
Abstract
2022 marks the 30th anniversary of diplomatic ties between Korea and Central Asia. Since the establishment of diplomatic ties, Korea and Central Asia have expanded exchanges in various fields, including politics, economy, and diplomacy. Cooperation between Korea and Central Asia utilizing the abundant medical manpower of Central Asia and Korea’s excellent medical and pharmaceutical technology was also selected as a promising area of cooperation between the two sides. Korea and Central Asia have continued to cooperate in the field of health and medical care, but there were limits to deepening cooperation. Recently, the importance of health and medical cooperation around the world has been highlighted again due to COVID-19. This thesis examines the status and problems of health care in Central Asia, and analyzes the achievements and limitations of health care cooperation between Korea and Central Asia. The purpose of this is to suggest directions for strengthening health care cooperation between Korea and Central Asia. This will help the new government, which aims to become a global center of bio-digital health, explore strategies and policies for preemptive health care cooperation in Central Asian countries.
Introduction
The year 2022 marks the 30th anniversary of diplomatic ties between Korea and Central Asia. Since the establishment of diplomatic ties, Korea and Central Asia have expanded exchanges in various fields, including politics, economy, and diplomacy. In particular, the revision of Korean medical law in 2009 allowed attraction of overseas patients in Korea, and Korean medical institutions actively advanced into Kazakhstan, the most economically advanced country in Central Asia, and Uzbekistan, the most populous country in Central Asia. Besides medical tourism, cooperation between Korea and Central Asia through the utilization of the abundant medical human resources of Central Asia and Korea’s excellent medical and pharmaceutical technology was also noted as a promising field. However, due to the high labor cost of Korean medical staff, the low rate of use of private hospitals by locals accustomed to public medical treatment, and institutional limitations, actual health and medical cooperation was low, except for medical tourism.
However, as the COVID-19 outbreak has highlighted the importance of cooperation in the health care sector and the demand for health hygiene products, medical facilities, and basic medicines in Central Asia, there is renewed possibility of health and medical cooperation between Korea and Central Asia. Additionally, the expansion of compulsory insurance and promotion of overall health care reform in Kazakhstan and Uzbekistan may enhance health and medical cooperation between Korea and Central Asia.
However, health and medical cooperation between Korea and Central Asia is primarily being conducted for medical tourism, led by private companies. Therefore, academic research to analyze the current status and problems of health and medical cooperation between the two regions is lacking. Existing studies dealing with health care cooperation between Korea and Central Asia include a paper analyzing the status and prospects of medical tourism in Korea in Commonwealth of Independent States(CIS) such as Russia and Central Asia (Sang Hyeon Kim, 2014), a study on the satisfaction of Kazakh patients with Korean medical institutions (Heeran Jamie Cho, 2020), a study on the overseas expansion strategy of Uzbekistan using Public Private Partnership(PPP) (You & Kim, 2020), and studies on Official Development Assistance(ODA) support strategies for health care in Uzbekistan in Korea (Eun Seong Park et al., 2013). However, since these studies are focused on detailed cooperation in fields such as medical tourism and medical ODA, a comprehensive analysis is lacking with regard to the status and problems of health and medical cooperation between the two countries that have been accumulated over the past 30 years.
Therefore, this study aims to derive limiting factors of health care cooperation between Korea and Central Asian countries by examining the current status and problems of health care in Central Asian countries and analyzing the current status of health care cooperation between Korea and Central Asia. This will help the new Korean government, which aims to become a global center of bio-digital health, seek out strategies and policies for preemptive health and medical cooperation in Central Asian countries.
This paper is structured as follows: Chapter 2 examines the current state and problems of the health care system in Central Asia, as well as the health care policies of each country. Chapter 3 analyzes the status, achievements, and problems of health and medical cooperation between Korea and Central Asian countries. Chapter 4 draws a plan for health care cooperation between Korea and Central Asia based on the results of the previous analysis. Chapter 5 describes the conclusion of this paper.
Health care in Central Asia
Central Asian health care system
The Central Asian countries that composed the Federation of Soviet Socialist Republics followed the Soviet Semashko model (Borowitz, & Atun, 2006). In this model, the state provides a single integrated service, and the basic principle is to provide free high-quality medical services to all citizens through the full participation of health and medical workers to prevent diseases and promote the health of the people. Thus, the Semashko model consists of a highly centralized process of training healthcare workers, financing healthcare and providing services. Its financing is not based on centrally designated infrastructure, the number of beds in a hospital, or population health requirements, but rather on a predetermined number of people (Romach, & Rutka, 2018).
Additionally, the Semashko model was built as a multi-level system of inpatient care delivery (with rural, central rayon, urban, regional, and federal hospitals and numerous specialized care facilities), where each of the levels corresponded to the severity of the disease (Sheiman, & Shevski, 2014). This is because such a system allows the efficient input of medical resources as the frequency of occurrence and the difficulty of treatment are different for each disease.
In this model, the Soviet Union introduced a medical delivery system that classified medical institutions into primary, secondary, and tertiary to efficiently inject medical resources in view of the different incidence and difficulty of treatment for each disease.
The characteristics of each medical institution classified according to the Semashko model are as follows. Primary medical institutions were polyclinics (outpatient clinics), family medical centers, and rural clinics managed by the local area (raion). Secondary medical institutions are large-scale general hospitals managed by the state (oblast’) and specialized outpatient hospital facilities, which are in charge of specialized treatment. Tertiary medical institutions are national-level medical institutions that provide more specialized and complex treatment such as national hospitals and medical science centers.
The medical delivery systems of Kazakhstan and Uzbekistan are also based on the primary, secondary, and tertiary medical delivery systems. However, as 30 years have passed since independence from the Soviet Union, these countries follow different arrangements. The following chapter will explore the major health indicators and health policies of Kazakhstan and Uzbekistan.
Leading health indicators for Kazakhstan and Uzbekistan
Population, life expectancy, infant mortality rate, and maternal mortality rate are used as major indicators of a country’s socio-economic and health and welfare levels because they affect national health. Knowing the level of health in a country allows you to determine the target and scope of medical cooperation. Therefore, this chapter will examine the health indicators of Kazakhstan and Uzbekistan, Korea’s major Central Asian health and medical cooperation partners, as follows.
Leading Health Indicators for Kazakhstan and Uzbekistan.
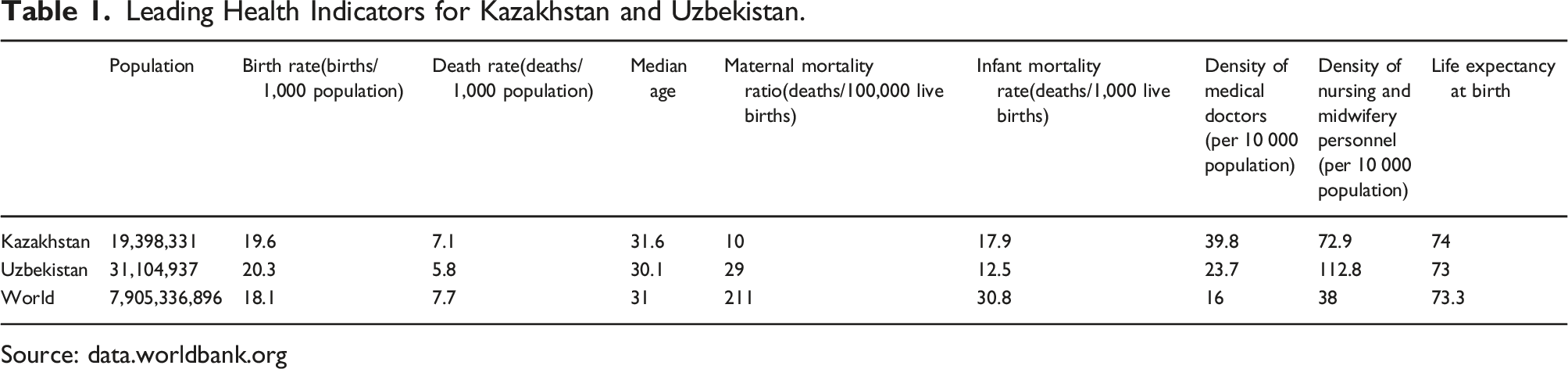
Source: data.worldbank.org
The reason the two countries show lower than the world average in maternal and infant mortality rates is because the medical systems being followed are based on the Soviet Semashko model, which aims for universal welfare, as discussed earlier. In fact, Kazakhstan and Uzbekistan had 39.8 and 23.7 doctors per 10,000 population, respectively, higher than the world average of 16, and the number of nurses was 72.9 and 112.8 per 10,000 population, respectively, far higher than the world average of 38. However, the average life expectancy in Kazakhstan and Uzbekistan was 74 and 73 years, respectively, which was similar to the world average (73.3 years).
Limitations of Kazakhstan and Uzbekistan’s medical system
Despite Kazakhstan and Uzbekistan showing much higher levels than the world average in maternal mortality, infant mortality, and the number of medical personnel, the reason why life expectancy is similar to the world average is because of the following reasons.
Top 10 causes of total number of deaths in Kazakhstan and Uzbekistan(2019).
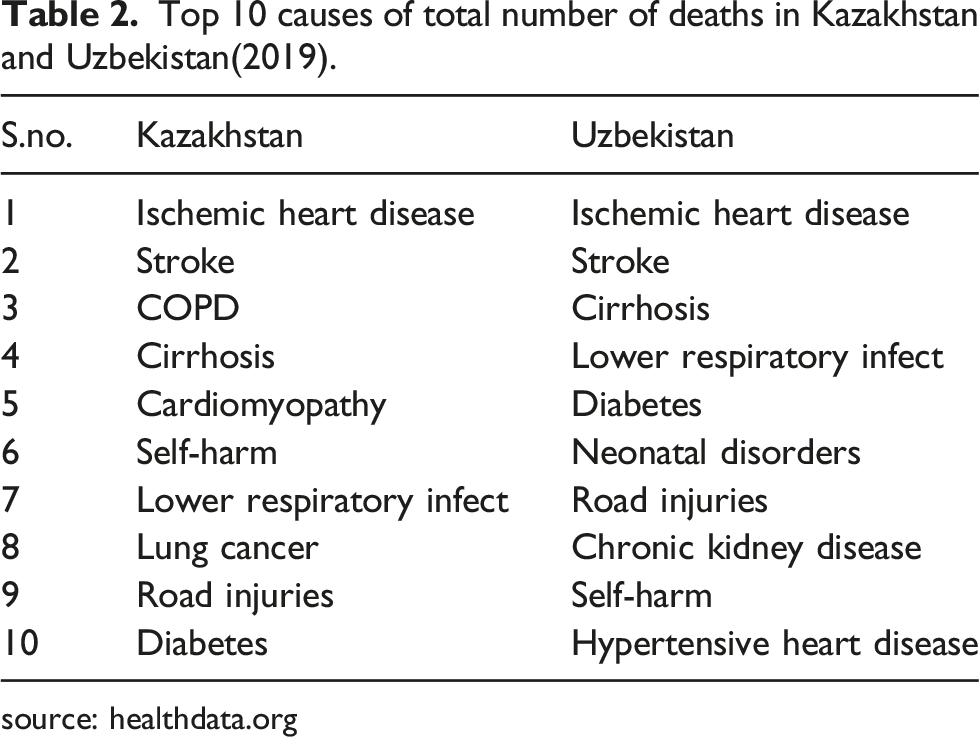
source: healthdata.org
Managing chronic diseases is expensive. The cost of managing diabetes, a typical chronic disease, for a single patient is $742.2 per year in Kazakhstan and $352 in Uzbekistan (IDF, 2019). However, current health expenditures in Kazakhstan and Uzbekistan were $742.2 and $352, respectively (Micah et al., 2019). Current health expenditures in both countries barely cover diabetes-related diseases. In other words, the current health expenditure in both countries is insufficient to treat chronic diseases such as high blood pressure and dyslipidemia as well as cancer, stroke, and liver cirrhosis as well as diabetes. As such, the current health expenditures of both countries are not sufficient to adequately support medical services that can guarantee proper health care for the people.
Second, there is a disparity in medical access between urban and rural areas. In Kazakhstan and Uzbekistan, the proportion of urban residents to the total population is 58% and 50%, respectively (World Bank, 2020). In other words, about half of the population in these countries lives in rural areas. The outdated Soviet era railway systems of Kazakhstan and Uzbekistan are not designed to meet the demands of modern Kazakhstan and Uzbekistan, which reduces accessibility in rural areas. In particular, the fact that Kazakhstan is the ninth largest country in the world in terms of land area, coupled with its low population density of 7 people/㎢ is also a factor hindering access to medical care in rural areas (UN, 2020). In fact, according to WHO’s Integrated People-Centered Health Services (IPCHHS) data, the number of doctors per 100,000 people in Kostanay, in northern Kazakhstan, was 266 in 2016, more than 100 fewer than the average number of doctors per 100,000 people in Kazakhstan (IPCHS, 2016).
Third, outdated medical equipment and medical infrastructure. The modernization of medical equipment used for diagnosis and treatment of diseases is one of the major factors affecting public health. However, medical equipment and medical infrastructure in Central Asia, earlier financed by the government, began to deteriorate rapidly as financial support and investment decreased as the Soviet Union collapsed and caused economic difficulties. In Kazakhstan, only 72.5% of all medical institutions have medical equipment, and the aging rate of medical equipment is 37% (Government of Kazakhstan, 2021). This low retention rate of medical equipment and obsolescence of medical equipment makes it difficult to provide appropriate diagnosis and treatment to patients, leading to a decline in the quality of medical care.
Finally, the low salaries of medical personnel. Wages are a major factor in attracting and retaining high-quality labor in a capitalist society. In 2018, medical practitioners in OECD member countries were paid two to four times the average monthly salary of all workers, and specialists were paid two to six times the average monthly salary of all workers (Health at a Glance 2019: OECD Indicators, 2019). On the other hand, doctors’ salaries in Kazakhstan were lower than the average salary of office workers. In fact, the average monthly salary of a doctor in Kazakhstan in 2018 was 142,200 Tenge, while the average salary of an office worker was 161,400 Tenge(Center for Health Economics Republican Center for Health Development, 2018). In the case of Uzbekistan, as in Kazakhstan, doctors are one of the lowest-paid occupations along with teachers. In 2021, the average monthly salary of an office worker in Uzbekistan was 1.98 million Som, while medical workers received 1.8 million Som (REGNUM, 2021). As such, the underdeveloped medical infrastructure and the treatment of medical staff have led to deterioration in the quality of medical services in both countries.
Health policy of Kazakhstan and Uzbekistan
Kazakhstan and Uzbekistan are promoting health care policies to provide high-quality medical services to the people and to promote public health. Currently, the Kazakhstan government is promoting the State program of development of health care of the Republic of Kazakhstan for 2020–2025. This program aims at ensuring the availability of high-quality health care, and the Program’s target indicators in 2025 are: growth of remaining life expectancy of citizens up to 75 years; decrease in risk level of premature death rate from 30 to 70 years from cardiovascular, oncological, chronic respiratory diseases, and diabetes to 15,43%; decrease in maternal death rate to 14,5 per 100 thousand live-birth (according to confidential audit); decrease in infantile death rate to 8,3 per 1000 live-birth (according to confidential audit) (State Health Development Program of the Republic of Kazakhstan for 2020–2025). This policy aims to bridge the gap between rural and urban medical access and to improve the quality of medical care through modernization of the health system. In addition, primary health care is being expanded for effective prevention and management of chronic diseases. In addition, as Kazakhstan has implemented Mandatory Social Health Insurance (MSHI) from January 1, 2020, medical insurance subscribers can easily use various facilities such as preventive health checkups, CT, MRI, and rehabilitation.
In particular, the Kazakh government is actively seeking to improve the salaries of medical personnel to prevent the outflow of excellent medical personnel abroad. This is because in Kazakhstan, doctors’ average salary in 2018 was 0.88 times the average salary of all workers, while doctors in OECD countries received more than twice the average salary. To this end, the Kazakh government has increased the wages of medical workers by an average of 20–30% from January 2022, and their wages are expected to double by 2023 (Kapital, 2021). At the same time, the Kazakh government announced measures to improve the treatment of medical personnel, such as lowering the patient burden per doctor to the level of the OECD (one doctor per 1,500 population)(AKIpress, 2019).
Due to the COVID-19 outbreak, the Kazakh government is actively promoting the introduction of mobile medical complexes and telemedicine that can be used in remote locations. The Kazakh government has supplied an additional 100 mobile medical complexes to enable rural populations to actively use medical services from 2021 (Baigenews, 2020). In 2021, 149 mobile medical complexes served approximately 1.8 million residents in 2,542 remote rural areas, screening approximately 132,000 patients (Primeminister, 2022). Telemedicine services are also being actively adopted, with approximately 6.4 million people provided with telemedicine counseling, of which more than 1.3 million have been provided to the rural population (Primeminister, 2022).
Uzbekistan’s health care reform has been promoted in earnest since Shavkat Mirziyoyev took office as president. President Mirziyoyev, who was elected president of Uzbekistan in 2016 after the sudden death of President Karimov, announced the Uzbekistan Development Strategy 2017–2021 with the main goal of improving the medical system in February 2017 (Tashkenttimes, 2018). Uzbekistan is currently preparing the National Health (Sector) Strategy (NHS) 2030, which contains a health care strategy up to 2030, being drafted with the participation of high-ranking officials from the World Bank and Korea’s KHIDI (Yuz, 2022).
In addition, the Uzbekistan government promulgated the “Comprehensive Measures for Fundamental Improvement of Uzbekistan Medical System” Act in 2018 to promote health care, and is promoting reforms in the health care sector such as primary care, emergency care, and medical support for the vulnerable. At the same time, President Mirziyoev is promoting reform policies from various angles to realize Universal Health Coverage (UHC), which enables all citizens to access high-quality medical services without financial burden from 2019 to 2025 (Reliefweb, 2021).
The Uzbekistan government has also announced the Concept of the Development of the Healthcare System of the Republic of Uzbekistan for 2019–2025 in 2018 to increase access in rural areas and provide efficient medical services (presidential decree of the republic of Uzbekistan, December 7, 2018 No. UP-5590). In addition, the Uzbekistan government is promoting the introduction of “smart medicine” to establish an integrated medical information center and a Unified Telemedicine Network (UTS)(Kun, 2018). Furthermore, the National Chamber of Innovative Healthcare of Uzbekistan and the Republican Specialized Scientific and Practical Medical Center for Cardiology launched a joint project in 2021 to provide telemedicine services. The project aims to provide medical services using telemetry equipment in different regions of the country, starting in the Tashkent region, in the cities of Karshi, Jizzakh, and in the Chilanzar region of the capital (UzDaily, 2021).
Achievements and limitations of Korea–Central Asia health and medical cooperation
Achievements of Korea–Central Asia health and medical cooperation
Although Korea’s health care industry possesses world-class medical technology and services, the government’s various regulations emphasizing the public nature of the health care sector have limited its pursuit of profit. In response to this, an amendment to the Medical Law was passed in 2009, allowing the attraction of foreign patients while the medical community continued to demand autonomy. Consequently, Korean medical institutions have started to actively promote the attraction of medical tourists, such as planning international medical projects and seeking to advance into the local market.
In this context, health and medical cooperation between Korea and Central Asia began to be centered on Kazakhstan and Uzbekistan, which have high demand for medical tourism. The advancement of Korean medical institutions into Central Asia began in 1996 when Keimyung University opened the Almaty Dongsan Clinic in Almaty, Kazakhstan for overseas medical missionary work. Private medical institutions’ entry into Kazakhstan began with the groundbreaking ceremony of the “Sejong Eurasia Clinic” in 2012. As a heart hospital, Sejong Hospital entered Kazakhstan by receiving capital investment without burden of cost with the brand reputation and technology of Sejong Hospital. With this as a starting point, Korean medical institutions are entering the local market through joint ventures or independent investments, or are cooperating with Kazakhstan in various ways in the medical field, such as medical consultation, medical education, sharing medical business, and medical service. Medical institutions that have entered Kazakhstan offer various medical fields such as cancer, dentistry, oriental medicine, spine, and heart, and the types of entry are diverse, such as solo entry, joint venture, technology transfer, and telemedicine.
Cooperation between the Korean and Kazakh governments was also carried out in the wake of President Moon Jae In’s visit to Kazakhstan in 2019. In April 2019, the two countries signed the Korea–Kazakhstan health and medical cooperation implementation plan and MOU, as well as the public and private sector health and medical cooperation MOU (KDI, 2019). At the first Korea–Kazakh Health and Medical Working Group Meeting held in November 2019, the two countries held a meeting of experts in the fields of medical devices, pharmaceuticals, e-Health, and medical services (KHIDI, 2019). The two countries also emphasized the importance of health cooperation for a joint response to COVID-19 at the 9th Korea–Kazakhstan Joint Economic Committee held via video conference in November 2020.
Due to the active marketing of medical tourism by Korean medical institutions and the Korean Wave in Central Asia, many patients from Kazakhstan and Uzbekistan visited Korea, and the bilateral health and medical cooperation in the field of medical tourism showed clear results. Looking at the growth rate of foreign patients in Korea for 10 years from 2009, when foreign patients were allowed to be attracted, the growth rates of Kazakhstan and Uzbekistan patients were 59% and 44%, respectively. This is higher than the average annual increase in attraction (23%) of all foreign patients during the same period (KHIDI, 2018).
In particular, health and medical cooperation between Korea and Kazakhstan has shown remarkable results in the field of medical tourism. Of the 5,067 Central Asian patients who came to Korea for medical tourism in 2020, 61% were from Kazakhstan (KHIDI, 2020), and the number of people treated in Korea as a percentage of the national population was the highest in Kazakhstan, with 36 patients per 10,000 people (Kmdianews, 2019).
Whereas health care cooperation between Korea and Kazakhstan was led by the private sector, health care cooperation between Uzbekistan and Korea is being done at the government level. Health and medical cooperation between Korea and Uzbekistan has been developing since the signing of the “Letter of Intent on Health and Medical Cooperation between Korea and Uzbekistan” in August 2011. In particular, with the Health and Medical Cooperation Agreement signed in 2015, medical personnel who have obtained a Korean medical license can engage in medical activities without a separate license recognition process (KDI, 2015).
Through ODA and EDCF, the Korean government provides comprehensive consulting and financial aid for Uzbekistan’s legal and institutional reform, hospital operation, and medical staff education, and is cooperating with Uzbekistan’s medical system advancement projects. Among them, the biggest achievement was the establishment of Bukhara Himchan Hospital on a general hospital-level scale and cooperation with high-level health policy experts.
Himchan Hospital in Bukhara was established in 2019 with active financial and tax support from the Korean and Uzbekistan governments. The Ministry of Health and Welfare of Korea and the Korea Health Industry Development Institute provided 360 million won for establishing Bukhara Himchan Hospital through the “Medical Overseas Project Support Project.” The Uzbekistan government helped to open Bukhara Himchan Hospital by simplifying various licensing procedures, reducing taxes, and transferring ownership of the 23,140 ㎡ site for free (Korea, 2019).
Health care cooperation between Korea and Uzbekistan through health professional officials is also one of the great achievements of Korea–Uzbekistan health care cooperation. In March 2019, at the request of Uzbekistan, who wished to introduce a Korean-style medical model, Lee Dong-wook, former head of population policy at the Ministry of Health and Welfare, a Korean health professional, was appointed as an advisor to the Deputy Prime Minister for Social Development and Deputy Minister of Health of Uzbekistan. In March 2020, as the Uzbekistan government urgently requested dispatch of experts to Korea due to the rapid increase in the number of confirmed COVID-19 cases, Korea University Professor Jae-wook Choi was dispatched as a special policy advisor.
Limitations of Korea-central Asia health and medical cooperation
Health and medical cooperation between Korea and Central Asia over the past 30 years has not yielded clear results for three main reasons. First, there are restrictions on the medical treatment of Korean medical staff due to institutional factors. Korean medical institutions advanced mainly from Kazakhstan, the most economically advanced country in Central Asia. However, it was Uzbekistan, not Kazakhstan, that actually succeeded in hospital-level overseas expansion. The biggest factor that made this difference was the resolution of institutional constraints. In the case of Kazakhstan, for local medical activities of Korean medical staff, they must undergo medical license certification process according to the Kazakhstan Licensing Act. In the case of Uzbekistan, the health and medical cooperation agreement between Korea and Uzbekistan signed in 2015 enabled Korean doctors to engage in medical activities without a separate license recognition procedure, enabling more active medical cooperation. In other words, the resolution of institutional constraints is essential for strengthening health and medical cooperation.
Second, the use of private medical institutions by the locals who are accustomed to free medical care is low. The Central Asian countries that were federations of the Soviet Socialist Republics have been operating free medical care for all citizens since the Soviet era. After the dissolution of the Soviet Union, many private medical institutions were established in Central Asian countries, but people accustomed to free medical care still prefer public hospitals. In addition, private medical institutions are relatively expensive compared to public hospitals, making it difficult for people in Central Asia with low income levels to use them. In other words, due to the low purchasing power of medical services of the people of Central Asia and the low rate of use of private medical institutions, profitability is not a guarantee for local medical institutions.
Third, it is difficult to hire Korean medical personnel. According to Salaryexplorer, a global payroll information site, the average monthly salary of Korean medical staff in 2022 is about 9.14 million won. This is more than three times the average monthly salary of doctors in Kazakhstan of 910,000 KZT (about 2.64 million won) in 2022, and more than 26 times the average monthly salary of doctors in Uzbekistan of 3,100,000 UZS (about 350,000 won) as of the same year. Therefore, Korean medical institutions that have entered Central Asia not only find it difficult to find Korean doctors who wish to stay in the country, but also have the burden of supporting the high salaries and expenses of Korean doctors.
On the 30th anniversary of the establishment of diplomatic ties between Korea and Central Asia, what can be done to preserve the achievements of Korea and Central Asia in health and medical cooperation over the past 30 years, overcome limitations, and strengthen bilateral health and medical cooperation? In the next chapter, we will discuss ways to cooperate in health care between Korea and Central Asia.
Korea-Central Asia health and medical cooperation plan
The purpose of health care cooperation between Korea and Central Asia has been highlighted as a field with great growth potential because it has complementary characteristics in terms of supply and demand for medical services. Nevertheless, due to institutional limitations, the low rate of use of private hospitals by local people, and the difficulty in hiring Korean medical staff, Korea and Central Asia were unable to achieve positive results despite the growth potential.
However, due to changes in the internal and external environment such as non-face-to-face interactions due to COVID-19 and the expansion of compulsory insurance in Kazakhstan and Uzbekistan, Korea-Central Asia health care cooperation is entering a new era. In particular, for Korea, where a new government has been formed, this environmental change may present an opportunity to expand health and medical cooperation. Therefore, based on the experience of health and medical cooperation between Korea and Central Asia over the past 30 years, we propose the following four measures to strengthen bilateral health and medical cooperation after the COVID-19 outbreak.
First, intergovernmental cooperation for deregulation is necessary. Korean medical institutions have entered Kazakhstan, the highest-income country in Central Asia, to attract medical tourists. As a result, the number of patients visiting Korea from Kazakhstan showed a high rate of increase, resulting in tangible results. However, as health and medical cooperation between Korea and Kazakhstan was conducted at the private level rather than intergovernmental cooperation, institutional cooperation such as accreditation of Korean medical practitioner licenses and simplification of the licensing system was not expanded. Consequently, unlike Uzbekistan, Korean hospital-level medical institutions with more than 100 beds did not enter Kazakhstan.
On the other hand, Uzbekistan, which recognizes Korean medical licenses, opened more than 100 general hospital-level facilities for the first time overseas with financial support and tax benefits from the two governments. Furthermore, Korean health care experts were dispatched to support Uzbekistan’s health care system reform and policy development. In addition, due to the advantage that medical treatment can be performed without a local medical license, Korea is entering Uzbekistan through telemedicine in earnest. Therefore, with reference to the case of Uzbekistan, deregulation is the priming water for cooperation, similarly, intergovernmental cooperation should be closely discussed to expand health and medical cooperation between Korea and Kazakhstan.
Second, cooperation in the medical information system. Kazakhstan and Uzbekistan are building a digital integrated medical system to establish an efficient medical system. Korea has been using the electronic medical record system for more than 20 years, stipulating the contents of electronic medical records in the Medical Service Act in 2002. According to the Ministry of Health and Welfare’s “2020 Survey on Health and Medical Informatization,” most hospitals have introduced electronic medical record systems at the upper level at 100%, 97.5% at general hospitals with less than 300 beds, 94% at the general hospital level, and 90.5% at the hospital level (Korea Health Information Service, 2020). Korea also has the world’s best network infrastructure and IT technology, and has introduced various electronic medical record systems and systematic certification systems. Therefore, Korea will be able to transfer its know-how by exporting the “medical information system” at the government level, just as it exported the “electronic government” in the past using these operating experiences and know-how.
Third, the export of the health insurance system. Recently, compulsory medical insurance systems were introduced in Kazakhstan and Uzbekistan. It has the advantage that it increases access to medical services by reducing the burden of medical service costs. The increasing demand for medical care due to these advantages also helps improve the quality of medical care. However, the operation of the health insurance system is complicated, such as reorganizing the insurance premium collection system, determining medical fees, and equity in adjusting health insurance finances.
In 1977, medical insurance system was introduced in Korea and insurance coverage was expanded to the entire nation in 1989. Korea, which has more than 30 years of experience in operating the medical insurance system, will be able to strengthen cooperation with the governments of Kazakhstan and Uzbekistan, which recently introduced medical insurance, in areas related to health insurance policies and screening manuals.
Finally, entering the medical platform business. In Central Asia, much of daily life is shifting from offline to online, with e-commerce exploding as mobile use expands to all generations due to COVID-19. In addition, as Central Asian countries such as Kazakhstan and Uzbekistan have introduced health insurance systems, local people’s medical options are expanded from public hospitals to private hospitals, a medical platform business model that reflects local people’s demand for medical services is expected to be promising. Through this medical platform, besides the inclusion of services such as price comparison, reservation, and review of local medical institutions, medical tourism in Korea can also be linked. In addition, if a platform is built in Russian language, the service can be expanded to Russian-speaking regions such as Russia and Central Asian countries.
Conclusion
Kazakhstan and Uzbekistan, which became independent from the Soviet Union, used to follow the Soviet Semashko model, which provides free, high-quality medical services to all citizens through the full participation of health care workers. The basic principle of this model is to provide free high-quality medical services to all citizens through the full participation of health and medical workers to prevent diseases and promote health of the people. As a result, the maternal and infant mortality rates in Kazakhstan and Uzbekistan are lower than the world average, and the number of doctors and nurses per 10,000 population is also much higher than the world average. However, despite the fact that these countries show much higher than the world average in terms of maternal mortality rate, infant mortality rate, and the number of medical personnel, the average life expectancy is similar to or lower than the global average.
There are three major problems facing these countries with regard to health care. First, there are insufficient financial resources to guarantee public health. The major causes of death in Kazakhstan and Uzbekistan are heart disease, stroke, and liver cirrhosis, which are closely related to diabetes, hypertension, dyslipidemia, and metabolic syndrome. Since these are chronic diseases, continuous management is required, but the current medical expenses in Kazakhstan and Uzbekistan are not sufficient to adequately cover diabetes-related diseases.
Second, there is a disparity in medical access between urban and rural areas. About half of the population of Kazakhstan and Uzbekistan live in rural areas. Medical access in rural areas is lower than in urban areas due to underdeveloped transportation infrastructure and low population density.
Third, old medical equipment and medical infrastructure. Public health services in Kazakhstan and Uzbekistan are still based on Soviet era facilities, with low medical equipment ownership and high rates of obsolescence, even if they do have them.
Lastly, the low salaries of medical personnel. The average salary of doctors in Kazakhstan is lower than the average salary of office workers, and in Uzbekistan, doctors are one of the lowest-paid occupations along with teachers. In a capitalist society, wages are a major factor that attracts and retains high-quality labor, and low wages for medical personnel act as a factor that deteriorates the quality of medical care and services.
Health and medical cooperation between Korea and Central Asia began in earnest in 2009 when Korea passed the Medical Act allowing the attraction of foreign patients. Korea’s major health and medical cooperation target countries were concentrated in Kazakhstan, the largest economy in Central Asia, and Uzbekistan, the most populous country in Central Asia. In particular, many private medical institutions have entered Kazakhstan, the most economically advanced country in Central Asia. As a result, many Kazakhstan medical tourists came to Korea, accounting for more than 60% of patients who came to Korea for medical tourism from Central Asia.
On the other hand, health and medical cooperation between Korea and Uzbekistan is being done at the government level. In particular, as the health and medical cooperation agreement signed in 2015 made it possible for medical personnel with Korean medical licenses to perform medical treatment in Uzbekistan, health and medical cooperation between the two countries began to deepen. The Korean government also supported the health care sector in Uzbekistan through ODA and EDCF, and the Uzbekistan government supported the advancement of Korean medical institutions into the local market through tax benefits and free transfer of ownership of the site. As a result, in 2019, Bukhara Himchan Hospital, a general hospital-level hospital with more than 100 beds, was opened in Uzbekistan for the first time as a Korean medical institution advancing overseas. In addition, high-level exchanges of medical experts between the two countries are also active, with Korean health and medical experts working as the Vice Minister of Health and Special Policy Advisors in Uzbekistan, and Korean health expert participating in the drafting of Uzbekistan’s National Health (Sector) Strategy (NHS) 2030.
However, health and medical cooperation between Korea, Kazakhstan, and Uzbekistan over the past 30 years has not yielded significant results for three main reasons. First, there are institutional limitations. As mentioned above, Korean medical institutions have invested heavily in Kazakhstan, which has the highest economic power among Central Asian countries. However, Kazakhstan did not recognize Korean medical licenses, and did not achieve great results compared to expectations due to institutional limitations such as complicated procedures and long time to register Korean drugs and medical devices. As in the case of Uzbekistan, if the two governments cooperate to resolve institutional constraints, health care cooperation between Korea and Kazakhstan will be further strengthened. Second, the low rate of use of private medical institutions by local people who are accustomed to free medical care. The people in Central Asian countries that became independent from the Soviet Union have been using free medical care since the Soviet era. In addition, local people’s low purchasing power for medical services acts as a factor hindering the profitability of Korean medical institutions that have entered the local market. At the same time, the difficulty of hiring Korean medical personnel who wish to stay in the country and the high salary of Korean doctors are factors that increase the current costs of Korean medical institutions entering the local market.
Then, as Korea and Central Asia celebrate the 30th anniversary of diplomatic ties, what are the plans for expanding health and medical cooperation between Korea and Central Asia? In this paper, considering the internal and external environment changes after COVID-19 and the achievements and limitations of the past Korea-Central Asian health care cooperation, the following three methods are proposed.
First, intergovernmental cooperation for deregulation in the health and medical field is necessary. In particular, in Central Asia, as non-face-to-face communication has become commonplace due to the COVID-19 outbreak and various pilot projects have been introduced to make telemedicine a reality, intergovernmental cooperation is necessary not only for local medical care but also for various regulations related to telemedicine.
Second, cooperation in medical information systems. Recently, Kazakhstan and Uzbekistan are building an integrated medical system that digitizes medical records to establish an efficient medical system. Korea, which has the world’s best network infrastructure and IT technology, has been using the electronic medical record system since 2002, so it has various certification systems and has abundant experience in operating the electronic medical record system. Therefore, export or cooperation of medical information systems can also be a promising field for Korea–Central Asia health and medical cooperation.
Third, the export of health insurance systems. The health insurance system is characterized by complex and difficult management, such as the insurance premium collection system and the determination of medical fees. Korea introduced the health insurance system in 1977 and has abundant know-how. Since Kazakhstan and Uzbekistan have recently introduced compulsory health insurance, cooperation in health insurance policies related to insurance operation such as health insurance policies and manuals for review claims can be strengthened.
Finally, as a promising cooperation method in the private sector, there is advancement into the medical platform business. E-commerce has exploded as mobile use has expanded to all generations in Central Asia due to COVID-19. At the same time, the introduction of the compulsory health insurance system is expected to increase the demand for high-quality medical care. Therefore, reflecting such changes in the internal environment, a medical platform business model that not only provides services such as price comparison, reservation, and review between medical institutions, but also connects medical tourism to Korea is very promising.
Footnotes
Acknowledgements
This paper expands on the knowledge presented in the KIEP research paper 21–33, 30th Anniversary of Diplomatic Relations between Korea and Central Asia: The Evaluation of Economic Cooperation and Four Major Cooperation Tasks.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.