
Abstract
Background
Tremor is reported by people with Parkinson's disease (PwP) as being one of the most troublesome symptoms.
Objective
To characterize the PwP experience of tremor.
Methods
An internet-based survey of PwP living with tremor was conducted in the US, from September 2023 to March 2024.
Results
Survey responses from 634 respondents (PwP = 599; care partner = 35) were analyzed. Most (93%) PwP had tremor in their upper extremities and of these, 59% reported ≥2 tremor subtypes (rest/postural/kinetic). Overall, 24% reported little or no effect of medication and a further 25% reported that medication only somewhat improved their tremor. At least mild functional impairment due to tremor was reported by 65% of PwP and most indicated that ≥1 daily activity (83%), sensory experience (77%), or psychosocial function (92%) was impacted. Multinomial logistic regression analyses revealed that the odds [95%CI] of reporting severe functional impairment due to tremor (vs. slight) were increased by worse tremor in the dominant hand (4.9 [1.36, 17.72]); presence of OFF-time (4.7 [1.22, 18.30]), number of body parts affected (2.0 [1.45, 2.88]) and lack of medication effect (1.6 [0.30, 8.22]). The presence of all three tremor subtypes was associated with increased odds of being “very dissatisfied” with quality of life (21.5 [2.51, 183.44]).
Conclusions
Results from this survey demonstrate that tremor in PD is often more than a rest tremor and frequently impacts function and activities of daily living. Medication response is inadequate in about half of cases, highlighting that effective treatment of tremor is an important unmet need.
Plain language summary
Tremor is one of the most common symptoms of Parkinson's disease. Until now, there has not been much research done to understand, from the patient's perspective, how living with tremor impacts their ability to do simple things and their overall quality of life. In this survey study, 634 people living with Parkinson's tremor were invited to complete an online questionnaire that explored these issues in depth.
Survey highlights include:
While rest tremor (tremor with the arm relaxed) is common, most people live with at least two out three upper limb tremor subtypes, including rest tremor, postural tremor (when the arm is held outstretched) and kinetic tremor (when the arm is moving) Current Parkinson's medication often fail to control tremor Respondents commonly reported that their tremor interferes with tasks such as handwriting and using everyday technology (smartphones, computers, keyboards, etc.) and that it causes discomfort and fatigue in the affected body part Most respondents said that they try to hide their tremor, that it makes them self-conscious, and that they worry about the perception of others.
Greater awareness of the full impacts of tremor on daily life should lead to better informed patient–doctor discussions and foster development of more effective treatments.
Introduction
Tremor is one of the most prominent and visible features of Parkinson's disease (PD) and is often the first symptom noticed. 1 It is estimated that about 75% of people with PD (PwP) experience tremor at some point during their disease course.2,3 There are currently no pharmacotherapies specifically approved for treatment of tremor in PD. Dopaminergic therapies (e.g., levodopa/carbidopa) are considered the gold standard treatment for motor symptoms; however, tremor response to these and other PD medications is highly variable, and tremor often remains inadequately controlled at tolerable doses. 4 When described as a ‘cardinal’ symptom, tremor in PD usually refers to an asymmetric resting tremor of 4–6 Hz in the fully resting limb, which is suppressed during movement initiation. 5 Nonetheless, a majority of PwP also experience action tremors,3,6 including postural and kinetic tremors.7,8
The presence of tremor is known to impair several physical and psychological quality of life (QoL) domains in PwP, 9 including personal and social relationships, self-image, and overall sense of well-being. 10 It is one of the few symptoms that is consistently ranked amongst the most troublesome across the disease, from early- to advanced-stage PD.11–13 However, despite its known impact on broad QoL domains, there is little in-depth information about its impact on daily life and how its presence relates to functional impairment and QoL. This survey was designed to understand the perceptions and experiences of tremor from the perspective of a large sample of PwP living with tremor.
Methods
Survey design
The structure and contents of the Parkinson's Disease Tremor Survey was initially drafted by a movement disorder expert clinician (RAH) and then revised in collaboration with the other authors and the national, not-for-profit organization, Parkinson and Movement Disorders Alliance (PMD Alliance). The protocol and a draft survey were submitted to the Institutional Review Board (IRB) of the University of South Florida and the IRB determined that the protocol met criteria for exemption from IRB review. Researchers did not have access to any identifiable information about the survey respondents. During a pilot pretesting stage, PwP volunteers (n = 9, mean age 66.7 years, mean time since PD diagnosis 7.7 years, 55.6% female) recruited from the PMD Alliance completed the draft survey online to provide feedback to the study team regarding aspects of the survey, including website functionality, understandability of survey items, response item-friendliness, time required for completion, and content. The draft survey was then revised into a final survey based on this feedback; these initial PwP responses were not included in the final results.
The survey was conducted online (hosted by Survey Monkey), in English, between September 11, 2023, and March 8, 2024. The survey is presented in full as Supplemental Material. It includes six main categories (demographics, tremor characteristics, functional impact, sensory and psychosocial impact, QoL, and medication response) and consists of approximately 46 questions referring to the respondent's experience of tremor over the prior week. Questions were multiple-choice and two of the medication-based questions included a free entry option. The single QoL question was based on the Kemp Quality of Life Scale, which is validated for adults living with impairments. 13 To submit responses, respondents were required to complete the entire survey and then click “finish” at the end. The survey was designed to take approximately 20–30 min to complete, however, there was no set time limit for completion and participants could take breaks during survey completion.
Survey participants
Eligible respondents were adults (aged ≥18 years), who were either diagnosed with PD (PwP) and experiencing tremor or a care partner of a PwP. Care partners were instructed to answer the survey from the perspective of their respective PwP. Survey instructions also indicated that there should only be one survey completed per PwP.
Invitations to complete the survey were sent to the email lists of the PMD Alliance and the University of South Florida (USF) Parkinson's Disease and Movement Disorders Center and were also posted on their websites. Additional national awareness was provided by online media coverage.14,15
Data analysis
No formal sample size calculations were performed for this cross-sectional survey. Descriptive statistics were used to summarize all survey data collected with no imputation for missing responses. Data for PwP and care partner responses were combined.
Statistical analyses were conducted to evaluate the relationships between individual demographic or tremor characteristics and ratings of functional impairment due to tremor as well as overall QoL. These associations were assessed using Chi-square or Fisher Exact tests for categorical variables (e.g., prior history of essential tremor (ET), rest tremor only) and the Kruskal-Wallis test for continuous variables (e.g., age, time since tremor onset). The effect of demographic and tremor characteristics on ratings of functional impairment due to tremor and on dissatisfaction (“dissatisfied” and “very dissatisfied”) with QoL were further assessed using multinomial logistic regression. The variables selected for inclusion in the two models were those that had a statistically significant impact during their respective individual tests; however, some of these variables were excluded due to multicollinearity. For the functional impairment due to tremor model, the category “slight” (as the highest frequency), and for the model of dissatisfaction with QoL the category “satisfied” (as the highest frequency) were used as references. The results are reported in the form of odds ratio (OR) [95% confidence interval].
Statistical analyses were generated using SAS version 9.4 (SAS Institute, Inc. Cary, NC). All statistical tests were two-tailed with statistical significance set at p-value ≤ .05.
Results
Sample characteristics
Six-hundred and sixty-seven respondents completed the survey and submitted results. Of these, 634 indicated that they (n = 599), or the person for whom they were responding as a care partner (n = 35), had PD and had tremor. Responses from these 634 individuals are reported here and are henceforth referred to as PwP. The mean age [range] of PwP at the time of the survey was 70 [33–96] years; 50% were female and most (94%) were white. PwP had a mean time (range) since PD diagnosis of 5.8 [1–25] years and mean time since onset of tremor of 7.2 [1–55] years (Supplemental Table 1). Almost a quarter (23%) reported a prior diagnosis of ET. Overall, 85% of PwP were right hand dominant, 12% were left hand dominant, and 3% were ambidextrous.
Clinical characteristics of tremor
On average (range), PwP reported that they experienced tremor 45% (2.5–100%) of their daily waking hours (7 [0.5–19] hours/day). As shown in Figure 1, the upper extremities were most commonly affected (left and right combined: 93%), followed by lower extremities (left and right combined: 44%), jaw (15%) and lips (10%). The presence of tremor was less common in the head, face, tongue, and torso. Regarding upper extremity tremor, 84% reported rest tremor, 59% reported kinetic tremor, and 45% reported postural tremor. Combinations of upper limb tremor subtypes were commonly reported with 59% of PwP reporting ≥2 upper limb tremor subtypes and 28% reporting all 3 tremor subtypes. In contrast, 29% reported rest tremor only, 10% reported kinetic tremor only, and 1% reported postural tremor only.
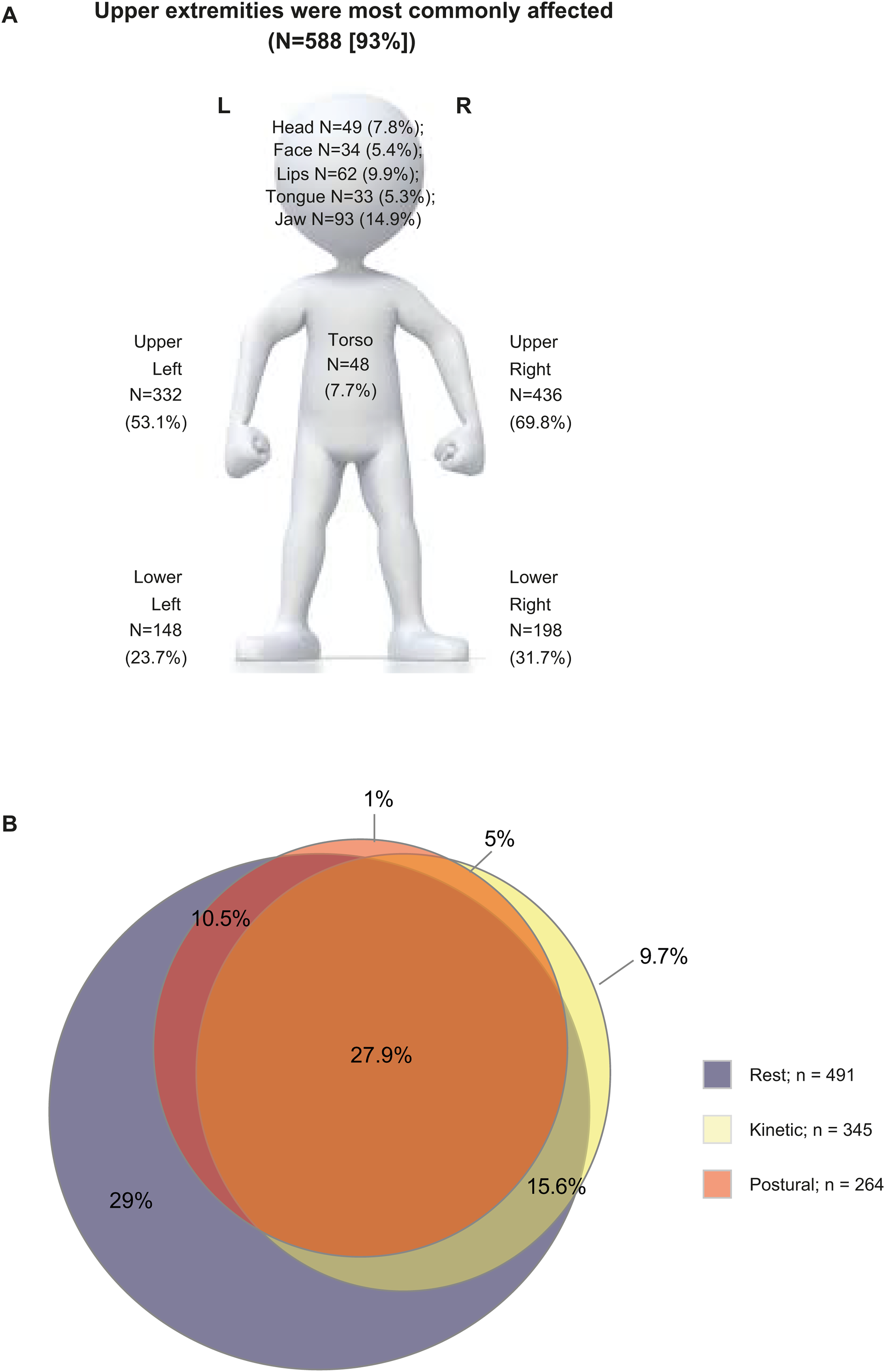
Anatomic location of tremor and upper limb tremor subtypes of the survey population. The survey provided lay-friendly descriptions of upper limb tremor subtypes as follows: Rest tremor: tremor when hands/arms were “laying in my lap or hanging by my side while walking”; Postural tremor: tremor “while I was holding my hands/arms outstretched in front of me”; Kinetic tremor: tremor while “actively moving or using my hands/arms such as when bringing a fork to my mouth or during handwriting”.
More than half (55%) of PwP with upper limb tremor (n = 588) reported that their tremor was worse on their dominant side, 35% reported that their tremor was worse on their non-dominant side, 3% reported being ambidextrous and reported tremor was worse on one side, while 8% reported that their tremor was about equal on both sides irrespective of their hand dominance. Reported amplitudes of rest, postural and kinetic tremor in the most and least affected hand/arm are displayed in Supplemental Figure 1.
Tremor response to treatment
A majority (56%) of PwP reported currently being on monotherapy, while 22% were taking two, 11% were taking three, and 5% were taking four or more PD medications. The most common PD medication class was oral levodopa (88%, including 59% on levodopa monotherapy; Table 1). Overall responses to PD medications were variable, with 12% reporting that medications had no effect on their tremor, 12% reporting that medications slightly improved their tremor, 25% reporting that medications somewhat improved their tremor, 30% reporting that medications greatly improved their tremor, and 15% reporting that medications complete resolved their tremor (Figure 2(a)).
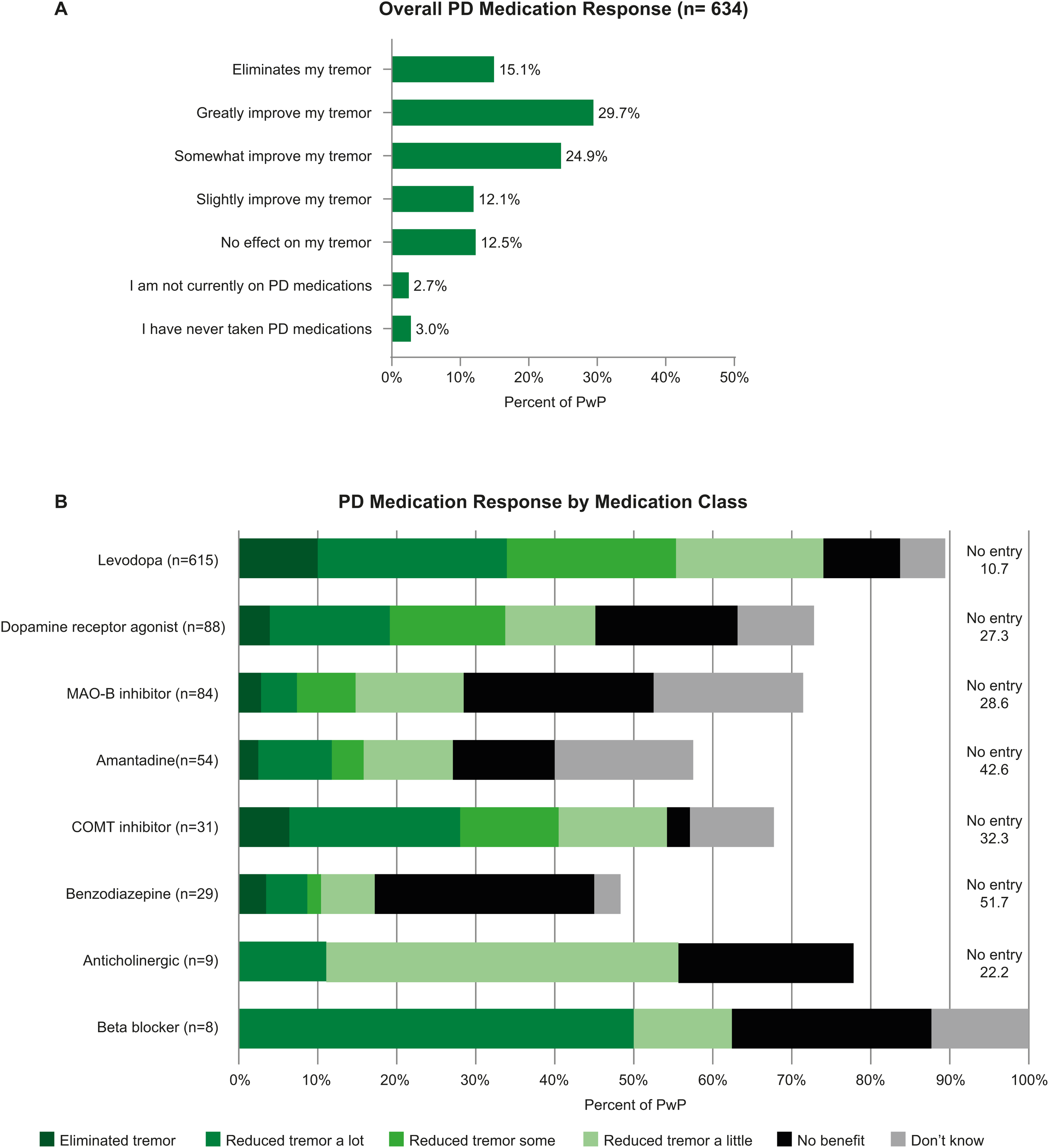
Tremor response to medication (a) overall (b) by medication category. PwP could take more than one medication within a medication class (e.g., Rytary and Sinemet). Their responses for all medications within the class were included. As a result, a PwP could contribute more than one response to a medication class. PwP could also choose multiple response categories for a single medication. In these cases, their responses were divided by the number of categories (n) selected (1/n). For example, if they selected 2 response categories (eliminated tremor, and reduced tremor some) for a single medication their response contributed 0.5 to each category.
Parkinson's disease medications.
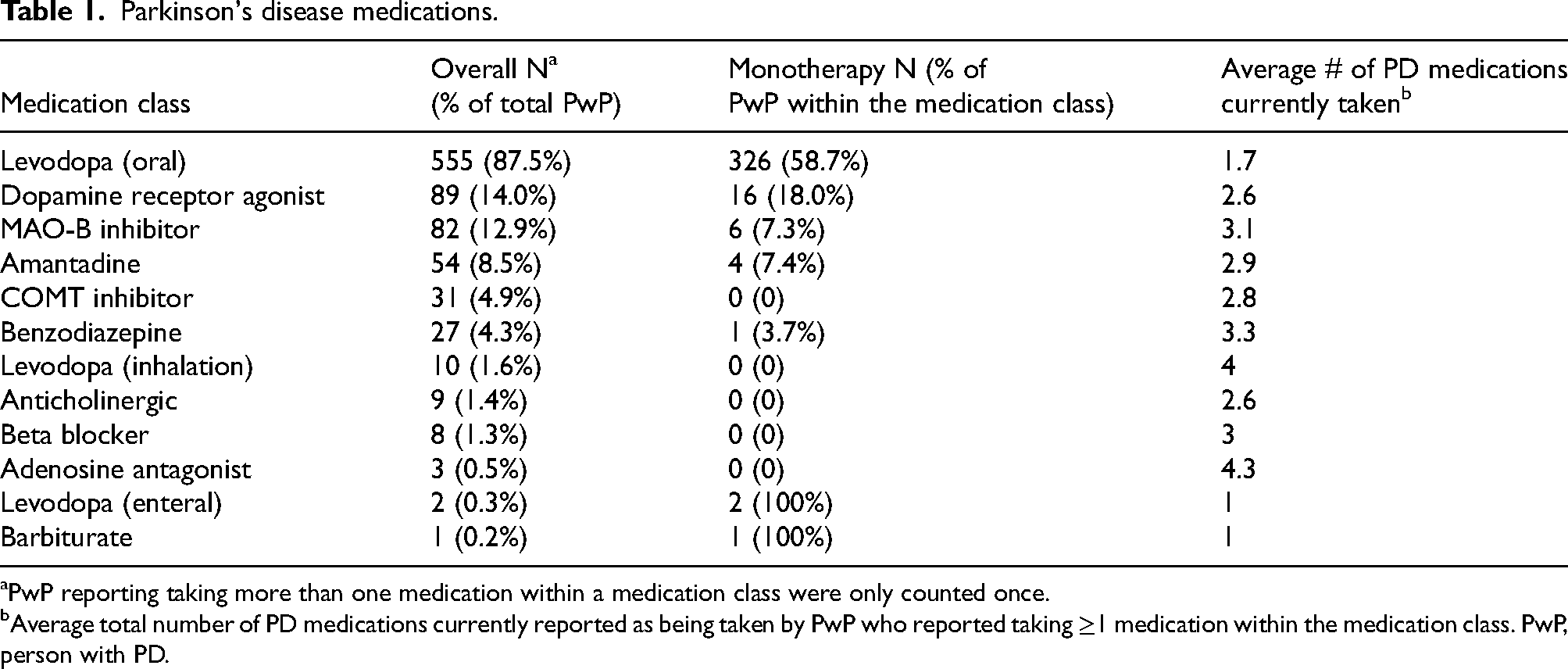
PwP reporting taking more than one medication within a medication class were only counted once.
Average total number of PD medications currently reported as being taken by PwP who reported taking ≥1 medication within the medication class. PwP, person with PD.
Figure 2(b) shows tremor response to PD medications broken down by medication class. The majority of PwP reported taking at least 1 medication from the levodopa class (and many taking more than 1 medication from this class). As a result, there were 615 responses for oral levodopa medications currently in use. Of these 615 responses, 34% indicated that oral levodopa eliminated or reduced tremor a lot, 21% indicated that oral levodopa reduced tremor some, and 28% indicated that oral levodopa reduced tremor a little or provided no benefit. The next most common medication classes were dopamine receptor agonists (n = 88), and MAO-B inhibitors (n = 84). Compared to the levodopa medication class, a smaller percentage of PwP reported that dopamine receptor agonists and MAO-B inhibitors eliminated or reduced their tremor a lot (22% and 9% respectively).
Over half (52%) of PwP reported they experience motor fluctuations, while 38% reported a stable response to medications throughout the day, and 11% were unsure if they were experiencing motor fluctuations. Of those reporting motor fluctuations (n = 329), 17% reported that their tremor was “very much worse”, 42% reported that their tremor was “much worse “, and 35% reported that their tremor was “slightly worse” when they were OFF. Only 5% reported that their tremor was not impacted by their OFF/ON status.
PwP were also asked about their experience with surgical treatments for PD. Specifically, 33 PwP (5%) reported they had undergone deep brain stimulation (DBS; subthalamic stimulation, n = 14, internal pallidum stimulation, n = 3, and unknown n = 16). In most cases (n = 30), tremor was reported to be among the main reasons for the procedure. The reported effects of DBS on tremor were: “Eliminated tremor completely” (n = 3), “Reduced tremor a lot” (n = 21), “Reduced tremor some” (n = 7), “No benefit” (n = 1), and “I no longer use my DBS” (n = 1). Only two PwP reported having undergone MRI-guided focused ultrasound.
Impacts of tremor
Most PwP (65%) said their tremor caused at least mild overall functional impairment over the past week, while 33% indicated that tremor did not have an overall impact on their function (Figure 3(a)). When asked about individual experiences, most indicated that ≥1 daily activity (83%), sensory experience (77%), or psychosocial function (92%) was impacted by their tremor. In terms of specific daily activities, tremor was most commonly reported to interfere (“some”, “quite a lot”, or “a great deal”) with handwriting (60%), using a keyboard (52%), or using a smartphone or tablet (47%). One in three PwP reported that tremor affected their ability to work (33%) or caused disrupted sleep (30%) (Figure 3(b)). Regarding sensory experiences, 62% of PwP endorsed that the tremor itself felt uncomfortable, and 48% reported fatigue in the affected body part (Figure 3(c)). Psychosocial impacts included 88% of PwP reporting that they disliked having tremor, 73% reporting that tremor reminded them of their illness, and ≥50% reporting that tremor made them feel self-conscious, that they tried to hide their tremor, that they were concerned about how they were perceived by others, and that tremor interfered with their ability to enjoy themselves (Figure 3(d)).
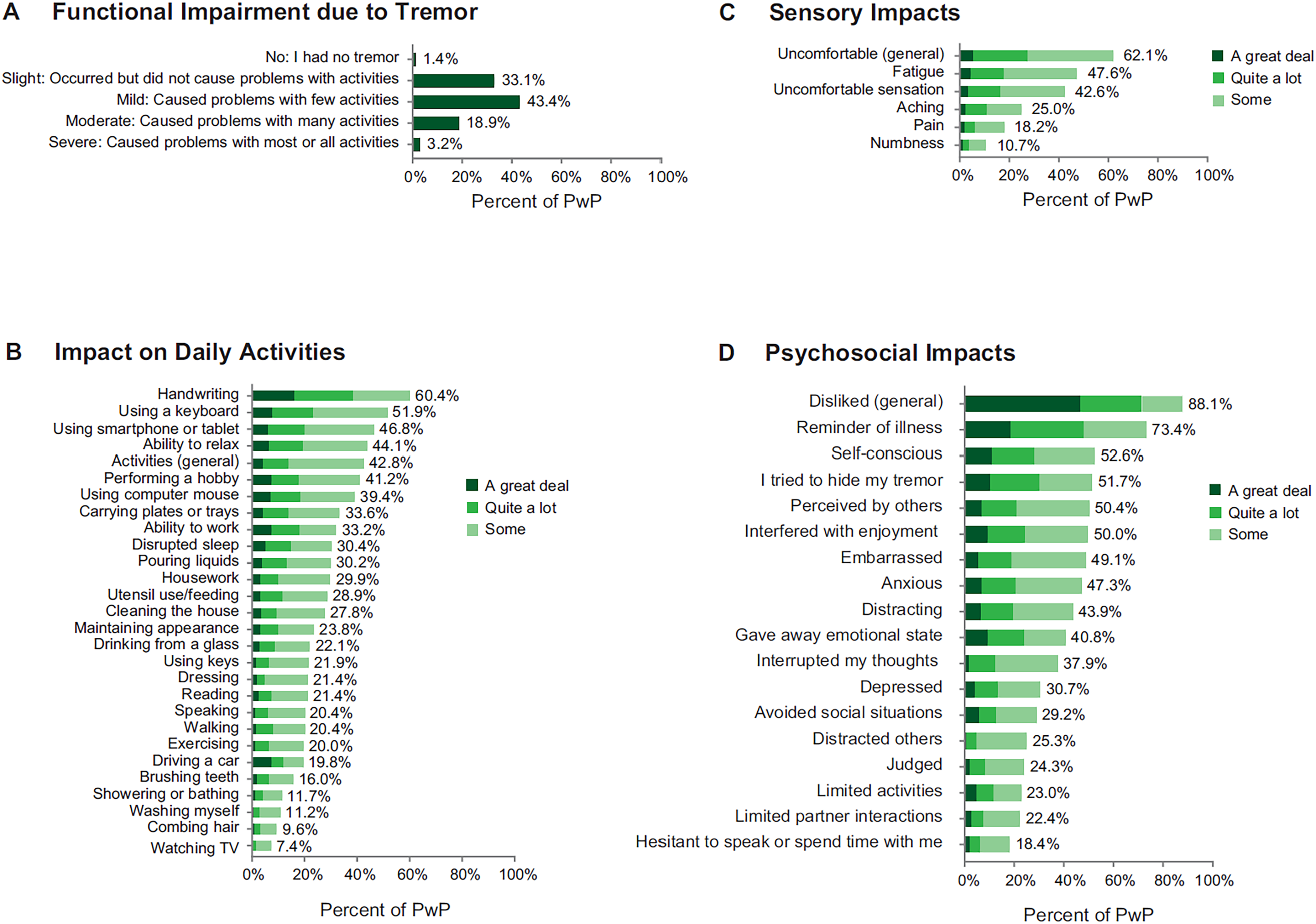
Impacts of tremor: (a) functional impairment, (b) impact on daily activities (c) sensory impacts, and (d) psychosocial impacts. All responses were reported based on experiences over the past week. For B-D, the % value provided represents the total for response categories “some”, “quite a lot”, and “a great deal”.
Variables associated with ratings of functional impairment and overall QoL due to tremor
Table 2 presents factors significantly associated with functional impairment and QoL in the multinomial logistic regression analyses (results for the individual comparisons are shown in Supplemental Table 2). The odds of a respondent reporting severe functional impairment (when compared to the reference of slight) was almost five times higher if their tremor was worse in the dominant hand (OR: 4.9 [1.36 to 17.72]) and was 1.6 times higher if they reported a lack of medication effect on their tremor (OR: 1.6 [0.30 to 8.22]). Additionally, the odds of reporting severe functional impairment were increased by the presence of OFF time (Severe: 4.7 [1.22 to 18.30]; Moderate: 3.0 [1.45 to 6.06]; Mild: 2.3 [1.40 to 3.92]) and the number of body parts affected (Severe: 2.0 [1.45 to 2.88]; Moderate: 1.6 [1.26 to 2.08]; Mild: 1.3 [1.06 to 1.64]). The odds of having a moderate impact on function was predicted by the percent of hours awake with tremor (OR: 1.0 [1.01 to 1.03]); and presence of all three upper limb tremor subtypes (OR: 3.0 [1.46 to 6.29]). In contrast, the odds of reporting higher levels of functional impairment due to tremor were significantly reduced by two characteristics. Specifically, reporting that medications greatly improved tremor reduced the odds of reporting severe functional impairment (OR: 0.03 [0.002 to 0.380]) and reporting only having rest tremor decreased the odds of reporting moderate and mild impairment when compared to slight impairment (Moderate: 0.4 [0.18 to 0.93]; Mild: 0.5 [0.31 to 0.90]).
Tremor variables significantly associated on multinomial analysis with functional impairment due to tremor and dissatisfaction with QoL.
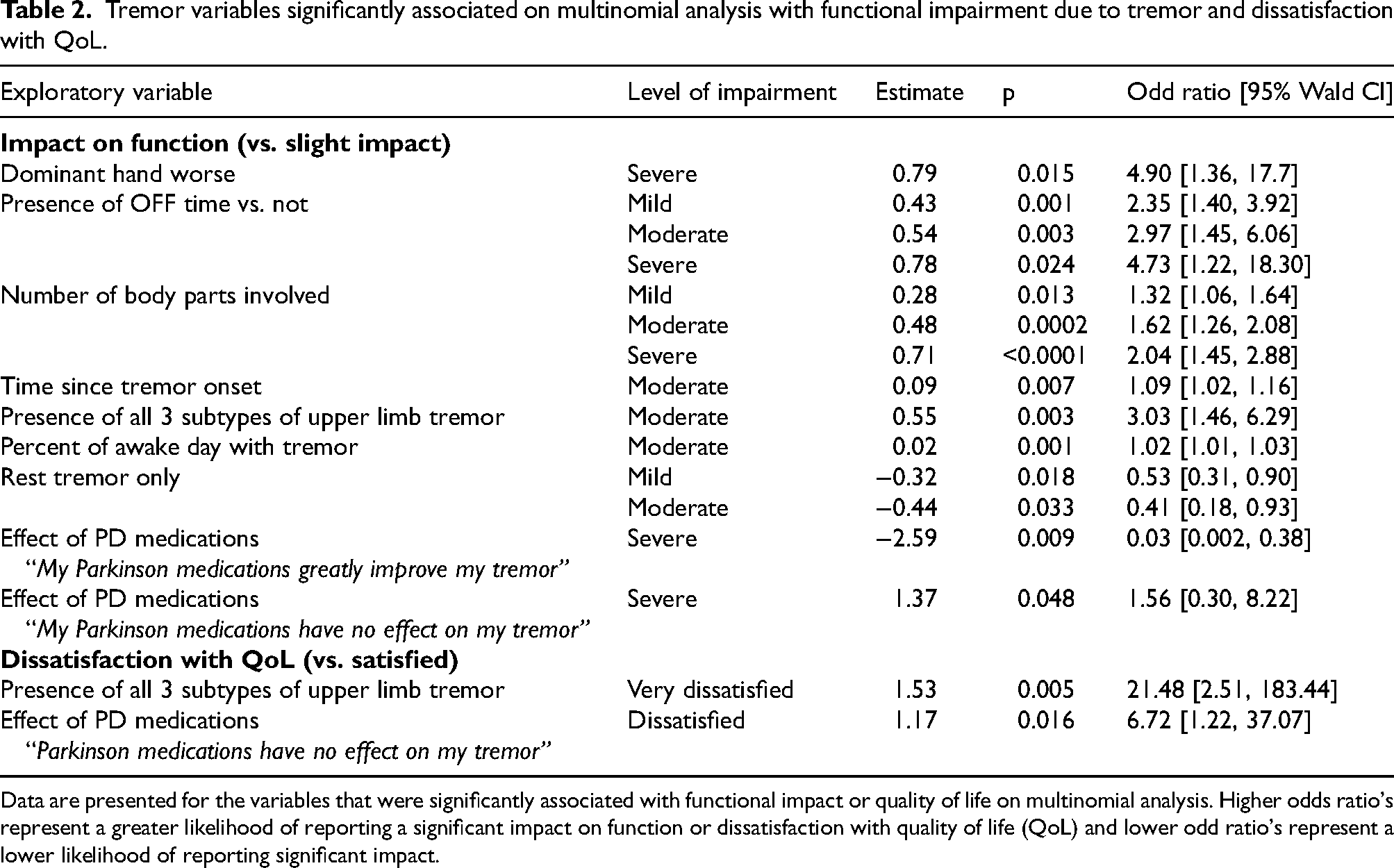
Data are presented for the variables that were significantly associated with functional impact or quality of life on multinomial analysis. Higher odds ratio's represent a greater likelihood of reporting a significant impact on function or dissatisfaction with quality of life (QoL) and lower odd ratio's represent a lower likelihood of reporting significant impact.
In the multinomial regression model of overall QoL ratings, the presence of all three upper limb tremor subtypes increased odds of reporting being “very dissatisfied” by more than 20-fold (OR: 21.5 [2.52 to 183.44) and lack of PD medication effect was associated with increased odds of reporting being “dissatisfied” (OR: 6.7 [1.22 to 37.07]).
Domains of greatest impact
PwP were asked to rank three possible responses from most bothersome to least bothersome to indicate the biggest way in which tremor impacts them. Out of 625 responses, “I don’t like the way tremor interferes with my function” was ranked number one by 50%, “I don’t like the way tremor feels” was ranked number one by 33%, and “I don’t like the way tremor makes me look” was ranked number one by 18%.
Most PwP (80%) noted that that a medication that effectively treats tremor would be personally valuable (“quite a lot” or “a great deal”) and 94% indicated that such a medication would be valuable to the PD community.
Discussion
To our knowledge, this is the largest and most in-depth survey to date examining the PwP experience of tremor and its impacts on function and QoL. Key findings from the survey were:
PD tremor is not just a rest tremor. Less than a third of PwP reported they only had rest tremor, while 59% reported ≥2 upper limb tremor subtypes. Medications commonly fail to adequately ameliorate PD tremor. Almost a quarter of PwP reported that medication had no effect (12%) or only slightly improved (12%) their tremor while another 25% reported that medication only somewhat improved their tremor. PD tremor commonly interfered with activities of daily living. Most PwP reported that their tremor interfered with many common activities of daily living including handwriting and using everyday technology such as a keyboard, smartphone and computer mouse. PD tremor is commonly associated with negative sensory experiences. Three in five PwP indicated that the tremor itself felt uncomfortable and almost half reported fatigue in the affected body part. PD tremor is commonly associated with substantial psychosocial burden. Overall, 88% of PwP reported that they disliked having tremor, 73% reported that tremor reminded them of their illness, and ≥50% reported that tremor made them feel self-conscious, that they tried to hide their tremor, that they were concerned about how they were perceived by others, and that tremor interfered with their ability to enjoy themselves.
The results of our survey provide insight with respect to the perceptions of the PwP population living with tremor and includes patients with a broad range of disease duration and severity. While cross-sectional, our data align with recent longitudinal data from the Parkinson Progressive Markers Initiative (PPMI; and others) which also indicate that multiple tremor subtypes are common in PD. 8 In the PPMI study, the proportion of PwP with all 3 tremor subtypes increased from 27.5% at diagnosis to 41.5% by 7 years and tremor severity scores (rest, postural and kinetic) significantly worsened over time. 8 Also in line with the PPMI study, 16 the results of our survey highlight the variability of tremor response to current antiparkinsonian medications, with results suggesting that medication response may be inadequate in about half of all cases. A levodopa challenge study in PwP with tremor showed that the resting tremor response (but not bradykinesia) did not follow a normal distribution but instead could be clustered into dopamine-responsive, intermediate, and dopamine-resistant tremor categories. 16 The granularity of PD medication data provided in this survey was a key strength as it allowed assessment of the effects of different medication classes and included questions about the impact of motor fluctuations on tremor.
The results of this study show that patients don’t experience tremor as merely a nuisance and instead report that it affects function, activities of daily living, and QoL. Its presence not only imposes physical but also psychosocial burdens. Altered self-perception was a common theme throughout the questionnaire with ≥50% of PwP reporting that tremor made them feel self-conscious and that they were concerned about how they were perceived by others.
To our knowledge, this survey is the first to assess whether tremor was worse in the dominant hand and how this affects daily function. Multinomial logistic regression indicated that PwP with worse tremor in their dominant hand are 4.9 times more likely to report severe (vs. slight) functional impact. While scales such as the MDS-UPDRS (Part III) 17 capture information for both sides of the body, they do not take into account whether the dominant side is affected, which our data indicate is an important consideration.
Remarkably, almost a quarter of PwP (23%) reported a prior diagnosis of ET. The relationship between ET and PD is complex 18 and there is debate as to whether ET confers an increased risk of developing PD or whether prior diagnoses of ET in PD patients are due in part or entirely to misdiagnoses. Studies have suggested that 30–50% of ET diagnoses are incorrect, with most misdiagnosed patients having PD. 19 There is limited information as to how many PD patients are initially diagnosed with ET. A retrospective chart review found that 7.1% of 210 PD patients seen for initial evaluation at an expert movement disorders center had a prior diagnosis of ET. 20 Our figure of 23% is substantially higher, and may in part be due to the fact that our population was comprised of PD patients with tremor. A chart review may also be less sensitive than direct online patient reporting.
Our findings have multiple implications that bear on clinical evaluation and management. An adequate history in a patient with tremor should include assessment of the impact of tremor, including physical, sensory, and psychosocial burdens and how these affect function, activities of daily living, and QoL. It should be noted whether tremor is worse in the dominant hand and to what degree medications have reduced or failed to reduce tremor. A prior or current history of ET should continuously be re-evaluated. When examining patients, it is important to examine the upper extremities in rest, postural maintenance and kinetic states. It is often useful to evaluate tremor with the patient performing specific tasks such as writing or drinking from a cup, as well as other activities that the patient reports cause them difficulty. Since tremor may not be present or at its worst all the time, a home video may be useful. If a diagnosis of PD is made and the patient is started on PD medications it is important to discuss the fact that medication effect on tremor is highly variable, and it may or may not provide adequate benefit. Lack of benefit for tremor does not mean that the diagnosis of PD is incorrect. Many patients with PD and motor fluctuations experience worsening of tremor during OFF periods. In these cases, medication changes to reduce or eliminate OFF may help reduce tremor through the day.
Findings from this study could be expanded in the future by studies enrolling well characterized populations both with and without tremor, to capture a more generalized PD population. This would allow comparison between PD patients with and without tremor. Such a study could also delve into other motor and non-motor features of PD and evaluate various associations and correlations.
Interventional clinical trials for PD tremor are needed. However, there is currently no validated scale for PD tremor. Our survey could potentially serve as a starting point for the development of such a scale. In addition, our results may help identify characteristics of patients whose tremors are causing impairment of function and QoL that would make them good candidates for such a trial.
Strengths of this study include its broad recruitment (including patients of all disease severities), large sample size, and comprehensive data collection across all domains relevant to function and QoL. Study limitations include those inherent to patient surveys. The results reported here were based on the PwP's own subjective understanding of their condition and were not compared with clinical information or observer ratings; there was no external confirmation of the PD diagnosis. To our knowledge, this was the first survey to address the impacts of tremor from the patients’ perspective. Although we designed the study with a small group of PwP to ensure face and content validity, we did not formally test its psychometric properties (e.g., internal consistency, reliability). However, the QoL questions were based on a validated scale. The fact that many patients were taking multiple PD medications could have made it difficult for PwP to accurately tease out individual medication responses, and their medication regimens might not have been optimized. Another limitation pertains to the recruitment methods as only those PwP with access and skills in internet use would be likely to respond to the survey and presumably only a percentage of PwP who were invited to complete the survey through the media campaign actually participated. Moreover, we do not know how many people the media campaign reached and therefore cannot comment on this source of potential bias. In addition, it is possible that individuals more impacted by their tremor would be more likely to complete the survey. Although the survey was comprehensive, there was little evidence of survey fatigue with most PwP completing most questions. However, there was an expected level of missing data (with no imputation), especially in the detailed analysis of medication effectiveness which may have affected the variability of self-reported data. We also note that we did not compare PwP with tremor to those without tremor.
We hope that our findings help serve as a catalyst for the development of new and effective treatments for PD tremor. This starts with the recognition that PD tremor is a major therapeutic unmet need. Our survey and results may also help provide the basis to develop better tools for the conduct of much needed interventional clinical trials.
Supplemental Material
sj-pdf-2-pkn-10.1177_1877718X251329328 - Supplemental material for Burden of tremor in Parkinson's disease: A survey study
Supplemental material, sj-pdf-2-pkn-10.1177_1877718X251329328 for Burden of tremor in Parkinson's disease: A survey study by Robert A Hauser, Tara Crowder Skarpaas, Andréa Merriam, Jason Rivera, Valmira Hoxhaj, Luigi M Barbato, Anita Chadha-Patel and Michelle Baladi in Journal of Parkinson's Disease
Supplemental Material
sj-pdf-3-pkn-10.1177_1877718X251329328 - Supplemental material for Burden of tremor in Parkinson's disease: A survey study
Supplemental material, sj-pdf-3-pkn-10.1177_1877718X251329328 for Burden of tremor in Parkinson's disease: A survey study by Robert A Hauser, Tara Crowder Skarpaas, Andréa Merriam, Jason Rivera, Valmira Hoxhaj, Luigi M Barbato, Anita Chadha-Patel and Michelle Baladi in Journal of Parkinson's Disease
Footnotes
Acknowledgements
The study was supported by an unrestricted grant from Jazz Pharmaceuticals who participated in the design and conduct of the study, data collection, and data management. The authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. We thank all the PwP and their care partners who participated in the survey.
Ethical considerations
The protocol and a draft survey were submitted to the Institutional Review Board (IRB) of the University of South Florida and the IRB determined that the protocol met criteria for exemption from IRB review.
Consent to participate
Respondents were informed of the purposes of this survey before the online questionnaire began and consented to the use of their anonymized survey answers in reports and publications.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Jazz Pharmaceuticals.
Conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Robert A. Hauser is supported in part by a Center of Excellence grant from the National Parkinson Foundation and is employed by the University of South Florida (Florida). He reports receiving personal fees from Acadia Pharmaceuticals, Acorda therapeutics, Adamas Pharmaceuticals, Affiris, AlphaSights, Amneal Pharmaceuticals, ApoPharma, Aptinyx, Aranca, Axovant, Britannia, Cadent, CAVR, Cerevel Therapeutics, ClearView Healthcare Partners, Clinical Score LLC, CNS Ratings LLC, Compass Group, Decision Resource Group (DRG), Dedham Group, Defined Health, Denali, Enterin, Extera Partners, F. Hoffmann-La Roche Ltd, First Word, Gerson Lehman Group (GLG), Global Kinetics Consulting (GKC), Global Life Sciences, Guidepoint Global, Huron, Impax Laboratories, Impel Neuropharma, Inhibikase, InSearch Consulting, Insignia Strategies, In-Trace Medical Systems, ISCO, IQVIA, Jazz Pharmaceuticals, Kaiser Permanente, Kashiv Pharma, KeiferRX LLC, KeyQuest, KX Advisors, Kyowa Kirin Pharmaceuticals, L.E.K Consulting, LifeSciences Consultants, Lundbeck A/S, Medscape, MJFF, MPTA, Neuro Challenge Foundation for PD, Neurocrine Biosciences, NeuroDerm, NOVUS, Orion, Parkinson Study Group, Pennside Partners, Perception OpCo, Pharmather, Pharma Two B, PSL Group, Regenera Pharma, Revance Therapeutics, Schlesinger Associates, Scion NeuroStim LLC, Seelos Therapeutics, Slingshot Insights, Sunovion Pharmaceuticals, Supernus Pharma, Teva Pharmaceuticals, Tolmar, Inc., US World Meds. Dr Hauser reports research support from AbbVie, Axovant Sciences Ltd, Biogen Inc, Biotie Therapies Inc, Cavion, Inc, Centogene, Cerevance, Cerevel Therapeutics Inc, Cynapsus Therapeutics, Enterin Inc, F. Hoffman-La Roche Ltd, Global Kinetics Corporation (GKC), Impax Laboratories, Intec Pharma, Jazz Pharmaceuticals, Michael J Fox Foundation, Neuraly, NeuroDerm Ltd, Northwestern University, Pfizer, Pharma Two B, Revance Therapeutics, Sanofi US Services Inc, Sun Pharma Advanced Research Company, Sunovion Pharmaceuticals Inc and hold stock in Inhibkase and Axial Therapeutics. Tara Crowder Skarpaas, Valmira Hoxhaj, Luigi M Barbato, and Michelle Baladi are full-time employees of Jazz Pharmaceuticals who, in the course of this employment, have received stock options exercisable for, and other stock awards, of ordinary shares of Jazz Pharmaceuticals. Andrea Merriam and Jason Rivera are employed by the not-for-profit organization, Parkinson and Movement Disorders (PMD) Alliance. Anita Chadha-Patel is employed by ACP Clinical Communications, Ltd, which was contracted by the PMD Alliance to provide medical writing services for this study and provides services to several companies active in the field of movement disorders.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.