
Abstract
When an institution is not easily accessible—for example, it is geographically far—it can be hard for institutional trust to develop. The institution is not only unavailable, but it can also be seen as inappropriate, non-affordable, unapproachable, and unacceptable. In this paper, we examine whether reducing distance to medical facilities and professionals can improve trust in the maternal healthcare system. We do so by focusing on developments in Georgia. Since 2013, the government has aggressively closed the distance to service access not by building more facilities or hiring more staff per se, but by upgrading and funding existing facilities and professionals in a national network to better coordinate service provisions at the local levels. Employing an original survey, we match GPS coordinates to measure distance and use regression analysis to demonstrate how ensuring every woman has access to maternal healthcare at the right place at the right time has improved institutional trust in the system. The implications highlight results that are generalizable beyond both the country and maternal healthcare.
Introduction
Trust in an institution is often low when the institution itself is not easily accessible. This is problematic if the institution is designed to serve the population. It is even more alarming when the consequences of low trust result in death. We see this concern manifesting with maternal healthcare systems. When pregnant mothers do not see the healthcare system as being accessible, they are less likely to engage with the facilities and professionals. In the absence of this engagement, trust in the institution cannot build. On the long term, this is problematic as the absence of trust can have detrimental health consequences (Falleti et al., 2020; Zarychta, 2015)—most notably maternal mortality (Shengelia, 2020).
Access is critical for citizens to trust public institutions. Barriers to access can take multiple forms, including financial burdens, lack of information, inadequate services, and even cultural differences. In this paper, we focus on what is arguably the most important barrier: availability of services. We explore whether making healthcare facilities and personnel more proximate—that is, making the system more available (see Miteniece et al., 2018)—can improve institutional trust. Specifically, we ask: Does reducing distance improve institutional trust, specifically, in the maternal healthcare system?
Maternal healthcare provides a unique opportunity to assess the effect of accessibility on trust through different types of repeated interactions between mothers and medical institutions. Pregnant mothers engage with the maternal healthcare system in a general way over a relatively long term (from 10 months of pregnancy through the 52-week postpartum period) and through a specific and short-term event (i.e., the childbirth itself). Mothers also need physical access to facilities and personnel to get ongoing care. All this means the geographic distribution of clinics and hospitals is critical for access to maternal healthcare.
We argue that geographic proximity to medical facilities and professionals improves trust in the maternal healthcare system. For the best medical care, a mother’s interactions with the system should be repeated and regular. Ease of access is crucial for these repeated and regular interactions to take place. When facilities are accessible, mothers will spend less time, money, and mental energy on each visit; and therefore, they are less likely to skimp on the requisite prenatal visits. Mothers who regularly see medical professionals are more likely to perceive adequacy in facilities and care. Through repeated interactions, mothers are more likely to be kept informed and develop rapport with the professionals and are better positioned to share cultural traditions and communicate personal values. The improved performance and accessibility of public services boost trust in the medical institutions. Conversely, when a pregnant mother must cover great distances to access the medical facilities and professionals, they are more likely to see the institution as inappropriate, unaffordable, unapproachable, and/or unacceptable—any of which hampers trust.
To test our argument, we focus on the Republic of Georgia. The provision and quality of maternal care in Georgia has fluctuated dramatically since independence (1991)—and even more so if we look back to the Soviet era. Under communism, the medical system was government-operated and publicly financed. With the Soviet collapse, there were efforts first to socialize and then to privatize the healthcare sector—a pattern we see in other sectors in the post-Soviet republics (see Sokhey, 2017). Both sets of reforms proved problematic for a mother’s ability to access the facilities and professionals, trusting the maternal healthcare system, and maternal death rates from childbirth related complications. Since 2013, there have been a new set of reforms to building a better network to increase geographic and financial access—not just to primary healthcare but also urgent hospitals and outpatient services for pregnant mothers. The drastic reduction in maternal mortality rates from a high of 43 (per 100,000 live births) in 2009 to 25 in2017 1 —coupled with a substantive increase in satisfaction with the maternal healthcare system (more below)—is testament to the country’s success. While there are multiple explanations for this drop—for example, the implementation of universal healthcare and the epidemiological surveillance of maternal mortality—one important factor has been the closing of geographical gap through the upgrading and coordination of existing facilities and professionals in a national network.
To examine the effects of distance on institutional trust, we employ a nationally representative survey where we oversampled on women. In all, we had over 700 women in the survey. We asked them about each pregnancy that resulted in the birth of a child (N=1208). We asked questions about their experiences with the medical facilities and personnel—from pregnancy to the post-partum period—for each pregnancy. We also asked them where each child was birthed. This allowed us to match GPS coordinates and employ regression analyses.
Why spatial proximity matters for institutional trust
When an institution is seen as inaccessible, trust in that institution is low. There are multiple barriers to accessibility (Miteniece et al., 2018; also see Selway, 2011, 2015; Zarychta et al., 2019). They include facility and professional inadequacies (appropriateness), prohibitive costs (affordability), a lack of awareness and information (approachability), tensions due to cultural and personal differences (acceptability), and—arguably the most important—geographical challenges (availability). For example, when people do not feel they have a voice in the courtroom because they cannot communicate in their own language or they are not represented in the jury box, they are less likely to trust the judicial system (Huebert and Liu, 2017; Liu and Baird, 2012). Likewise, when people believe bribes must be paid in order to expedite some paperwork—whether it is dealing with the police (Kutnjak Ivković, 2008; McCarthy et al., 2021) or registering a business (Frye and Shleifer, 1996)—they are less likely to trust the bureaucracy. In both examples, there is a barrier—linguistic (ascriptive) or financial—that makes the institution not wholly accessible. In this paper, we draw on Miteniece et al. (2018) and focus on another type of barrier: spatial. When people have to travel great distance to engage in the requisite services, these services are less available—thereby hampering institutional trust.
Spatial barriers are especially pronounced with the maternal healthcare system—more so than the courts, police, or even other dimensions of the healthcare system. Since the maternal healthcare system includes 10 months of pregnancy, the childbirth itself, and the postpartum period, effective care means being able to access the medical facilities and professionals repeatedly. Reporting a crime to the police, for example, is a one-time interaction. Likewise, getting a knee replaced—while it may take multiple visits and physical therapy—requires far fewer repeated exchanges.
Spatial distance matters for two reasons. The first is through generalized trust. Mothers are recommended to make multiple doctor visits during the pregnancy and after childbirth. These checks serve multiple purposes. They identify and manage potential concerns for the mother’s health. They are also opportunities to test the wellbeing of the fetus (and the young baby). These visits allow mothers to be better informed; they are also opportunities for mothers to be better acquainted with the requisite medical professionals. Put differently, this knowledge and familiarity—that is, approachability—parlays into generalized trust.
But if mothers have to travel great distance to make these regular visits, they will make fewer visits. First, there are matters pertaining to affordability. Traveling long distances can be costly—in money and/or time. Second, there are factors of appropriateness: When mothers make these visits, they will arrive physically uncomfortable and mentally exhausted. They are likely to perceive facility and professional inadequacies. And third, there is the acceptability factor: When mothers have to travel great distance, this puts her out of her comfort zone. While each of these factors may be small, when compounded, a large distance exacerbates each one—thereby dampening generalized trust of the institution.
The second reason why spatial distance matters is about specific trust. The maternal healthcare system also includes the childbirth itself. The greater the distance mothers must go to deliver a baby, the longer they are in physical trauma and mentally frightened. This touches upon matters of approachability and appropriateness. Once in the hospital, interacting with medical professionals—who may not be from their village, understand and speak the local vernacular—can be daunting. In Georgia, these cultural barriers are even more pronounced in areas with large Armenian, Azerbaijani, and other ethnic minority populations. In fact, it is possible the medical professionals may subconsciously discriminate against the mother. For example, a mother’s cry that she is experiencing unusual pain could be dismissed as an exaggeration. This suggests increased concerns with matters of acceptability. A greater distance also means more challenges—from an affordability standpoint—for family members. It is harder for family members who accompany the mother to run back home to grab something. The heightened trauma from the childbirth can negatively affect specific trust in the maternal healthcare system itself.
Because of the length of pregnancies and postpartum periods and the intensity of childbirths, large distances to medical facilities can dampen a mother’s trust in the maternal healthcare system—whether generalized or specific. The following hypothesis summarizes our argument:
A mother’s trust in the maternal healthcare system decreases as spatial barriers to maternal healthcare access increase.
Overview: Maternal healthcare in Georgia
In this section, we provide overview of Georgia’s maternal healthcare system. In general, we can break down the story into a trilogy—with a prequel. The prequel is the Soviet period (–1991). During this time—per the 1964 Basic Law on Health in the USSR and Soviet Republic—hospitals were government-owned and financed through public funds. Access to maternal healthcare specialists—from medical nursing outposts to polyclinics, from obstetrics and genecology specialists to regional hospitals—was widespread even in the most rural areas. Healthcare coverage—from treatment to medication to food—was universal and nominally free although bribes were common (Dagargulia and Badashvili, 2008; Shengelia et al., 2016).
All this changed with the collapse of the Soviet Union. Independence came hand-in-hand with acute economic woes. To be fair, these troubles had started to manifest in the last decade of the Soviet era (Rowland and Telyukov, 1991). Nonetheless, these financial challenges meant the government was in no position to either sustain the monstrous infrastructure from before or invest in an alternative, smaller system—as evident by the drop in healthcare spending per capita: from $95.5 USD in 1985 to $0.90 in 1994 (Jinjolava, 1998). In the first episode, during President Eduard Shevardnadze’s tenure (1992–2003), the government adopted a controversial reform package (1995) per World Bank recommendations (Sumbadze & Dolidze, 2002). The reforms were extensive—from decentralization of healthcare to the creation of a licensing system (Gzirishvili and Mataradze, 1999). They included privatization of all healthcare institutions—whether allowing employees to buy their shares or to auction off their shares (Dagargulia and Badashvili, 2008). The result was a drastic reduction in the number of healthcare facilities and medical professionals. This would affect the maternal healthcare system as well.
The reforms of this first episode also included a transition to a state medical insurance system. The government created a fund that pooled together payroll contributions from both employers (3%) and employees (1%); the state itself also contributed funds to cover pensioners, children, and the unemployed (Collins, 2003; Gamkrelide et al., 2002; Gotsadze et al.,2009; Veillard et al., 2005). In principle, funds from this insurance system—along with funds from other sources (Chanturidze et al., 2009; Kalandadze et al., 1999)—would cover basic healthcare needs for the general population. But it was not enough to cover selective diseases such as cancer treatment. Additionally, given poor management and widespread corruption, the system proved to be underfunded. All this meant an increase in out-of-pocket payments—estimated at 87% of total health expenditures (UNFPA, 2005)—which proved especially problematic for the more marginalized populations, for example, women, ethnic minorities, and those in remote areas, borderlands, and conflict zones (Balabanova et al., 2004).
We see some efforts to address these newfound challenges in the second post-Shevardnadze episode. During President Mikheil Saakashvili’s administration (2003–2013), the government recentralized all healthcare authority. For example, the central government was once again in charge of budgeting and decision-making. However, given the tremendous costs to maintain the oversized infrastructure and overstaffed hospitals—coupled with strong lobby interests by pharmaceutical companies—the government effectively privatized the entire health sector (Shengelia et al., 2016). The government adopted a vertical maternal healthcare program—for example, antenatal care through private women consultation and maternity house (Interview 1 with National Center for Disease Control and Public Health representative). 2 By 2010, nearly all government health facilities were privately owned; moreover, the government adopted a vertical maternal healthcare program—for example, antenatal care through private women consultation and maternity houses (Shengelia et al., 2016). And in the absence of a regulation over costs, this meant increasing prices across the board in all health services. Bregvadze et al. (2002) talk about how the state introduced an obstetrics voucher system to offset the costs of birthing a child. However, as it turned out, the market price for childbirth services increased at a faster rate than the amount afforded by the vouchers (Interview 2 with National Center for Disease Control and Public Health representative). 3 And as a result, the vouchers—which were initially meant to be universal financial support—ended up manifesting more as a state subsidy (Dagargulia and Badashvili, 2008).
It was also during Saakashvili’s tenure that the government terminated the social health insurance system and replaced it with a private one (Djakeli, 2013). While multiple private insurance companies emerged—with the hopes that market competition would force transparency and accountability—the market itself developed with neither an assessment of population needs nor the guarantees of support for those who could not pay their healthcare. While the government would later buy insurance from these private companies for the most vulnerable, it was not enough (Shengelia et al., 2016).
Since the government had privatized both the healthcare facilities and the insurance system without consulting the general public (Chanturidze et al., 2009; Gamkrelidze et al., 2002), these reforms were highly unpopular—and not surprisingly, subject to reversal post-Saakashvili. In the third episode (post-2013), the government launched a universal healthcare program while maintaining the extant health insurance system. This ensured healthcare access to the whole population. The implications for maternal healthcare have been far reaching. Prenatal screenings are covered—from hepatitis to HIV to syphilis; from detection of congenital anomalies (babies) to management of high-risk pregnancies (mothers). Folic acid and iron supplements are also free of charge. And the costs for the childbirth itself are covered by the government, regardless of childbirth method (Shengelia et al., 2016; Zoidze et al., 2012).
Also, as part of the new reforms, the government focused on increasing geographic and financial accessibility for all—and not just to primary healthcare but also urgent hospitals and outpatient services. To make this happen, local doctors were recruited and incorporated into a larger network. The previously standalone local clinics were now upgraded and brought into a national system to manage medical emergencies—putting patients closer to these requisite services. The coordination of multiple doctors and facilities first addressed outpatient assistance, urgent hospital assistance, and scheduled outpatient and polyclinic services. They were later expanded to also include primary healthcare services, urgent outpatient assistance, extended urgent hospitalization, planned surgeries, treatment of oncological diseases, and childbirth (Shengelia et al., 2016). We see similar coordination efforts to reduce the geographical gap by expanding access for maternal healthcare. The development of a national network of women consultation centers 4 and maternity houses 5 —funded by the government and administered through multiple agencies—ensures that all pregnant women are “at the right place at the right time” (Interview with Health Ministry representative) 6 . Having discussed the trajectory of the (maternal) healthcare system in Georgia, in the next section we test whether access has mattered for institutional trust.
Research design
To test our argument, we employ survey data (IRB protocol: UT 2019-03-0094 and NCDC 2019-020). We worked with a reputable survey company in Georgia (Gorbi). The surveys were piloted in June 2019 and then administered in July 2019 to a nationally representative sample with an over-sampling of adult women (N>700 women). 7 The surveys were administered face-to-face on a tablet. All respondents were warned about an audio recording. Only those who consented were administered the survey. The purpose of the recording was to ensure quality control. 8 Additionally, Gorbi equipped each tablet with GPS trackers to verify the random-route sampling. This would also allow us to identify each respondent’s place of residence (more below). In the survey, women were asked about each birthed child—from the pregnancy itself to the birth to the post-partum experiences. 9 We treat each birthed child as a unique observation. On average, women birthed fewer than two children, although the number was higher for ethnic minorities (2.5) than ethnic Georgians—figures consistent with Dagargulia and Badashvili. (2008). The unit of analysis is mother-child (N = 1208).
Institutional trust
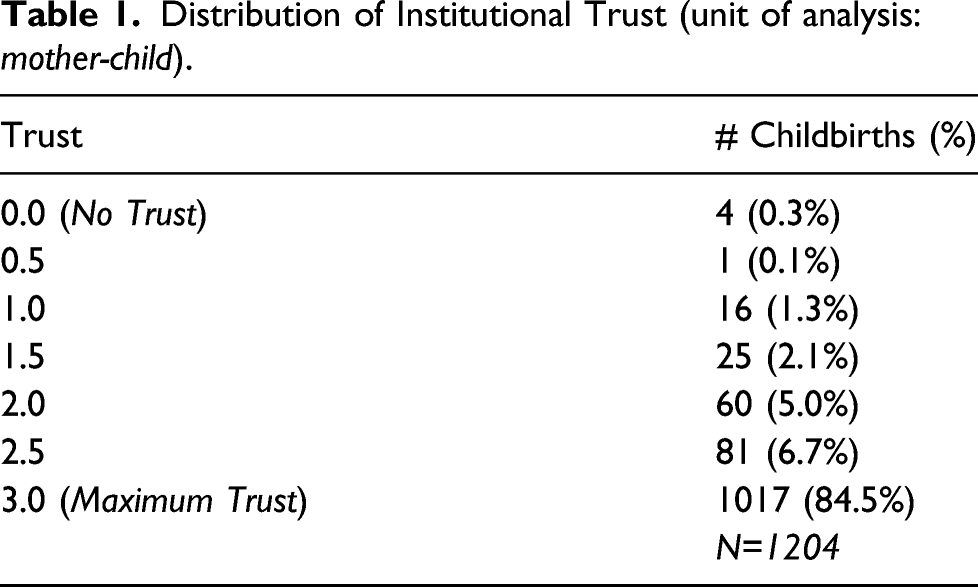
To measure institutional trust, we used two questions about satisfaction with the facilities and personnel. The first focuses on the pregnancy in general: “How strongly do you agree with the following statement: During my n-th pregnancy, the doctor and nurses respected me and listened to my needs.” This question taps at diffuse institutional support (see Baird, 2001; Tyler, 2006; Tyler and Rasinski, 1991)—that is, whether mothers feel the maternal healthcare system runs well. Responses ranged along a four-point scale from strongly disagree (0) to strongly agree (3). The mean, median, and mode are all at a 3: Almost 90% of the respondents answered strongly agree—with fewer than 1% of the respondent saying strongly disagree.
Conversely, the second question is about the childbirth in particular: “How strongly do you agree with the following statement: When I gave birth to my n-th child, the doctor and nurses respected me and listened to my needs.” By focusing on the birth of the child, we are better able to isolate for the specific institutional support (Gibson et al., 1998; Huebert and Liu, 2017)—that is, whether mothers are satisfied with the outcome. Responses again ranged along a four-point scale—with the mean, median, and mode also at a 3. Note, however, that while 89.6% of the respondents answered strongly agree, the number of respondents who said, strongly disagree doubled when it came to the specific pregnancy (1.9%).
Three comments warrant mention. First, recall, the unit of analysis is not the mother but rather, the mother-child. And thus the question is about the mother’s experience birthing this one particular child and not across all childbirths. In the survey, each question was repeated for each child. As such, a mother can theoretically have a terrible experience with one childbirth but a positive one with another. Second, since we are asking mothers to focus on each childbirth, inevitably this means responses of institutional trust for the oldest child versus the youngest child are drawn from more distant memories. Here we are not concerned since there is no reason to assume the most recent childbirth is objectively that recent. Moreover, it is possible that someone may have had multiple children in a short period—and all recently. Third, because the survey was nationally representative on regions and had quotas for age, there is a natural imbalance on how many childbirths were in each period: Soviet era (N = 367), Shevardnadze era (N = 479), Saakashvili era (N = 107), and post-Saakashvili era (N = 216).
Distribution of Institutional Trust (unit of analysis: mother-child).
Maternal healthcare access: Geographical distance
Our key explanatory variable is the distance between the respondent’s place of residence and the hospital where the child was delivered. Here, we operationalize distance in driving kilometers (versus as the crow flies). In the survey, we asked respondents to provide the name of the hospital where each child was delivered.
10
We matched hospital names to those on the Georgian Health Ministry website. In the cases where they matched, we then identified the corresponding GPS coordinates. Some hospital names, however, changed over time. In other cases, hospitals ceased to exist. In the cases where we were not able to match the names,
11
we then employed two country experts. The Head of the MA Gender Studies Program at Tbilisi State University and the Head of the Division of Maternal and Child Health at the Georgian National Center for Disease Control and Public Health helped us triangulate and identify the missing GPS coordinates. Once we had the hospital coordinates, we then used Google Map’s Distance Matrix API to measure the distance between the hospital and the mother’s residence—as identified by the location tracker on the survey tablet. The median distance to a hospital is 12.4 km (mean: 43.2 km). Figure 1 shows the histogram distribution of distances for each period. Given the non-normal distribution of this variable, we take the log transformation of the distance. Histogram of Kilometers to medical facilities (% of total childbirths per era).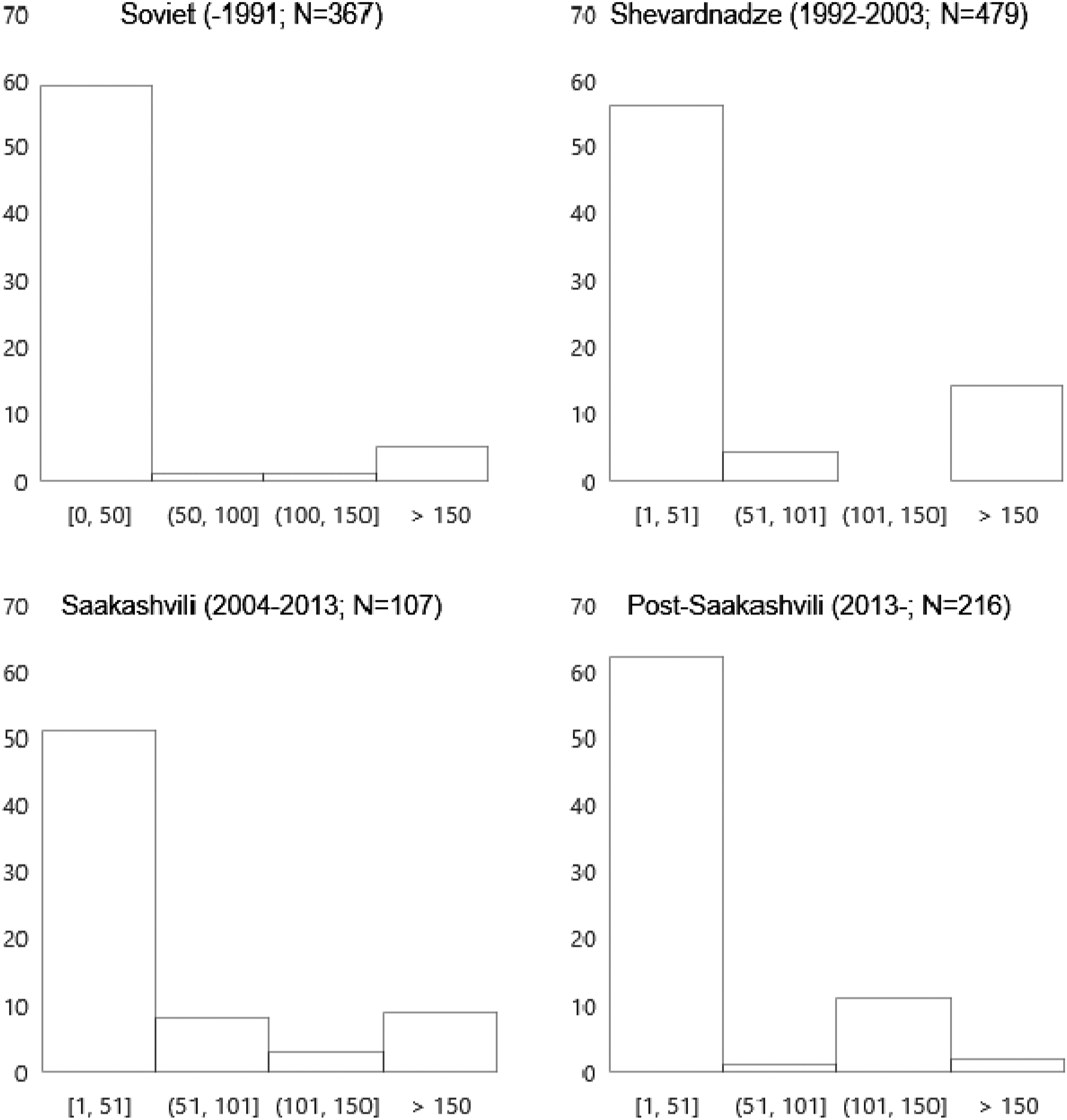
There is the possibility that a respondent lived in a different location previously—and delivered a child from that other location. And since the mother’s GPS location only identifies the current place of residence, this would result in a mismatch. To address this concern, we asked respondents to identify how long they have lived in their current place. With this information, we could then drop the observations where a child was delivered prior to the mother moving into her current place.
Control variables
To consider possible confounding factors, we include four sets of controls. The first set includes those specific to the pregnancy—that is, the child. Here we consider the number of prenatal visits the mother made (# Prenatal Visits). The World Health Organization (WHO) recommends a minimum of four visits. When mothers make more visits to the doctor while pregnant, it increases their opportunity to interact with doctors and nurses. Questions that they may have are more likely to be addressed during these visits—that is, knowing the fetus is growing at a healthy rate or that the mother has preeclampsia. These repeated interactions and knowledge can improve how mothers see the maternal healthcare system (Miteniece et al., 2018). Another prenatal concern has to do with costs (Cost Concerns). The average out-of-pocket expenses for childbirth remain a burden (Shengelia et al., 2016; Zoidze et al., 2012)—and in fact, the wealthier pay more out-of-pocket (Curatio International Foundation, 2015). Moreover, the cost of medicine is almost triple that of other European countries (Shengelia et al., 2017). As costs become prohibitive, the inability of the mother to pay—or the even the stress of how to pay—for what is necessary can affect the actions they take and how they subsequently see the maternal healthcare system. The variable is a four-point ordinal scale from none to slight to somewhat to major.
We consider circumstances surrounding the childbirth itself as well—for example, whether it was a c-section (if yes, Cesarian=1); whether the mother teared (if yes, Tear=1); and whether the mother experienced any post-birth complications (if yes, Post-Birth Complications=1). Given the stresses of childbirth and being a new mom, we also control for the number of postnatal visits (# Postnatal Visits). And finally, since environmental matters can also affect pregnancies—or indicate other ongoing stressors in the immediate surroundings—we also control for whether the mother drank (if yes, Consumed Alcohol=1); whether the mother smoked (if yes, First-Hand Smoke=1); and whether other people in the mother’s household smoked (if yes, Second-Hand Smoke=1).
The second set of controls pertains to the mother
We also control for the number of abortions and miscarriages the mother has had. To be transparent, the theoretical mechanisms are very different. While abortions were a common form of birth control particularly in the 1990s (Dagargulia and Badashvili, 2008), there is still stigma surrounding it. Mothers may experience more guilt when delivering a baby; alternatively, doctors and nurses may be more likely to shame the mother for having had multiple abortions. Conversely, miscarriages happen for many reasons. But mothers may feel grief—or intense happiness—when they successfully deliver a child. This can affect how they see the maternal healthcare system. Given the topic sensitivity, we were not comfortable directing asking respondents to tell us how many times they had an abortion and how many times they miscarried. Instead, we asked them to identify how many times they have been pregnant and how many children they delivered. The difference between the two (# Abortions and Miscarriages) is the result of one of the two mechanisms.
The third set of controls is temporal
And finally, the last set of controls is a spatial one—that is, some regional effect. Regions vary in their economic development, population size, and demographics. The region of Kvemo Kartli—in southeast Georgia, on at the border of Armenia and Azerbaijan—is home to a larger non-ethnic Georgian population. Regions can also differ in their available resources. For example, Tbilisi is likely to command more attention—both domestically and internationally—than other regions. Because of this asymmetry, there have been efforts to spread resources to other regional centers such as Kutaisi and Batumi.
Empirical evidence
As a first glance, we look at the average levels of institutional trust across the prequel and the three episodes in the trilogy: (1) the Soviet era (−1991); (2) the Shevardnadze era (1992–2003); (3) the Saakashvili era (2004–2013); and (4) the post-Saakashvili era (post-2013). If our priors are right, we should see higher trust levels during the Soviet and post-Saakashvili eras—and certainly the lowest during the Shevardnadze years. Figure 2 shows the distribution across the four periods. Recall, trust is the measured along a four-point scale—where a minimum of 0 means no trust whatsoever (and a maximum of 3 suggests complete trust). Histogram of institutional trust (% of total childbirths per era).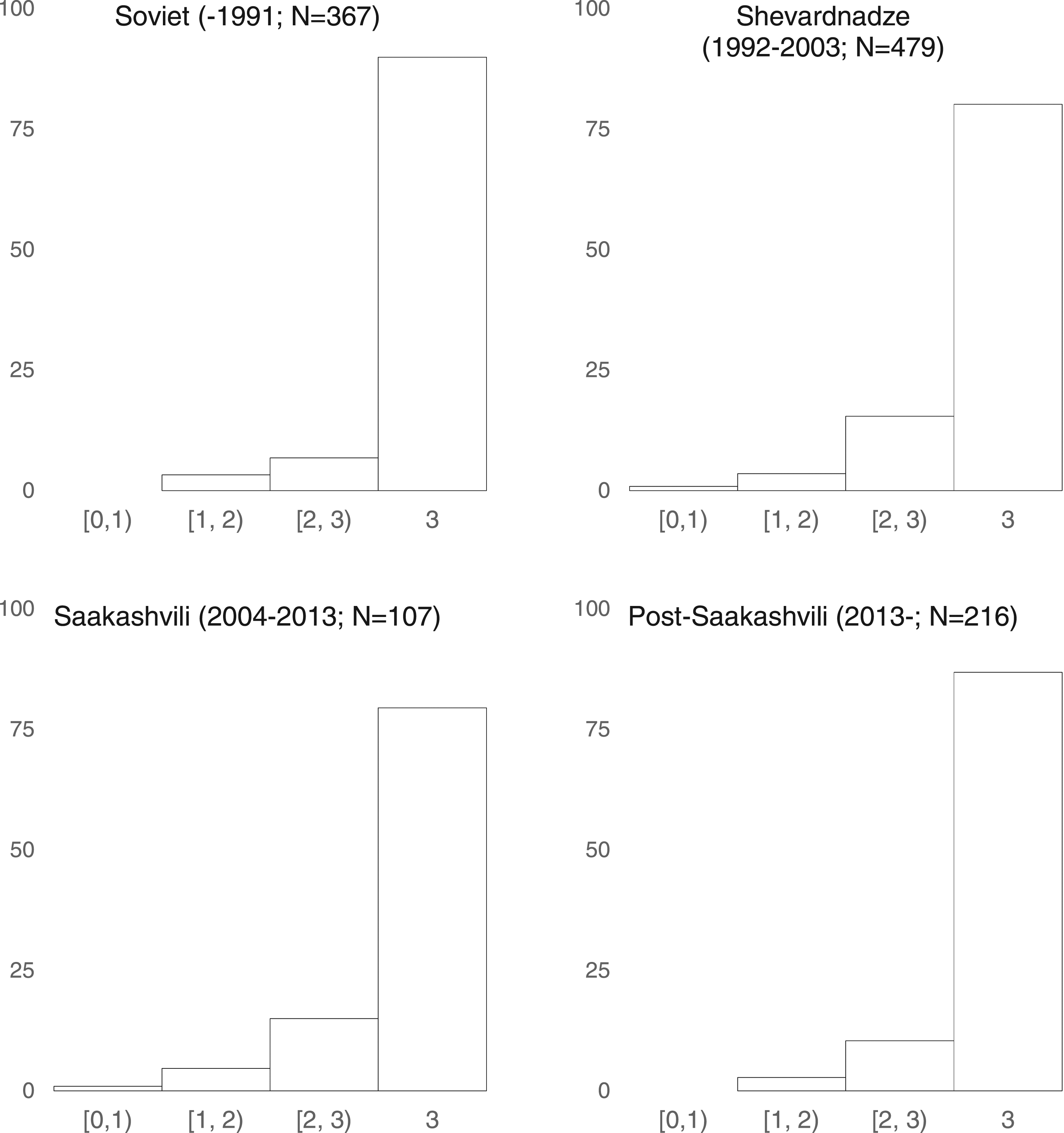
Several observations merit discussion. First, it seems that institutional trust seems largely robust and stable across all four periods. The distribution skews left where the modal response in all four periods is a 3. This is normatively welcomed. However, there is some difference in the average levels of institutional trust. The difference between the Soviet era (average: 2.90) is significantly different from that of the Shevardnadze (average: 2.80; p-value=0.00) and Saakashvili (average: 2.78; p-value=0.00) eras. It is, however, not statistically different from that in the post-Saakashvili era (2.89; p-value=0.81). Moreover, note that in both the Soviet and post-Saakashvili eras, no respondent gave the lowest response of a “0”. This is all in accordance with our priors.
Next, we consider the average distances (measured in kilometers) traveled across the four periods. Consistent with expectations, the distance to medical facilities and personnel was shorter during the Soviet era (average: 31.56) than in any of the subsequent three periods (see Figure 2). And as expected, the average distanced traveled also increased over time in the post-Soviet era—peaking at an average of 52.22 during the Saakashvili years, but since then decreasing to a level that is statistically no different from the Soviet era (average: 34.01; p-value=0.81).
Effects of kilometers traveled on attitudes towards maternal healthcare.
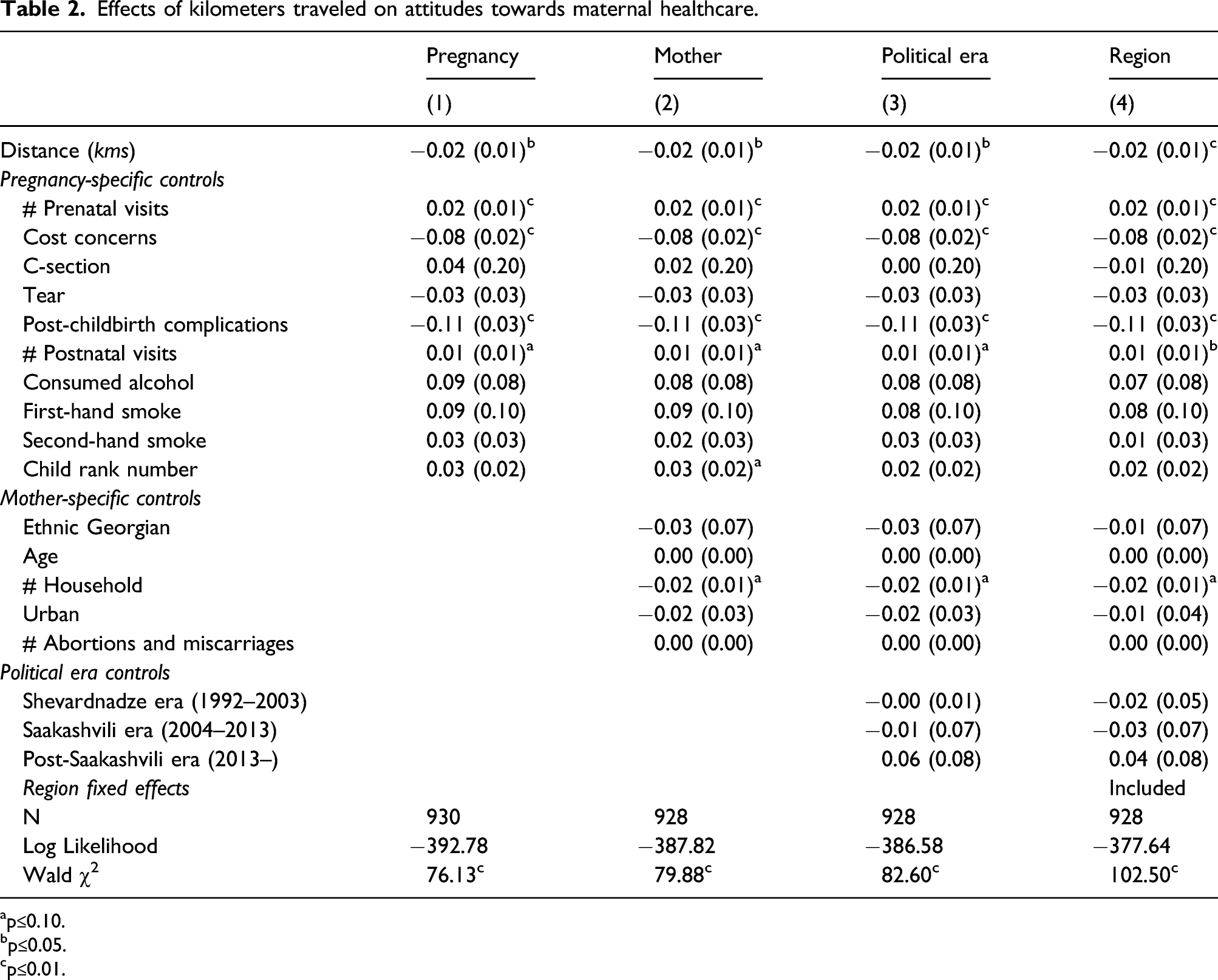
ap≤0.10.
bp≤0.05.
cp≤0.01.
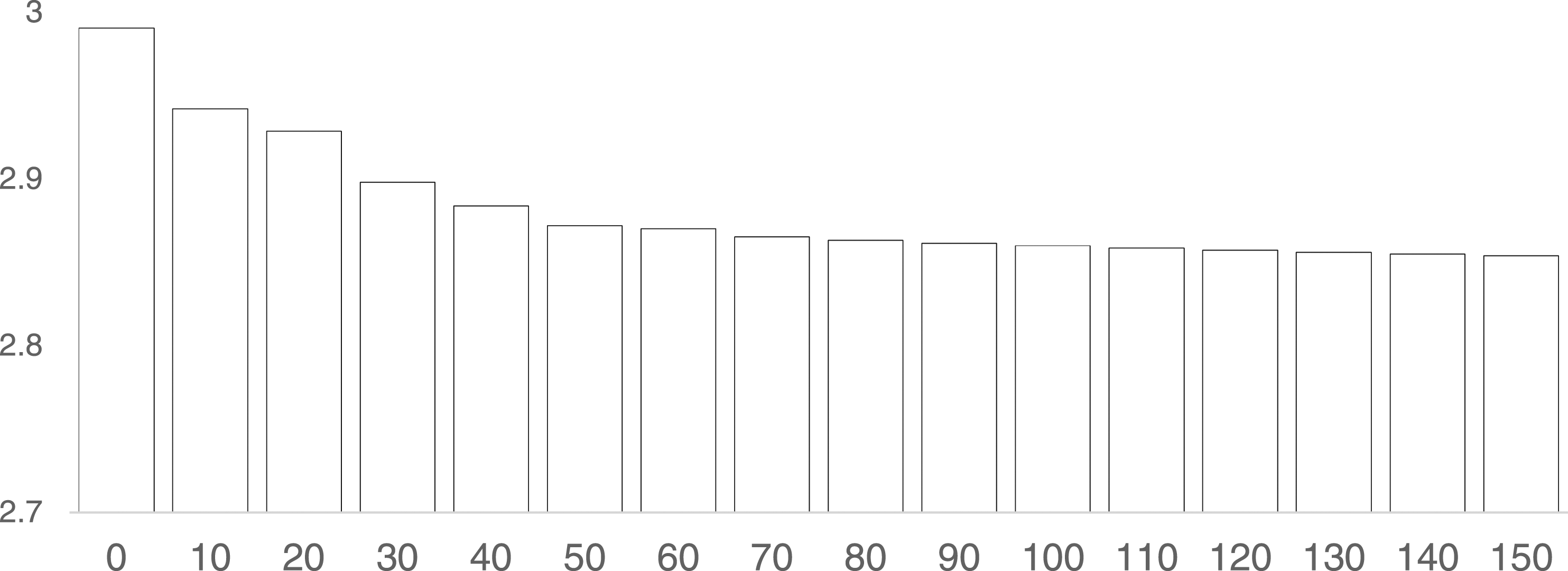
Predicted values for institutional trust across Kilometers.
Several pregnancy-specific controls matter for institutional trust. First, as the number of prenatal visits increases, trust in the maternal healthcare system also increases. On average, mothers visited the doctors six times per pregnancy. From a medical standpoint, this is encouraging—especially considering almost a quarter said they visited the doctor 10 times during their pregnancy. However, another 15% visited the doctor less than four times (6% had zero visits)—the minimum threshold recommended by the WHO. Second, cost concerns were also important. And in fact, this one variable singularly has the largest effect. A shift from no cost concerns to a slight concern can decrease trust by up to 0.16—on a four-point scale! Third, post-birth complications also affected how much mothers trusted the maternal healthcare system. Whether it was high blood pressure, post-partum depression, hemorrhaging, or infections, the presence of any one of these complications decreased trust by 0.13—a non-trivial magnitude larger than that of distance to hospital. Fourth, the child order matters as well. First-time mothers are twice as likely as mothers who have birthed previously to evaluate the maternal healthcare system negatively, although the average effects are much smaller. And finally, the number of postnatal visits—just like the number of prenatal visits—has a positive effect. As the frequency of visits increases, institutional trust increases as well. However, unlike prenatal visits, the numbers for postnatal visits are much smaller with a sample mean of 2. Interestingly, whether the mother had a terrible childbirth itself—including having to deliver a baby by cesarian section or tearing—had no bearing on how she evaluated the system. Likewise, the alcohol consumption and smoking behavior of the mothers (and those around them) has no effect.
Among the mother-specific controls, the only variable that is significant across all model specifications is household size. Mothers from larger households were less likely to trust the maternal healthcare system. Some of this could emanate from the stress of having to oversee a large household with many children while pregnant and nursing a newborn. Alternatively, large households could also suggest aging parents (or in-laws) living with the mothers. The challenges of having such individuals could also tarnish how mothers evaluate the maternal healthcare system. For example, a mother (in-law) continuously talking about things were better during the Soviet era when everything was free could make a mother annoyed with having to pay anything in the contemporary.
While none of the other mother-specific controls was significant, they were all signed in the correct direction. Interestingly, ethnic Georgians were more critical of their own maternal healthcare system than non-Georgians, whether it was Armenians, Azerbaijanis, or Russians—although the effect flips (and remain non-significant) once we control for regions. One possibility is that the mothers who cannot communicate in Georgian or Russian—and thus experienced discrimination during the pregnancy and childbirth—are also the ones not being surveyed. The survey was administered only in Georgian and Russian. Older mothers may seem more critical although the effect is neither significant nor substantive. In fact, among mothers birthing in the post-Saakashvili period, age has no effect whatsoever on institutional trust. A simple means test comparing young mothers under 25 (N = 34) versus older mothers over 35 (N=56) shows consistently high levels of institutional trust (2.90 vs 2.88; p-value=0.26).
Mothers who have had more abortions or miscarriages were also more critical. Although here it is important to clarify that we do not know the specific numbers for abortions and miscarriages—that is, we cannot disentangle whether it the general pattern is driven by guilt or grief. All we know is how many times the mother was pregnant and how many times she has gave birth. Finally, mothers in urban areas generally are also less trusting of the hospitals—although again, the effect is not statistically significant. One possibility for this is that while hospitals may be more accessible, they also service more people. Thus, the attention each doctor can render on the mother decreases.
When it comes to temporal effects, 1992 was indeed a bad year for institutional trust (results not reported). For example, mothers who birthed a child in 1992 was anywhere between 0.20 to 0.30 points more negative (on a 1 to 4 scale) about the maternal healthcare system than mothers who birthed a child between 2014 and 2018. This is consistent with theoretical expectations: Not only was the year following the Soviet collapse difficult, but recent developments to the maternal healthcare system have also improved institutional trust.
Healthcare systems, however, can take time to change; the effects of adopting a policy—for example, vouchers—does not happen overnight. Moreover, the effects may be interactive as opposed to merely additive. As such, it may make more sense to look not at the individual years but at the political era. When we do this, the direction of each of the coefficients is interesting. Mothers birthing during the Shevardnadze and Saakashvili eras were more critical (albeit not statistically) of the maternal healthcare system than mothers birthing during the Soviet era. Yet, mothers birthing in the post-Saakashvili were more positive and trusting than those in the Soviet era. While these differences are not statistically significant—suggesting a lot of the variance is being picked up by the other control variables—they are normatively welcomed. There are two ways to interpret these results. First, they are consistent with policy changes to maternal healthcare. For example, between 1995 and 2017, the system only covered four free antenatal visits. In 2017, the number increased to eight. We would expect the number of reported antenatal visits for pregnancies to also increase. And indeed, we see this: 5.5 during the Soviet era to 6.5 during the Shevardnadze era, from 7.4 during the Saakashvili era to 7.9 in the post-Saakashvili era.
Second, there could be a survey respondent effect. It is possible that people who birthed a child a long time ago—for example, during the Soviet era—are less likely to recall specific details. In fact, it is possible that if their child is now an adult, they may be more inclined to think of the whole experience positively. In contrast, people who had really bad experiences—especially during the Shevardnadze era—have moved abroad, and therefore their experiences are not being captured by the surveys. Nonetheless, all this suggests that what the current Georgian government is doing to address maternal healthcare is manifesting positively. And finally, these effects are also largely uniform across the different regions—whether it is Tbilisi (the capital), Kutaisi (the capital of Imereti region, one of the cities for the pilot maternal healthcare programs), or Batumi (the capital of Adjaria region, one of the cities receiving large maternal healthcare funds).
Alternative measure of distance: driving time
Spatial proximity is not only about distance in kilometers. A hospital just a few kilometers away can be hard to reach if the road winds through the mountains. Likewise, a hospital many kilometers away can still be accessible if the road to there is well paved. Put differently, what may matter is not the number of kilometers per se, but the time required to get to the hospital. In this subsection, we consider this alternative measure. We focus on the number of minutes required to go from the mother’s place of residence to the hospital—again, per Google’s Distance Matrix API. The average time spent getting to a hospital is 43.8 min, although this is certainly pulled to the right because of several extreme outliers (e.g., the top one percentile exceeded 307 min with a maximum of 549 min). At the other end, more than 21% of the pregnancies were less than 10 minutes from the hospital (N = 249). The median distance measured in time is 21 min. The correlation between distance in kilometers and distance in minutes is 0.98 (p-value=0.00).
Effects of time traveled on attitudes towards maternal healthcare.
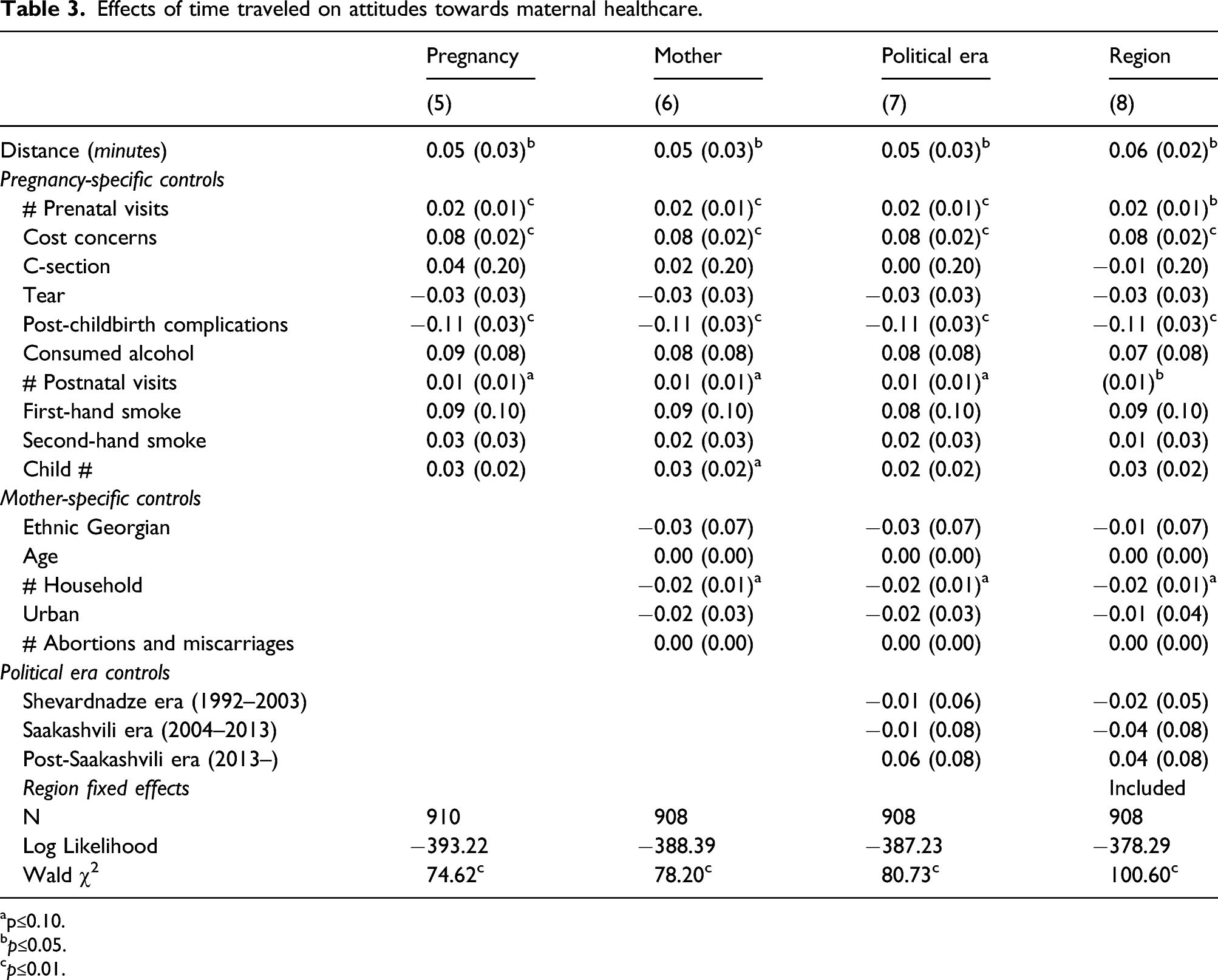
ap≤0.10.
bp≤0.05.
cp≤0.01.
Disaggregating institutional trust
Thus far we have measured institutional trust as the average of diffuse support (pregnancy) and specific support (childbirth). And while the two types of support are positively correlated—that is, as one goes up, the other goes up as well—mathematically, the correlation itself is quite low with an alpha Cronbach score of 0.56. In this subsection, we consider the effects of distance on the two constituent terms. Specifically, we are interested in whether traveling a large distance has a greater effect on how the mother evaluates the entire pregnancy in general or the childbirth in particular—or whether the effects are the same.
We rerun the full models from before (inclusive of political era controls and regional fixed effects). But in the first instance, we use only the diffuse support (pregnancy) question for the dependent variable. And then in the second instance we use the specific support (childbirth) question for the dependent variable. Figure 4 plots the marginal effects for distance in both models in the same figure to compare their magnitudes. Disaggregating institutional trust: Marginal effects.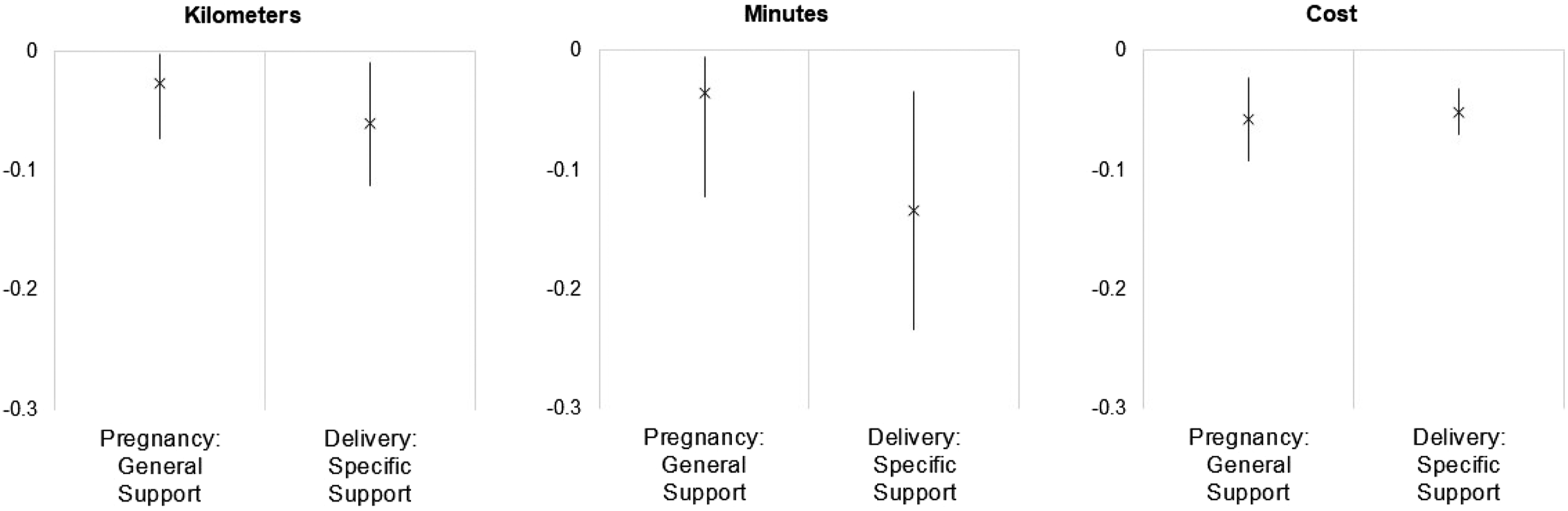
We see in the first panel, as distance (measured in kilometers) increases, the effect on institutional trust decreases (as noted by the negative marginal effects). The effect is statistically significant for trust in the general maternal healthcare system—per our question on satisfaction with facilities and personnel during the pregnancy. The effect is also significant for trust specifically based on the childbirth experience. And while the magnitude is larger for the specific trust (−0.06 versus −0.02), the difference is not in of itself significant. This suggests that while it the experiences from the childbirth itself matters more, the experiences throughout the pregnancy are not necessarily less important.
We subject this finding to two other reference points. The first is the use of the alternative measure of distance. We see in the middle panel that the effects for minutes are qualitatively the same as those for kilometers: As the minutes needed to access medical facilities and personnel increases, trust in the system decreases—both generally and specifically. And while the effects seem to have a larger range, they are (1) neither statistically different between the two types of trust; and (2) neither statistically different from the effects from the kilometer models.
The other reference point is that of cost. We know from the literature and from the empirics that cost is important. The high rate of paying out of pocket can negatively affect how often mothers can access the maternal healthcare system; it can also color their overall experience; and most important, it can parlay into whether they have a good or bad experience in childbirth. In the third panel, we plot the marginal effects for cost in both models (using the kilometer measure for distance). Again, we see the effects are statistically significant and negative—for both generalized and specific trust. However, the effects are neither differentiable between the two types of trust nor differentiable from the effects of distance.
Conclusion
In this paper, we explored whether geographical distance hinders institutional trust; and if so, whether reducing this gap can improve satisfaction. Using original survey data, we find that spatial proximity matters for how mothers see the maternal healthcare system—whether it is about the pregnancy in general or the childbirth specifically. Women whose homes are closer to the clinics where they see medical staff and give birth report significantly higher levels of trust in the medical system. The results are robust to how we measure distance and how we conceptualize institutional trust.
Improving access to quality maternal care is not just about increased trust per se. It is about saving lives. Fewer mothers are dying because the government is not just spending more money but spending money to develop and coordinate a national network of medical facilities and personnel. The improvements in accessibility for mothers has led to a drastic reduction in the number of mothers dying by almost half—from 43 to 25 deaths per 100,000 live births. The results are also normatively reassuring for a country that has labored to ensure the “right woman is at the right place at the right time.”
The link between accessibility and trust and the possibility of drastically reducing maternal mortality are by no means restricted to Georgia. While Georgia is “an oasis of a democracy in an authoritarian sea” (Ishiyama et al., 2018, p. 19), in many ways the country is also very representative of a larger global sample of countries: It recently democratized but is plagued by widespread corruption; it embraced market reforms but struggles with inequality; and it is determined to be an independent, sovereign state but continues to battle foreign interferences. Improving access to maternal health through the upgrading and coordinating of local clinics, regional hospitals, and service provision near all populations can make a dramatic difference for the quality of care and institutional trust. How the Georgian government has responded from its post-Soviet calamities to build trust in the maternal healthcare system should serve as a best practice, blueprint for other countries.
The finding that spatial proximity matters for institutional trust is by no means specific to the maternal healthcare system—or even the healthcare system at large. It speaks to any system that exists to serve the public and requires trust for legitimacy—for example, the judiciary (Bolkvadze, 2020), pensions (Veshapidze and Karalashivili, 2018), or the police (Kakachia & O’Shea, 2012; Light 2014; Puppo, 2010). If the average citizen cannot easily engage with the facilities or personnel, the system is inaccessible. Note, however, there is an important caveat: While spatial proximity is a necessary condition to build institutional trust, it is not sufficient. As Miteniece et al. (2018) demonstrate, accessibility can also be blocked for other reasons. Still, one lesson for government officials and NGOs is to examine the availability of services—not just by examining the total supply but by focusing on the location of both the supply and demand to ensure services are appropriately located.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by University of Texas at Austin (President's Award for Global Learning).