plots, (2) running a leave-one-out meta-analysis where the summary effect size is repeatedly estimated from k-1, where k is the total number of studies, omitting a different study each time (Willis & Riley, 2017) and (3) subgrouping by overall risk-of-bias and reporting the summary effect size of studies rated low overall risk-of-bias only.
Treatment of Qualitative Research
It was prospectively decided that studies which only reported qualitative data would be excluded. For studies reporting mixed data, only quantitative data was extracted for narrative synthesis and meta-analysis.
Summarization of Evidence
A “Summary of findings” table was prepared for the following comparisons: • Meta-analysis of single arm studies pooling for prepost standardized mean difference in attitudes towards EOL and ACP • Meta-analysis of two-arm studies pooling for standardized mean difference in attitudes towards EOL and ACP at follow-up between intervention and control group participants • Meta-analysis of single-arm studies pooling for mean proportion of participants which adopted EOL-related or ACP behavior postintervention • Meta-analysis of two-arm studies pooling for relative risk of adopting EOL-related or ACP behavior postintervention amongst the intervention group compared to the control group.
The results for each of the major primary outcomes as outlined in the types of outcome measures section for comparison would be summarized. Sources and the rationale for each assumed risk cited in the table(s) were reported, and the GRADE system was used to rank the certainty of evidence on the GRADEprofiler (GRADEpro) platform (Alonso-Coello et al., 2016). Two review authors independently rated the certainty of each outcome, and any disagreements were resolved via discussion with the senior author. The certainty of evidence for each outcome was reported according to GRADE using the five criteria: study limitations (risk of bias), inconsistency, indirectness, imprecision, and publication bias.
The levels of evidence were prospectively defined as “high”, “moderate”, “low”, or “very low”. These grades are defined as follows. 1. High certainty: this research provides a very good indication of the likely effect; the likelihood that the effect will be substantially different is low. 2. Moderate certainty: this research provides a good indication of the likely effect; the likelihood that the effect will be substantially different is moderate. 3. Low certainty: this research provides some indication of the likely effect; however, the likelihood that it will be substantially different is high. 4. Very low certainty: this research does not provide a reliable indication of the likely effect; the likelihood that the effect will be substantially different is very high.
Results
Description of Studies
A total of 36,394 abstracts were identified from CINAHL, Cochrane Central Register of Controlled Trials, Embase, PsycINFO and PubMed from their respective dates of inception to 20 July 2025, of which 20, 126 were screened against the selection criteria after removing duplicates. 374 full-texts were sought for retrieval and assessed for inclusion. A total of 83 studies were included in this review, of which 67 studies were included in the meta-analysis. The study selection process is summarized in the PRISMA flowchart (Figure 2). PRISMA Flowchart of Study Inclusion
Included Studies
Study Design
Amongst the 83 included studies, 28 (33.7%) studies were randomized controlled trials (RCTs), 24 (28.9%) studies were quasi-experimental, 16 (19.3%) studies were prospective observational studies, 14 (16.9%) studies were cross-sectional in design while 1 (1.2%) study was a retrospective observational study.
Setting
Amongst the 83 studies, most studies 46 (55.4%) recruited directly from the community, while 27 studies (32.5%) recruited participants at outpatient or primary care clinics. 5 studies (6.0%) recruited from faith-based settings such as churches, 3 studies (3.6%) recruited participants from a rural community, 1 study (1.2%) recruited from a homeless shelter while 1 study (1.2%) recruited from senior citizen centers.
Population
Amongst the 83 studies, 32 studies (38.6%) recruited healthy participants of all age groups, 30 studies (36.1%) recruited specifically the elderly age group with minimal age cut-offs from 50 to 75 years old, 15 studies (18.1%) recruited community-dwelling participants with known non-terminal disease that are currently seeking and or undergoing treatment, 4 studies (4.8%) specifically recruited vulnerable populations such as the homeless, and 2 studies (2.4%) recruited participants with known cognitive impairment.
Interventions
Amongst the 83 studies, 29 (34.9%) studies primarily implemented a workshop intervention to introduce and discuss EOL and/or ACP-related topics, 20 (24.1%) studies implemented one-to-one counseling for the participants and 15 (18.1%) studies organized a discussion group for the participants centered around EOL and ACP. 12 (14.5%) studies designed and disseminated printed or online materials on EOL and ACP topics amongst the participants, 4 (4.8%) studies employed a modified advanced directive (AD), 2 (2.4%) studies implemented a large-scale public education initiative while 1 (1.2%) study employed a modified AD information system. Amongst studies which employed a control, namely the RCTs and quasi-experimental studies, these typically exposed participants to usual care without additional EOL or ACP counseling.
There were some similarities and distinctions between the different categories of interventions. Amongst studies which implemented one-to-one counselling as the primary intervention, study participants received advice, counselling and support from a single dedicated professional which may include social workers (Heyman & Gutheil, 2010; Pearlman et al., 2005), nurses (Overbeek et al., 2018) and physicians (Duffield & Poszamsky, 1996; Kaplan-Weisman et al., 2020) trained in EOL or ACP counselling. Counselling was often longitudinal with repeated check-ins done through home visits (Park et al., 2025), telephone calls (Molloy et al., 2000) or clinic consults (Kaplan-Weisman et al., 2020). Such interventions were intended to offer longitudinal and personalized support to each participant towards eventually realising specific ACP or EOL behavioral endpoints.
Meanwhile, studies implementing EOL group discussions gathered study participants with other individuals of similar disposition or medical conditions. Discussions were then led by a facilitator that can be a study team member, healthcare worker or counsellor trained in EOL or ACP. Some discussions were further framed within a previously designed EOL or ACP curriculum (Gutheil and Heyman, 2005), with facilitators using a brochure, booklet or some tool which can include conversation cards (Jia et al., 2021; Van Scoy, Reading, et al., 2017) to lead the discussion. Emphasis is placed on prompting participants to share their own knowledge, attitudes and practices towards EOL or ACP, and to provoke behavioral or attitude changes from hearing the experiences of others.
Workshop interventions were often educational in nature and primarily intended to educate participants on the objectives and outcomes of early EOL conversations and ACP. These interventions were often held in groups, and were either one-off sessions (Hinderer & Lee, 2019; Haywood et al., 2023) or a curriculum with multiple workshops conducted over a few weeks (Bravo et al., 2016; Chiu wu et al., 2020). Modalities within this intervention comprise viewing audiovisual materials (Nouri, Tan, et al., 2023; Wong et al., 2022), sharing sessions from EOL and or ACP professionals (Beltran et al., 2025; Chiu wu et al., 2020) and interactive activities such as role-play (Davies et al., 2023) and card-games (Phenwan et al., 2025).
For studies implementing modified AD, this involved designing AD forms to be more user-friendly and culturally diverse, often with input from target demographics. Modifications include altering language for simplicity and brevity to a basic reading level (Song et al., 2010; Sudore et al., 2007) and including culturally-relevant graphics alongside presented options (Sudore et al., 2008). Such redesigns were intended to lower barriers to understanding and completion, as well as to render EOL and ACP concepts more relatable across different cultures.
Lastly, studies which distributed printed or online material as an intervention involved presenting participants with printed educational materials for them to refer to at their own time (Hamel et al., 2002; Thulesius et al., 2002), or a website with multimedia educational resources (Lindquist et al., 2017; Sudore et al., 2017a). Some studies further designed the educational material to be more culturally appropriate as the target demographic was specific to an ethnicity (Sudore et al., 2017a, 2018). Other studies designed websites which guided participants step-by-step through the ACP process, which enhanced interactivity of the intervention (Skolarus et al., 2021). This intervention does not involve additional EOL and ACP counselling or any other form of interaction and thus was highly dependent on the motivation of each individual participant.
Excluded Studies
Amongst the 291 excluded studies, 184 (63.2%) were excluded as they were of the wrong publication type. These include editorials, reviews, journal letters or any other paper that did not report primary data or fully communicate its methodology and findings as usually done in a research article. 54 (18.6%) studies were purely descriptive in nature whereby quantitative outcomes were absent. 28 (9.6%) studies investigated populations that were unsuitable for our research question as they either included participants with terminal illness, participants who are currently hospitalized or residing in care facilities, or targeted interventions at caretakers or loved ones of those with terminal illness. 20 (6.9%) studies did not employ their interventions in the community, instead implementing them within the context of a healthcare institution or facility. 3 (1.0%) studies were not in English and 2 (0.7%) studies were preprints and therefore not peer-reviewed.
Risk of Bias in Included Studies
Risk-of-bias assessment was done using the NICE quality appraisal checklist for each study independently by two assessors, with complete agreement between the two assessors following consensus-making discussions.
Of the 83 studies, 44 studies (53.0%) were rated as low risk-of-bias overall, 26 studies (31.3%) were rated as moderate and 13 studies (15.7%) were rated as high risk-of-bias. (Figure 3(a) and (b)). (A) Traffic Light Plot of Risk-Of-Bias by Study as Assessed With the National Institute for Health and Care Excellence (NICE) Quality Appraisal Checklists for Quantitative Intervention Studies and Quantitative Association Studies. (B) Traffic Light Plot of Risk-of-Bias by Domain as Assessed With the National Institute for Health and Care Excellence (NICE) Quality Appraisal Checklists for Quantitative Intervention Studies and Quantitative Association Studies
The “Population” domain assessed the description and representativeness of the sample included in a study. Of the studies rated low risk-of-bias for this domain, they described the baseline characteristics of the included population thoroughly, identified a specific target population in their study objectives, outlined clear inclusion and exclusion criteria, and eventually the recruited participants were representative of those criteria.
The “Allocation” domain assessed the process of allocating participants to exposure groups, and control if necessary. RCTs and quasi-experimental studies which were rated low risk-of-bias for this domain described rigorous randomization of participants. These studies also ensured that no cross-contamination occurred, which in this context meant that control participants were not exposed to EOL or ACP-initiating conversations or tools. Furthermore, these studies ensured that all other factors, apart from the implementation of EOL or ACP-initiating interventions, were accounted for and kept as similar as possible between intervention and control participants. For all studies that were rated low risk-of-bias in this domain, the studies thoroughly described the participant flow throughout the duration of the study and fully reported loss-to-follow up and reasons for such.
The “Outcomes” domain assessed the relevance, completeness and reliability of outcomes measured. Amongst studies which rated low risk-of-bias in this domain, the outcomes collected were relevant to their study aims, such as measuring the uptake of EOL or ACP-related behaviors and attitudes towards the same, reported all primary and secondary outcomes completely and loss-to-follow-up rates, as well as implementing a reasonable follow-up duration, which the assessors set a threshold for three months or more.
The “Analysis” domain assessed the reporting and rigor of analyses undertaken in a study. Studies rated low risk-of-bias in this domain ensured similarity of intervention and control groups at baseline through tests such as Chi-squared tests for homogeneity, did sample size estimation, reported effect sizes where appropriate and reported meaningful effect size precision values.
The “Other Biases” domain assessed the internal and external validity of the study’s results. Studies rated low risk-of-bias for this domain reported unbiased outcomes which were reasonably generalizable to the source population.
Synthesis of Results
Of the 83 studies, 67 (80.7%) were included for meta-analysis. Meta-analysis was conducted for the following primary outcomes: (1) difference in self-reported knowledge, attitude and perceptions towards EOL/ACP either before and after an intervention or between the intervention and control at follow-up and (2) proportion of uptake of EOL/ACP behaviors. Heterogeneity in interventions assessed across included studies was addressed by subgrouping the meta-analysis by intervention types.
Meta-analysis of standardized mean difference was conducted to pool the outcomes from different instruments across included studies.
Early EOL Interventions Improved Uptake of EOL/ACP Behaviors
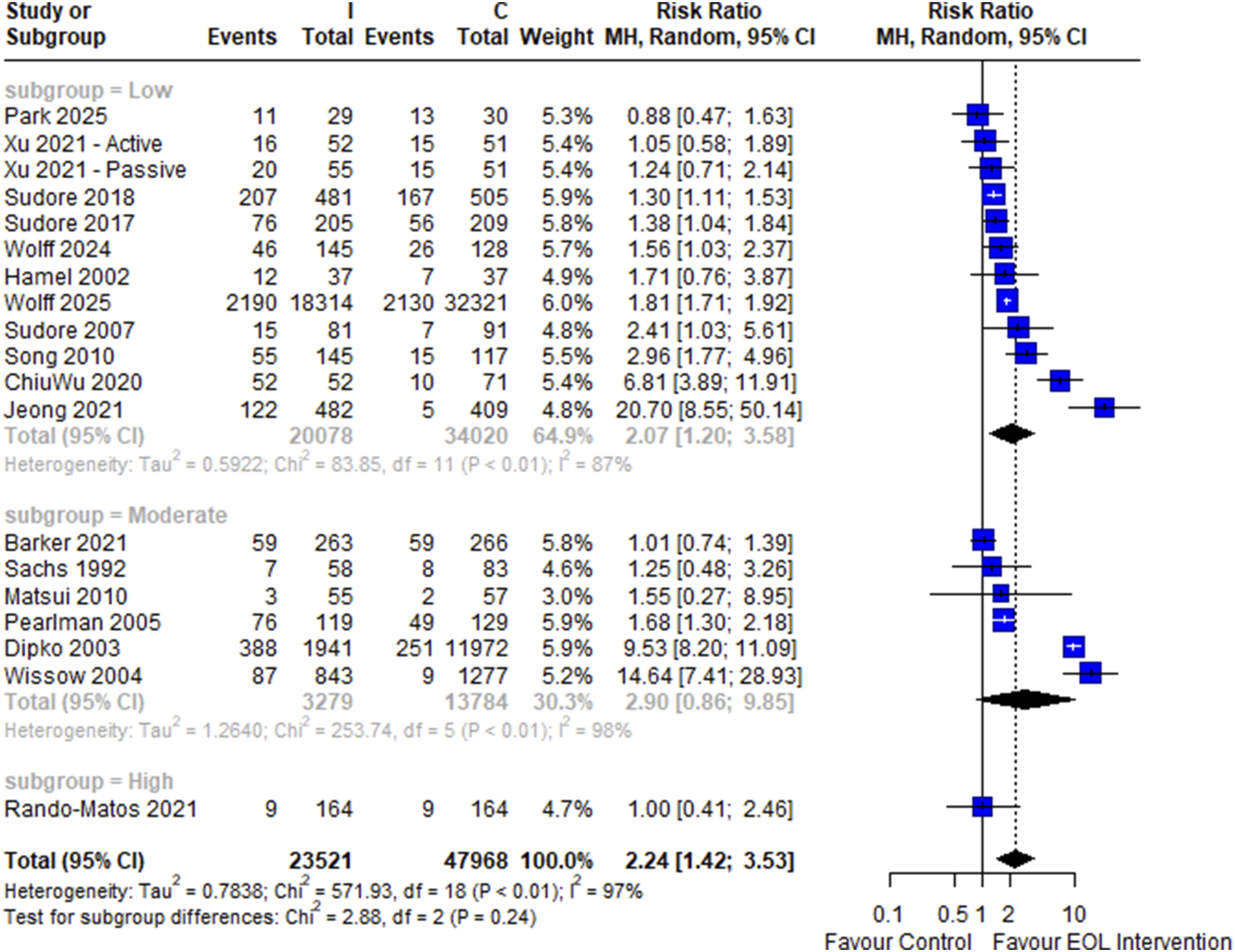
19 studies involving 23,521 intervention and 47,968 control participants were included in the two-arm meta-analysis of pooled risk ratio of carrying out EOL or ACP-related behaviors post-intervention. Early EOL intervention was significantly associated with carrying out EOL or ACP-related behaviors post-intervention (RR = 2.24, 95% CI: 1.42 to 3.53) (Figure 4), with high heterogeneity (I2 = 97%). There was a significant difference between the intervention subgroups (p < .001) and no significant differences between subgroups of overall risk-of-bias (p = .24) (Figure 5). On including only RCTs, early EOL interventions remained significantly associated with postintervention increased EOL or ACP-related behavior (RR = 1.81, 95% CI: 1.22 to 2.68, I2 = 86%) (Figure 6). Forest Plot of Two-Arm Meta-Analysis of Risk Ratio of Uptake of EOL and ACP-Related Behaviour Amongst Participants Receiving the Intervention Over Control, Stratified by Intervention Type Forest Plot of Two-Arm Meta-Analysis of Risk Ratio of Uptake of EOL and ACP-Related Behaviour Amongst Participants Receiving the Intervention Over Control, Stratified by Risk-Of-Bias Forest Plot of Two-Arm Meta-Analysis of Risk Ratio of Uptake of EOL and ACP-Related Behaviour Amongst Participants Receiving the Intervention Over Control Amongst Randomized Controlled Trials Only, Stratified by Intervention Type

28 studies involving 5,569 patients were included in a one-arm meta-analysis to pool the proportion of participants who carried out EOL-associated or ACP behavior after the intervention. The meta-analysis found that close to half of participants demonstrated such behaviors post-intervention (Mean Proportion = 0.46, 95% CI: 0.35 to 0.57) (Figure 7). There was high heterogeneity across the pool of studies (I2 = 98%). An omnibus test did not reveal a significant difference in effect size between the different intervention categories and risk-of-bias subgroups (p = .25, p = .60) (Figures 7 and 8). Forest Plot of Meta-Analysis of One-Arm Pooled Proportion of Post-intervention Uptake of EOL and ACP-Related Behavior, Stratified by Intervention Type Forest Plot of Meta-Analysis of One-Arm Pooled Proportion of Post-intervention Uptake of EOL and ACP-Related Behavior, Stratified by Risk-of-Bias Level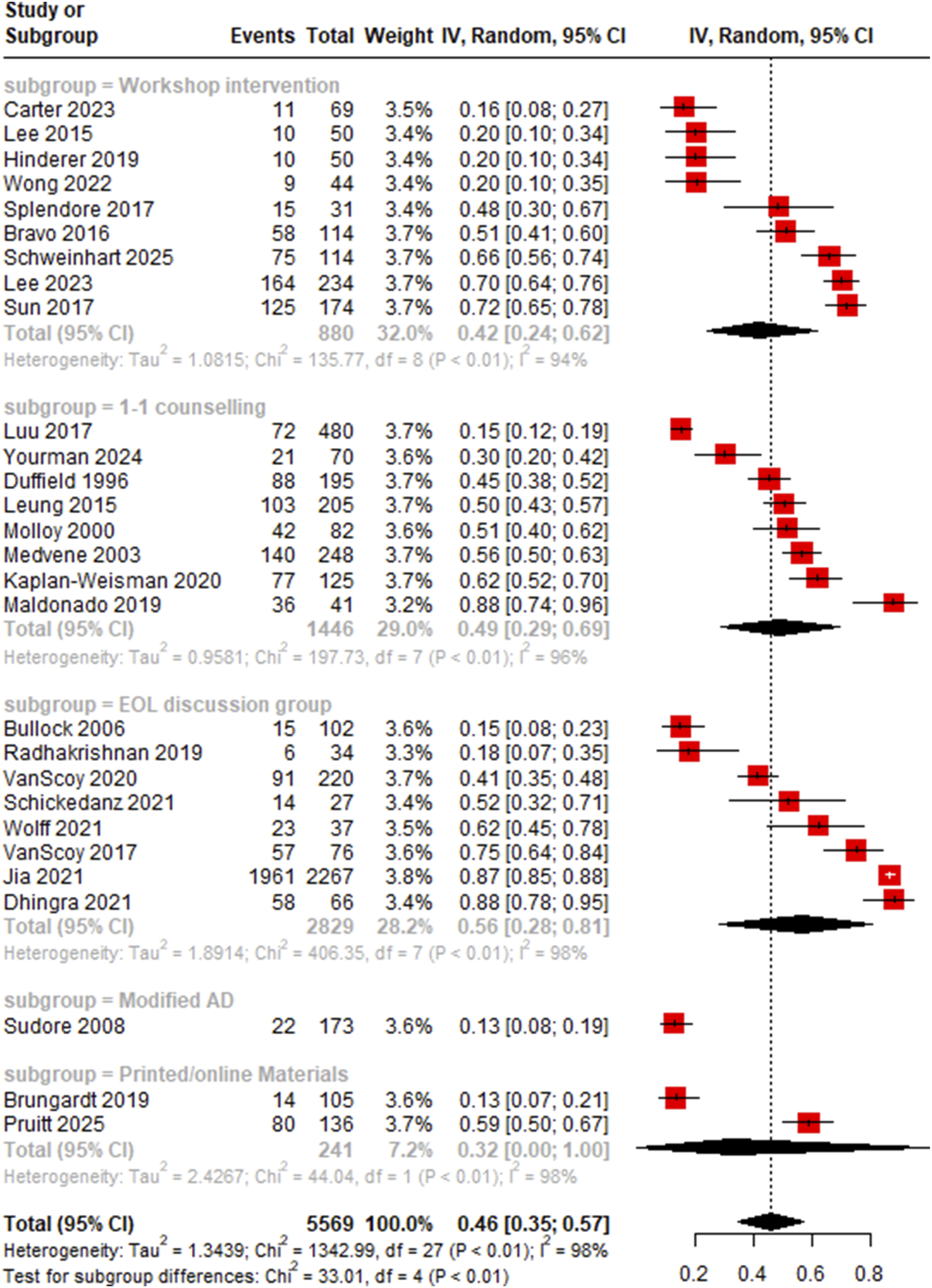

Meta-Regression Results for Two-Arm Risk Ratio of Post-intervention Uptake of EoL and ACP-Related Behavior

*: OR >1 indicates that uptake of EoL and ACP-related behaviours was greater amongst the intervention arm in the respective comparisons compared to the referent group.
Legend: ACP = advance care planning; AD = advance directive; CI = confidence interval; EoL = end-of-life; NA = not applicable; OR = odds ratio.
Meta-Regression Results for Pairwise Comparisons of Two-Arm Risk Ratio of Post-intervention Uptake of EoL and ACP-Related Behavior

*: OR >1 indicates that Intervention 1 was associated with significantly greater uptake than Intervention 2.
Legend: ACP = advance care planning; AD = advance directive; CI = confidence interval; EoL = end-of-life; NA = not applicable; OR = odds ratio.
Meta-Regression Results for One-Arm Pooled Proportion of Post-intervention Uptake of EoL and ACP-Related Behavior

*: Coefficient >0 indicates that a greater proportion of participants undertook EoL and ACP-related behaviours post-intervention.
Legend: ACP = advance care planning; AD = advance directive; CI = confidence interval; EoL = end-of-life; NA = not applicable.
On assessment of publication bias the funnel plot for the two-arm was visually assessed to not be asymmetrical, which corroborated with the Egger’s regression results (p = .727, Figure 9), suggesting absence of publication bias. However, the funnel plot was asymmetrical for the one-arm meta-analysis with a significant Egger’s regression test (p = .02, Figure 10), suggesting possible publication bias. The effect estimates did not vary much across the studies omitted in the leave-one-out analysis, demonstrating that none of the studies disproportionately contributed to the effect size (Figures 11 and 12). Funnel Plot of Two-Arm Meta-Analysis of Risk Ratio of Uptake of EOL and ACP-Related Behaviour Amongst Participants Receiving the Intervention Over Control, Categorized by Intervention Type Funnel Plot of Meta-Analysis of One-Arm Pooled Proportion of Post-intervention Uptake of EOL and ACP-Related Behavior, Categorized by Intervention Type Leave-One-Out Analysis of Meta-Analysis of One-Arm Pooled Proportion of Post-intervention Uptake of EOL and ACP-Related Behavior Leave-One-Out Analysis of Two-Arm Meta-Analysis of Risk Ratio of Uptake of EOL and ACP-Related Behaviour Amongst Participants Receiving the Intervention Over Control



Early EOL Interventions Improved Attitudes Towards EOL/ACP
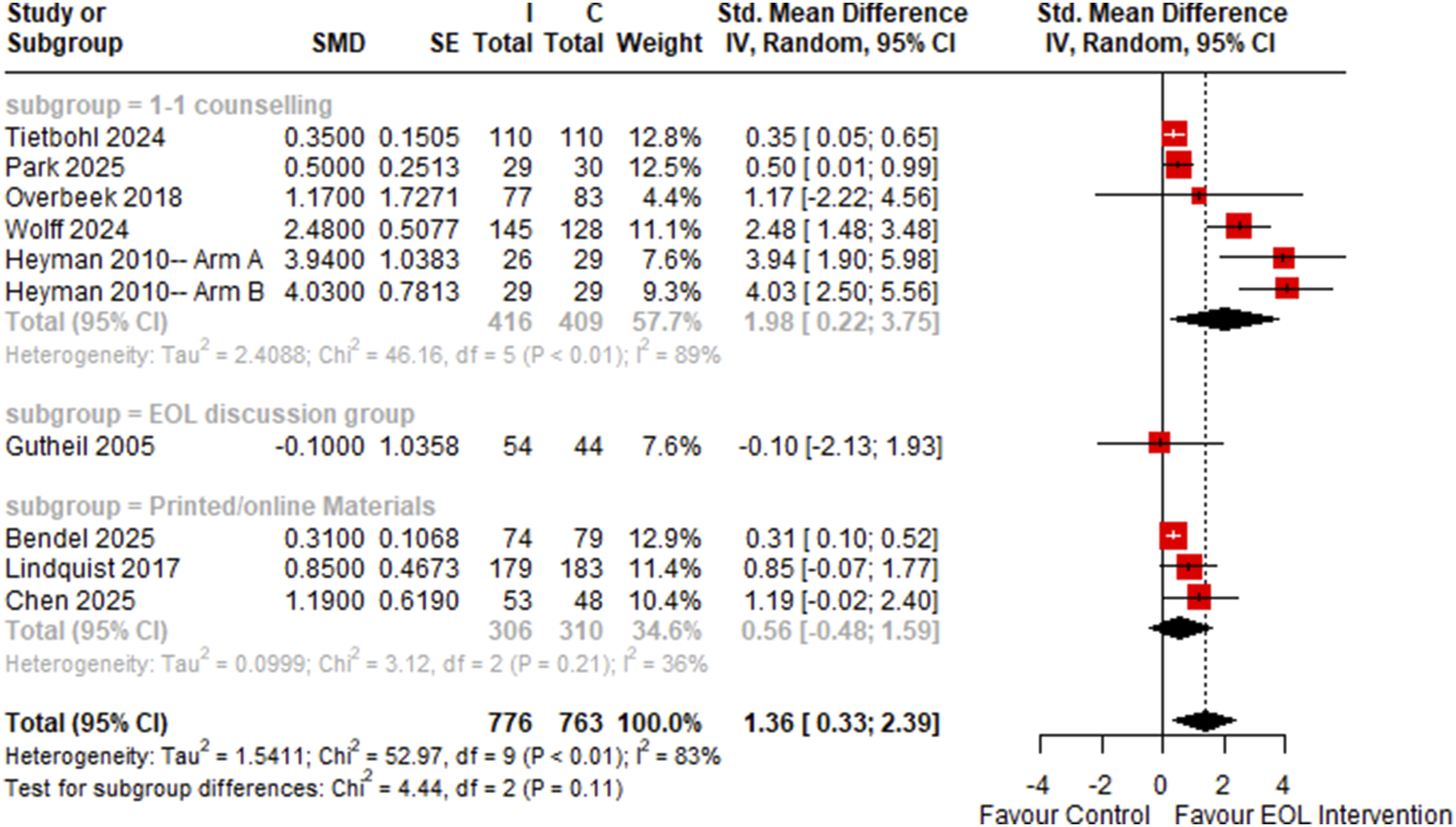
12 studies involving 841 control and 925 intervention participants were included in the two-arm meta-analysis of post-intervention attitudes towards EOL and ACP. Employing early EOL interventions were significantly associated with more positive attitudes towards EOL and ACP (SMD = 1.24, 95% CI: 0.42 to 2.06) and was highly heterogeneous (I2 = 87%) (Figure 13). On omnibus testing, overall risk-of-bias was a significant predictor of effect size (p < .01, Figure 14) while intervention type was not a significant predictor (p = .21, Figure 13). Amongst RCTs only, early interventions remained significantly associated with an increase in post-intervention positive attitudes towards EOL and ACP (SMD = 1.36, 95% CI: 0.33 to 2.39, I2 = 83%) (Figure 15). Forest Plot of Two-Arm Meta-Analysis of Standardized Mean Difference Between Intervention and Control Knowledge, Attitude and Perception Scores, Stratified by Intervention Type Forest Plot of Two-Arm Meta-Analysis of Standardized Mean Difference Between Intervention and Control Knowledge, Attitude and Perception Scores, Stratified by Risk-Of-Bias Level Forest Plot of Two-Arm Meta-Analysis of Standardized Mean Difference Between Intervention and Control Knowledge, Attitude and Perception Scores Amongst Randomized Controlled Trials Only, Stratified by Intervention Type

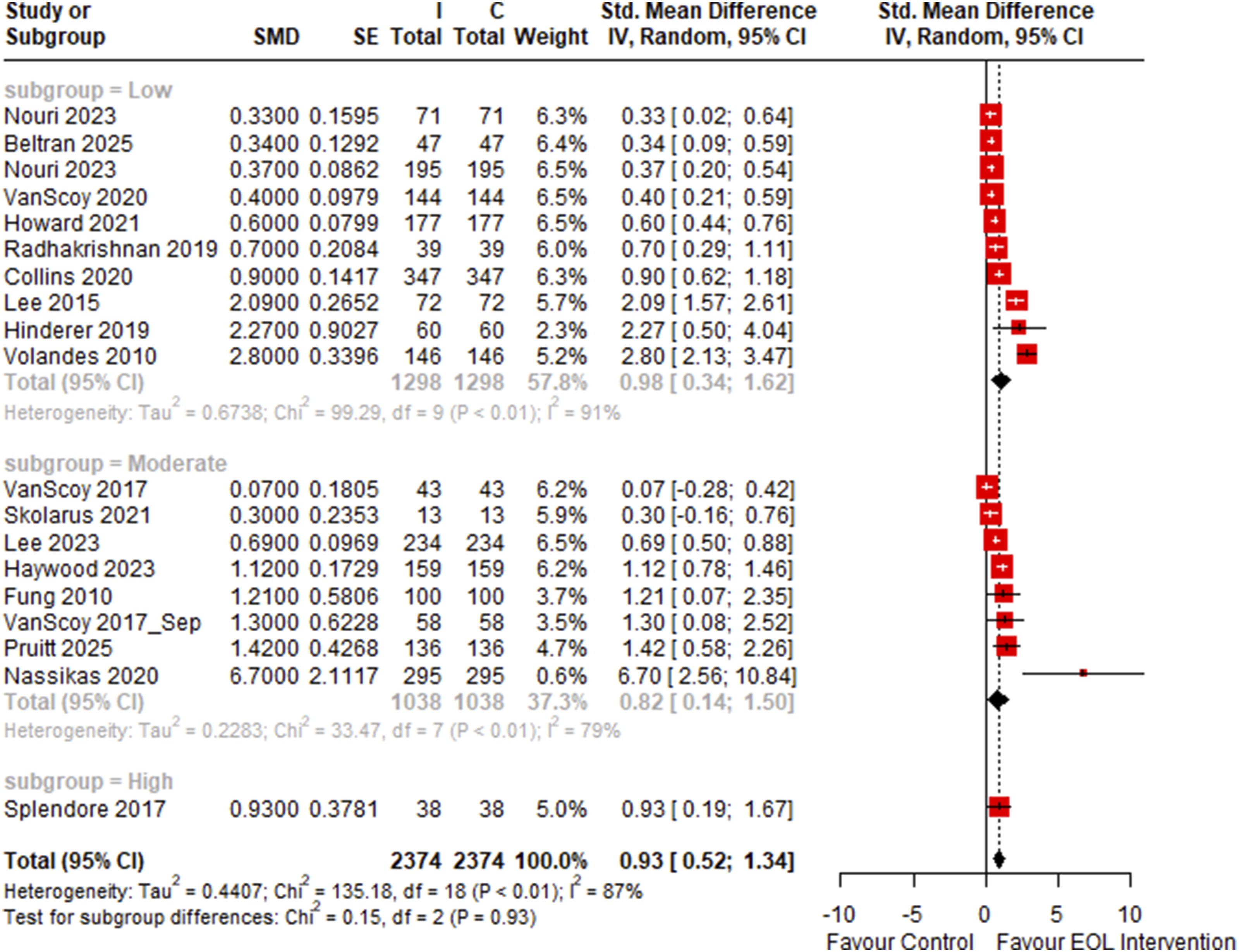
19 studies involving 2,374 participants were included in a one-arm meta-analysis of standardized mean difference of attitudes towards EOL and ACP before and after an intervention. Early EOL interventions were associated with more positive attitudes towards EOL and ACP post-intervention (SMD: 0.93, 95% CI: 0.52 to 1.34). The meta-analysis was highly heterogeneous (I2 = 87%) (Figure 16). On subgroup analysis, only workshop interventions (SMD: 1.24, 95% CI: 0.37 to 2.11), were significantly associated with more positive attitudes towards EOL and ACP amongst participants post-intervention. The effect of intervention on EOL and ACP attitudes was invariant with intervention type (p = .22, Figure 16) and risk-of-bias (p = .93, Figure 17). Forest Plot of One-Arm Meta-Analysis of Standardized Mean Difference Between Pre-Intervention and Post-Intervention Knowledge, Attitude and Perception Scores, Stratified by Intervention Type. Legend: C = Control, I = End-of-Life Intervention Forest Plot of One-Arm Meta-Analysis of Standardized Mean Difference Between Pre-Intervention and Post-Intervention Knowledge, Attitude and Perception Scores, Stratified by Risk-of-Bias. Legend: C = Control, I = End-of-Life Intervention
On assessment of publication bias for both one-arm and two-arm studies, funnel plots were visually assessed to be asymmetrical (Figures 18 and 19) and on corroborating with Egger’s regression, it was significant for publication bias amongst one-arm studies (p = .022) two-arm studies (p = .00285). The meta-analysis was robust to leave-one-out analysis in both studies, demonstrating that none of the studies contributed disproportionately to the summary effect size (Figures 20 and 21). Meta-regression demonstrated that overall risk-of-bias level and duration of intervention were significantly associated with post-intervention EOL and ACP attitudes amongst two-arm studies (Table 5) while study design and publication year were significantly associated with post-intervention attitudes amongst single-arm studies (Table 6). Funnel Plot of One-Arm Meta-Analysis Standardized Mean Difference Between Pre-Intervention and Post-Intervention Knowledge, Attitude and Perception Scores, Categorized by Intervention Type Funnel Plot of Two-Arm Meta-Analysis of Standardized Mean Difference Between Intervention and Control Knowledge, Attitude and Perception Scores, Categorized by Intervention Type Leave-One-Out Analysis of One-Arm Meta-Analysis of Standardized Mean Difference Between Pre-Intervention and Post-Intervention Knowledge, Attitude and Perception Scores Leave-One-Out Analysis of Two-Arm Meta-Analysis of Standardized Mean Difference Between Intervention and Control Knowledge, Attitude and Perception Scores Meta-Regression Results for Two-Arm Standardized Mean Difference of Post-Intervention EoL and ACP-Related Attitudes *: Coefficient >0 indicates that the difference in post-intervention EoL and ACP-related attitudes between the intervention and control arms were favored the intervention more in the comparison groups compared to the referent group. Legend: ACP = advance care planning; AD = advance directive; CI = confidence interval; EoL = end-of-life; NA = not applicable. Meta-Regression Results for One-Arm Standardized Mean Difference of Prepost Change in EoL and ACP-Related Attitudes *: Coefficient >0 indicates that EoL and ACP-related attitudes were more positive post-intervention. Legend: ACP = advance care planning; AD = advance directive; CI = confidence interval; EoL = end-of-life; NA = not applicable.





Discussion
Summary of Main Results
To our knowledge, this is the first systematic review to comprehensively appraise the evidence regarding community-based interventions to initiate EOL and ACP conversations, which demonstrated the positive effect of such interventions on improving knowledge, attitude and perceptions towards EOL/ACP as well as related behavioral change. Our SRMA shows that early EOL community interventions increased positive attitudes by 1.24 SMD (95% CI: 0.42 to 2.06) and EOL and ACP-related behavior by 2.24 times (95% CI: 1.42 to 3.53) compared to usual care. Interventions may be grouped into (1) workshops, (2) one-to-one counselling, (3) discussion groups, (4) printed and online materials, (5) modified AD and (6) others, with distinctive features of each.
Factors of Effective EOL Interventions
Generally, community-based interventions were associated with more positive KAP scores towards EOL/ACP. Most studies measured EOL/ACP KAP through the 15-item ACP Engagement Survey (ACPES) (Sudore et al., 2013), which assessed knowledge, contemplation, self-efficacy, and readiness of the user towards ACP. Included studies used various renditions of the ACPES, such as the extended (Van Scoy et al., 2020) and abbreviated (Yeung et al., 2023) versions as well as translations (Park et al., 2025). As the ACPES is a relatively recent tool, earlier studies often include investigator-designed questionnaires which also evaluated similar constructs of knowledge towards ACP and EOL, and attitudes which included factors such as anxiety (Payne et al., 2009), self-efficacy (Lindquist et al., 2017), perceived usefulness (Yourman et al., 2024) or willingness to engage in ACP (Bullock, 2006). Extensive heterogeneity was expected, which informed the a priori decision to conduct a meta-analysis of standardized mean differences. The study team further included the overall ACPES score as the endpoint analyzed in the meta-analysis as much as possible to reduce any bias that might arise from instrument heterogeneity due to factors apart from the difference in scales.
Additionally, these interventions were also associated with greater uptake of EOL/ACP-related behaviors. This was differentiated from KAP scores, especially the construct of “Practice”, as we had defined KAP to be self-reported, whereas EOL/ACP-related behaviors included actions such as signing of ADs, advanced care plans and living wills (Schweinhart et al., 2025; Splendore & Grant, 2017; Sun et al., 2017; Wolff et al., 2024), engaging in EOL conversations with a care provider (Bravo et al., 2016; Brungardt et al., 2019) or naming of surrogates (Overbeek et al., 2018; Wolff et al., 2024). The measurement of uptake of such behaviors was more objective, as these outcomes were extracted from hospital record data since these actions often involved a care provider and hence documented as a clinical encounter. There were other behaviors which were reported by various studies, such as engaging in fact-finding of ACP and EOL processes (Matsui, 2010; Radhakrishnan et al., 2019) or discussing preferences with family members (Dhingra et al., 2021; Yourman et al., 2024). However, we did not include such outcomes in the meta-analysis given the self-reported nature and hence potential bias of these endpoints.
As such, with reference to our initial logic model (Figure 1), the meta-analysis findings demonstrated that the interventions, of which some were further contextualized with input from local community leaders and stakeholders, translated to both short-term, namely self-reported KAP, and long-term, specifically documenting EOL preferences or initiating ACP, outputs which favored greater EOL/ACP adoption amongst community-based, nonterminally-ill adults. Given the lack of individual participant data as well as simultaneous measurement of KAP and behavioral uptake across most studies, we were not able to comment whether a causal sequence existed from intervention to more positive KAP of EOL/ACP to adoption of EOL/ACP behaviors. This presented the need for studies to follow-up individuals over a longer duration with repeated measures to better characterize the trajectory of EOL/ACP engagement postintervention and the concomitant uptake of EOL/ACP-related behaviors. To further extend the impact of EOL/ACP interventions, it might be prudent for future studies to measure other long-term outcomes described in our logic model. At the individual-level, such outcomes include fulfilled goals of care and quality of death, while at a societal level, it would comprise reduced unwanted admissions for terminally ill adults, reduced anxiety, depression and stress amongst caregivers and family members of the diseased and improved societal outlook towards EOL/ACP. These outcomes represent the endpoint of our logic model, as the documentation of EOL preferences or initiation of ACP, outcomes measured in our meta-analysis, are only fruitful if it ultimately improves quality of death for the diseases and quality of life for family members and caregivers throughout the dying and grieving process.
EOL discussion groups and workshop interventions were found to be the more effective methods for engaging participants in the community towards EOL and ACP-related behaviors, possibly due to the meaningful and bidirectional engagement with participants. This was demonstrated by the larger effect sizes in behavioral uptake odds across two-arm studies for subgroups utilizing EOL discussion groups or workshops in the intervention, although the association is insignificant. The majority of studies employing such approaches regularly engaged participants through a multimodal approach. For example, Wu et al. (Chiu-Wu et al., 2020) engaged participants over four weeks through educational pamphlets, video lectures, group discussions and counseling. Furthermore, these interventions often involve community leaders or respected figures to co-create or co-deliver these programs, which led to more culture-appropriate and specific interventions that were favorably received by the target community. For example, Nouri et al. utilized a community-based participatory research methodology to co-create an ACP engagement program for the Latinx community with local members (Nouri, Tan, et al., 2023). As such, ACP events with elements familiar to the Latinx population were held in trusted community spaces and conducted by known community leaders, which contributed to its effectiveness. Clearly, the lay referral system and social networks are strong determinants of health and health behavior (South & Phillips, 2014), and is increasingly recognized in EOL care as well (Rosenberg et al., 2016). This is because concerns and ideas surrounding EOL are not universal but rather specific to each community’s cultural characteristics such as language, religious beliefs and habits (Ohr et al., 2017; Toscani et al., 2003). By meaningfully involving the community from conceptualization to execution, EOL and ACP engagement projects can be tailored to each community’s cultural needs. This avoids professionalization of the discourse surrounding EOL and ACP while ensuring trust and participation amongst the community in the program (Noh et al., 2016; Rosenberg et al., 2016). Hence, complex public health interventions, such as EOL and ACP engagement, need to meaningfully involve and engage community members beyond just situating the intervention within the community in order to be effective.
Overall Completeness and Applicability of Evidence
We conducted a comprehensive systematic review of the international literature consisting of a total of 20 title-abstracts and 374 full texts. A total of 83 articles were included across different study designs (e.g. prospective cohort, randomized controlled trials), settings (e.g. community centers, primary care clinics) and interventions (e.g. workshops, 1-to-1 counselling). Thus, we report a complete summary of the existing EOL community interventions up till 2024 in the international literature. Our meta-analyses are limited by heterogeneity across such diverse community-based interventions and cultural contexts internationally. Nevertheless, this SRMA serves as a comprehensive summary of existing interventions and can help to inform future community-based EOL intervention design.
Quality of the Evidence
Using the NICE quality appraisal checklist, we found that 44 studies were rated low risk-of-bias overall, 26 were rated moderate and 13 studies were high risk-of-bias.
Generally, there were issues with allocation concealment and blinding of the intervention to both the investigators and participants. However, participant blinding was unfeasible as they had to actively engage with the EOL interventions such as attending workshops and reading educational materials. Meanwhile, investigator-blinding was not routinely practiced in the included studies, which may bias the administration of questionnaires or assessments done. Lastly, the community setting of most studies complicated control over confounders compared to a clinical setting.
Community-Based Interventions Compared to Usual Care Protocols for Promoting End-of-Life and Advanced Care Planning Conversations and Behaviours Amongst the Nonterminally Ill

CI = confidence interval; RR = risk ratio; SMD = standardised mean difference.
Explanations.
aMore than half of the studies were rated as moderate or serious overall risk-of-bias using the NICE quality appraisal checklist.
bStudies used different instruments to measure attitudes and constructs of EOL/ACP attitudes measured were heterogenous across studies as well.
cFunnel plot was asymmetrical with positive Egger’s regression test result (p = .0085).
dStudies were heterogeneous in study design and intervention design.
For similar outcomes amongst two-arm studies, evidence certainty was down-rated by two levels. This was due to serious issues with risk-of-bias, as a significant proportion of studies had moderate or high risk-of-bias, as well as serious issues with inconsistency in outcome measurement As the effect size had a wide confidence interval and was highly variant with sensitivity analysis, there were serious issues with precision as well. Lastly, publication bias was strongly suspected due to asymmetrical funnel plot and a significant Egger’s regression test outcome. Hence, the evidence certainty for this outcome was rated “Low” (Table 7).
For the relative risk of undertaking EOL or ACP-related behaviors amongst those who received community-based interventions compared to those in the control group, evidence certainty was down-rated by one level. This was due to serious issues with inconsistency similar to the previous outcome. Yet, due to the large effect size demonstrated implying a strong association between community-based interventions and increased EOL or ACP-related behaviors, the evidence certainty was rated as “Moderate” (Table 7).
Potential Biases in the Review Process
Amongst the strengths of this review, firstly a review protocol was previously drafted and published to define clearly and transparently the review’s objectives and methodologies (Lim et al., 2021). Furthermore, our research question was well-placed due to the focus on community settings, which increases the applicability and generalizability of our findings to pragmatic settings as compared to clinical studies where interventions and other factors are more tightly-controlled and thus less representative of the real world (Katz et al., 2011). Our meta-analyses were also robust due to the large sample sizes and the reasonable use of imputation methods recommended by Cochrane that did not introduce bias to the analysis (Higgins et al., 2021). Furthermore, we conducted sensitivity analyses by subgrouping by risk-of-bias, including only RCTs, and conducting leave-one-out analyses to test the robustness of outcomes. Lastly, our meta-analyses were of minimal publication and language from the funnel plot assessment and low number of non-English language articles excluded respectively.
However, a few limitations remain. Firstly, we acknowledge that the follow-up duration for most of the included studies did not extend past one year, and thus the long-term effects of community-based interventions remains unclear, especially as participants approach end-of-life in their own lifetimes. However, given the large effect sizes in our meta-analyses, our findings provide some evidence that EOL interventions may be helpful towards facilitating behavioral change in EOL care. Future studies with extended follow-up and repeated measures of EOL and ACP engagement or behaviors, especially of initially asymptomatic older adults up to terminal illness may be warranted. Such studies can then elucidate how various interventions may modify the trajectory of EOL and ACP knowledge, attitudes and practices, as well as the persistence of the intervention effects (Randall & Wolff, 1994). Secondly, there was high heterogeneity in the study designs, interventions and methods of outcome assessment which translated to high heterogeneity in the meta-analyses. This was mitigated through subgrouping by risk-of-bias and intervention types, both of which were significant sources of heterogeneity, which improved interpretability of findings. Furthermore, broad meta-analyses are advantageous due to their greater generalisability across different settings, patient demographics and intervention subtypes (Gøtzsche, 2000). By comprehensively describing and appraising the evidence landscape for all community-based interventions, we demonstrate its association with benefit in diverse settings.
Agreements and Disagreements With Other Studies or Reviews
Prior to this review, only one systematic review on this topic was done in 2013, specifically amongst community-dwelling populations (Abba et al., 2013). Our review only included 1 study out of the 4 included by Abba et al. (Sato et al., 2009), as the three studies only reported qualitative data (Hickey & Quinn, 2012; Sanders et al., 2008; Seymour et al., 2013). Abba et al. concluded that the evidence on different interventions to promote end-of-life care discussions in the general public remains limited, but suggests that participatory approaches may be more beneficial than passive ones. Our review was conducted a decade later and thus included more recent studies. With the increased quantity of evidence, our findings corroborate well with the previous review’s conclusions that participatory methods may have more benefit. We found that workshops and EOL discussion groups, which are more participatory interventions, were more effective in promoting EOL and ACP-related behaviors compared to passive interventions such as reviewing educational material or using a modified AD. Furthermore, both of our reviews also agree on the limited comparability of findings across studies given the high heterogeneity in study methodology and interventions employed in the literature.
Authors’ Conclusions
Implications for Practice and Policy
Our review demonstrated low to moderate evidence for the effectiveness of community-based interventions, such as workshops, one-to-one counselling, discussion groups, modified ADs, and education materials, on increasing EOL or ACP-related behaviors and increasing positive attitudes or awareness towards such related topics. Evidence certainty is partly compromised by high heterogeneity in settings and intervention, and the inconsistency in methodological quality across included studies. These points of consideration ought to be seriously considered by policymakers wishing to implement large-scale programs related to EOL and ACP awareness.
However, investigators and communities are encouraged to explore these interventions nonetheless due to the large and robust effect sizes reported from the various meta-analyses, demonstrating the potential of such interventions. Uncertainty remains as to how effective these interventions remain over the long-term, especially years or decades after exposure when participants actually approach their respective end-of-life phases.
Implications for Research
We highlight key areas of consideration for future investigators conducting research into this or similar fields.
With regards to study design, future studies ought to remain community-based to allow generalizability to a real-life setting. Furthermore, studies ought to include a control arm if possible, in order to control for baseline exposure to EOL or ACP-related communications or content that every individual will experience. This effect is especially pronounced for elderly study populations, due to the age-appropriateness of introducing them to such topics in a healthcare setting. Future studies ought to also control for baseline awareness and acceptability towards EOL or ACP, so as to assess the true effectiveness of the interventions employed.
With regards to outcome measurement, future studies ought to use a standardized instrument to measure ACP awareness and acceptability, such as the Advanced Care Planning Engagement Survey. This ensures results across different studies are more reasonably cross-referenced and interpreted together. Furthermore, studies should make an attempt to follow-up with participants as long as possible, up to their end-of-life phases.
With regards to setting, more studies can be done that recruit ethnically diverse or vulnerable groups. These populations have significantly different sociocultural views towards EOL and ACP preferences compared to the Caucasian or European populations observed in the majority of studies. This can be further enhanced by conducting such studies outside of the North American or Western European regions. It will be interesting to see how ethnicity and geography can affect the effectiveness of such interventions, given how large a role upbringing, prevailing societal values and other sociocultural milieu factors play in shaping one’s views towards end-of-life (Barnato et al., 2009; Kwak & Haley, 2005).
Supplemental Material
Supplemental Material - Community-Based Interventions for Initiating Early End-of-Life Conversations in Nonterminally Ill Adults: A Systematic Review
Supplemental Material for Community-Based Interventions for Initiating Early End-of-Life Conversations in Nonterminally Ill Adults: A Systematic Review by Yong Yi Tan, Shuning Fu, Khi Yung Fong, Samuel Miny, Pin Sym Foong, Noreen Cheng Chan Guek, Gerald Choon Huat Koh, and Mervyn Lim Jun Rui in Campbell Systematic Reviews.
Footnotes
Acknowledgements
We thank Ms. Annelissa Chin, Senior Librarian from the National University of Singapore, Medical Library for her kind assistance with the design of the search strategy and Dr. Zachus Tan, Resident, Singapore General Hospital for his help with reviewing the protocol for this review.
Author Contributions
• Content: Yong Yi Tan, Mervyn Jun Rui Lim.
• Systematic review methods: Yong Yi Tan, Samuel Miny, Mervyn Jun Rui Lim.
• Statistical analysis: Yong Yi Tan.
• Information retrieval: Yong Yi Tan, Shuning Fu, Khi Yung Fong.
All authors have read, reviewed and approved the submitted manuscript draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.