
Abstract
Parkinson's disease (PD) shows pronounced clinical heterogeneity, with individuals presenting differing cognitive and motor trajectories despite similar levels of neurodegeneration, in particular striatal dopamine terminal loss. This variability underscores the relevance of considering resilience mechanisms, particularly cognitive and motor reserve, that may support preserved function in the face of progressive pathology and neurodegeneration. Building on a previously proposed conceptual framework of resilience in PD, this review provides an updated and integrative synthesis of recent evidence, including longitudinal studies, neuroimaging findings, and emerging insights into lifestyle-related factors. The review further extends the existing framework by addressing current methodological challenges and outlining future directions for incorporating resilience into neuroimaging research, biological staging models, and personalized intervention strategies in PD. Together, this work emphasizes the growing importance of resilience research in PD and its potential to improve prognostic accuracy and inform more precise and individualized therapeutic approaches.
Keywords
Introduction
Not all individuals with a neurodegenerative disease, such as Parkinson's disease (PD), experience disease progression in the same way. Some remain clinically stable for years, whereas others exhibit rapid decline despite comparable levels of neuropathology. As early as the late 1980s, Katzman and colleagues reported a striking dissociation between pathological burden and clinical presentation in dementia, 1 emphasizing that neuropathology alone cannot fully account for symptom variability. Since then, converging evidence has shown that cognitive and motor decline vary widely among individuals with similar degrees of neuronal loss. These differences have stimulated growing interest in the concept of resilience, 2 the brain's ability to adapt and maintain function in the face of progressive neurodegeneration. Resilience is commonly described in terms of various forms of reserve, including brain, cognitive, and, more recently, motor reserve. 3 These mechanisms are shaped by lifelong factors such as education, occupational complexity, physical activity, and vascular or genetic risk, all of which influence how pathology and neurodegeneration translate into clinical outcomes.
Notably, resilience research has been in the limelight of aging and Alzheimer's disease (AD) research and has only recently received more interest in movement disorders, such as PD. Yet, understanding resilience is increasingly recognized as central to explaining the marked clinical heterogeneity observed in PD. Because certain aspects of resilience (i.e., neural network resources, neuroplasticity) are thought to be build-up over and shaped across the lifespan, it also offers a framework for identifying modifiable protective factors and designing interventions to support long-term functional maintenance.
Building on prior conceptual work that introduced a framework for resilience and motor reserve in PD, 3 the present manuscript aims to extend and refine this framework in light of recent empirical and methodological advances. It first revisits the conceptual foundations of cognitive and motor reserve and then critically examines current approaches to quantifying and operationalizing resilience in vivo, highlighting both their potential and their limitations. Building on this, the manuscript delineates how lifestyle-related factors shape the development and modulation of cognitive and motor reserve across the disease course. It further integrates emerging neuroimaging evidence to identify the neurobiological substrates through which these influences manifest. Finally, the manuscript outlines key challenges and future directions for incorporating resilience into neuroimaging research, biological staging models, and personalized intervention strategies for PD.
Cognitive and motor reserve: A conceptual definition
The delayed emergence of motor symptoms in PD, typically occurring only after approximately 30–70% of dopaminergic neurons in the substantia nigra have degenerated,4,5 combined with the considerable clinical heterogeneity of the disease, strongly suggests the presence of neurobiological mechanisms capable of buffering the functional consequences of progressive neurodegeneration.
These buffering capacities may on one hand occur in response to acute neural disruption broadly across individuals, which would relate to the concept of compensation. It was recently for example shown that motor compensation was linked to increased M1–striatal connectivity and enhanced interhemispheric cortical plasticity, 6 which temporarily counterbalanced dopaminergic dysfunction. And while there is a large body of evidence on compensatory mechanisms in PD (for review see 7 ), it remains unclear whether such compensatory responses occur only short-term and ubiquitous across people with PD or whether they arise preferentially in certain individuals.
While compensation undeniably contributes to resilience, it is the interindividual variability in these adaptive resources that is conceptualized as resilience. Resilience is an umbrella term, which encompasses brain, cognitive, and motor reserve and refers to the cumulative individual capacity of neural resources that allows individuals to maintain functional performance despite progressive pathology (definition summary is provided in Table 1). While certain genes have been linked to higher resilience levels,8,9 resilience per se is generally not considered as a trait, but thought to develop dynamically across the lifespan and to vary substantially between individuals as a consequence of lifelong experiences and lifestyle-related exposures.
Defintions for the different concepts relating to resilience, reserve and compensation.
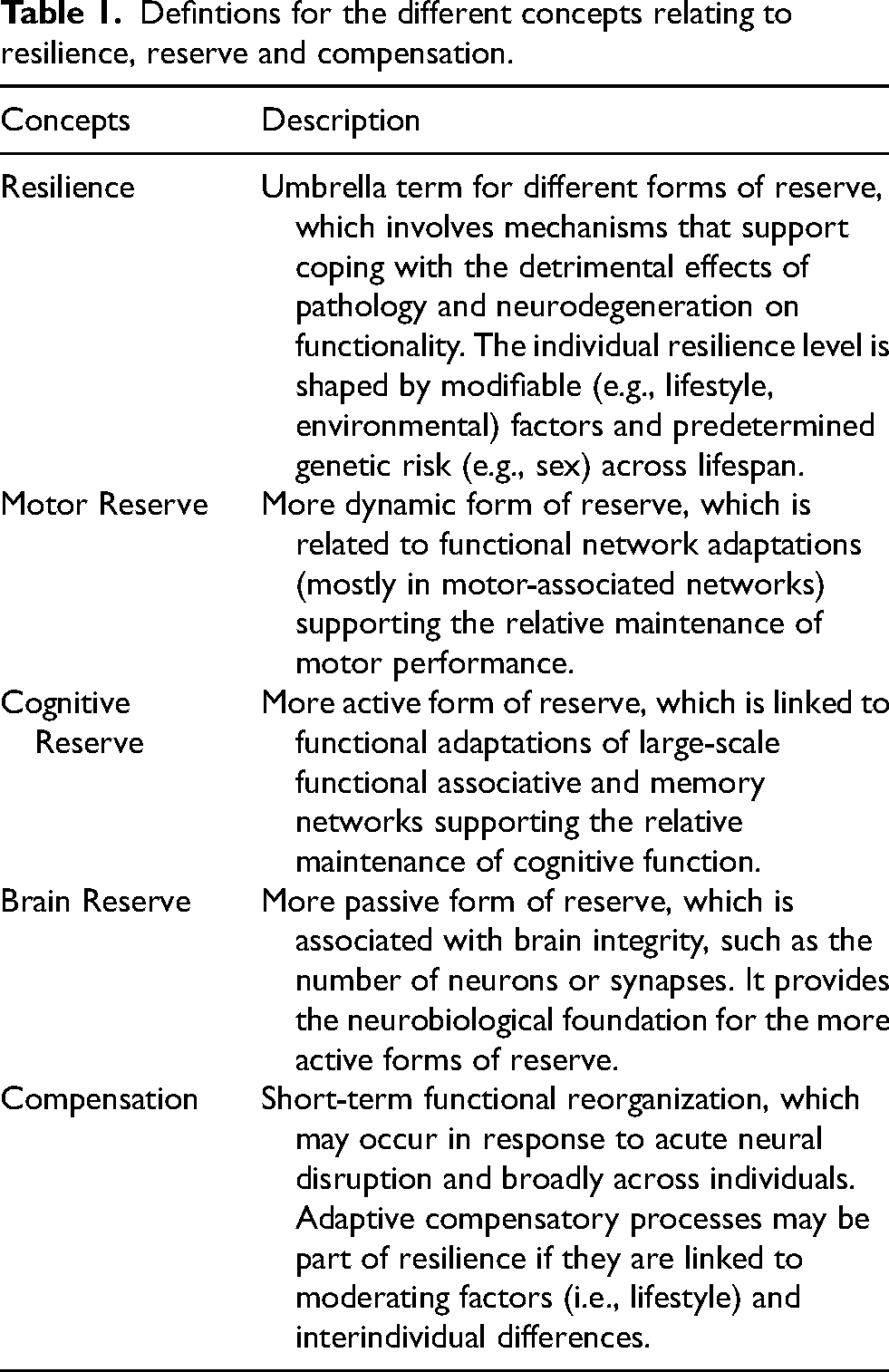
Resilience can manifest across multiple domains, including brain, cognitive, motor, psychological, and stress-related reserve, each reflecting distinct adaptive processes in the context of neurodegenerative disease. While psychological and stress reserve are highly relevant for overall well-being in PD10,11, brain reserve reflects relatively static structural capacity, often conceptualized as the brain's “hardware”. 12 In contrast to the more passive form of brain reserve, cognitive and motor reserve represent dynamic, experience-dependent processes that promote efficient neural recruitment, reorganization, and compensation, often described as the brain's “software”. Cognitive reserve refers to mechanisms that primarily support cognitive functioning, whereas motor reserve reflects the capacity to maintain motor performance despite comparable dopaminergic loss. 3
The present article focuses specifically on cognitive and motor reserve, as these domains are closely linked to both neuroimaging-based markers and the cardinal clinical features of PD. Overall, it is important to identify factors that contribute to the emergence and modulation of adaptive reserve mechanisms, as they may inform both preventive and interventional strategies. Achieving this requires robust approaches to quantify resilience in vivo, thereby enabling the link between these influences and their underlying neurobiological substrates.
Quantifying and operationalizing resilience in Parkinson's disease
A central challenge for the field is how resilience can be robustly quantified in vivo. Up to date, several approaches have been developed to operationalize cognitive and motor reserve, each capturing distinct aspects of resilience in PD.
One approach that has gained considerable attention in PD research is the residual-based method. This approach models the expected level of clinical impairment as a function of biological disease burden, such as dopaminergic deficits (as quantified by DaT SPECT or PET), using a regression model. Individual residuals, thus the error in the prediction of the regression model, represent deviations from the predicted clinical outcome (e.g., UPDRS III score), with positive residuals indicating better-than-expected performance given the degree of pathology and negative residuals indicating worse-than-expected performance. These residuals are therefore interpreted as a proxy for resilience, capturing preserved functional capacity despite ongoing neurodegeneration. These residuals can then subsequently be related to longitudinal motor or cognitive outcomes or correlated with neurobiological measures to identify the mechanisms underlying the preserved functionality. This approach thus enables resilience to be operationalized as a continuous, individual-level construct. However, it remains dependent on the choice of predictors and underlying model assumptions, which may influence interpretability. In addition, most implementations to date have relied on clinical symptom severity rather than direct measures of motor or cognitive performance.
Only recently, more complex paradigms that challenge neural resources under increasing or varying cognitive and motor task demands have been introduced to capture resilience across neurodegenerative disorders and functional domains.13,14 These approaches are not only based on clinical symptom severity, but also consider the close interdependence of cognitive and motor processes, as motor performance in PD relies heavily on attention, executive function, and action planning. In line with this, composite measures integrating cognitive and motor reserve have been proposed. For example, a motor–cognitive reserve index derived using a semi-supervised machine learning model combined performance on a motor–cognitive stress task with wearable sensor data to quantify the ability to maintain function under increasing task difficulty and thereby predicted both cognitive and motor decline across neurodegenerative disorders. 14 These methods operationalize resilience as a task-based measure of functional reserve that complements model-based approaches such as residual analyses.
While residual-based and demand-challenging approaches provide complementary and dynamic perspectives on resilience, they do not allow direct inference about the factors that drive its development. To address this limitation, these methods need to be combined with proxy-based lifetime and lifestyle measures, such as educational attainment or physical activity, which provide insight into potential drivers and modulators of resilience.
Lifestyle factors shaping resilience in Parkinson's disease
In this context, identifying specific lifestyle and environmental factors that either impede or support the development of cognitive and motor reserve is of critical importance. Modifiable environmental risk factors, such as pesticide exposure and air pollution, or chronic may hinder the accumulation of these mitigating resources (for review see. 15 ). Although such environmental exposures clearly confer an elevated risk for developing PD, they remain modifiable and, therefore, potentially avoidable. Conversely, a growing body of evidence suggests that favorable lifetime and lifestyle factors may actively contribute to the development and maintenance of motor and cognitive reserve. To date, resilience has been associated with a range of lifestyle variables, including educational attainment, physical activity, diet, and social engagement, which together reflect lifelong enrichment.2,16 Within this article, particular emphasis is placed on education and physical activity, as the strongest evidence linking lifestyle factors to identifiable neural signatures of resilience has been reported for these domains in PD.
Nevertheless, also diet (for review see17,18 and social engagement19,20,21) have been associated with preserved or restoration of functional performance over the course of the disease. In this regard, several dietary patterns, low-fat and ketogenic diet, 22 Mediterranean diet intervention, 23 low-carbohydrate high-fat diet 24 have been associated with improvement of motor and non-motor symptoms as well as quality of life. With respect to social engagement, emerging evidence from randomized controlled trials suggests that community-based interventions, such as structured dance programs, may mitigate disease progression and support functional outcomes in PD.19,20 Importantly, these findings indicate that even later-life lifestyle modifications may still influence disease trajectories. However, the specific biological mechanisms through which diet and social engagement contribute to resilience in PD remain largely unknown.
In contrast, other lifestyle factors, particularly lifelong physical activity, are more well established as critical contributors to the development and maintenance of resilience in PD. 3 Higher levels of lifetime physical activity in PD have been associated with both slower motor and slower cognitive decline.25,26 However, given that detailed measures of physical activity are generally limited to research contexts and not systematically collected in clinical care, numerous studies have relied on education to examine cognitive and motor reserve in PD, leveraging its consistent availability in routine clinical documentation. A meta-analysis by Hindle and colleagues demonstrated that higher levels of education predicted better cognitive performance and slower cognitive decline in PD. 27 More recently, it was also shown to be associated with slower motor decline.28,29 Interestingly, individuals with higher educational attainment further exhibit more severe regional hypometabolism and general atrophy at the time of PD diagnosis compared with individuals with lower education, indicating preserved functional capacity despite ongoing neurodegeneration.30,31,32 These findings support the notion that higher educational attainment enables more effective compensation during the early stages of the disease, thereby delaying the emergence of clinically recognizable and measurable symptoms. Consequently, at the time of diagnosis, people with PD and higher education may present with a more advanced neurodegenerative pattern than their lower-educated counterparts.
Elucidating the mechanisms that enable prolonged compensation in PD requires a comprehensive understanding of when resilience is shaped across the lifespan, which lifestyle factors contribute most strongly to its development, and which neurobiological substrates underlie interindividual variability. Up to date, it remains unclear which periods are most critical for building resilience, and whether early-life enrichment, mid-life lifestyle patterns, or late-life behaviors exert the strongest effects on reserve development. Importantly, evidence from intervention studies in PD indicates that physical exercise, dietary changes or social engagement can alter disease trajectories22,23,24,33,34,35,36 and induce structural and functional brain changes,26,37 suggesting that resilience-enhancing interventions may remain beneficial even after disease onset. At the same time, it is not yet well understood which of these lifestyle factors are most relevant for building resilience, or whether specific combinations are particularly effective. Furthermore, the neurobiological mechanisms underlying these effects remain to be fully characterized, including which structural and functional brain networks are influenced by different lifestyle factors and how these changes contribute to resilience in PD. Addressing these questions ultimately depends on identifying the neurobiological substrates through which resilience manifests, as explored in the following section.
Neurobiological substrates of resilience in Parkinson's disease
Research on resilience mechanisms in PD is still emerging, and consequently only a limited number of studies have examined the neural substrates of resilience, in particular cognitive and motor reserve. Existing work has applied several complementary approaches, including (1) residual-based modeling approaches that estimate variance in clinical outcomes not explained by pathology, (2) analyses linking resilience to premorbid and current lifetime and lifestyle factors, and (3) longitudinal assessments of clinical and behavioral performance in relation to these measures.
Residual approach
Studies applying the residual approach have consistently shown that higher motor reserve (i.e., negative residuals) is associated with stronger regional functional connectivity, 38 preserved white matter integrity,39,40 greater regional grey matter volume, 12 slower motor deterioration, 41 lower non-motor dysfunction, 42 and reduced risk of dyskinesia. 41 Individuals with high baseline motor reserve also demonstrate lower risk of dementia and better postural stability. 42 Notably, recent work suggests that it may take up to seven years for individuals with high motor reserve (i.e., negative baseline residuals) to converge on the motor trajectory of individuals with low reserve. 12 Moreover, recent evidence indicates that higher motor reserve in the early stages of PD predicts more favorable long-term outcomes, with adequate treatment and regular physical activity supporting the maintenance of motor reserve over time. 43 While these studies provide partial insights into potential neurobiological underpinnings of resilience, this approach has three major drawbacks: (1) it is based on the error in the model (i.e., residuals), which may be influenced by incomplete or poor surrogates (i.e., predictors) and small sample sizes; (2) it relies on regression models fitted within the study sample, rather than on normative reference data from large, independent cohorts, which may introduce sample-specific bias and limit comparability across studies; (3) it does not allow to infer which factors (e.g., lifestyle) actually contributed to the observed variance. Thus, it remains unknown how the observed protective neurobiological mechanisms can be promoted by modifiable factors and whether it truly reflects resilience and not just differences in the disease stage.
Lifestyle associations
Circumventing the drawbacks of the residual approach, a few studies have focussed on combining lifetime and lifestyle factors with functional network-based analyses. One study reported that both cognitive reserve (indexed by premorbid intelligence, which was based on composite information on former lifestyle such as occupation, reading, writing, language skills, musical abilities, etc.) and brain reserve (whole-brain grey matter volume) were positively associated with the relative increase in network integration observed in the dopaminergic OFF state. 44 A shift in network topology toward the frontal cortex, insula, thalamus, and amygdala following dopamine withdrawal was linked to higher resilience. The results of this study imply that premorbid intelligence, shaped by previous lifestyle, may exert broad, system-level effects on network integrity that help preserve motor function despite dopaminergic loss.
Additional support for network-level resilience comes from recent neuroimaging studies demonstrating that greater topological robustness of certain networks, assessed using an attack-analysis framework, was associated with preserved cognitive and motor function in PD.45,46 The network attack tolerance approach is used to test the robustness of brain networks to targeted damage. In this method, brain regions (nodes) are sequentially removed from the network in order of their connectivity, starting with the most highly connected regions (hubs). After each removal, network efficiency is recalculated to quantify how effectively information can still be exchanged across the remaining network. A rapid decline in network efficiency following the removal of highly connected nodes indicates a fragile network that is strongly dependent on a small number of regions (hubs), whereas a more gradual decline suggests greater network robustness and an enhanced capacity to maintain communication despite targeted disruptions. In the context of neurodegenerative diseases, such as PD, this approach provides insight into how disease-related damage to key brain regions, e.g., the putamen, may compromise large-scale network organization and functional integration. It was recently shown by a longitudinal study that people with PD without cognitive decline over time exhibited higher network attack tolerance in the fronto-parietal network. 45 Building on this, we found that lifetime physical activity moderated the relationship between global motor performance and somatomotor network attack tolerance, suggesting that resilience mechanisms supporting motor outcomes may similarly depend on network robustness. 46 Higher robustness of these networks towards attacks through progressing pathology may provide a mechanism of compensating the disease up to a certain threshold. Whether such network robustness can be facilitated through interventions such as transcranial magnetic stimulation (TMS) remains to be tested.
In terms of lifestyle factors contributing to the maintenance of neural resources, a recent longitudinal study reported that higher levels of sustained physical activity were linked to slower rates of neurodegeneration, suggesting that exercise may have the potential to preserve brain structure even in the presence of ongoing pathological processes. 26 Complementing these findings, habitual exercisers with PD were shown to exhibit increased ventral striatal activity during a reward-based task compared with sedentary people with PD. 47 Importantly, this heightened activity correlated with better cognitive performance, pointing to a potential role of the ventral striatum in supporting cognitive reserve in the context of progressive dopamine depletion. Moreover, it was shown that higher educational attainment was associated with preserved structural integrity of the basal ganglia and dorsolateral-prefrontal cortex 48 and fewer white matter hyperintensities, implicating lifelong cognitive enrichment as a factor that supports white matter substrate and thus cognitive reserve. 49
Together, despite the still limited number of neuroimaging studies on resilience in PD, these findings underscore the capacity of certain lifetime and lifestyle factors to support both motor and cognitive reserve in PD and highlight how enhanced network connectivity, integration, and robustness consistently emerge as key features underpinning resilience to neurodegeneration in PD.
Future directions in resilience research in PD
With the current advancements in the field of resilience research in PD, several key question remain to be addressed:
First, despite growing interest in the timing of lifestyle adaptations, the relevance of lifestyle exposures during the prodromal phase of PD, such as in REM sleep behavioral disorder remains poorly understood. Many lifestyle-related factors that contribute to motor and cognitive reserve accumulate over decades, raising the possibility that resilience is already shaped during prodromal stages, when non-motor symptoms, such as hyposmia, constipation, sleep disturbances, and subtle cognitive changes, may precede clinical diagnosis by several years. Importantly, resilience-related neural signatures are unlikely to be static; instead, they may evolve as the disease transitions from prodromal to clinically manifest PD, reflecting changing demands on compensatory and reserve mechanisms across disease stages. 50
Beyond questions of timing, the specific neurobiological pathways through which lifestyle factors confer resilience remain to be fully elucidated. Converging evidence suggests that sustained engagement in healthy behaviors may promote neuroplasticity through mechanisms such as increased brain-derived neurotrophic factor (BDNF) expression (for review see. 51 Moreover, given that lifestyle and environmental factors are known to substantially influence the epigenome, studies focusing on gene–environment interactions may provide further insight into the biological mechanisms underlying resilience.52,53 Epigenomic studies offer a powerful framework for understanding resilience by capturing how lifestyle and environmental exposures are biologically embedded and exert lasting effects on gene regulation without altering DNA sequence. By identifying epigenetic signatures associated with certain neural signatures and preserved motor and cognitive function despite comparable neurodegeneration, such studies may help explain interindividual differences in resilience and clarify how modifiable behaviors exert durable protective effects on neural systems. 52 Another advantage of epigenetic approaches is their ability to capture the cumulative biological impact of multiple lifestyle behaviors over time. 53 This integrative readout may thus facilitate the assessment of interrelated lifestyle factors, such as sleep quality, mental health, and cognitive stimulation, within a unified framework, reflecting their combined and interactive contributions to resilience. Ultimately, these mechanistic insights may provide a rationale for translating resilience research into clinical interventions.
Indeed, recent clinical trials have begun to evaluate whether targeted lifestyle adaptation can actively enhance resilience and modify disease progression in PD. The SENSS trial (NCT06669455) in the Netherlands investigates an integrated and personalized lifestyle intervention combining physical activity, nutrition, sleep, and stress management to improve quality of life in individuals with PD. The LifePD study (NCT06603012) in the United States focuses on behavioral strategies to increase and sustain physical activity in people with PD. Similarly, the SPARX-3 study (NCT04284436), evaluates the efficacy of high-intensity endurance exercise as first-line therapy for individuals diagnosed with PD within 3 years. Moving to a remotely administered smartphone intervention, the SlowSpeed study (NCT06993142) investigates the feasibility of an app-based intervention aimed to increase physical activity in daily life in individuals with LRRK mutation. Together, these trials exemplify a growing translational effort to determine how modifiable behaviors in several domains can be optimally leveraged to enhance resilience, both before substantial neurodegeneration has occurred and across later disease stages.
Notably, future advances in resilience research in PD may further provide important insights into both shared and disease-specific mechanisms across neurodegenerative disorders, particularly in comparison with AD. This perspective is especially relevant given that PD is frequently characterized by mixed pathologies (for review see. 54 ) In this context, certain resilience signatures, which still need to be determined, may represent common mechanisms across diseases rather than disorder-specific phenomena. Supporting this notion, higher cognitive reserve, indexed using residual-based approach relating pathology to cognitive performance, has been associated with distinct gene expression profiles (including ENC1 and UNC5C) across individuals with AD, Lewy body dementia, and PD, pointing toward partially shared molecular underpinnings of resilience. 55
Despite shared mechanisms, it must be noted that AD and PD nonetheless present differences in resilience resources given that the needs for functional compensation may potentially differ. Indeed, individuals with AD and higher resilience consistently present more severe and wide-spread pathology56,57,58 and a steeper decline post diagnosis19,20,21 in comparison to AD individuals with lower resilience levels. In contrast, individuals with PD and higher resilience levels, approximated by education 59 or premorbid physical activity,46,60 do not show evidence of more severe dopaminergic terminal loss at comparable levels of motor impairment and present a slower motor decline over time in comparison to individuals with lower resilience levels.12,25,42,41 These different observations may be linked to differences in functional disease trajectories and may reflect a combination of factors, including the temporal dissociation between pathology and neurodegeneration, differences in network topology, and the extent to which compensatory mechanisms can be sustained across distributed neural systems. A deeper understanding of how resilience modulates functional trajectories across disorders is therefore critical and requires longitudinal designs across disorders.
Finally, the recent work on resilience and motor decline in PD emphasizes that prior lifestyle factors and demographic characteristics substantially shape disease trajectories.12,42,41 Recognizing these sources of interindividual variability is crucial for enhancing the accuracy of staging models, strengthening prognostic predictions, and eventually informing personalized approaches to disease management. Whereas AD has benefitted for several years from a biologically anchored staging framework, which also accommodates clinical heterogeneity and incorporates resilience,61,62 an equivalent biological framework for PD had been lacking since only recently. In 2024, two biological staging systems were proposed for PD and related Lewy body disorders, the Neuronal α-Synuclein Disease Integrated Staging System (NSD-ISS) 63 and the broader SyNeurGe 64 framework, both aiming to classify PD according to pathobiological processes rather than clinical milestones alone. Although differing in scope and level of detail, both models recognize the extensive clinical heterogeneity in PD that cannot be fully explained by α-synuclein accumulation or dopaminergic dysfunction. This variability underscores an important conceptual gap: neither framework currently incorporates resilience-related modifiers, such as cognitive or motor reserve, despite growing evidence that these factors influence symptom onset, longitudinal progression, and functional outcomes. Incorporating resilience into PD staging systems would likely help explain why individuals with comparable biological disease stages show markedly different phenotypes and rates of transition, and thus refine prognostic accuracy in preclinical stages, and improve stratification in early-intervention trials. As the NSD-ISS and SyNeurGe systems continue to evolve, embedding resilience within these biological classifications may overall represent a necessary and promising step toward a more individualized, mechanistically informed understanding of PD trajectories.
Conclusion
Overall, future research on resilience mechanisms, and in particular motor reserve, in PD is poised to deepen our understanding of why individuals with similar degrees of neurodegeneration exhibit differing motor symptoms and disease progression. A more complete understanding of shared and distinct resilience mechanisms, including motor, cognitive, and brain reserve, will require study designs that intentionally span different neurodegenerative disorders (e.g., AD and PD), disease subtypes (such as body-first vs. brain-first presentations), lifestyle profiles (from sedentary to highly active individuals), and disease stages ranging from prodromal to clinically manifest. 3 Advances in neuroimaging, electrophysiology, and computational modeling are expected to help identify the neural substrates that underlie resilience. Longitudinal studies integrating multimodal data, including structural and functional connectivity, genetics, and lifestyle factors, will be crucial to map how resilience evolves across disease stages. Emerging tools such as machine learning and wearable technology may allow for personalized tracking of motor performance and reserve-related adaptations in real-world contexts. Moreover, the exploration of interventions aimed at enhancing motor reserve, such as targeted physical exercise, cognitive training, and neuromodulation, could open new therapeutic avenues. Ultimately, integrating resilience levels into PD management represents a step toward precision medicine, where rehabilitation and pharmacological therapies are tailored not only to pathology, but also to the brain's capacity for compensation and resilience.
Take home messages
Accounting for resilience may help to explain why patients with similar pathology burden experience markedly different motor and cognitive outcomes in PD
Resilience-based mechanisms are built up over the long term and thereby shape neural mechanisms that mitigate the impact of ongoing neurodegeneration
Modifiable lifestyle factors, such as physical activity, diet, and cognitive enrichment, represent promising targets to support motor and cognitive reserve in PD
Incorporating resilience into PD staging and management frameworks may enable more accurate prognosis and personalized intervention strategies
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – Project-ID 431549029 – SFB 1451 and JPND research – project 2024-280 TRACE-PD.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.