
Abstract
The paper discusses providing (or not) information about coronavirus during the pandemics of COVID-19 in minority languages in Russia. It explores different minority languages, indigenous, and migrant, in the announcements and doctor-patient communications. The study is based on the observation of the linguistic landscape in 4 Russian cities (N=150) and on materials from semi-structured interviews. According to the data, Russian has been the preferred language for communicating official information about COVID-19. Doctor-patient communication in the multilingual regions was also predominantly in Russian, but there is a tendency to use another, minority native language in communication with mid-level medical staff and with all other actors in the rural area. The paper discusses creation of a more trusting relationship between a doctor and a patient by using the native language.
Introduction
The paper examines medical communication and the announcement of information about the COVID-19 pandemic within Russia’s minority language communities. It is based on case studies of indigenous languages, Buryat and Chuvash, in Buryatia and Chuvashia, respectively, and additionally Yakut, as well as the most spoken migrant languages in major cities, namely, Kyrgyz, Tajik, and Uzbek.
Effective communication and linguistic inclusion are particularly crucial during times of crisis. However, paradoxically, most information about COVID-19 is predominantly available in the majority languages, leaving non-majority language speakers in need of translation. As highlighted by Hopkyns and van der Hoven, “in crisis communication, quick decisions need to be made and often monolingual messages are the default choice due to a sense of urgency” (Hopkyns, van der Hoven, 2022: 205). Consequently, individuals who do not speak the majority languages may face exclusion or misinformation.
Especially in the initial stages of the pandemic, when public knowledge regarding appropriate actions was limited and new information emerged daily, the unequal distribution of announcements in the dominant language and minority languages was of utmost importance. It is worth noting that in the case of a pandemic, informing the minority languages directly benefits the linguistic majority by containing the spread of the disease. Visual materials, such as COVID-19 safety signs, played a significant role in public spaces, events, and understanding safety protocols. They were essential for everyone, regardless of their language background.
Throughout the pandemic, various projects emerged, primarily focusing on translating core ideas (such as mask-wearing or social distancing) into minority languages through a combination of machine translation and crowdsourced editing. 1 Additionally, World Health Organization recommended to use infographics for adequate access to COVID-19 health warnings (WHO, 2020). These efforts only required minimal knowledge of the language. However, towards the end of 2020 and throughout 2021, more detailed information regarding vaccination became crucial, including access to vaccines, common immunization inquiries, prioritization criteria, and more. Consequently, it was necessary to provide comprehensive descriptions in minority languages to ensure informed decision-making regarding individual health and safety measures. Achieving such objectives in minority languages necessitates distributing information in each respective community, developing medical vocabulary, establishing terminology, and possessing a solid understanding of communication practices.
How was the announcement and dissemination of information about the COVID-19 pandemic organized in the Russian Federation? This study offers a preliminary analysis of communication in minority languages, drawing from observations made during the pandemic and interviews conducted with native speakers of Chuvash and Buryat. The ultimate goal is to identify a successful model of crisis communication in a multilingual context for practical implementation.
The paper is structured as follows: The Theoretical Approach to the Multilingual Healthcare Communication section provides theoretical background on “crisis translation” and multilingual healthcare communication. The Background of the Study: Multilingualism and Health Care in Russia section discusses the study’s context and explores multilingualism in the Russian Federation. The Methodology section is an overview of the study’s methodology. The Results section focuses on the description of announcements through linguistic landscape materials and social media, along with an analysis of the experiences of minority language speakers during the pandemic. Finally, the Discussion and Conclusion section concludes by discussing the study’s findings and highlighting cases of effective communication, emphasizing the importance of not only disseminating information but also ensuring a deep understanding and trust among all groups.
Theoretical Approach to the Multilingual Healthcare Communication
As many studies show, language-minority patients can be marginalized and a minority language can be a barrier, especially for migrants (Jaeger et al., 2019; Martinez, 2011; Nielsen, Krasnik 2010). The impact of a minority language results in a lack of medical care for indigenous minorities is still less studied; however, it also takes place both in written and oral communication.
The inequality of any minority language, in written form, is reflected in the linguistic landscape inside clinics, in the form of poor, majority-language-only signage. For example, Shuster (2015) proposes an “accessibility index” that quantifies the level of language accessibility of the hospital signage in Israel (iconic signs, Hebrew, English, Arabic, and Russian) (Shuster 2015). Another important issue is an understanding of a signed agreement before care: for example, in the Russian context, the language of such documents is very complicated and formal and is hardly understood by non-native speakers. Further, the difficulties with medical assistance, concerning spoken communication between a healthcare provider and a minority-language-speaking patient highlight this. How, exactly, does a patient from a minority group understand a doctor’s instruction and follow a course of treatment? The development of a more inclusive and patient-oriented system is a great challenge for a multilingual setting.
How can a healthcare system reduce the existing barriers for non-dominant language speakers? There are several possible strategies, then can be structured in four main ways: 1) special language courses for medical workers from majority speaking population during the professional education; 2) medical education for speakers of a minority language or recruiting the doctors from diaspora; 3) a translator/an interpreter for patients; and 4) innovative health communication in the digital age, that is, non-verbal devices or special mobile applications for medical purposes. The classification is rough and in practice, there are combinations of these decisions and there are benefits and disadvantages in every strategy used alone. Some cases are briefly discussed here.
The experience of courses for non-minority-language-speakers shows that it does not resolve all problems with doctor-patient communication but helps, as in the case of a year-long module of isiZulu language teaching for English-speaking medical students in KwaZulu-Natal, South Africa (Matthews & Van Wyk, 2016). The opportunity to get a medical education for minority speakers can be viewed as a more inclusive way, aiming both in social mobility for ethnic minorities and trust-building communication with patients. Medical education is prestigious and expensive, so enrolling in a medical program for minority students needs support. Some countries have specific recruitment policies for indigenous students, for example, the Australian Medical Council requires a certain percentage of minority students (Garvey et al., 2009).
Two other strategies assume a kind of mediation between a doctor and a patient, by human or by tools. The use of professional interpreters was not often adapted to the context of multilingual healthcare; more often there are “cultural brokers” within the mid-level medical community and relatives of a patient in South African healthcare settings (Penn, Watermeyer 2018). The professional translators often provide the help with written communication with clinics, especially for foreigners seeking around-the-globe treatment of serious or rare medical conditions. The presence of an interpreter in a hospital is hampered by the current organization of work (especially in the pandemics' context under discussion) as well as ethical responsibilities and restrictions. Thus, in oral communication, mediated by “cultural brokers,” patients and their companions obtain just quick and restricted communication with medical workers. A possible solution is increasing the quality of machine translation. The translation of the sufficient information can be provided by interactive screens in clinics and digital devices (see, for example, Canopy App or Starling Health mobile applications 2 ). The development of mobile tools for multilingual healthcare communication, as a part of telemedicine, are increasing nowadays; however, it is still often not enough for adequate communication on sensitive topics.
The notion of “crisis translation” (Federici, O'Brien 2020) concerns different disasters, that is, earthquakes or tsunamis and pandemics. It is tightly connected with the current pandemic of COVID-19. “Multilingual crisis communication” (Piller et al., 2020) presupposes an effect of quick and informative translation. There is an important balance between machine and human translation, a native speaker translator, and a person who is familiar with medical terminology. There are different goals from translation for specific purposes, a translation of medical scientific papers and reports for medical workers, and a translation of rules of social distancing. The pandemic has also revealed the risks associated with delays in translation and miscommunication. It has resulted in both a lack of time and resources (i.e., the absence of professional translators for many minority languages, the cost of printing parallel texts, etc.) and the linguistic difficulties in medical terminology. In multilingual countries, the texts in different languages have mistakes or provide only minimal information, see Peru, Bolivia, and Ecuador (García et al., 2020).
At the early stage of the pandemic, a lack of linguistic inclusion in COVID-19 public signage in different multilingual settings was observed (Chen, 2020; Garcia et al., 2020; Hopkyns, van der Hoven 2022). At the same time, a quick response to language planning for new challenges can be part of an official language policy: “Guidebook of Wuhan Dialect for Medical Assistance” was created in a short time in reaction to understanding the differences between standard Chinese and the Wuhan dialect at the beginning of the COVID-19 pandemic (Piller, 2020). At the same time, the local and bottom-up levels of language planning are more effective than the top-down. Zhang and Zhao (2020) emphasize the role of “micro-influencers” in making the attitudes of the diaspora and circulating the information about the virus. I. Piller and co-editors of the special issue on multilingualism in the pandemic, reinforce the importance of collaboration between policymakers, activists, and linguists for being ready for further crises (Piller et al., 2020).
The inclusion of “local and indigenous knowledges and grassroots practices” (Piller et al., 2020: 512) can help with a translation in the time of global crises and leads to multilingualism in health communication in the framework of the agenda of Language and Social Justice (Piller, 2016). It also reveals the agency of native speakers which is an important notion for modern LPP (Bouchard & Glasgow 2019, Ricento, 2000). This study follows the approach and takes into account the local level and grassroots initiatives. How do religious and cultural institutions, small business enterprises, or NGOs provide help to minority people during the pandemic? Through analysis of my ethnographic data, I developed a framework to categorize the practices of crisis communication that I had observed.
Background of the Study: Multilingualism and Health Care in Russia
The examples of minority languages chosen for analysis are relatively benign in terms of language loss. According to the latest census of 2020–2021, there were 800,100 Chuvash speakers, 392,979 Buryat speakers and 479,484 Yakut speakers (Russian Population Census 2020). These languages are official in their respective regions (the Republic of Chuvashia, the Republic of Buryatia, and the Republic of Sakha) and are used to address state bodies, write laws, conduct court proceedings, and for mass media and signage, as stated in the constitutions of the republics (Buryatia, 1992; Chuvashia, 2003; Yakutia, 1992). The government’s policies often contradict each other, with official support programs for minority languages existing alongside discriminatory regulations on multilingual signs (Baranova, Fedorova, 2020b).
Language planning encompasses not only legislative measures at different levels, but also practical initiatives undertaken by various entities. While the mandatory duplication of state body signs and official information into the official languages of the republics does not consistently occur, there have been notable advancements in this regard. In Buryatia (Ivanov, 2021), Chuvashia (Alòs i Font, 2019), and Yakutia (Ferguson, Sidorova 2018), the prevalence of minority-language signs have been on the rise in recent years. Business owners frequently opt for names in their native languages, which resonate with the local population. Additionally, language activists actively monitor the provision of official information in minority languages, further promoting linguistic diversity and inclusivity.
The Russian megalopolises, Moscow and St. Petersburg, are multilingual places but I predominantly took into account the languages from Central Asia, Uzbek and Kyrgiz (both Turkic) and Tajik (Iranian) spoken by the main migrant groups in Moscow and St. Petersburg. Although these languages are not legally supported in any way, they are sometimes used in the linguistic landscape, including in official announcements (Baranova. Fedorova 2020a).
The linguistic barrier and lack of information in minority languages pose significant challenges in Russia. It is important to note that linguistic exclusion primarily affects labor migrants from Central Asia, as most indigenous speakers typically speak Russian and other foreigners often have access to information in English. Over the past few decades, rapid economic development and waves of immigration have transformed cities like St. Petersburg and Moscow into diverse hubs with people from various social, cultural, and linguistic backgrounds. However, the understanding and recognition of linguistic diversity have been slow to progress, with recent indications of a shift away from the monolingual ideology (Baranova, Fedorova 2020c).
A particular aspect of linguistic (in)equality manifests in the realm of medical treatment. It should be noted, that multilingual medical needs in the past pandemics like flu or other vaccinations was almost not given to consideration. Regular medical needs are also neglected, especially for migrants rather than native speakers.
Medical organizations and business structures catering to migrants often overlook the need for multilingual support and fail to address potential comprehension issues with texts exclusively in Russian. Barriers to accessing healthcare services for labor migrants in Russia predominantly arise from their legal and financial status. To overcome limited access, working migrants from Central Asia employ different strategies. In St. Petersburg, for example, these strategies include delaying seeking help and waiting for a trip back to their home country, as well as seeking advice from friends or pharmacy workers (Kuznecova, 2018). Additionally, immigrants often establish parallel medical infrastructure, such as “Kyrgyz Clinics” in Moscow staffed by healthcare professionals from Central Asia (Kashnitsky, Demintseva, 2018). These clinics provide affordable medical treatment and cater to patients who share common languages, traditions, or religious beliefs with the doctors. However, doctors in Kyrgyz clinics not only serve their compatriots but also attend to immigrants from other backgrounds and even Russian citizens with low incomes.
In times of crisis, a lack of understanding regarding multilingualism can have critical consequences. Many working migrants have limited proficiency in Russian, and during the pandemic, they were unable to return to their home countries and continued to work in delivery and other services even during lockdowns. In terms of medical treatment, inequality is evident in the context of vaccination during the pandemic, as foreigners often have to pay for immunization in Russia.
For indigenous minority languages, the situation in healthcare is relatively better based on the citizenship of native speakers. There are minority language courses for doctors and mid-level healthcare staff, such as those offered in the Republic of Chuvashia or the Republic of Tatarstan. 3 Medical terminology has been developed for most minority languages with official status, for example, for Chuvash, one of the languages in this study there is a special dictionary of medical terminology (Ivanov, Minnebaev 1998). There are videos in Buryat on the Health Center website about healthy eating, and on a heart attack. 4 After the pandemic ended in 2022, a Russian-Buryat medical phrasebook for doctors was published (Baikal Daily, 2022).
However, the linguistic inclusion of indigenous language speakers remains problematic. There is no state-level program to support multilingualism in healthcare, even in regions of Russia with multilingual populations. There is also a lack of specific programs aimed at encouraging students from minority groups to pursue medical education. The language courses are very short and are intended mainly for mid-level medical professionals, not doctors.
Methodology
The paper aims to describe the linguistic inclusion in the COVID-19 pandemic in Russia (2020–2021). The research is based on the analysis of two sets of data: 1) public data: signs in linguistic landscapes, official communication and announcements, posts, and comments in social media related to the pandemic and 2) semi-structured interviews with minority language speakers of their experience during the pandemic.
The first step of analysis deals with public signage. The data include some materials in linguistic landscape (LL) and the social media on Turkic and Mongolic languages. The choice of data is due to the fact that the first information about the pandemic for city dwellers was got from the linguistic landscape: the announcements in health clinics, the safety rules in the public space, and the specific requirements for transport that changed very quickly. In summer of 2021, I collected signs in the Republic of Chuvashia (Yadrinskiy district and Cheboksary, the capital) and in Yakutsk, the capital of the Republic of Yakutia, and two multilingual cities, St. Petersburg and Moscow. Not having the materials from Buryatia, I asked the respondents about linguistic landscape of Ulan-Ude. The data are not quantitatively equal, due to the restricted mobility during the lockdowns (most photos were from St Petersburg, where I lived, and other places represented observations from limited short trips). In total, I have collected over 150 photos related to COVID precautions or other things related to the disease, such as vaccinations. Additionally, it analyzes some online data concerning the COVID-19 pandemic in Kalmyk, Buryat and Chuvash.
The second part of the materials consists of 20 conducted semi-structured interviews with native speakers of Buryat (Mongolian), Chuvash, and Yakut (both Turkic languages). These interviews delve into the experiences of multilingual individuals during the COVID-19 pandemic, encompassing both those who fell ill and those who received vaccination. I specifically chose minority languages with official status, as opposed to including different migrant groups, due to their juridical status and the potential for receiving treatment. To capture a comprehensive picture, I focused primarily on middle-aged and elderly respondents. This decision was influenced by the tendency of younger individuals to overlook their health, leading them to not consider the pandemic as a significant risk. Additionally, the younger Chuvash and Buryat populations are experiencing a language shift towards Russian. To investigate these challenges, I collected the interviews in a rural area of the Republic of Chuvashia, and conducted online interviews with Buryat native speakers between 2021 and 2022. Two additional interviews were obtained from Yakutia (the Republic of Sakha).
Results
The linguistic landscape and public announcements during the pandemic
According to observations in Yakutia and Chuvashia, there is a lack of health warnings in the Yakut and Chuvash languages. Respondents from Ulan-Ude, Buryatia, mentioned that they rarely saw signs in Buryat. Some exceptions were found in private businesses and a creative space, suggesting that these signs may be part of language activism by the owners or artists (see Picture 1). In the considered area, it is important to determine whether the absence of multilingual information hinders access to information for these populations or if they are able to read Russian. Only one person from a small town mentioned bilingual signs in a health clinic, providing instructions on handwashing and other information (female, Buryat, 60 years old). It should be noted that the lack of multilingual information does not necessarily hinder access to information for these minority groups, as they are able to read Russian. Buryat, Russian, and English sign in Ulan-Ude.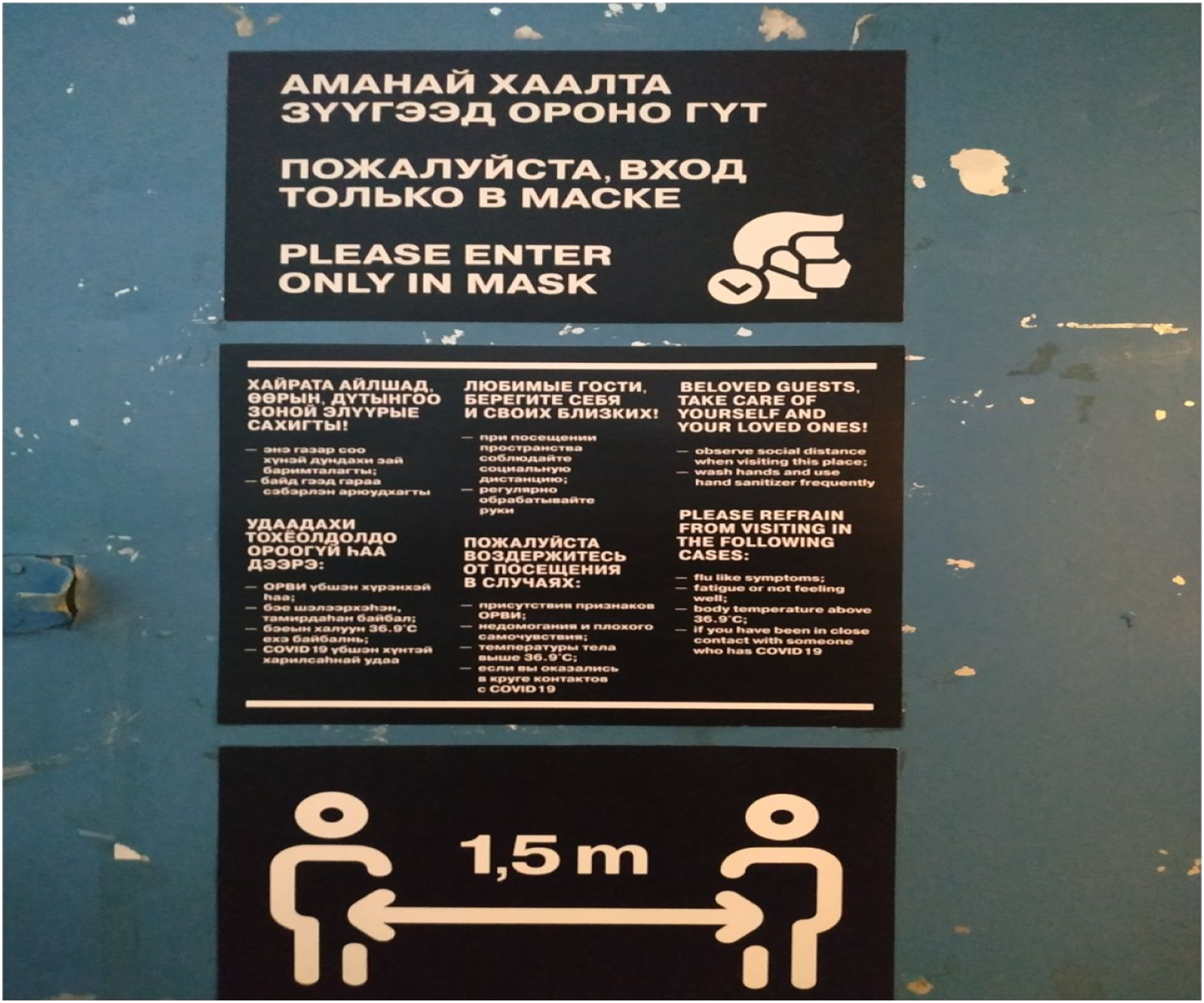
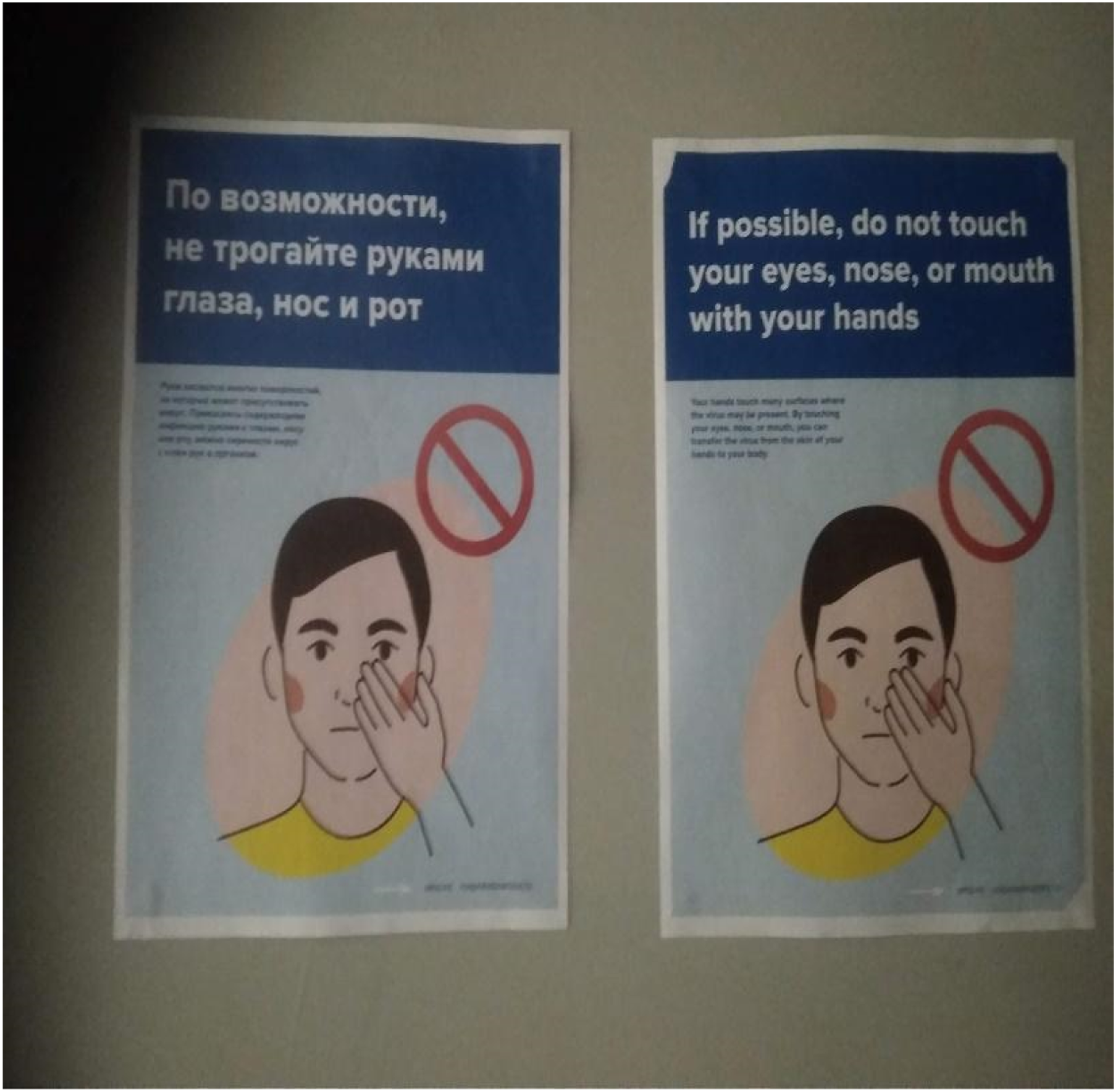
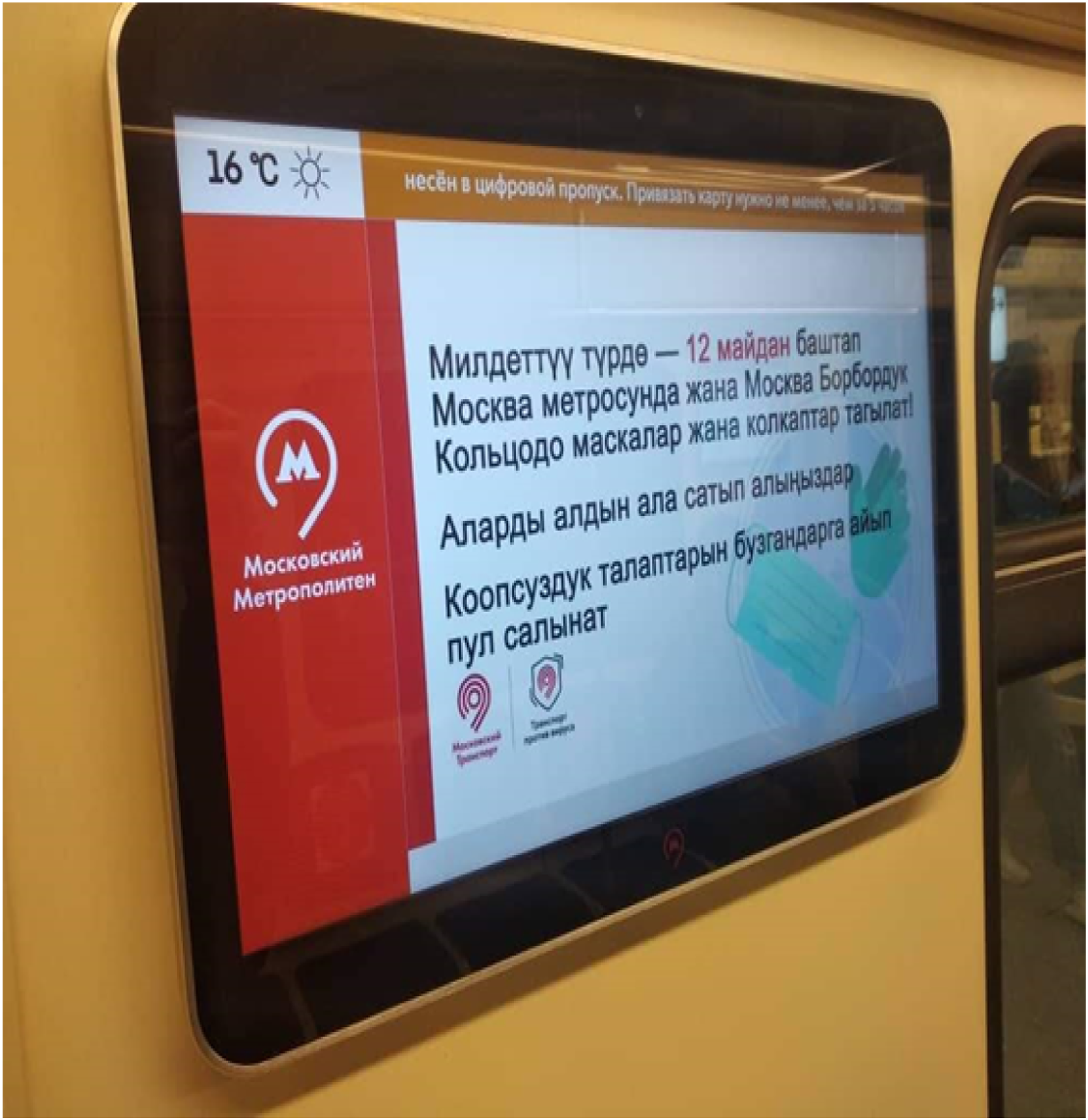
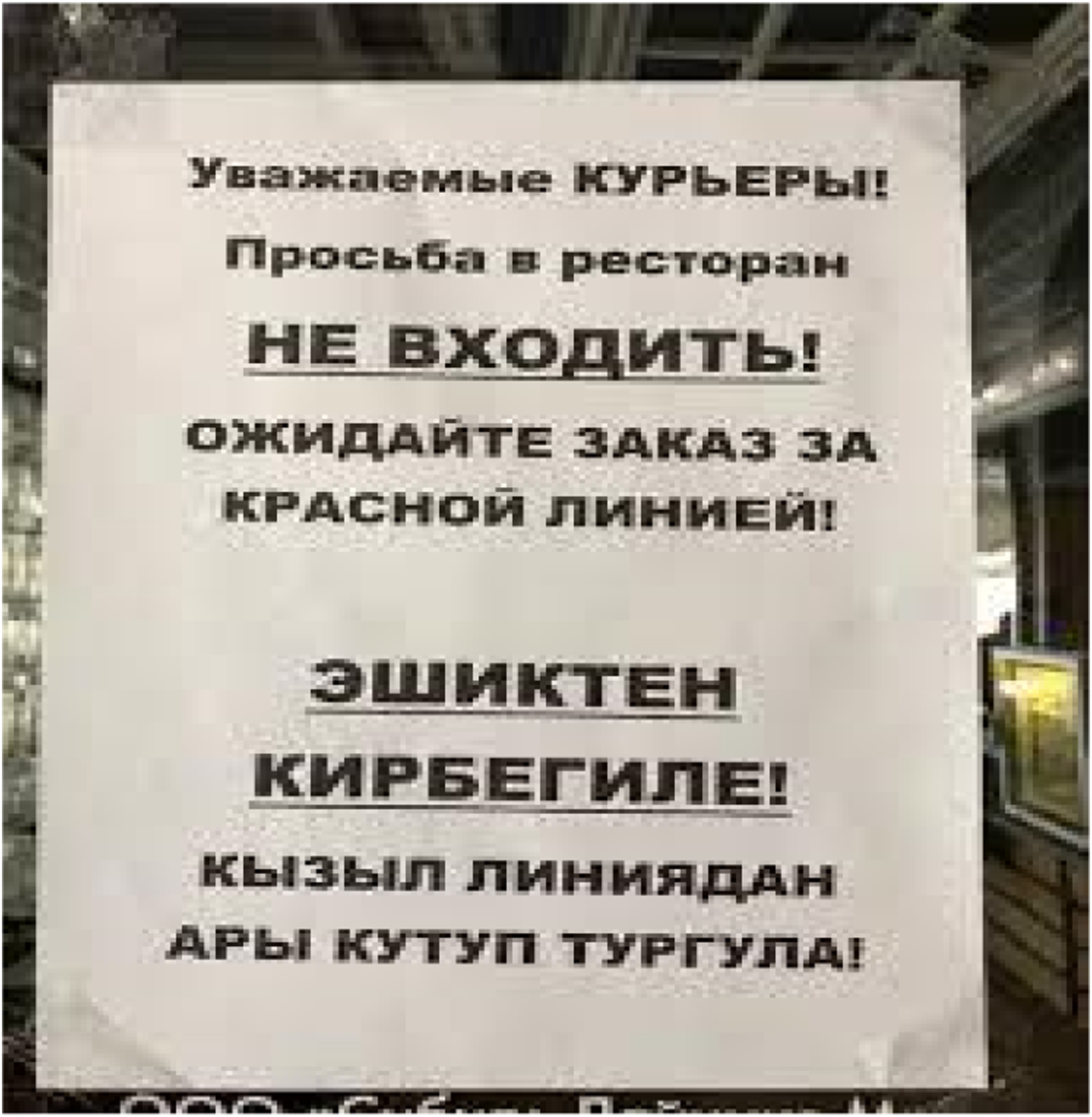
Other observations were made in Moscow and St. Petersburg, which have highly linguistically diverse populations. Photos of pandemic signs (N = 150) indicate that they are predominantly in Russian, and infographics are less common than expected. There is minimal English in tourist spaces and international workplaces, such as universities (see Pictures 2 and 3). Minority languages were not found in healthcare announcements. However, there were instances of Kyrgyz in signs related to pandemic work organization. One case involves digital screens in the Moscow subway, where the Kyrgyz part of the official announcement in Russian is displayed (see Picture 4). English and Kyrgyz signs address the penalty for passengers without masks in the Moscow metro (May 2020) (see picture 4). It should be noted that switching between languages on screens is common in some transit locations in Russian cities, such as airports, but in the metro, information was previously available only in Russian and English. Therefore, the crisis prompted an expansion of languages used for communication. Another example involves communication between catering business owners and delivery workers, with a Kyrgyz sign instructing couriers to wait behind the red line to comply with social distancing rules (see Picture 5). Russian and English. St. Petersburg, New Holland (a touristic site). Russian and English. St. Petersburg, HSE University. Kyrgyz, a digital display in the Moscow metro. A bilingual Russian and Kyrgyz announcement in Moscow for delivery staff regulating the physical distancing. “Dear couriers! Do not enter the restaurant! Wait for the order behind the red line!”.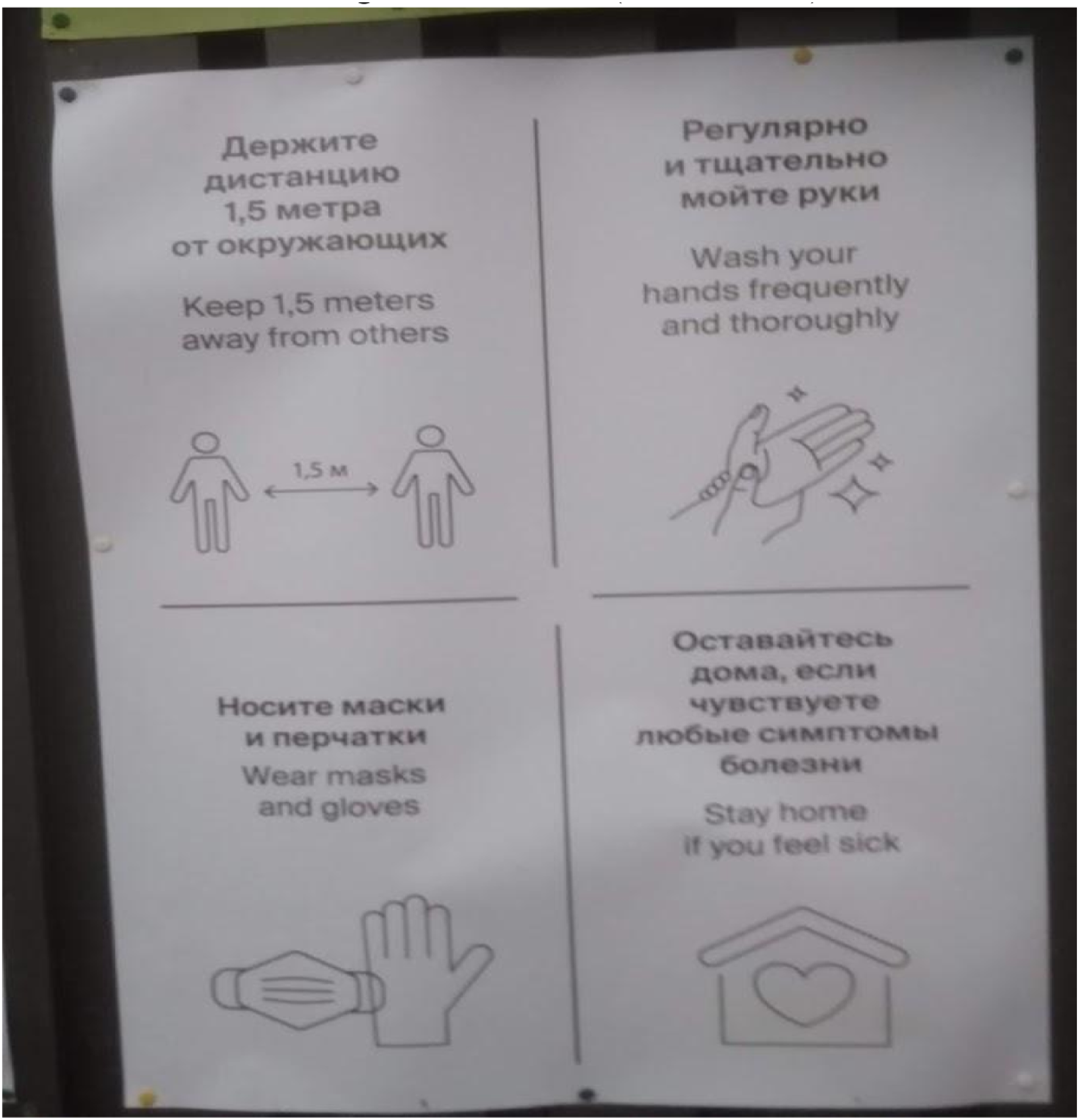
Most people in the republics of Buryatia, Yakutia, and Chuvashia, especially in the main cities, are bilingual and can understand signs in Russian. Thus, providing information about the pandemic in their native language relates to both trust in the information and the symbolic status of the language. In other cases, many working migrants in large cities have limited proficiency in Russian. Consequently, non-Russian speakers may be excluded or misinformed due to the design of visual materials. Therefore, the linguistic landscape data reveals an underrepresentation of migrant languages and initial signs of change in the monolingual regime. The case of multilingualism on screens is particularly interesting. What will be the impact of this growing digital linguistic diversity? It could be part of a transformation in language ideology or simply a temporary change during the pandemic. Importantly, all examples discussed focus on controlling migrant behavior rather than healthcare itself.
However, not everything is determined by official language policies. Individual actions by journalists, medical workers, and community leaders can be equally important as state actions. There are examples of cards and booklets on coronavirus symptoms created by volunteers (see Picture 6). Other examples include signs from Ulan-Ude, Buryatia, provided by business owners (see picture 1 above), representing individual efforts to assess language awareness and provide information about safety measures in two official regional languages. Multilingual COVID-19 safety rules in Tajik.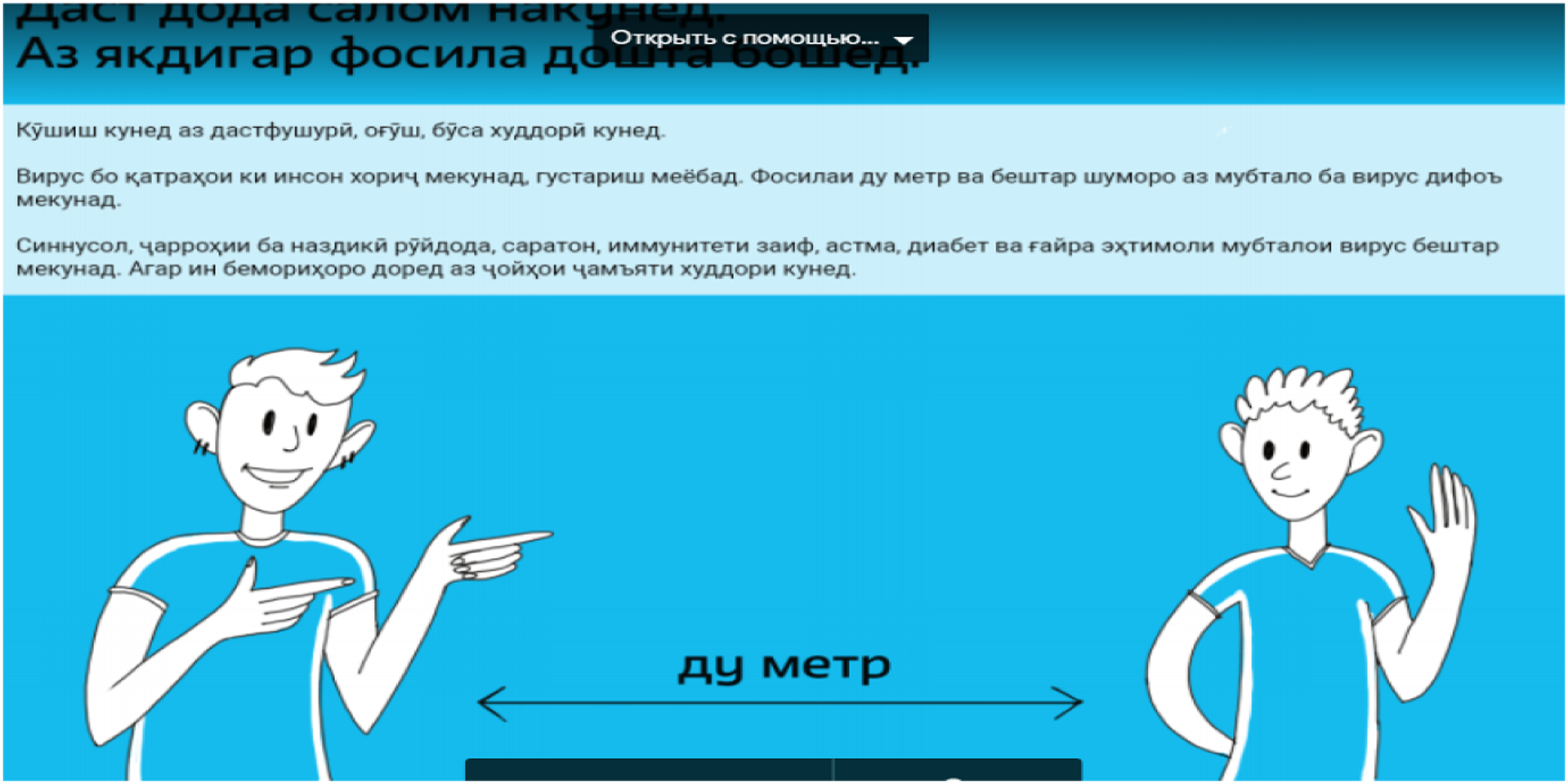
Interviews
People often do not emphasize negative experiences when seeking treatment and assistance for COVID-19 infection. During the pandemic, they tend to acknowledge the challenges in accessing medical care but focus on positive experiences. It is important to note that among my respondents, none reported serious COVID-related problems.
Respondents from the capitals of ethnic republics described healthcare communication as predominantly monolingual in Russian, even between co-ethnic doctors and patients. As one respondent explained, “All in Russian. There, you know, all doctors and nurses are young. We have young doctors, so they speak Russian” (female, 47 years old, Buryat, Ulan-Ude). In both Buryatia and Chuvashia, respondents mentioned that although Russian is the initial choice for official communication with doctors, it can be switched to the native language as a sign of familiarity and more comfortable interaction.
Even Buryat-speaking people start the dialogue in Russian. That’s why No, doctors don’t [speak Chuvash]. Just when you start… When you have had several appointments you know (a doctor) but without it – no. I was ill last year and on the first visit we spoke Russian and then a few times with the same doctor, we communicated in Chuvash (No, doctors don’t [speak Chuvash]. Just when you start… When you have had several appointments you know (a doctor) but without it – no. I was ill last year and on the first visit we spoke Russian and then a few times with the same doctor, we communicated in Chuvash (m, 60 y.o., Chuvash, Yadrinskiy district).
It is important that health communication may be in Chuvash if the patient knows the doctor. The communication between doctors and patients is considered highly hierarchical and typically requires the usage of Russian. However, with paramedics and other mid-level medical staff, it is possible to choose the native language for communication. Nurses – they are a rung below doctors, and sometimes (they) can communicate [in Buryat], for example, if a Buryat speaker and a nurse is the same ethnicity she speaks Buryat (f, 60 y.o., Buryat, Ulan-Ude). For example, one nurse there, she is from our side, from our village. She usually works in the children’s department (of the hospital) but now she is working in the ‘red zone’. We spoke Chuvash with her. But it depends on the person (f, 55 y.o., Chuvash, Yadrinskiy district).
However, it should be noted that communication in the “red zone” (where medical staff wear protective suits) is often anonymous and challenging due to the inability to recognize doctors and understand their speech (female, 48 years old, Buryat, Mogotoy).
There are differences between rural and urban settings, particularly in the capital cities of the republics. In Aginskoe, a hospital serves district citizens, and medical personnel use the Buryat language when treating patients from villages without sufficient medical equipment for COVID-19 treatment. In Maloe Karachkino village, Chuvashia, the older age group prefers to communicate in Chuvash, especially when discussing private topics like their health. A rural paramedic mentioned that senior individuals predominantly communicate with her in Chuvash or mix languages (female, 50 years old, Chuvash). This highlights the need for coronavirus information in the Chuvash language and communication with doctors and nurses in their native language when villagers visit the district center hospital. Respondents mentioned that during vaccination, doctors visited the village, and one of them was Russian-speaking while the other was a Chuvash-speaking medic, allowing patients to choose the language. To those who do not understand Russian, who are older, (she) explains in Chuvash. She knows Chuvash but speaks predominantly Russian. Usually, she speaks Russian. And the second (doctor) explains in Chuvash (m, 55 y.o., Chuvash).
In a hospital, the choice of language is not only about talking to doctors, but also to other patients. Some people described choosing their native language in difficult cases or during the pandemic. Due to the presence of Russians in a hospital ward we spoke Russian. Well, that Buryat felt extremely sick when things got to be too bad – I approached her and spoke, naturally, Buryat. (f, 48, Buryat, Mogotoy).
The important aspect of medical communication is the When the native language (is used) it makes the communication more honest, the native language. (Everyone) wants to emphasize compassion (from medical staff) (f, approx. 60, Buryat, Ulan-Ude).
Discussion and Conclusion
As mentioned in the introduction, the COVID-19 pandemic has presented various challenges regarding multilingualism and translation. This issue is of utmost importance as effective communication of health and safety procedures directly impacts lives. Despite this significance, there has been a notable absence of public discussion on multilingualism and the equality of individuals during the pandemic, creating a barrier to the dissemination of crucial information regarding safety measures and treatment.
In all observed cases, Russian was the predominant language used for official COVID-19 information. This lack of linguistic inclusivity is not unique to this situation; as previously mentioned in the introduction, similar issues were identified in other multilingual settings. Generally, this stems from a lack of language awareness among speakers of the majority language, particularly among decision-makers and officials. The diverse linguistic landscape is often underestimated by those who speak the dominant language and hold positions of authority. However, there has been a gradual shift away from the monolingual approach in recent years, and the crisis itself has served as a unifying force for the greater good, prompting transformative changes. What are the main findings regarding language ideology and practices in Russia that emerged from this study?
Firstly, the study identified individual efforts made by business owners, volunteers in NGOs, and others, as a response to the failure of state language policies in addressing the linguistic challenges faced by indigenous groups and foreigners during the pandemic. In the absence of official support for multilingualism, individuals have taken on the responsibility of creating new projects that support minority languages in Russia, as well as foreign languages. Secondly, crisis communication now encompasses not only the “official minority languages” but all languages spoken by individuals, including the “non-prestigious” languages of migrant workers. This represents an important step towards linguistic inclusion and what Rampton et al. (2018) refer to as “sociolinguistic citizenship,” building upon Stroud’s concept of “linguistic citizenship” (2015). However, it should be noted that the observed cases of signs in migrant languages primarily focus on regulating migrant behavior to protect others, and there remains a lack of official information in minority languages for the migrants themselves.
What can be done to promote linguistic equality in medical settings? On an official level, there should be a stronger emphasis on the requirement to include minority languages in communication within bilingual areas. This can be achieved by restructuring existing medical education courses and providing support to healthcare professionals with knowledge of minority languages. However, the most crucial aspect is promoting multilingualism and fostering a welcoming environment within medical facilities. Engaging and involving groups willing to participate in this process can offer fresh insights into strategies for enhancing multilingualism, as outlined in Section 2. While grassroots initiatives cannot replace official language planning in the medical sphere, they can provide additional flexible solutions and support existing efforts.
Furthermore, it is essential to have discussions on doctor-patient communication and establish more nuanced guidelines that consider the emotional state of patients. The study found that the practices of doctor-patient interaction vary depending on familiar or less familiar contexts, as well as rural or urban settings. Paramedics, who serve as “cultural brokers,” use native languages and play a crucial role, particularly with older age groups. This individualized approach reshapes language attitudes and challenges the predominance of Russian in institutionalized communication. By fostering a trusting relationship between doctors and patients through the use of their native language, medical communication can become more empathetic and ultimately contribute to the overall well-being of patients.
Footnotes
Acknowledgments
I would like to express my gratitude to Yaron Matras for his meticulous reading and insightful discussions which greatly contributed to the improvement of this article. I am also deeply appreciative of the anonymous journal reviewers for their valuable comments. Furthermore, I am thankful to the participants of the project “Discourse Practices across Professional, Cultural, and Social Groups” at HSE University, where I collected the data and initiated the work on this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The results of the project “Discourse Practices across Professional, Cultural, and Social Groups”, carried out within the framework of the Basic Research Program at the National Research University Higher School of Economics (HSE University) in 2021-2022, are presented in this work.
Notes
Author Biographies
References



