
Abstract
This study explores perceived benefits and use cases of three smart furniture prototypes, a smart chair, a smart mirror, and a smart table, designed to support ageing-in-place and care delivery. The research applies the Design for Somebody (DfS) methodology, focusing on modular, user-centered development for individuals with specific needs.
An online survey incorporating video demonstrations was conducted with 21 healthcare professionals and 18 end-users across six European countries. Participants assessed the perceived benefits of the prototypes, proposed enhancements, and identified relevant user groups. Quantitative data were analysed using descriptive statistics and chi-square tests, while qualitative responses were subjected to thematic analysis.
Findings indicate that the smart chair received the most positive feedback, particularly for promoting physical activity and motivation. The smart mirror was valued for daily reminders and memory support, while the smart table raised concerns due to reliance on smartphone interaction. Although no statistically significant differences were found between user groups, responses varied by role and gender.
This study provides practical contributions to the development of inclusive and adaptable smart furniture within care environments. By integrating co-design practices, DfS methodology, and video-based surveys, the research demonstrates an effective approach to mapping user needs. The findings offer novel insights into modular, user-driven design strategies that support the advancement of ambient assisted living technologies.
Introduction
The global shortage of social and health care professionals is an increasing challenge, exacerbated by the increasing aged population, rising care demands and cost (World Health Organization, 2016). The workforce shortage strains the provision of existing services, leading to concerns about the quality, efficiency, and accessibility of care (Pittman et al., 2021). Simultaneously, demographic shifts result in a growing number of elderly individuals requiring long-term tailored support (Belmonte et al., 2025), increasing the need for innovative solutions to fill in the care gap caused by the shortage in trained humans. In this context, technological innovations such as smart furniture present an opportunity to enhance care environments (Fewella, 2024). By integrating automation, sensors, and AI-driven functionalities, smart furniture can support both caregivers and their clients, improving safety, comfort, and efficiency in social and health care settings (Hu et al., 2020; Maulana et al., 2024; Merilampi et al., 2020).
Smart furniture can be utilized by diverse users and for different purposes. One of the promising areas for smart furniture is ambient assisted living (AAL) (Stodczyk and Uhp, 2020). The trend of supporting independent living can be seen in many health and safety technology solutions on the market. However, people may postpone the use of technologies due to the associated stigma or cost. Unlike traditional assistive devices, smart furniture and smart home products are designed not just for users with special needs but are integrated as part of modern living. This design philosophy allows technology to be discreetly embedded, providing no visual clues about the users need for assistance, thereby reducing potential stigmatization (Merilampi et al., 2020).
In AAL applications, one of the main aims is to enable independent living. This can be achieved through many approaches, for example by monitoring and alarming about potential risks or accidents, assisting in safe daily living and executive function and enhancing social inclusion (Pinard et al., 2019). Despite the advances in smart furniture technologies, there remains a challenge in aligning these innovations with the actual needs of the individual user rather than another mass produced one size fits all technology, which is crucial for the successful implementation of such technologies.
Co-creation is an essential element in user-centered technology development. In the co-creation process, users are seen as the experts for their own life needs and they actively participate in the development of any supportive furniture. The joint understanding is built in this iterative and cyclic process in which the following steps are repeated until the final individualized design is achieved: emphasize, define, ideate, prototype, test (Pande and Bharathi, 2020). In this paper, Design for Somebody approach (Merilampi et al., 2018) is applied in the co-design of smart furniture. The goal of this approach is similar to Design for All (DfA). DfA is a well-known concept which means the design of products, environments, programmes and services to be usable by all people, to the greatest extent possible, without the need for adaptation or specialized design (Design for All definition, 2025). Although the two approaches aim for the same goal, DfS differs from the mindset. The goal of Design for Somebody (DfS) philosophy is to provide solutions to live in optimum capacity despite of limitations in functioning. DfS serves especially target groups with specific needs as a ‘bottom-up’ philosophy (from small to all). Modular design with replaceable ‘modules’ is the key in individualized modification utilizing the generic solution base designed for the big crowds added only with required specific modules. A person, referring to even an individual or small target group, is at the centre in the DfS development process. First, a thorough and deep user needs analysis is performed by a multidisciplinary team, including the end-user. This follows a joint problem definition and ideation phase leading to first prototypes which are evaluated by the users. This first level iteration round may consist already of several iterations. The second level iteration round concentrates on widening the involved users to find replaceable modules which are required for the prototypes, to serve different user groups. Also, the second level may consist of several iterations. The third level iteration round then contains finalized prototypes, which are tested by many users.
First, three smart furniture prototypes, a smart chair, a smart mirror, and a smart table, were developed through a co-creation process with end users (see, e.g. Merilampi et al., 2020; Sakif et al., 2024; Schwarz and Lobo, 2007). This article thus considers the second level iteration round of prototype development and concentrates on the further development needs and new potential use cases which are studied by an online survey. The feedback will provide invaluable insights for further development of smart furniture solutions, ultimately aiming to bridge the gap between technological possibilities and real user needs in the context of an ageing population facing resource constraints in social and health care.
Materials and methods
An online survey was selected as the primary method for this second-level DfS iteration to support need mapping and early-stage requirement analysis in a cost-effective and scalable way. The survey enabled the validation of the perceived benefits of the prototypes and the collection of feedback from both a geographically diverse group of new end-users and a secondary user group, i.e. healthcare professionals. This broader reach aligns with the goals of the second DfS phase (Merilampi et al., 2018): identifying additional user groups, assessing usability across contexts, and informing modular development. Additionally, the inclusion of video-based prototype demonstrations allowed participants to engage with the concepts remotely, making it a suitable method for evaluating early-stage smart furniture solutions still under development. The online survey details and research questions are briefly presented next, followed by introductions of the prototypes being developed and presented in the videos of the survey.
The online survey
The online survey was conducted in two languages: Finnish (available from April first to September 30 2024 via the project webpage) and English (available from July first 2023 to May 31 2024 via the SurveyMonkey platform). Both versions were designed for voluntary participation and were promoted through public and professional channels without individual targeting. The English version was shared via LinkedIn, the ReACTIVE Too consortium, and the University of Wolverhampton's internal newsletter WLV Insider. The Finnish version was distributed through SAMK's (Satakunta University of Applied Sciences) extensive stakeholder networks, Satakunta Testbed's website, LinkedIn, Facebook, and in-person contacts. Separate but structurally similar surveys were created for end-users and healthcare professionals to ensure relevance to each group.
The survey included background questions (e.g. gender, age, country, work situation, and possible disability), prototype demonstration videos, and both multiple-choice and open-ended questions. For each prototype video, participants were asked to evaluate: (1) potential benefits, (2) desired additional information or functionalities, and (3) improvement suggestions. The survey was pre-tested with four participants (two end-users and two care professionals from Finland and the United Kingdom), leading to minor adjustments based on their feedback. Ethical approval was obtained from the Faculty of Science and Engineering Ethics Committee of the University of Wolverhampton (LSEC/2022-23/FM/004).
The recruitment approach aimed to ensure wide accessibility without targeting individuals directly. Because the prototypes are primarily designed for elderly users, the survey descriptions explicitly encouraged seniors to participate. As a result, the sample includes a higher proportion of older adults and may not reflect national demographic distributions. This purposive sampling aligns with the study's focus but may limit generalizability. No stratified sampling by age or other demographics was applied.
Healthcare professionals were mainly reached through the Satakunta Testbed and the professional networks of SAMK and the University of Wolverhampton. These networks represent professionals engaged in care services, welfare technology, and healthcare innovation. While diverse, the sample may reflect individuals more inclined towards technology adoption and development, potentially introducing a bias towards innovation-awareness.
Confidentiality and anonymity of data within the research process were achieved by coding participants. Any collected data about participants were stored in a password-protected computer/encrypted laptops and online (on the University's database) protected by passwords according to the General Data Protection Regulation (GDPR) principles.
To ensure a thorough interpretation of the results, a multidisciplinary team of experts having backgrounds in healthcare, software and hardware engineering, furniture design, co-creation as well as materials science, conducted the analysis. Quantitative data was processed using Excel, while qualitative data underwent content analysis, focusing on themes that could further guide prototype development and better address user needs and potential user groups. All free-text comments were initially translated into English, then condensed and categorized for analysis. The researchers were seeking answers to the following research questions (RQ): RQ1: What benefits did the respondents identify in these prototypes for end users? RQ2: What benefits did the respondents identify in these prototypes for professional care? RQ3: What improvements did end-users and care professionals suggest for these prototypes?
Prototypes presented on videos of the online survey
The preliminary versions of the smart furniture prototypes under development were presented in the videos as part of the online survey. The prototypes include smart chair, smart mirror as well as smart table which are introduced on the videos by speech as well as by use demonstrations.
Smart chair for activation and monitoring
Chairs can be found in every household, which makes them interesting platforms for smart functionalities. In this example, force (pressure) sensors (Figure 1) were embedded into a chair seat. The sensors may be placed inside an upholstered seat or alternatively, a removable cushion might be used in case the seat must be portable (for example wheelchair users). The chair in the video uses a matrix of 9 force sensors and detects if a person sits on the chair or if the person sitting leans in different directions.
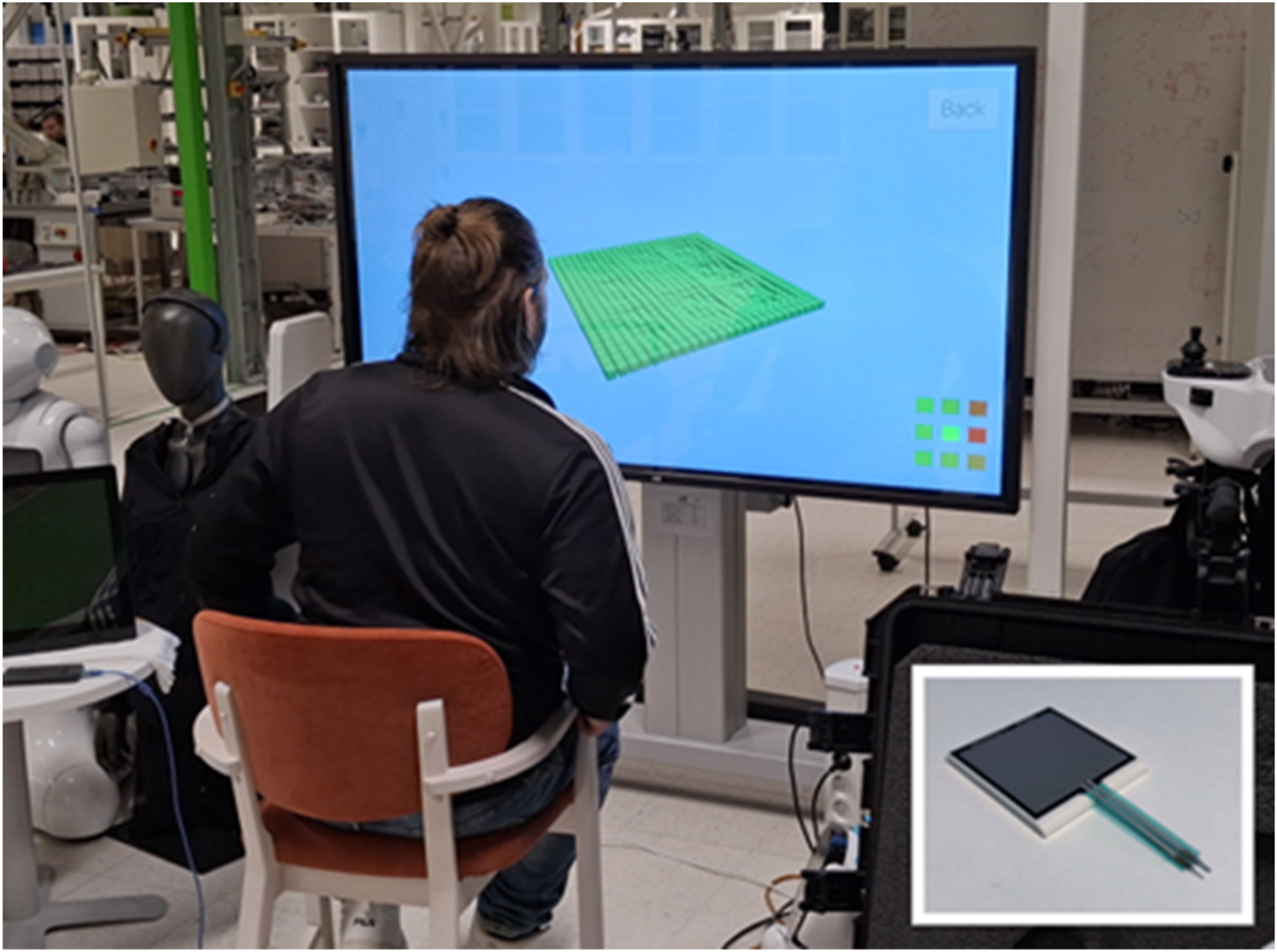
Force sensing resistor (FSR, Interlink Electronics Model 406) attached to a chair. The screen displays real-time visualization of force distribution as the user leans, illustrating pressure changes across the seating area.
Arduino Nano 33 BLE connected to power bank was used for powering the sensors and sending (via Bluetooth) the sensor data to Android device to be used by different applications, such as applications for monitoring or controlling.
In the video, the data was used to control exergames in order to enhance the users’ physical ability to function. Two exergames, ski jumping and snowboarding, were developed on Android device to visualize the chairs functioning. In ski jumping, the player initiates a jump by getting up from the chair and in snowboarding, the character is moved by leaning left and right while sitting on the smart chair. Screenshots of the two mini games are presented in Figure 2.
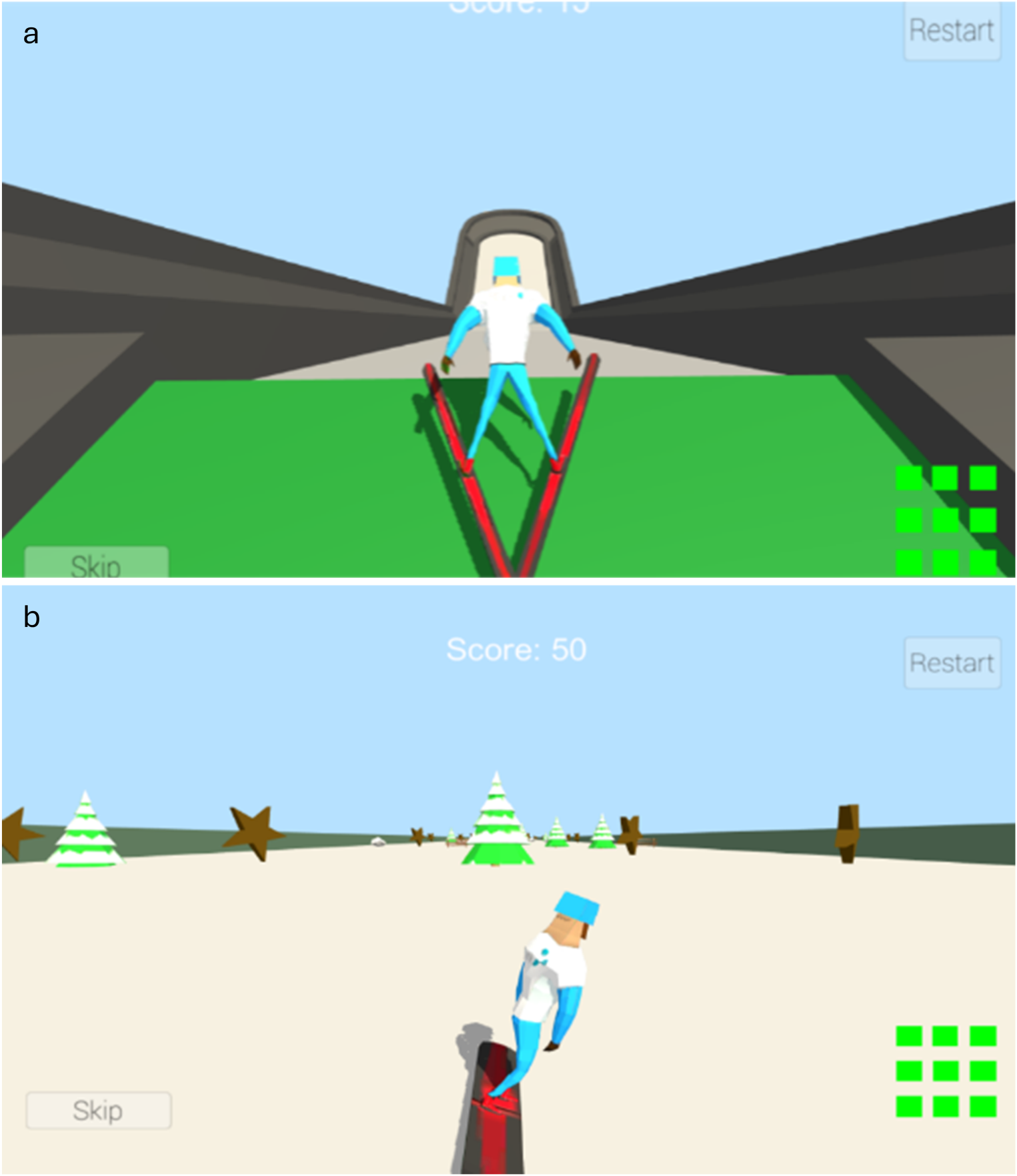
Screenshots of the exergames where the character is controlled either by standing up (a) or by leaning (b) in a smart chair.
As mirrors are present in almost all homes and institutions they can be used, besides their main functionality, as displays in a static or interactive manner. The created mirror, in its current form, is intended to display information about the current weather conditions, weather forecast and the calendar synchronized with the chosen scheduler of the user. The calendar allows the user to display information about important events and activities planned for the day. These can be activities related to professional life, but also supporting routine home activities such as emptying waste containers, performing physical activities or taking medication. The mirror with the calendar displayed is shown in Figure 3.

A smart mirror interface displaying a digital calendar allowing the user to display information about important events and activities planned for the day.
The hardware design of the mirror utilizes semi-transparent glass with a bright computer monitor behind it. The monitor displays the information provided by the Raspberry Pi microcomputer. The software implementation is based on the MagicMirror2 package run under the control of the Raspberry Pi OS. MagicMirror2 is a modular, highly configurable open-source software offering a variety of extensions, apart from calendars and weather information also displaying messages, news, jokes and other interesting information. It can be integrated with a local home automation system enabling the customization of displayed information. Besides the informational functionalities, additional modules can also play music and videos and make the mirror interactive by voice or gesture recognition.
Tables have also been used as an interactive platform, for example to show pictures and identify touch or objects (Schwarz and Lobo, 2007). Instead of adding complex electronics into a table, Near Field Communication (NFC) technology offers another approach to create augmented content and functionality for a table or basically any piece of furniture or environment. In this example, a smart restaurant table prototype was developed by adding NFC stickers, operating at 13.56 MHz, to a tablecloth with a printed world map (Figure 4). Each tag represents specific language and country on the map. The NFC stickers can be read with NFC equipped mobile device. The idea is to use the mobile device for showing and reading aloud the content (restaurant menu) linked to the tags. Basically, after starting the app, the user puts the smartphone on the desired tag. The app displays the menu text in the language of the country that the phone is placed on the table and speaks the text aloud. Additionally high contrast and big font were used to help the user to see the menu.
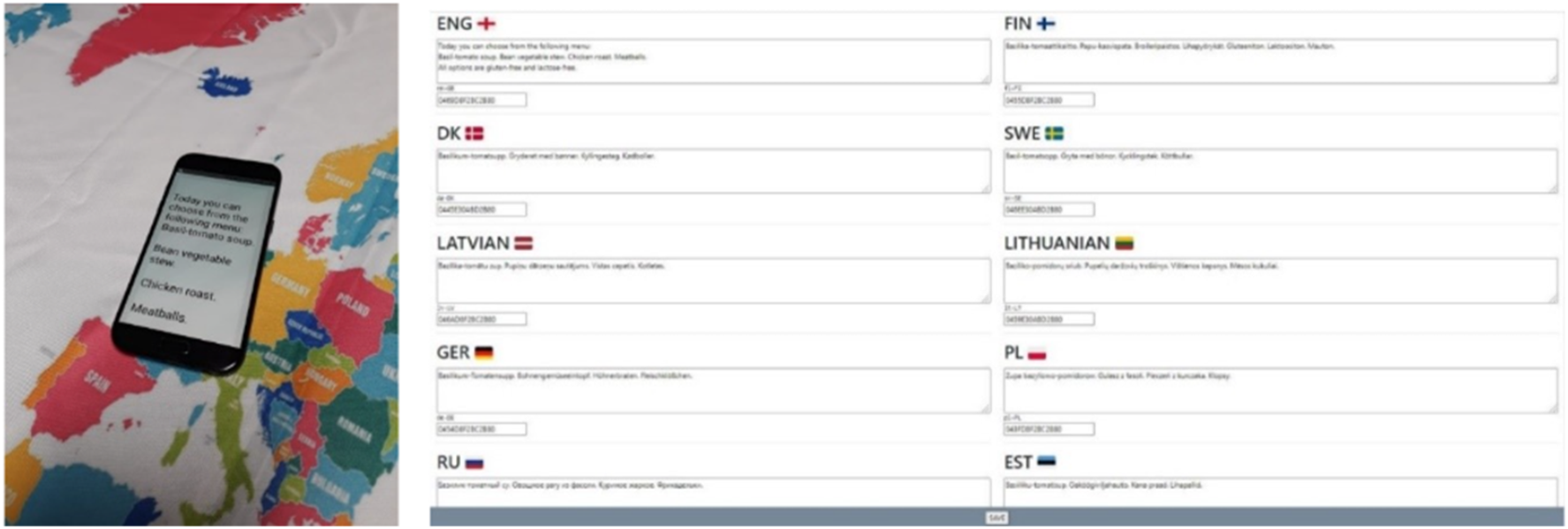
A smartphone placed on the English-language tag of the smart tablecloth displays the restaurant menu in English (left). The right image shows a screenshot of the associated website, where the content linked to each tag can be easily modified, enabling dynamic and multilingual menu updates.
The same technology can be modified for various other use cases. To enable modifiable tag content, a webpage was built to change the information linked to the tags. Tag ID code which is filled through the webpage page (Figure 4) is stored in the web server in JSON (JavaScript Object Notation) file with language information and the text content, which is displayed on the app and read aloud by the phone. This content can thus be easily modified and updated without any programming skills.
In Sakif et al. (2024), two basic NFC tags, operating at 13.56 MHz, were embedded in two corners of a wooden table. The table measures 1000 mm × 850 mm, and the surface is laminated. The table's interior is constructed from 25 mm thick chipboard underlayment, reinforced with high-pressure laminate. The table's sides feature 18 mm wide birch strips placed between the laminates and coated with Morrells antibacterial lacquer. The NFC tag locations are not marked on the tabletop, though they can be painted if needed.
The smart table functions as an integral component of a comprehensive system that also includes a cloud-based web user interface and the If This Then That (IFTTT) service (IFTTT - Automate Business & Home, 2025). A web user interface enables to define the functionalities associated with NFC tag readings, ensuring that the end-user's mobile interface remains as simple as possible, requiring only the tapping of tags to trigger different functions. The presented first version of the system offers several functionalities, including sending text messages, sending emails, making phone calls, playing music, and accessing either a coffee-making tutorial or useful contact information (Sakif et al., 2024).
The two smart table examples, the fabric-covered version and the wooden version, represent two implementations of the same prototype concept, each tailored slightly for a different use case. While they share the same core functionality, the differences in materials and design reflect adaptations to distinct application contexts.
In total 21 healthcare professionals and 18 end-users from Finland, United Kingdom, Norway, Portugal, Poland and Estonia responded to the survey. For professionals, the age range varied between 18–24 (3), 25–34 (2), 35–44 (7), 45–54 (8) to 55–64 (1). For end-users, the corresponding age range was: 25–34 (1), 35–44 (1), 45–54 (5), 55–64 (0) and over 65 (11). Among professionals, 17 were women and 4 men, while among end-users, 7 were women, 10 men and 1 of the non-gender group. Of the professional respondents, one said they were disabled, while six of the end-users were describing themselves as disabled. The results are presented in 3.1 and 3.2.
Quantitative results
The quantitative results can be found in Figures 5 and 6.
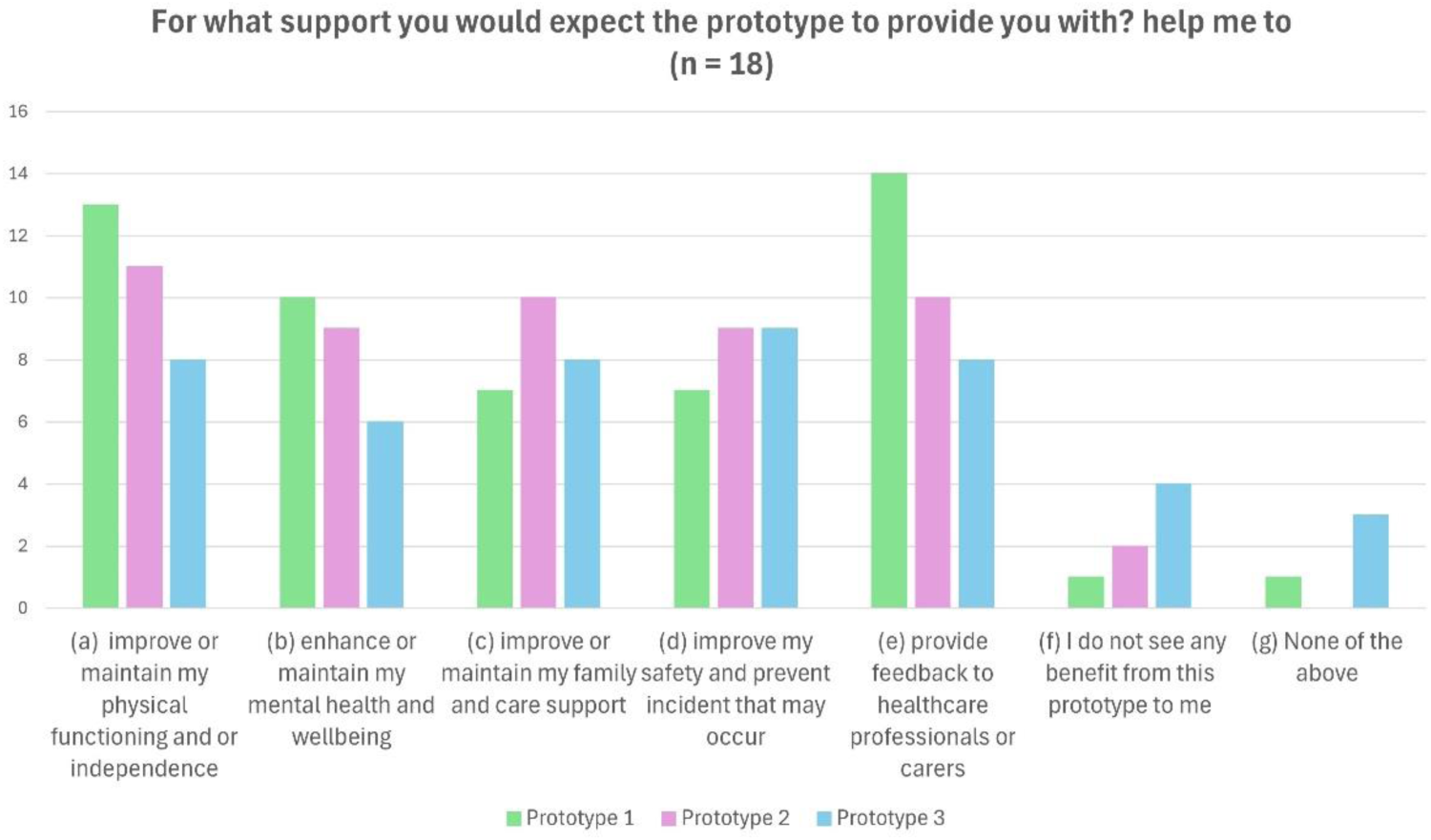
End-user (n = 18) expectations regarding the support provided by each of the prototypes.
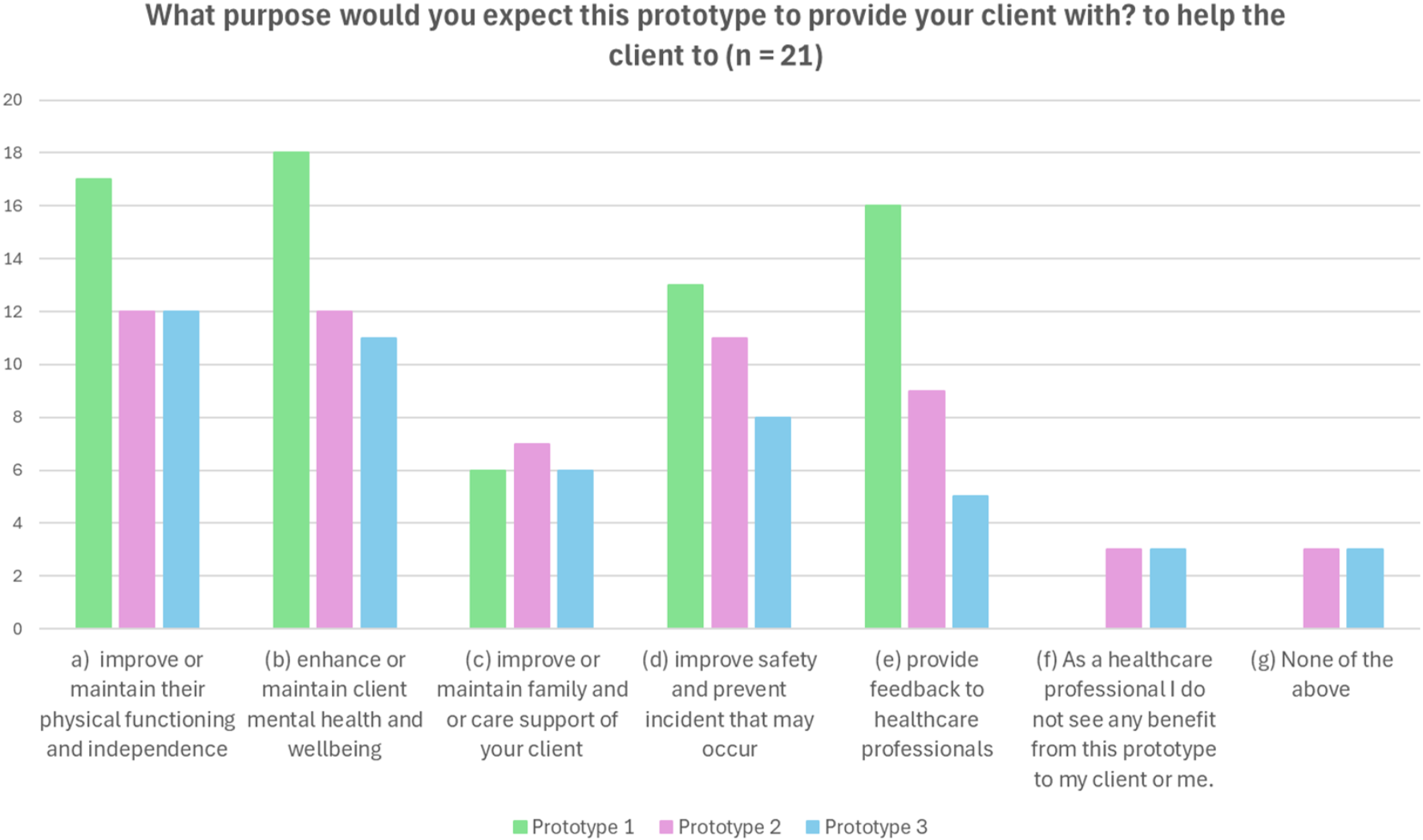
Responses from healthcare professionals (n = 21) regarding the expected benefits of each of the prototypes for their clients.
In general, smart chair prototype with exergames got the most positive results from the quantitative questions from both groups. The professionals as well as the end users saw especially benefits related to physical and mental abilities and supporting independence as well as the feedback for the care professionals. From the participants, 72% of end-users and 81% of professionals agreed that the smart chair improves or maintains their or their clients’ physical functioning and/or independence. By gender 83% of women and 64% of men agreed.
Similar benefits were also seen for the smart mirror. From the participants 61% of end-users and 57% of professionals agreed that the smart mirror improves or maintains their or their clients’ physical functioning and/or independence. By gender 67% of women and 50% of men agreed.
The end-users’ answers about the potential benefits were more evenly spread to different categories in the case of smart table. From the participants 44% of end-users and 57% of professionals agreed that the smart table improves or maintains their or their clients’ physical functioning and/or independence. By gender 50% of both women and men agreed on this. The table got the most modest quantitative results from both groups. One potential reason for this was the video, which already got some criticism in the pre-testing. The video was improved after the pre-tests, but there could still be some cumbersome aspects. Another reason might be the order of the prototypes. One of the end user respondents only replied to the smart chair related questions (presented 1st in the survey).
To assess whether there were statistically significant differences between the responses of end-users and professionals, chi-square tests of independence were conducted for each prototype. The tests assumed that the data consisted of categorical response frequencies, that categories were mutually exclusive, and that all expected cell frequencies were ≥5, which was met in each case. The null hypothesis in each case was that the distribution of perceived benefits was independent of respondent group. The results showed no significant differences between the two groups (smart chair: χ2 = 4,24, P = 0644; smart mirror: χ2 = 4,13, P = 0659; smart table: χ2 = 3,41, P = 0756), suggesting that professionals and end-users shared broadly similar views on the potential benefits of each prototype.
The care professionals found most use for the table related to improving physical and mental ability, whereas the end-users found improving safety as the clearest benefit. End-users also found potential benefits in improving physical well-being and independence as well as family/care support and providing feedback for care professionals.
The qualitative results give further insight into the potential of the prototypes and the answers of the respondents. The results highlight how different prototypes address the needs of end-users and healthcare professionals, as well as potential areas for improvement.
End users’ needs and perceived benefits of the prototypes
The responses from end-users reflected a broad spectrum of needs, ranging from physical and cognitive support to enhancing independence and daily functioning. The prototypes were generally seen as promising, although perceptions varied depending on the device and its intended use.
Smart chair: supporting mobility and cognitive engagement
End-users perceived the smart chair as a valuable tool for promoting physical activity and mobility (in total 10 comments). Many highlighted its potential to encourage movement, improve balance, and enhance posture. ‘It would encourage the user to move more and even improve the posture’. They found possibilities in measuring activities and abilities (in total 15 comments), these could be sitting time, movement data and sitting posture/symmetry.
Beyond physical benefits, respondents also emphasized the chair's cognitive and emotional impact, particularly in fostering engagement and enjoyment (in total six comments). Several participants noted that the chair's interactive elements could make physical activity more appealing, thereby reducing resistance to exercise. ‘It could help people with reduced mobility to exercise. Also, it could allow people to stay active and intellectual stimulated. It could improve the level of happiness and help to relax’.
The chair was also seen as a tool for enhancing independence, particularly for individuals with limited mobility. Some participants saw potential in integrating feedback mechanisms, such as alerts for poor posture or excessive inactivity, to further support autonomy.
Smart mirror: memory support and daily routine assistance
The smart mirror was primarily valued for its role in supporting memory and daily routines (in total eight comments). Participants frequently mentioned its usefulness in providing reminders for medication, appointments, and daily tasks, making it particularly relevant for older adults and individuals with mild cognitive impairments. ‘It could be used as a diary and memory aid’.
Additionally, some respondents noted the potential for the mirror to facilitate communication, whether through visual cues or interactive messaging. However, while some users found the mirror's functionality intuitive and useful, others suggested that it might not be suitable for individuals with advanced cognitive decline, as it could lead to confusion.
Smart table: accessibility and information delivery
The smart table was perceived as a versatile tool for improving accessibility, independence and providing essential information in an easy-to-use format (in total 6 comments). Respondents emphasized the potential benefits for individuals with speech or visual impairments, noting that the table could deliver verbal instructions or text-to-speech features. ‘It could give the information in the persons own language’, ‘It could help people with speech problems’.
Additionally, the table was seen as useful for assisting in daily tasks, particularly in meal preparation, guidance for how to use technology and medication management (in total 13 comments). Some respondents suggested that integrating barcode scanning could further enhance the table's ability to provide relevant information (in total five comments), for example the persońs well-being and daily activities.
Care professionals’ perspectives on the prototypes
Healthcare professionals generally recognized the potential clinical applications of the prototypes, particularly in rehabilitation, patient monitoring, and supporting daily activities. However, they also identified practical considerations and limitations that could influence implementation.
Smart chair: clinical applications and functional monitoring
Professionals largely echoed the end-users’ perspectives regarding the physical benefits of the smart chair (in total 11 comments). ‘I think that this chair could improve not only the motor skills like propriocetive and balance, but also the cognitive skills like attention/concentration’, ‘Playing by sitting is a great way to activate also senior who cannot stand as they do not get enough exercise’. Many viewed it as a valuable rehabilitation tool for encouraging movement and mobility maintenance. Additionally, professionals highlighted the potential for real-time health monitoring (in total 22 comments), emphasizing the importance of tracking sitting posture, weight distribution, and movement patterns. They suggested that such data could be instrumental in pressure ulcer prevention and identifying mobility-related risks.
Professionals identified benefits concerning mental and cognitive aspects (in total 11 comments). For example, using the smart chair could improve attention and concentration. Seven (n = 7) professionals highlighted the smart chaiŕs gaming attraction which they considered to be fun for end-users. ‘Smart chair could provide enjoyable moments for elderly as gamification can motivate all aged people’.
However, concerns were raised about data integration and usability. Some professionals emphasized the need for seamless data transfer to healthcare systems to ensure that information gathered by the chair could be effectively utilized.
Smart mirror: supporting independence and professional monitoring
Care professionals viewed the smart mirror as a potential tool for improving autonomy, particularly among individuals with mild memory impairments. The ability to provide structured reminders and guidance was seen as a valuable feature for maintaining daily routines (in total 11 comments). ‘It could provide important information such as reminders about upcoming nurse visits or visitors or give hints on what to wear considering the current weather conditions. It could also advice not to go out in the middle of the night’.
However, some professionals raised concerns about its suitability for individuals with advanced dementia or psychiatric conditions. They noted that a highly interactive mirror might cause confusion or anxiety, making it less useful (in total 6).
Smart table: information accessibility and communication tool
Healthcare professionals saw the smart table as a useful information hub that could support memory, communication, and daily task management (in total 6). They particularly emphasized its role in reminders for medication and appointments. ‘The table could “tell”’ about the schedule of the day and remind about important things such as appointments’.
While some professionals saw potential applications in assisted living environments, others expressed concerns about the usability of Radio Frequency IDentification (RFID)-based interactions, particularly for older adults who may struggle with technology adoption.
Suggested improvements for the prototypes
Participants provided many suggestions to improve usability and functionality, ensuring all prototypes are user-friendly. Both end-users (in total eight comments) and professionals (in total 13 comments) suggested improvements to the smart chair features and hardware. Different chair sizes, modifications to the features like headrests, adjustability, and sensors for armrest were highlighted. Professionals brought up practical aspects in use e.g. easier mobility with wheels and hygienic related features like antimicrobial and washable materials. The end-users’ improvement ideas related to the software were mostly about providing more versatile content and possibilities to control different kinds of content (in total six comments). More accurate movement tracking and real-time feedback were recommended to improve rehabilitation applications and respondents desired a wider range of exercise programmes and interactive content.
Concerning the smart mirror end-userś and professionalś improvement ideas differed from one another. Almost all improvement ideas of end-users were dealing with communication and interaction (in total seven comments.) like involving voice commands. Only two healthcare professionals mentioned improvement ideas for communication, as an ability to make video calls to family or caregivers. Healthcare professionals pointed out more diverse and tailored content (in total 3), like individualized information and user preferences. In addition, they mentioned visual and information design (in total three comments), these were colour contrasts, vision options and clearer information.
The technology of the smart table was questioned by end-users and care professionals. End-users mentioned that there already are existing technologies like QR-codes and other technologies that could work as well (in total four comments). Already existing technologies could enhance the usability of the smart table like barcode and active sensors. Healthcare professionals brought up the challenges with using the phone (in total three comments). Instead of using the phone they suggested using the tablet or operating by touch and getting the response as speech.
End-users and professionals identified different user groups to whom these technologies could be suitable for. The smart chair was seen to best serve seniors even with specific conditions related to health (neurological diseases) (n = 4) as it is easy to use. The benefits were seen for people with limitations in functional ability (n = 2), inactivity (n = 2) and back problems (n = 2). Professionals suggested that the chair could be used in care homes and also loaned for individuals’ home use. They also highlighted the requirement for the user to be capable of using simple technical devices and even with clear information and simple guiding the user might need a care professional to assist the use.
Concerning smart mirror end-userś response did not describe any specific user groups, except seniors were mentioned once. Several potential user groups were mentioned by professionals, like seniors, as well as people with mild memory impairment. However, the device wasńt seen suitable for people with advanced memory impairment (in total 5). Neither did end-users specify any particular user groups for the smart table, whereas health care professionals had concerns with memory impaired users (in total 6 comments). Only one healthcare professional pointed out that it would be useful for persons with memory impairment.
Discussion
The survey with demonstration videos was found a suitable tool in user need mapping in one of the iterations of the user-centered development process as it offers a way to involve users from wide geographic area. However, it should not be the only tool used. Instead, users should be seen as experts of their own lives and involved throughout the entire development process.
The survey results imply that the presented prototypes could help the users as well as health care professionals in multiple ways, but further development is needed. The respondents found multiple potential user groups for the smart chair prototype, such as seniors and disabled but also health care professionals to whom the chair would be a new tool. Especially seniors were often considered as the end-user in the open-ended answers. Potential use cases for the chair could be found in healthcare environments, but it could also be seen as a self-used product for home environments. Smart chair was the only prototype, which was not mentioned unsuitable for memory impaired users, while concerns were raised regarding the usability of the other prototypes. It should be noted that the smart chair was not explicitly stated to be suitable for users with memory impairments; instead, it was simply not identified as unsuitable, unlike the other prototypes. This lack of negative remarks may suggest a relative openness towards its use by this group, but it does not confirm its appropriateness. The smart table was considered potentially too complicated to use, as it requires certain technical skills: ‘For memory impaired people the use may be too complicated as it requires technical skills’. Similarly, the smart mirror was perceived as possibly frightening or confusing for these users. One participant noted, ‘Memory impaired persons might not recognize their own reflection in the mirror and might be anxious in case the mirror would talk to them, they might break the mirror’. In the case of the mirror, end-users’ responses did not strongly suggest any specific user groups for the mirror whereas care professionals had several thoughts about the potential user groups. Senior users were brought up as well as people with mild memory impairment. People with advanced memory impairment it was seen unsuitable. The end users did not specify any particular user groups for the smart table prototype in their answers whereas the healthcare professionals had concerns with (advanced) memory impaired users. The participants pointed out that the use of the prototype requires the participant's ability to use the phone.
Health monitoring, activation and motivation, entertainment as well as assisting in daily living were clearly seen as potential use cases for the prototypes. These are discussed further from the viewpoint of the research questions.
Many identified benefits of the smart chair were related to improvement of physical ability such as increasing and monitoring activity levels as well as movement, posture and balance. These benefits are in accordance with previous studies considering smart chair's potential. The previous studies found posture monitoring and health monitoring potential ways to encourage healthier sitting habits, to prevent musculoskeletal disorders as well as to inform care providers in case of abnormalities in well-being (Kumari et al., 2023; Odesola et al., 2024). However, the smart chair prototype introduced in this article also contained activation games. This may be one of the reasons why also mental and cognitive benefits were found such as attention training, brain activation and enjoyment. The data which was desired the chair to produce was about additional content such as exercising instructions and health guidance, as well as about measuring the activity and abilities. Data about weight and physiological measurements was also desired. To conclude, the prototype could serve multiple needs especially related to measuring and improving not only physical but also cognitive and mental well-being.
The benefits of the smart mirror, which were identified, were mostly to do with helping to remember activities in daily living such as giving reminders of activities and schedules. The mirror could also present some important data to users such as the weather. Some ideas were also to do with well-being related monitoring and communication. Information which end-user participants were hoping for the mirror to produce was mostly similar as in calendars but also information related to daily living and entertainment such as exercises, news, relaxation techniques and dietary recommendations.
Some previous studies also found smart mirrors as potential tools for displaying health metrics and reminders and thus helping users manage their wellness routines effectively and through interactive features they also to facilitate telehealth consultations, allowing users to connect with healthcare providers from home, enhancing accessibility (Maulana et al., 2024). However, this study also revealed much wider potential for the smart mirror.
The respondents identified benefits about the table, related especially to assisting in daily living such as providing info about ingredients of the meal or drink or proper dose of the medicine. The benefits of being able to access information with minimum physical and mental efforts were clearly illustrated in the participants’ answers such as giving information in the user-own-language or as speech. Data which was hoped the smart table to provide was versatile. Many comments were related to the users’ own needs for daily living and everyday life such as recipes in kitchen, tv-programmes of the day or any information in speech format. In earlier studies, identified benefits have been, e.g. enhanced Interaction when being integrated as part of smart home and adaptive functionality through which adjustments could be made for different users (Maulana et al., 2024). These features, however, were not highlighted in this study's respondents’ answers.
In addition to end-user benefits, benefits related to professional use of the prototypes were many. It is also worth noticing that end user benefits also have indirect benefits to care professionals through increased abilities and well-being as well as independence of their clients.
The smart chair benefits were related to professional use, especially additional motivation and information about rehabilitation and movements as well as pressure ulcer prevention. The information which was hoped for in professional use was mainly about health monitoring including (changes in) activity levels weight, balance and other physical abilities. The measurement data could be used to assess physical ability and the changes in it, but also to adjust training programmes. Also, more content to motivate the user by informing about the importance of physical activity or by providing joy to training was hoped for.
The potential benefits of the smart mirror were mostly about helping end-users in daily living such as reminders and memory support, which has indirect benefit to professionals. Also, communication with relatives and monitoring the clients’ performance in daily living were identified as potential use cases. Data needs from social and health care service and care work point of view were for example acknowledgement from the client about performed tasks, such as morning routines or doing the groceries.
The benefits and the data which was hoped for from the smart table prototype were almost all related to the data provided for the end-user, but respondents also brought up some perspectives related to data about their daily lives, such as drinking and eating rhythm. Also, information for care providers about important non-care related issues of the clients, such as insights into the client's preferences.
Smart furniture's potential in professional care has also been identified in earlier studies as they have potential to enhance health monitoring, security, convenience, and adaptability, thereby improving user experience and meeting specific needs in healthcare environments (Maulana et al., 2024).
Improvement ideas for the smart chair were about the chair design and features, measurement hardware as well as the software. Improvements related to the chair and the hardware included modular design (being able to change dimensions) and additional sensors to provide more detailed data, especially adding sensors to armrest. Also, material considerations arose (antimicrobial or water repellent material). Improvement ideas related to the software were mostly about providing more versatile content and possibilities to control different kinds of content such as more games and adding measurement results to the software. In clinical use data transfer to care professionals should be considered.
The most improvement ideas for the smart mirror were dealing with communication and interaction such as voice commands and introduce video conferencing or reporting if certain task is performed. Also, improvement ideas related to more diverse and tailored content such as giving individualized information or pointing out user preferences to care givers were mentioned. Some improvement ideas about visual and information design such as colour contrasts or clearer information were also brought up.
Many improvement ideas for the smart table were related to technology. Especially bar code/QR code capability was mentioned as a beneficial feature. Also, more extensive customization options for users to tailor the interactive features and content to their preferences, dietary restrictions, or cultural backgrounds were hoped for. The use of a phone to activate the content was seen potentially complicated for some users. In general, the technological aspects of the table received the most commentary and criticism.
Previous studies have also highlighted that privacy concerns are significant when using smart home health technologies for caregiving, emphasizing the need to address ethical and social implications to foster trust and acceptance among users regarding health monitoring features in smart furniture (Tian et al., 2024). This was not pointed out in the responses but is an important feature also considering the further development of the prototypes.
In general, in healthcare and ambient assisted living contexts, the protection of personal and sensitive data is paramount. Smart furniture prototypes used for care purposes are under the medical device regulation and should be developed accordingly. The prototypes must comply with data protection regulations such as the GDPR in the EU. This includes ensuring that all personal data is processed lawfully, transparently, and for a specific purpose. In practice, data collected by the prototypes must be encrypted during transmission and storage to prevent unauthorized access. Access controls and authentication mechanisms (e.g. secure logins or user-specific permissions) are also essential to ensure that only authorized personnel or users can view or manage data. In user-centered development, clear communication about data ownership and usage is crucial – users must be informed of what data is collected, who can access it, and how it will be used. In future development phases, data minimization principles will be applied to collect only what is necessary, and local data processing (e.g. on-device analytics) will be considered to reduce the need for transferring sensitive information. Privacy-by-design and security-by-design approaches will be integrated into future iterations to ensure that personal data management aligns with both ethical standards and regulatory requirements (Preece, 2019).
Design for somebody as a co-design approach
Based on the development steps so far, the DfS approach has proven to be suitable for ‘from small to all’ development. In general, the results from the survey provided important perspectives for the second level iteration round DfS process. The results form the basis for modular designing of the refined prototypes before the third level iteration round with large number of testees, which is our future work. Based on previous research (Merilampi et al., 2020) and the results of this study, the DfS process was formulated as a model described in Figure 7.
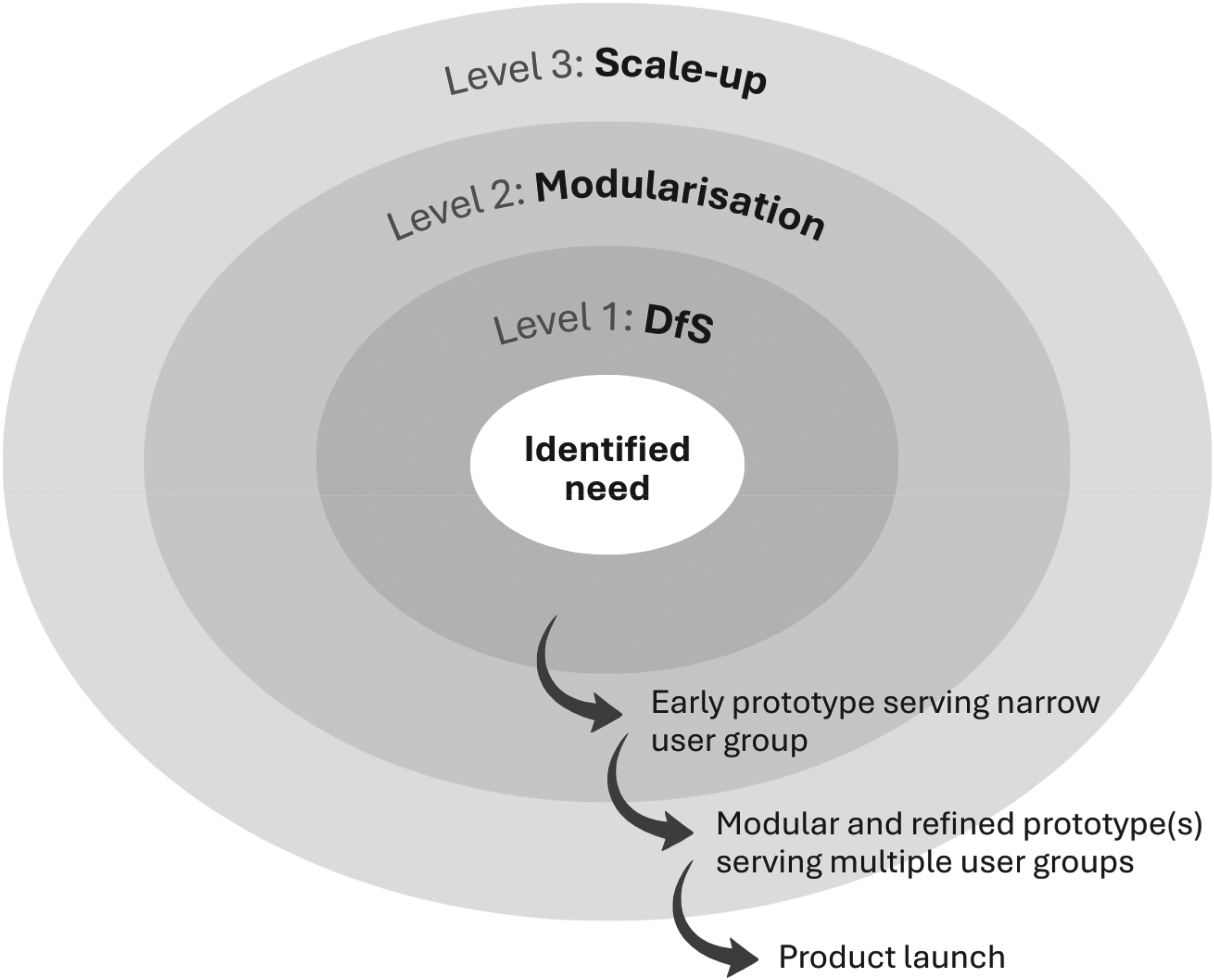
DfS model for co-design.
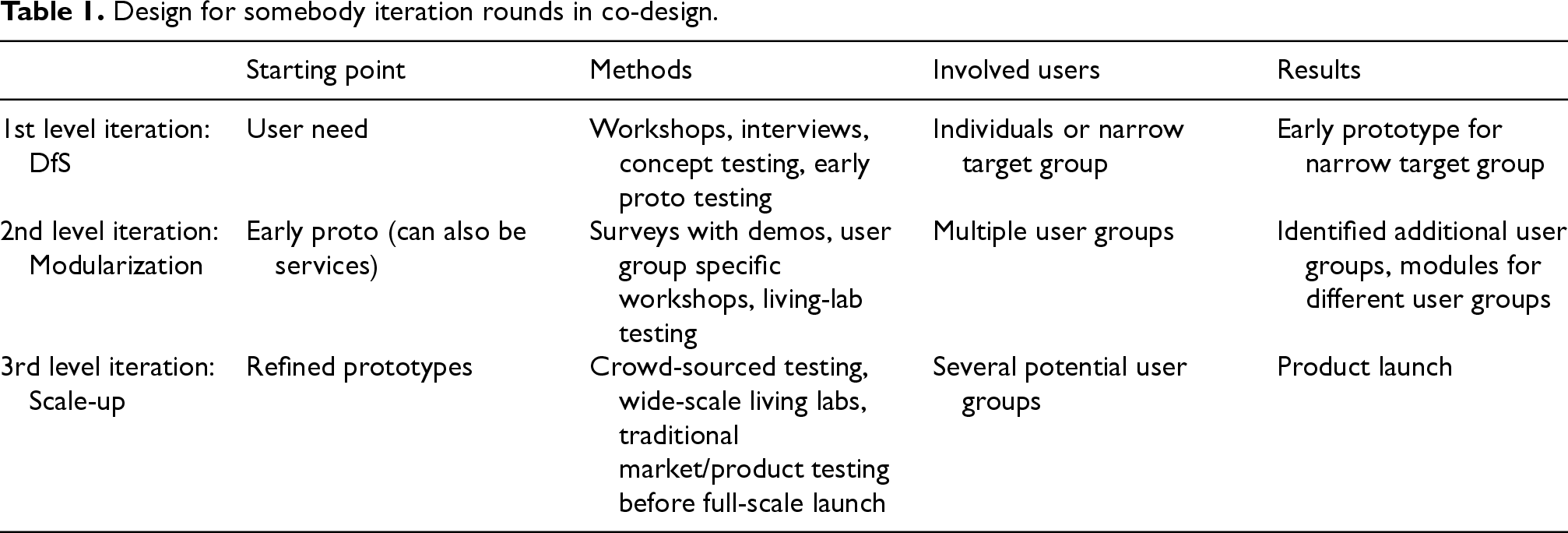
In the first level iteration, the focus of the development is on individual users, and the emphasis is in the real user need visualization with a concrete early prototype. In this phase the users are very heavily involved into the process. However, this paper described the first steps of the second level iteration, in which the focus shifts towards widening the potential users and formulating the modules, which allows the prototype to serve wider set of user groups. The DfS iteration rounds, and their characteristics are further described in Table 1. In this paper a secondary user group, health care professionals, was considered in addition to the primary users. However, in the second level iteration the role of the involved users is different, and the involvement is not as thorough as in the first level. Although the users should be intensively involved throughout the process, the higher the number of the participants, the less in-deft user perspective can be achieved. This is why in the second level the methodology and the aim of the development differs from the first level, the focus being on the fine-tuning and modularization of the prototype for different user groups. This study identified various additional functionalities for the prototypes, if the prototypes were utilized in professional care settings. These requirements can be in the future formed as the modules of the prototypes. Our future work is also to further finetune the prototypes and the modules after which they should be tested with large number of users. This ‘mass-testing’ level aims at scaling-up the modular prototypes which would finally lead to product launch. Even after the product launch, the products should be further tested. It is worth to notice that each iteration level provides information and feedback not only for the product under development, but also ideas for other prototypes and insights about user needs.
Design for somebody iteration rounds in co-design.
In general, many potential benefits as well as improvement ideas were identified in this study. All prototypes were found useful in many ways. This is a positive result considering further development and research on smart furniture. However, the respondents were all voluntary and potentially open-minded for smart technologies. This may cause some bias, i.e. too positive results.
It should be noted that the video quality may have influenced participants’ perceptions, particularly in the case of the smart table. The prototype's functionalities relied on interaction with a smartphone, which may not have been clearly conveyed through the video. Future studies should ensure higher-quality and more detailed demonstrations to minimize misunderstandings and support more accurate feedback.
A greater number of respondents is needed to draw conclusive conclusions. The relatively small sample size (n = 39), as well as the diversity of the participants’ backgrounds across six different countries, limits the generalizability of the findings. Although the sample included a range of ages, genders, and both healthcare professionals and end-users, the representation within each subgroup remains limited. For example, the number of respondents in some age categories was very small, and only a few participants identified as disabled. These limitations suggest that the results should be interpreted with caution and may not fully reflect the views or experiences of the wider population. A more extensive sample would be necessary to ensure broader applicability and to explore potential differences between demographic subgroups in more detail.
Even though the respondents were from different European countries, there were no country specific needs identified. Furthermore, the professional background and specific work tasks of the participants remain unknown. Most end-users were seniors whereas the professionals were working-aged. The gender distribution was different among end-users and among professionals. This was not clearly seen in the results, which were relatively consistent between the respondents.
Future work
The findings highlight several concrete directions for future work. The smart chair demonstrated the strongest potential for both healthcare and home settings and was the only prototype not perceived as unsuitable for users with memory impairments. This suggests it could be further developed for people with mild to moderate cognitive decline, particularly through enhanced activation and monitoring functionalities. For the smart mirror, future research could explore how such mirror-based technologies can support daily routines, especially through reminders or prompts. The smart table raised concerns due to its reliance on smartphone use, making it potentially unsuitable for users with advanced memory issues. Future development should focus on simplifying interaction, for example through voice control or other accessible interfaces. Overall, further work should refine each prototype based on the achieved insights, test them with clearly defined user groups, and involve users in co-design to ensure relevance and usability in real-world contexts.
Conclusions
Co-designing is essential in smart furniture development. This study explored the potential benefits and further development needs of three smart furniture prototypes – smart chair, smart mirror, and smart table – by engaging healthcare professionals and end-users from multiple European countries in an online survey. The findings confirm that these prototypes could enhance safety, comfort, and efficiency in healthcare environments, supporting both caregivers and clients. Key use cases identified include health monitoring, activation and motivation, entertainment, and assistance in daily living, with seniors frequently mentioned as primary end-users.
Despite the positive feedback, further development is required to refine functionalities, improve usability, and ensure seamless integration into healthcare settings. The study also highlights the value of online surveys with demonstration videos as a practical approach for gathering user insights during the iterative development of smart solutions. Future research should focus on expanding the participant base, conducting real-world trials, and exploring interdisciplinary collaborations to optimize the design and implementation of smart furniture in diverse care environments.
Footnotes
Acknowledgments
This research was carried out as part of Reliable Electronics for Tomorrow's Active Systems (ReACTIVE Too) project. The project is funded by the Marie Skłodowska-Curie Research and Innovation Staff Exchange Programme of the European Union under Grant Agreement No 871163.
ORCID iDs
Ethical considerations
The study followed established ethical guidelines for research involving human participants. All participants received written information about the studýs aims, procedures, and data protection practices prior to participation. Informed consent was obtained from, all participants before they completed the online survey. Participation was voluntary, and participants could withdraw at any point without consequences. Ethical approval was obtained for the study from the Faculty of Science and Engineering Ethics Committee of the University of Wolverhampton (LSEC/2022-23/FM/004).
Confidentiality and anonymity of data within the research process were achieved by coding participants. Any collected data about participants were stored in a password-protected computer/encrypted laptops and online (on the University's database) protected by passwords according to the GDPR principles.
Given the exploratory and low-risk nature of the study, which focused on user needs and perceptions of non-invasive smart furniture technologies, the research posed minimal ethical risks to participants.
The video material was created by the research team specifically for research purposes to illustrate the prototypes and their potential use. No external participants appeared in the videos.
Consent to participate
Participation in this study was voluntary, and respondents accessed the online survey after reviewing the privacy statement and providing their informed consent by actively selecting the approval option.
Author contributions
Conceptualization, S.M., K.T., S-M.P. & J.V.; methodology, J.H., T.J., F.T. & H.M; software K.T., A.K. & P.C.; validation M.L. & J.V.; formal analysis, S.M., M.L., J.H. & T.J.; writing, all authors. All authors have read and agreed to the submitted version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are grateful for the financial support of the European Research Agency through the EU Horizon 2020 MSCA RISE Project, ReACTIVE Too, Grant Agreement No 871163.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.