
Abstract
Recently, two proposals for defining Parkinson's disease and its related pathogenic processes have been published. In this viewpoint, we discuss the primary drivers behind these efforts, the future directions, and the challenges that must be addressed. While finding biomarkers is a mandatory step for better precision medicine and optimal patient stratification in therapeutic trials, we argue that a biological definition of Parkinson's disease based on a single biomarker will struggle to account for the complexity of the mechanisms involved in developing the disease. Additionally, a biological definition of asymptomatic patients should rely on a thorough understanding of patients’ clinical trajectories, which is currently not the case in synucleinopathies.
Plain language summary
Two recent articles proposed a biological definition of Parkinson's disease, highlighting the importance of detecting aggregated alpha-synuclein in biofluids or tissues. This viewpoint explores the motivations behind these proposals, their potential implications, and the challenges they face. It emphasizes that relying on a single biomarker to define Parkinson's disease is unlikely to capture its complexity. The authors advocate for combining clinical and biological insights. They also discuss parallels with Alzheimer's disease and how similar approaches influenced its diagnosis and therapeutic development.
Introduction
Finding biomarkers in neurodegenerative diseases is mandatory for the development of therapeutic targets. It has become evident that patient selection and monitoring in clinical trials should be more than just measured through diagnosis criteria or scales largely built from clinical features. This approach is at risk of misdiagnosis, recruiting patients in stages when significant neuronal loss has already occurred, and needs more sensitivity for evaluating primary outcomes. Besides, the absence of specific biomarkers restrains the evaluation of target engagement. However, whether one unique marker could bring all those kinds of information is more complex. This is particularly the case for Parkinson's disease (PD), whose predominant pathological hallmark is the presence of alpha-synuclein (aSyn) aggregates in neural but also, to a certain extent, in non-neural tissues. However, how aSyn dynamics correlate with disease severity and progression or whether they act as the main component of neurotoxicity has yet to be established.1,2 Moreover, some patients suffering from monogenic causes of PD are exempt from aSyn lesions, while their clinical presentation and therapeutic management can be nearly indistinguishable from idiopathic “aSyn-related” PD. PD patients’ trajectories are also highly heterogeneous. While distinct proportions of patients could display prodromal aSyn-related symptoms, no feature can predict future trajectories. This uncertainty also applies to clinically established PD. Different patterns of evolution or emergence of motor or non-motor features between individuals suggest that subtypes of PD could exist.3,4
Two recent position articles published in The Lancet Neurology in February 2024 aimed to address some of these issues and proposed a roadmap for developing either a biological definition, classification, or staging of PD. One of them proposed a radical change in the current nosography by dropping the entity of PD from their system. 5 The other could be understood as the state-of-the-art of current measurement tools for classifying pathogenic processes, including neurodegenerative and genetic features, thus giving more credit to phenotypic and biological diversity. 6 Both proposals outlined the importance of detecting aggregated aSyn in biofluids using seed amplification assays (SAAs).
Interestingly, some of the reactions from the PD community focused on the semantics employed in the articles. Although each proposal aimed to address separate goals (i.e., either “definition/staging” or “classification”), both have been broadly understood as initiatives to redefine PD (but also dementia with Lewy bodies – DLB).7–10 Other reactions arose from the focus on aSyn status. While the promising avenues of in vivo pathological assessment of aggregated aSyn have been acknowledged, some remarks pointed out the importance of non-aSyn-related pathological mechanisms in PD, which is currently lacking in both proposals.9,11–13 Ethical concerns also emerged, considering that a positive SAA for aSyn could be confounded with “disease” states under present frameworks.
The International Parkinson and Movement Disorder Society recently summarised these comments and, given that present proposals are preliminary, proposed that 1) clinical definition of PD and DLB should remain, 2) biological definitions of PD should be enriched with other pathological processes, and that 3) ethical considerations are central for current and future developments. 10
We should sympathise with the evolution of neurological taxonomy and acknowledge that disease entities are partially historical constructs. This is particularly true for PD, whose seminal description more than two centuries ago is still valid for its current phenotypic definition. However, with such categorisation and simplification, one must clearly state what information is lost in the process. More precisely, when anchoring pathological entities with biological markers, those must have enough accuracy to cover such different presentations before discarding clinical descriptions.
In this viewpoint, we aim to reinforce this direction for the biological characterisation of neurodegenerative diseases providing a translational (clinical and biological) point of view. Finding surrogate biomarkers is mandatory for better precision medicine and optimal patient stratification in therapeutic trials. We briefly review the two positions above and describe some of the main biological processes and their related challenges that should be accounted for in the future optimisation of these criteria. We also provide some insights into similar directions in Alzheimer's disease (AD) and their consequences in disease definition and therapeutic development.
A better biological characterization of PD is crucial
In their Neuronal Synuclein Disease Integrated Staging System (NSD-ISS), Simuni and colleagues exposed an iconoclastic position by introducing the so-called neuronal synuclein disease (NSD). 5 NSD is defined by positivity for aggregated synuclein (S) and the eventual presence of neuron dysfunction (D, i.e., degeneration). Considered measures for defining S and D status are seed amplification assays (SAA) in cerebrospinal fluid (CSF) and molecular imaging (i.e., DAT imaging), respectively. One central point of this system is the complete overlap between disease phenotypes. The NSD-ISS makes no distinction between patients who suffer from early cortical involvement (i.e., DLB) and those who do not (i.e., PD). The authors also consider that the motor phenotype is one over the multiple expressions of NSD, encompassing isolated REM sleep behavior disorder (RBD) and pure autonomic failure. Moreover, the absence of positive evidence of S discards patients currently qualifying for a PD diagnosis from being diagnosed with NSD. In this line, many patients with genetic mutations such as LRRK2 or PRKN are not considered by the NSD-ISS. On the contrary, asymptomatic patients who are incidentally detected as S + could be diagnosed with NSD. The second purpose of NSD-ISS is staging. Asymptomatic S + individuals are defined as NSD stage 1, while stages 2 and 3 involve those with different degrees (mild/non-motor versus motor) of clinical involvement. The authors pointed out that this staging further requires integrating supplemental biological features that have yet to be entirely determined.
In their SynNeurGe system, Höglinger and colleagues alternatively focused on the synergistic impact of synuclein (S), neurodegeneration (N), and genetic (G) features on pathogenicity. 6 Positive S measurement is supported by SAAs from CSF or skin and N status by suggestive dopaminergic, cortical, or even cardiac/sympathetic pathological patterns using molecular imaging. Once again, motor symptoms are unnecessary to achieve a biological definition of the disease. However, the authors clearly distinguished between sporadic Parkinson's disease (S+, N+) and sporadic Parkinson's type synucleinopathy (S+, N-), highlighting the currently unknown implications of S+/N- status. Interestingly, this system then recognizes biological PD without any central nervous system involvement in individuals with skin aSyn pathology and evidence of cardiac sympathetic denervation. Another difference with the former proposal is the explicit addition of a third biological term anchored in patients’ genetic status (G). The authors broadened the genetic status to fully penetrant variants such as SNCA or PRKN (Gf), predisposing genetic factors to PD like GBA1 and LRRK2 (Gp). Finally, the authors discarded biological staging, considering the low value of current methods for predicting disease progression.
Both proposals offer some entirely orthogonal conceptions and strategies. While the NSD-ISS suggests unifying biology sustaining all future clinical presentations, the SynNeurGe classification broadens future directions to multiple interleaved pathogenic mechanisms. Both proposals highlighted the considerable advancement of in vivo detection of aggregated aSyn using SAAs.
Whether these criteria, with the current use of SAAs as a central marker, should be used for screening, diagnosis, or prognosis purposes has yet to be determined, with specific questions emerging from each situation.
Screening: How valid are biological criteria and current measures for predicting the conversion of asymptomatic S + subjects to a clinical disease state (i.e., what are the risks of treating test results rather than a disease)? Diagnosis: Are biological criteria and current measures more accurate than pre-existing tools to detect a disease in a symptomatic population? Prognosis: How accurate are current biological features to define disease trajectories?
Current limitations and diagnosis performances of seed amplification assays
Two relatively similar techniques, Protein Misfolding Cyclic Amplification (PMCA) and Real-Time Quaking-Induced Conversion (RT-QuiC), are currently used to detect seeding activity of misfolded protein aggregates in biosamples. Briefly, aSyn-SAAs trigger protein polymerization by adding exogenous seed-free aSyn to a given sample prone to self-aggregation. This is performed by applying several rounds of vigorous intermittent shaking/rest to induce cycles of fragmentation/elongation, followed by detection through amyloid-sensitive Thioflavin-T (ThT) dye fluorescence at each cycle. This allows the production of time-dependent aggregation curves that usually follow a sigmoid pattern. It is characterized by an initial lag phase reflecting seed formation (nucleation phase) and a subsequent growth phase leading to a stable state.14,15 While both protocols are similar, PMCA is longer than RT-QuiC.16,17 Detection thresholds vary among studies, using absolute (all samples above a pre-determined fluorescence value in arbitrary units) or relative values (for example, mean background signal plus n-fold standard deviations). The often-neglected ThT negative recombinant or human-derived polymorphs are of particular importance, thereby questioning the ThT exclusivity of these SAAs.18–23 The amount of positive replication often decides one sample's positive status.
An important methodological aspect is the biological nature, significance and specificity of SAA reaction products. New structural biology techniques, in particular cryo-electron microscopy (EM), helped to unmask failures in the fidelity of the amplified seeds of aSyn. The cryo-EM structures of aSyn filaments from the human brain of patients with PD, DLB and multiple system atrophy (MSA) differ from those of recombinant proteins assembled in vitro, even when using brain-derived filament preparations to seed in vitro assemblies.24–27 This structural mismatch between human and synthetic products was also observed using beta-amyloid or tau species.28–30 This discrepancy could be due to aSyn assemblies’ reliance on physical/chemical factors such as temperature, pH, buffer composition, and monomer concentration.17,31,32 Overall, current assays are not suitable for precisely mimicking the structural aspects of the natural aSyn aggregates.
SAAs showed high sensitivity (more than 95%) to detect Lewy-body (LB) pathology in brain homogenates or CSF of patients with pathological confirmation and specificity close to 100% in CSF samples from healthy controls or patients without LB pathology.33–36 SAA could then be a proxy for detecting in vivo aSyn pathology, and some recent works suggested that quantitative kinetics parameters could be related to LB burden. 35 Whether this feature is sufficient and necessary to define a clinical pathological entity remains uncertain since extensive incidental LB pathology can be seen in asymptomatic individuals. 37 To date, we have little information on the risk of progression to motor or cognitive symptoms in asymptomatic S + patients. Only one longitudinal study in a memory clinic cohort showed that 23% of asymptomatic individuals with a positive SAA developed prodromal DLB or PD after a mean follow-up of 4.5 years. 38 This suggests that at least in the medium term, most S + patients will remain asymptomatic, calling into question the clinical relevance of this pathological definition.
When assessing the diagnostic performance of clinical PD, CSF SAAs showed 88% sensitivity and 95% specificity when compared to healthy individuals or patients with non-synucleinopathies. Similar values were obtained from skin, while assays from other tissues remain investigational.39–41 These accurate performances validate this technique against the gold standard, which is clinical criteria. This credit has also been confirmed in the framework of clinical trials, as 91% of biological samples showed seeding activity in untreated de-novo PD patients, who were recruited into the SPARK and PASADENA trials. 42 Another interpretation could be that the clinical PD diagnosis using current criteria is effective since it displays accurate pathological validation. However, some variability could exist depending on the assessors’ level of expertise and training.43,44 Several limitations also remain in current procedures. Although some studies reported the value of quantitative parameters, SAAs currently deliver dichotomous readouts using different cut-offs. This restrains the value of SAAs alone for better predicting phenotypic variability. Moreover, positive rates on patients with MSA are still inaccurate since around 30%, on average, display a seeding activity, especially using RT-QuiC. 16 Although semi-quantitative measures using PMCA could help discriminate between Lewy body or MSA-type aggregation profiles, a positive SAA alone could likely not help distinguish between those two entities.20,45 One explanation could lie in the structural differences of aSyn strains between synucleinopathies. For example, both ex vivo and in vitro MSA aSyn filaments differ from those observed in PD and DLB.23,25,46,47
The challenge of predicting a clinical diagnosis of PD, DLB, or MSA in individuals at risk
RBD is one of the most studied predictors of synucleinopathy, with an estimated annual conversion rate of about 6%. After 12 years of progression, 70% of patients have a clinically established synucleinopathy, with equivalent proportions between DLB and PD.48,49 Finding accurate predictors is crucial given that the estimated RBD prevalence is about 1% in a healthy middle-to-older age population and its highly variable lag phase (over decades) before disease onset. 50 Longitudinal studies showed that mild motor symptoms, cognitive changes, impaired olfaction, or dysautonomic features could predict a clinical diagnosis of PD, DLB, and MSA in patients with isolated RBD.48,51 However, some of those changes are too subtle to provide accurate predictions at the individual level (plus 3 points of the MDS-UPDRS part III between disease-free and converters), and they hardly discriminate between cognitive or motor-predominant evolution. While abnormal DAT imaging has also been considered a short-term predictor, additional biological markers may prove useful for better prediction. 52
Studies exploring SAAs in RBD subjects found that they are predominantly positive (around 90%) in CSF.51,53,54 The remaining small subset of SAA-negative subjects in those studies had lower conversion rates, which may suggest a lower aSyn pathology burden or a later clinical MSA diagnosis rather than a “neuronal” synucleinopathy. Therefore, SAA positivity in RBD subjects is consistent with an underlying aggregated aSyn neuropathology. However, SAA measures require going beyond dichotomic readouts to enhance their value to predict future clinical presentation. Some kinetic parameters, such as longer lag phases before reaction initiation or smaller maximum fluorescence intensity, allowed RBD to be distinguished from PD in one study. 55 Whether those parameters could help distinguish aSyn pathology burden or different aSyn conformations as observed in MSA patients remains to be confirmed (an issue further complexified by the inter-centre variability in mastering SAAs). Less invasive samples such as olfactory mucosa, blood, or skin still have lower sensitivity than CSF or require more replication. However, some studies on skin tissue showed comparable accuracy to CSF.
Evidence from pure autonomic failure (PAF), another “pre-motor” presentation of aSyn, is less abundant. SAA has been recently shown to help distinguish conversion to PD and MSA phenotype, although this result remains to be replicated in larger cohorts. 45
Genetic predisposition is another essential feature for predicting disease status. More than 90 gene loci are the source of risk variants depending on the geographical location of individuals. 56 LRRK2 variants are the most frequent causes of monogenic PD and could be present in the absence of a family history. On average, about one per cent of non-familial PD patients carry the most frequent mutation (p.G2019S), with substantial variability depending on geographical localization. This proportion rises up to 40% in North African Arab sporadic cases. 57 LRRK2 mutation is also characterized by reduced penetrance, and polygenic interactions may determine the emergence of clinical symptoms. 58 Importantly, aSyn pathology is inconstant in LRRK2 patients, although its presence may predict worse cognitive impairment and clinical trajectories are nearly indistinguishable from sporadic PD. 59 Thus, both aSyn pathology and polygenic features, including LRRK2 variants, may be essential for stratification.
The incorporation of multiple biological and phenotypic components is necessary for better predicting patient trajectories
One final challenge remains in predicting disease course and severity based on biological and genetic predisposition. GBA1 variants constitute a significant feature that affects disease progression, especially for the occurrence of cognitive impairment. GBA1 polymorphism is frequent in PD patients (10%), but not all variants have a documented pathogenic effect. Over 300 variants were identified in the PD population, and the pathogenic status of the vast majority remains unknown. 60 While low-risk mutation carriers display similar disease trajectories compared to noncarriers, those with high-risk mutations have faster progression to major cognitive disorders.
Cognitive decline may occur at early prodromal stages, even in individuals without motor symptoms, linking GBA1 mutation to DLB phenotype.61–63 Asymptomatic individuals or subjects with RBD with GBA1 variants also convert to PD earlier than subjects with no mutation and may display more aggressive motor progression.64–66 GBA1 mutations affect lysosomal protein degradation through glucocerebrosidase dysfunction, thus enhancing the accumulation of aSyn species. 67 Several gene polymorphisms involved in lysosomal pathways are frequently observed in PD patients, and additional variants related to lysosomal functions among GBA1 mutation carriers may exert negative effects on the disease course.68–71 These observations highlight the importance of better understanding biological pathways, such as lysosomal functions, to fully describe aSyn dynamics in patients. 72
The co-existence of other biological features could also substantially impact patient trajectories. As reported recently, more than one-third of AD patients with confirmed amyloid and tau pathology in CSF are positive for aSyn on SAA. 73 Similarly, the presence of amyloid and tau co-pathology is frequent in patients with PD and correlates with worse cognitive outcomes. 74 These findings confirm the importance of co-pathology assessments and, once again, reduce the likelihood of patient stratification solely based on one neuropathological marker.
Finally, an optimal assessment of biological markers should account for the clustered trajectories of clinical progression. For instance, one can extract different progression profiles from multiple time-dependent clinical outcomes. This approach would provide meaningful results for addressing disease course heterogeneity among patients using a data-driven (hypothesis-free) approach. This approach would prevent substantial loss of information from an a priori categorization anchored in one or another unique marker and allow a better understanding of aSyn pathology dynamics among different clusters of disease progression.3,4,55
Recent lessons from AD
The recent efforts for a biological definition of PD align with those for AD in 2018 by the National Institute of Aging and the Alzheimer's Association (NIA-AA). 75 Clifford Jack, the lead author of the NIA-AA biological criteria, recently welcomed this conceptual advancement in synucleinopathies. 76 This conceptual shift has sparked numerous debates since 2018, opposing the NIA-AA with the International Working Group (IWG). The latter proposes to anchor AD diagnosis on specific clinical presentation with biological diagnostic support. This clinical-biological definition is in line with its historical clinicopathological concept.77,78
The main argument of the IWG is the substantial amount of amyloid pathology in the asymptomatic ageing population (30% of cognitively healthy subjects aged 80 are amyloid-positive, as measured with PET or CSF biomarkers). 79 Furthermore, the progression to dementia in asymptomatic amyloid-positive subjects is highly variable and uncertain over a lifetime, ranging from 5% to 77%, depending on demographics, additional biomarkers, and APOE genotype.80,81 This decoupling between individual biological status and cognitive outcome motivated the IWG to define amyloid-positive cognitively healthy people as subjects “at risk” of developing AD rather than patients with a “preclinical” disease. Furthermore, the IWG emphasizes the risk of misdiagnosis and management error associated with a biological definition of AD, mainly due to the high frequency of co-pathologies. Indeed, cognitive impairment in patients with positive AD biomarkers is not necessarily attributable to AD neuropathological changes. This is illustrated by the critical co-occurrence of amyloid pathology in patients with Lewy-body disease presentation.
The biological definition of AD is still debated even after the publication of several longitudinal cohorts of healthy subjects with confirmed amyloid and tau status, thus allowing an in-depth validation of biological criteria. 77 A lower prevalence of PD and DLB in the general population makes these studies more challenging than in AD. Nevertheless, one cohort enriched in individuals with cognitive complaints demonstrated that after five years of follow-up, those with evidence of aSyn seeding activity were more likely to remain asymptomatic rather than developing any cognitive or motor symptoms. 38 This example illustrates the challenges in linking a given biological presentation to a specific clinical progression in synucleinopathies.
One must also consider the tempting drift from “research” to “clinical” criteria over the years. While 2018 NIA-AA biological criteria were initially proposed for research purposes, their 2024 revision suggested a clinical use. 82 This paradigmatic shift will have a tremendous epidemiological impact, considering that only 17% and 8% of individuals meeting this definition in the general population will have mild cognitive impairment and dementia, respectively. 83 It also carries the risk of disconnecting researchers and clinicians from the societal perception of neurodegenerative diseases (biological definition in asymptomatic individuals vs. individuals experiencing loss of autonomy). After reviewing all recent literature, the IWG has once again opposed the biological definition of AD supported by the AA in its 2024 recommendations. 84 However, it opens the possibility of diagnosing presymptomatic AD in cognitively healthy individuals who present a combination of biomarkers indicating a very high risk of short-term clinical progression (such as being amyloid-positive and tau-PET-positive in neocortical areas). 85 Other biomarker-positive asymptomatic individuals remain classified as “at risk” for AD because they will not become symptomatic among a proximate timeline. According to the amyloid cascade hypothesis, the AA envisions a deterministic biological continuum from proteinopathy to dementia. The IWG, on the other hand, identifies discrete nosological entities, distinguishing between at-risk proteinopathy and presymptomatic or symptomatic AD. This distinction between latent and manifest states may also apply to synucleinopathies. 86
The biological definition of AD coincided with the US approval of anti-amyloid immunotherapies, even before these treatments demonstrated clinical efficacy. 87 Indeed, the FDA considered that the amyloid-lowering effects were “reasonably likely to predict clinical benefit”. However, amyloid PET imaging has not been validated as a surrogate marker for clinical efficacy. 88 The parallel is intriguing today with the field of PD, in the era of the development of anti-aSyn therapies.
Conclusion
All efforts to better understand pathogenic mechanisms in neurodegenerative diseases should be welcomed and encouraged. Even if debatable, strong statements are incentives for an in-depth and creative reshaping of our traditional knowledge. The simultaneous publication of both proposals induced an optimal situation for such considerations. That said, we should remain open-minded and be cautious when considering the dimensions of PD reduced to a few biological features. Biological assessments of aSyn pathology remain static values of one isolated dimension without considering precise interactions with other processes like genetic predisposition and co-pathology (Figure 1). Moreover, SAA products should not be regarded as direct evidence of natural aSyn aggregation, whose pathogenicity likely implies additional biochemical and cellular parameters. Finally, analysing biological dynamics without considering clustered symptom trajectories may be a significant limitation of their predictive value, especially for markers of early diagnosis of PD, DLB or MSA.
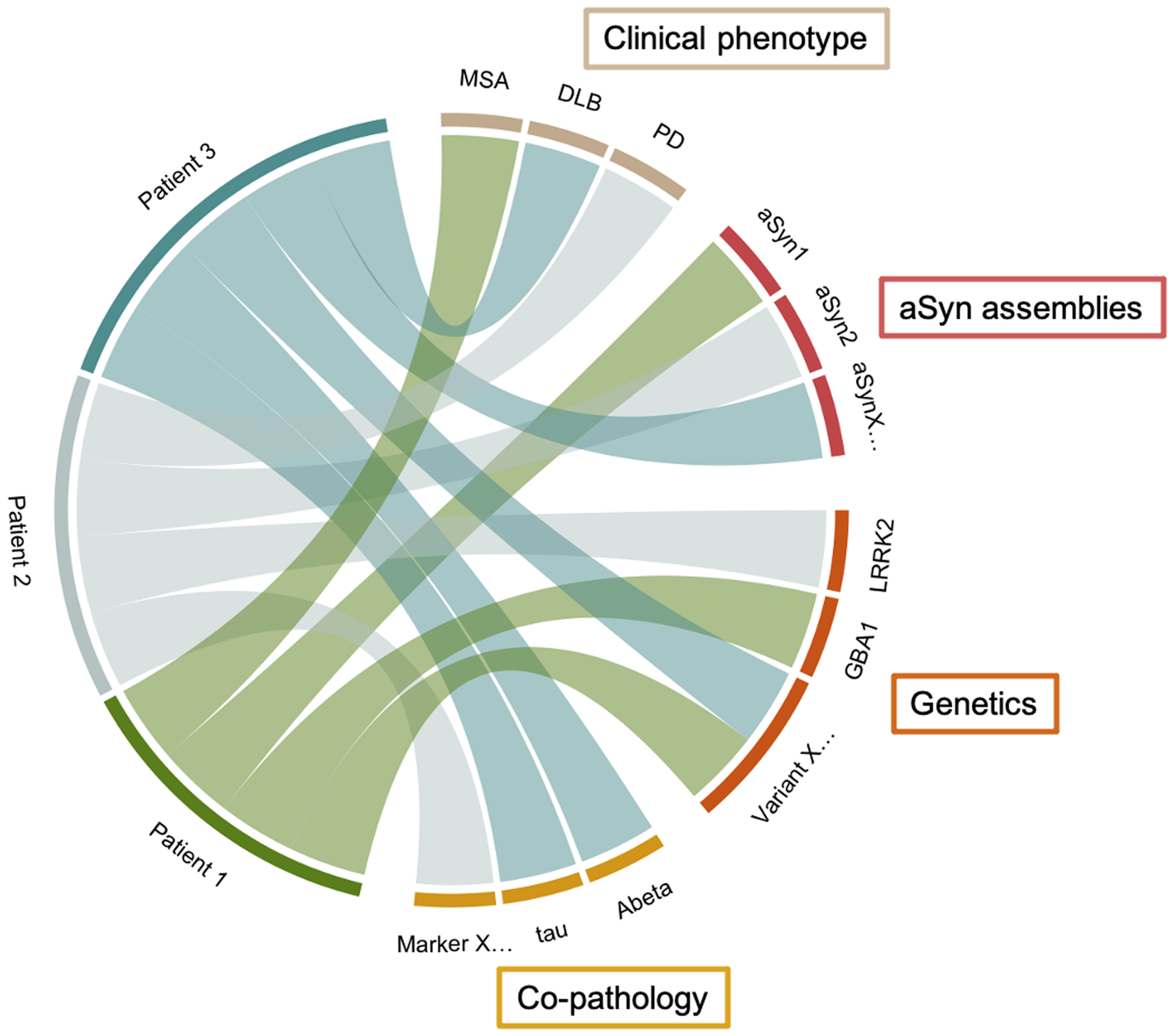
Schematic representation of a clinico-biological framework based on hypothetical aSyn aggregate subtypes, co-pathology markers, genetic features, and clinical phenotypes.
Further technical advancements are necessary to validate the accuracy and fidelity of amplified seeds in reflecting the actual content of patients’ brains. One way of achieving this could be using a panel of SAAs for different proteopathic seeds (including ThT-negative ones) to compare biological samples from patients with suspected neurodegeneration. To this end, it would be beneficial to establish and enhance the diagnostic accuracy of these SAAs through large-scale longitudinal studies to identify incident clinical symptoms and ideally incorporate anatomopathological assessments. Additionally, ensuring standardization and reproducibility across different centers is crucial before implementing such a diagnostic panel. In this regard, the initiation of a worldwide reflection on the standardization driven by health authorities could emerge through the establishment of guidelines on the harmonization and standardization of an SAA protocol with the ultimate goal of demonstrating reproducibility between different laboratories on an international scale, facilitating communication between researchers, and informing the interpretation of clinical biomarkers. This time of reflection was beneficial for harmonizing and improving RT-QuIC sensitivity and specificity for sporadic Creutzfeldt-Jakob disease.89,90
Nevertheless, these proposals point to implications for clinical trials. Accordingly, SAAs should be considered as an additional tool for patient selection in aSyn-targeted trials. This simple and pragmatic statement aligns with what has already been done in different fields, like cancer therapy, in which patients are selected and stratified through a panel of genetic/biological markers to provide personalized treatment. However, their use to define other features, such as target engagement or outcome measures, needs to be improved in the absence of quantitative assessment.
Finally, the biological definition of a disease tends to assume that any effective action on biology will have a clinical impact. However, this can only be the case with a well-established link between biology and clinical trajectory. Therefore, one should be careful about future semantics when defining “disease”, “prodromal,” or “at risk” states, as these terms rely not only on biological but also societal and public health features such as autonomy or long-term expectations.
Footnotes
Acknowledgments
We apologize to the authors of several high-quality scientific articles that contributed significantly to the development of the field but could not be cited due to space limitations.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: D.B. is a recipient of a Clément Fayat Foundation fellowship (France). INSERM, CNRS, CHU Bordeaux and the University of Bordeaux provided financial and infrastructural support. This study received financial support from the French government in the framework of the University of Bordeaux's IdEx “Investments for the Future” program (GPR BRAIN_2030).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: During the past 3 years, DB was a local unpaid sub-investigator for clinical trials granted by UCB Biopharma, Ionis Pharmaceuticals, Hoffmann-La Roche and Theravance Biopharma. During the past 3 years, VP was a local unpaid investigator or sub-investigator for clinical trials granted by Novo Nordisk, Biogen, TauRx Pharmaceuticals, Janssen, Green Valley Pharmaceuticals and Alector. EB is a director and shareholder of Motac Neuroscience Ltd EB is a shareholder of Treefrog Therapeutics and SE Therapeutics. Outside the present work (past 12 months), WGM has received consultancy fees from Lundbeck, Inhibikase, Takeda and Koneksa. BD declared no conflict of interest.