
Abstract
Purpose
This study aimed to assess pediatric rehabilitation medicine (PRM) physicians’ experiences with disability education and opinions regarding a structured curriculum during graduate medical education.
Methods
This was a mixed-methods, descriptive survey study of current PRM physicians including PRM attendings, PRM fellows, and Pediatrics/Physical Medicine and Rehabilitation residents. Respondents completed an electronic survey via REDCap. Survey topics included prior disability education, current institutional disability education, and future development of formal disability education. Responses were de-identified. Data was analyzed with descriptive statistics and thematic analysis.
Results
Sixty-five PRM physicians completed the survey. Four themes emerged to describe disability education of PRM physicians: 1) There is a lack of structured disability education, 2) PRM physicians are leaders in caring for children with disabilities and should receive formal education, 3) Patient-centered experiences are considered a key part of the disability curricula, 4) Disability education can aid PRM physicians in advocacy.
Conclusion
Current disability educational experiences are variable amongst PRM physicians, and there is no standardized approach. The majority of PRM physicians surveyed in this study perceived current disability education practices as inadequate and were in favor of a formal curriculum.
Introduction
Approximately 19% of Americans have a disability, including 17% of children aged 3–17 years.1,2 Disability has been defined by the World Health Organization as an umbrella term for impairments, activity limitations, and participation restrictions. 3 It is a complex concept that involves the interaction between the individual, their health condition, their environment, and other personal factors. Each individual lives with a unique disability experience, and providers should be able to demonstrate comfort and competence when interacting with this population. 3 It is well documented that individuals with disabilities experience disparities in screening and preventive services, cancer diagnosis and treatment, reproductive and pregnancy care, communication with healthcare professionals, and satisfaction with care.1,4 While the Americans with Disabilities Act was enacted more than 30 years ago, physicians across specialties continue to report decreased confidence in taking care of individuals with disabilities. Recent surveys reveal only 40.7% of physicians across multiple different specialties were “very confident” about being able to provide the same quality of care to disabled patients as non-disabled patients. 4 This lack of confidence is thought to stem in part from inadequate education and training to prepare them to care for patients with disabilities.1,3,5
This discomfort is present early in medical education, as evidenced by one survey in which 80% of medical students reported inadequate disability education. They reported feeling less comfortable obtaining a history, performing a physical exam, and establishing a differential diagnosis when working with individuals with disability. 6 As recently as 2015, only 52% of surveyed medical school deans reported having a disability awareness program, defined as “a program that provides education about living with a disability that is not limited to teaching about the medical/biological aspects of disability but extends to education on the psychosocial aspects of living with a disability”. 7 Of those institutions who had structured disability education, students spent an average of just 10 h over four years on disability-related topics.3,7,8 The Disability Education Network and the Disability Education Toolkit are two current efforts to create readily available disability modules for medical students. 9 In recent years, the Liaison Committee on Medical Education, the accreditation body for medical schools in the United States, has begun to target this area of education. Disability is now included under the umbrella of healthcare disparities, and accredited medical schools are required to provide education regarding healthcare disparities and inequities. 10 While this is a positive change, the content and format of this education remain variable and may be insufficient to replace dedicated education offered at a more advanced stage of medical training.
However, graduate medical education programs (i.e., residency and fellowship training) have also been limited in the disability education they provide. Emergency Medicine program directors reported only 43% of training programs offer disability-focused content, which averages 1.5 total h annually. 11 Similarly, only 28.9% of Internal Medicine residency programs reported offering disability-focused curricula and, of those, only 61.5% made this education mandatory for their residents. These primary care program directors felt both internists and their own residents (88.3% and 77.8%, respectively) were inadequately educated in the care of people with disabilities. 12
There is limited data on this topic regarding Physical Medicine and Rehabilitation (PM&R) residency programs and Pediatric Rehabilitation Medicine (PRM) fellowship programs. All PRM physicians participate in general PM&R training, which is focused on the management of rehabilitation medicine conditions in adults. PRM physicians receive additional specialized education in the management of rehabilitation of children and adolescents, through either a PRM fellowship program or participation in a pediatrics/PM&R residency program. Therefore, education offered through both PM&R residency programs and PRM fellowship programs are pertinent to training a PRM physician.
A recent survey of PM&R program directors revealed that 58% of residencies included a disability awareness program; however, the response rate was only 47% of programs. 13 The only other published study specific to PM&R explored the impact of a one-day disability training in residency. 14 The Accreditation Council for Graduate Medical Education (ACGME) guidelines for PM&R residents do state that “Residents must demonstrate competence in the evaluation and management of patients with physical and/or cognitive impairments, disabilities, and functional limitations” but do not delineate how programs should accomplish this. 15
PRM fellowship program guidelines also do not specifically require education on disability. ACGME guidelines for PRM fellowship programs state that fellows “must demonstrate competence in caring for individuals with disabilities”; 16 however, education beyond clinical management such as knowledge of disability culture, history, legislation, and advocacy are not addressed. It has been recommended that medical education should include more training about disability, including disability cultural competence and etiquette. 4 PRM physicians are well-poised to serve as leaders to advance the health and functioning of children with disabilities 17 and are in a unique role to promote, design, and participate in disability education initiatives across the medical education timeline.
To the best of the authors’ knowledge, there is no prior study exploring experiences with disability education amongst PRM physicians. The purposes of this study were to determine the amount and format of formal education on disability received by PRM physicians. Additionally, this paper aimed to gather PRM physician opinions related to formal education on disability for PRM physicians.
Materials and methods
Study participants and procedure
A survey was distributed to PRM attendings, PRM fellows, and Pediatrics/PM&R residents across the United States. An email list was compiled based on information obtained from PRM social media channels, PRM residency and fellowship program director listservs, and personal networking contacts. The survey was distributed to 258 individuals from multiple different institutions and geographic regions; however, some of these are likely to represent duplicate or invalid email addresses. Survey responses were collected from August 2022 until September 2023. Several reminders to complete the survey were distributed throughout the timespan. All responses were anonymous. A total of 65 responses were obtained with an estimated response rate of 25.19%. Exclusion criteria included not practicing or training in the field of PRM. Data collection occurred via a survey (see Supplementary Material) that included both multiple choice and open-ended questions and was administered online via REDCap, a HIPAA compliant online database often used in healthcare settings. Respondents were informed that completion of the survey implied consent. Individual surveys were de-identified, and data was stored on a password protected site. The study was reviewed and approved by the Institutional Review Board of Cincinnati Children's Hospital Medical Center. The project was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH), under award number 1UM1TR005265. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. 18
Survey design
A novel survey developed by the authors aimed to assess the respondents’ demographic data, personal disability education history, disability education available at their current institution, and opinions on the development of formal disability education courses and curricula. This survey was created by three PRM physicians at one institution. It was reviewed by these three physicians for clarity and content prior to dissemination but was not otherwise validated or tested. This mixed-methods survey study included quantitative questions (i.e., multiple choice) as well as qualitative questions with options to provide free text responses. To the authors’ knowledge, a similar type of survey has not been created, nor has this survey been utilized in previous studies.
The terms “disability,” “disability topics,” and “formal education” were defined. “Disability” and “disability topics” were used in reference to disability history, models of disability, disability culture, disability legislation, disability humility, education on how to interact with those with disability, quality of life in those with disability, etc. These terms did not refer to a pathology-specific impairment or activity limitation. “Formal education” referred to structured education with clearly outlined objectives. Specific examples included didactics/lectures, standardized patient encounters with individuals with disabilities, and structured community outings for the purpose of disability exposure and education. It did not refer to daily patient encounters with individuals with disabilities.
Data analysis
Quantitative data were analyzed with descriptive statistics, and results were reported in aggregate without identification of individual respondents. Mean and standard deviations were calculated when appropriate. Qualitative data were analyzed using thematic analysis and grounded theory framework. Three reviewers individually reviewed narrative data and identified codes. Individual codes were reviewed by the group for similarities and differences. Qualitative and quantitative data were then triangulated and placed into themes.19,20
Results
Demographics
Sixty-five surveys were completed, and demographics of respondents can be seen in Table 1. Respondents’ individual experiences with disability can be seen in Figure 1. The majority (54.8%) indicated personal experience with disability, in themselves (6.3%), in a close family member or friend (28.1%), or multiple of the above (20.4%). Forty-two percent indicated they do not have a disability themselves, nor do they have a close family member or friend with a disability.
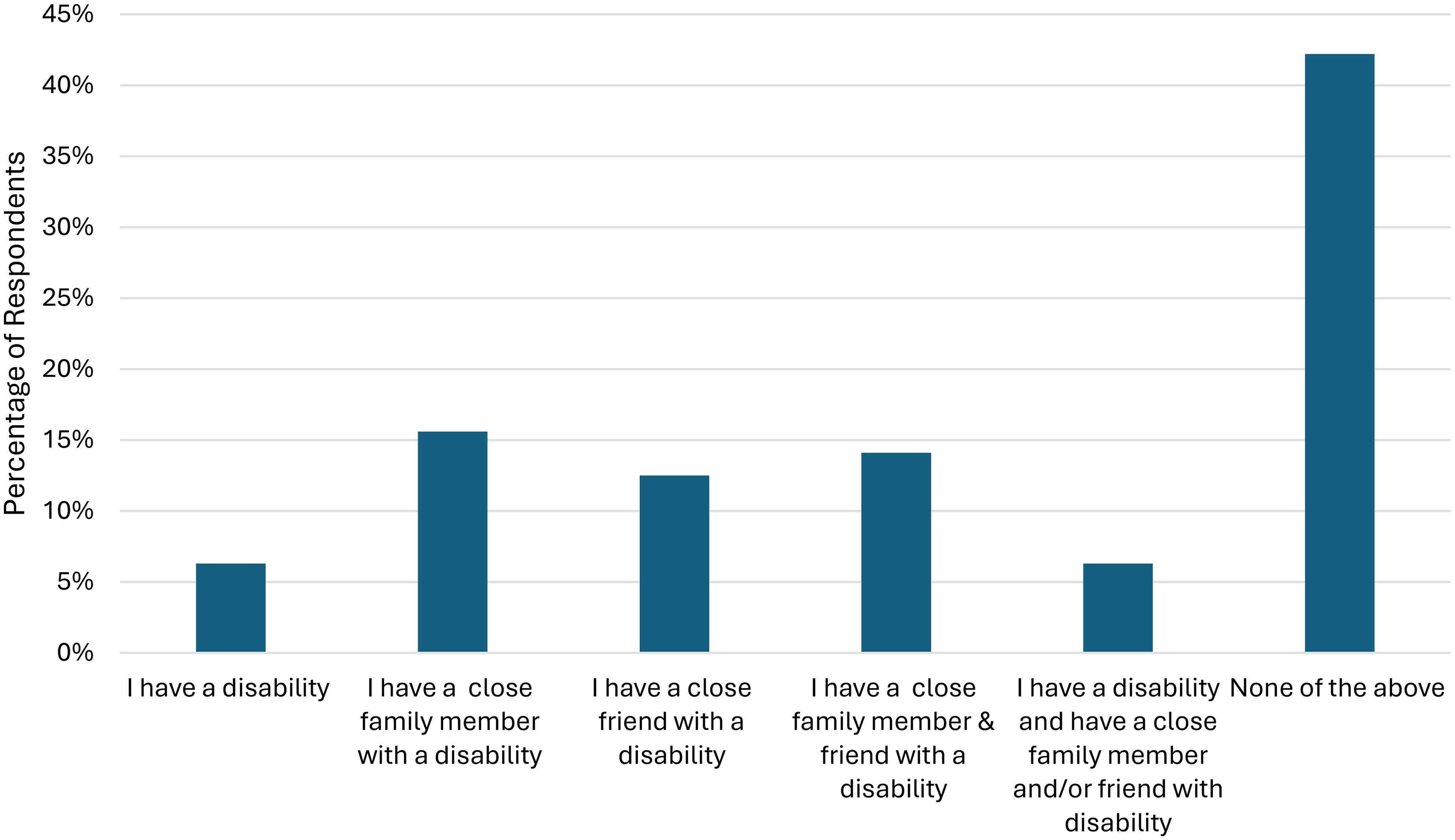
PRM physicians’ personal experience with disability.
Respondent demographics.
PM&R: Physical Medicine and Rehabilitation; PRM: Pediatric Rehabilitation Medicine
Themes
Quantitative and qualitative data were triangulated, and four themes emerged regarding the current state of and recommendations for disability education.
PRM physicians reported a large variability in disability educational experiences, time spent completing formal education, current institutional offerings, and individual approaches to seeking out disability education.
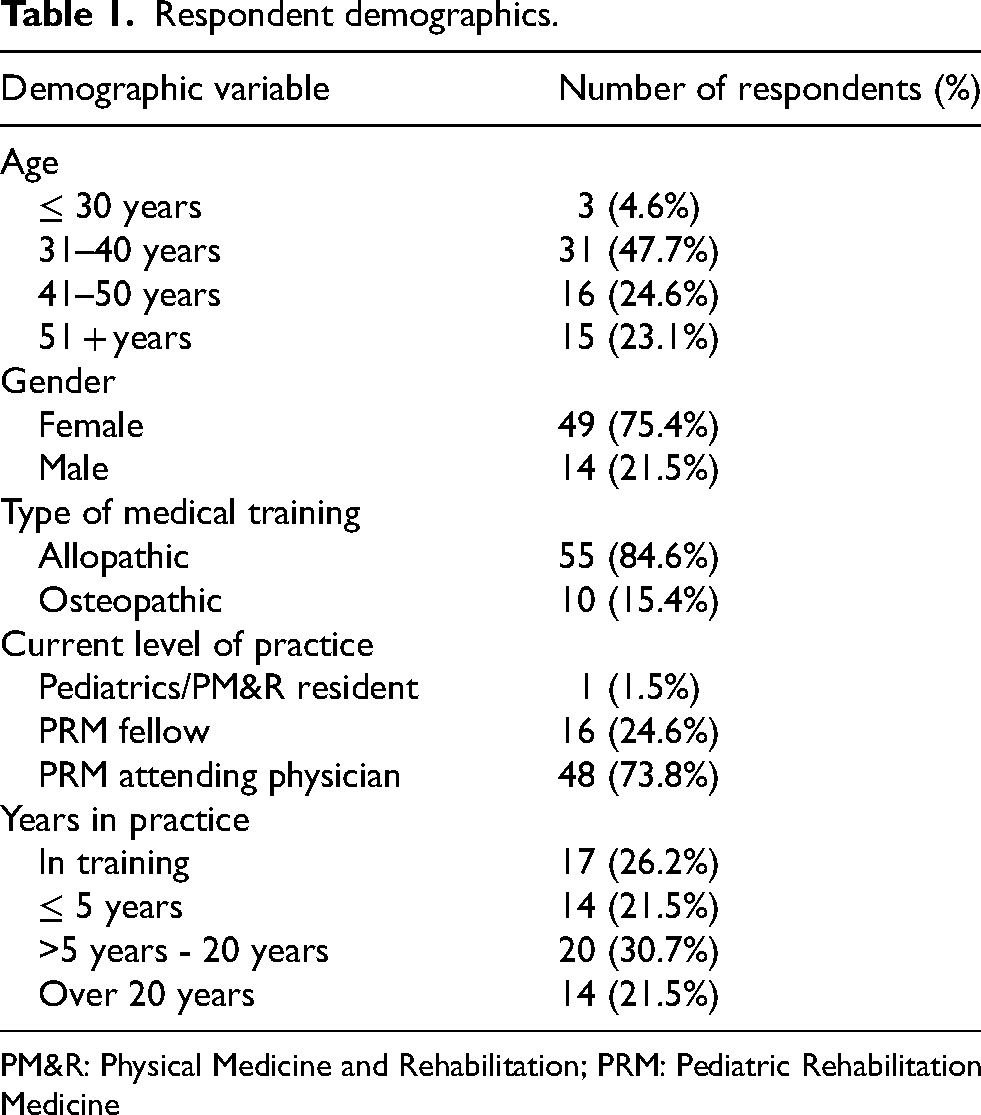
PRM physicians identified a variety of experiences with disability education before and during graduate medical education (Figure 2). While didactic lectures were the most reported experience across all periods of time, a large percentage of respondents reported not receiving any formal disability education. Other unique experiences included following individuals with disability on social media, participation in volunteer activities such as adaptive sports and summer camps, independent reading of news articles, listening to podcasts, working with advocacy groups, and Leadership Education in Neurodevelopmental and related Disabilities (LEND) training, which is federally funded training that focuses on improved provider education and health for those with developmental disabilities.
Format and timing of disability education received.
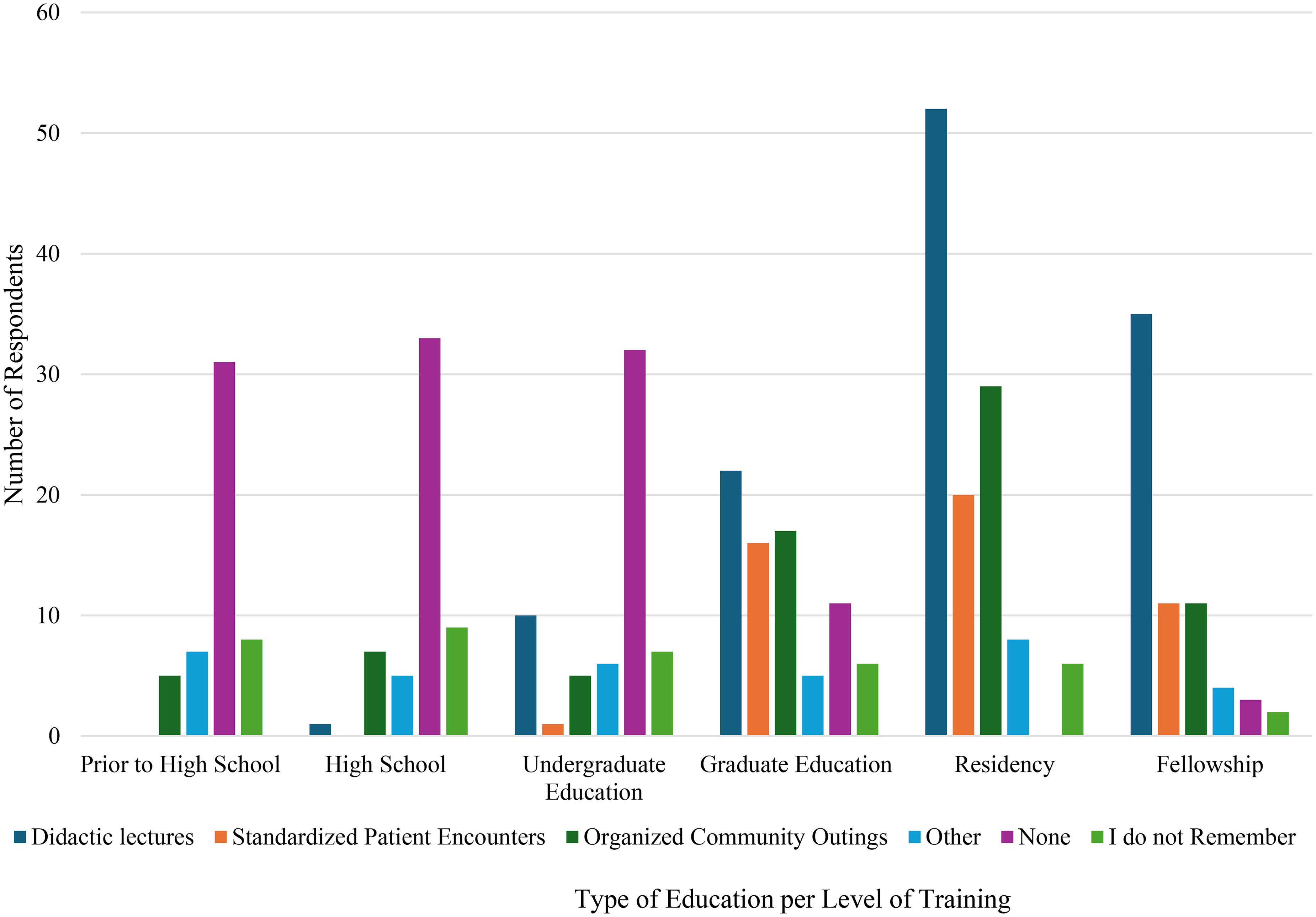
When considering only formalized disability education, the time spent was variable as well (Figure 3). Amongst all survey respondents, the largest percentage of individuals indicated spending under 10 h on this education, while others reported having spent over 100 h. Amongst only residents and fellows, the largest percentage of individuals reported 10–20 h of education whereas the largest percentage of faculty reported spending under 10 h on formal disability education. A similar percentage of both the trainee group and the faculty group reported spending over 100 h on education (Figure 4).
Lifetime hours of formal education on disability.
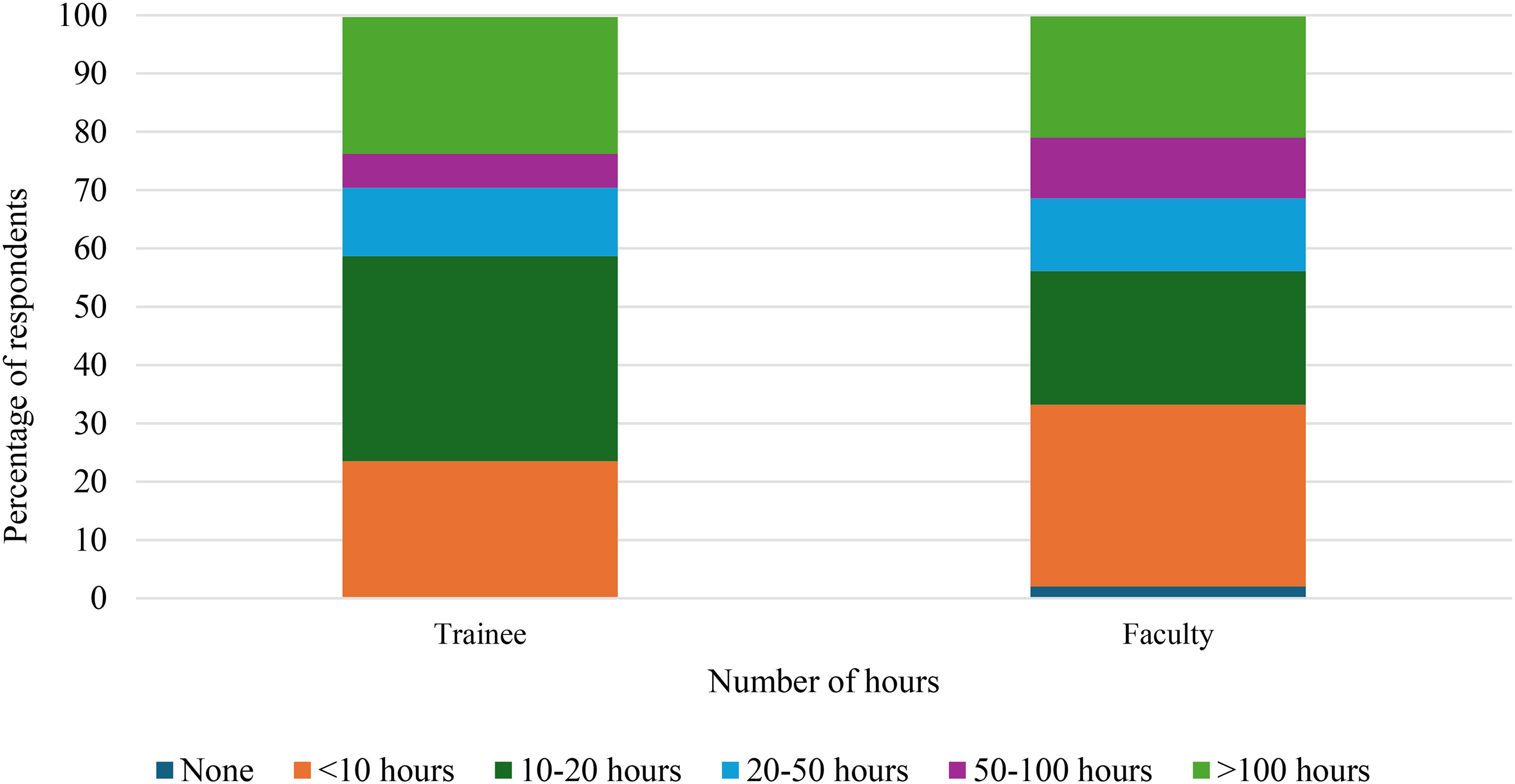
Lifetime hours of formal education on disability for trainee versus attending.
Respondents who were associated with residency or fellowship programs were asked what their current institution's training programs provide related to disability education. The majority reported that training programs did currently offer formal disability education, and specifics can be seen in Figure 5. However, many respondents independently sought out disability education. This was done most often at the levels of attending physician (46.9%, n = 30) and resident (48.4%, n = 31) followed by medical student (39.1%, n = 25) and fellow (32.8%, n = 21). Only 12.5% (n = 8) reported that they did not independently seek out education on disability.
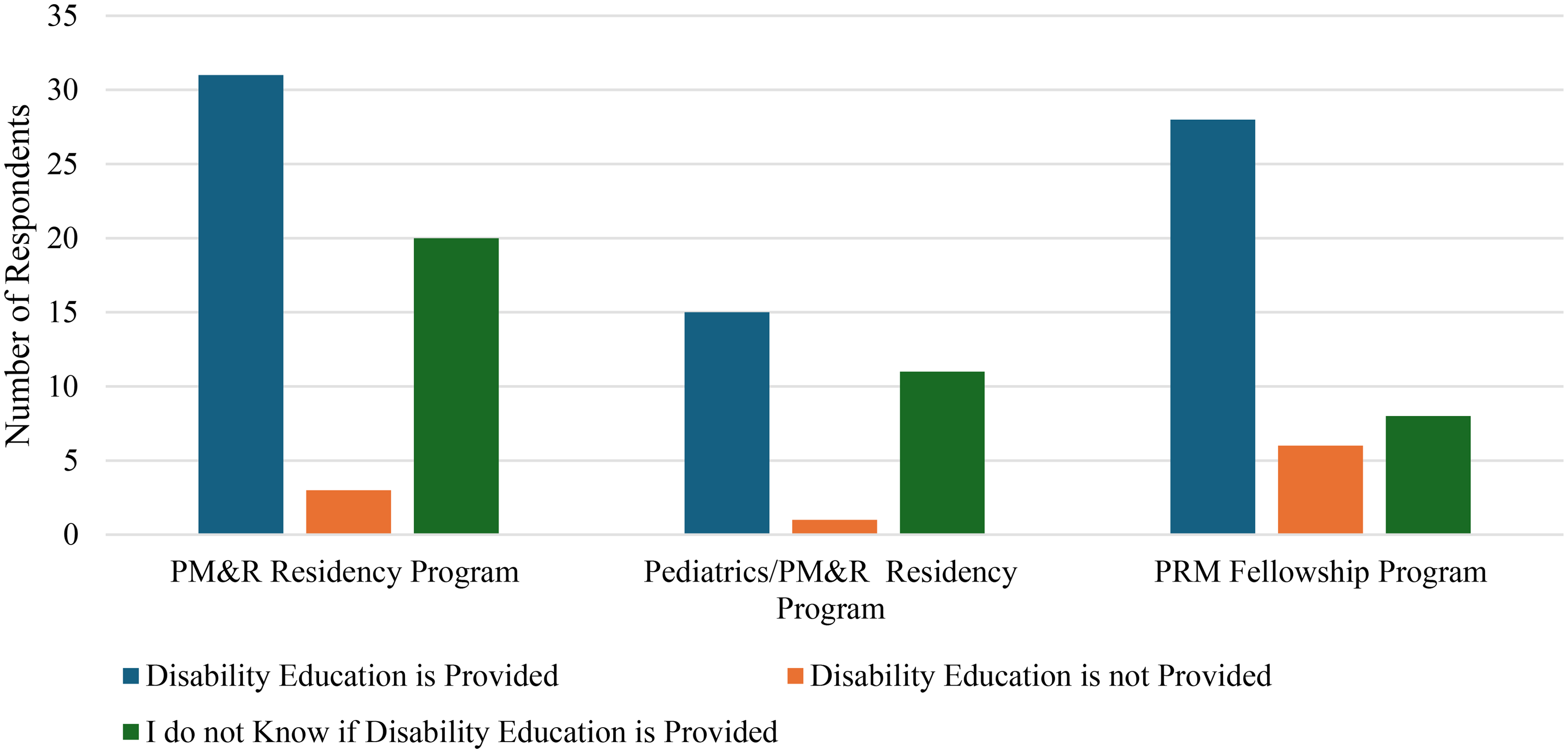
Current disability education in associated graduate medical education programs.
Many experiences sought out by PRM physicians were a form of informal education and did not follow a structured curriculum. Several survey respondents expressed concern with the shortcomings of informal education when not accompanied by formalized education: 76.6% (n = 49) of respondents felt “informal” disability education (i.e., knowledge gained during daily patient encounters) is not sufficient for PRM trainees. “It is hard to see the whole picture when you only learn about things informally.” “I think that knowledge is invaluable as a physiatrist, but it should be tied back to formal education to ensure everyone is learning relevant and important topics to help future patients.” “Informal education is critical to developing as a physician, but it relies too heavily on the attending physician's knowledge and desire to teach, and does not have a way to ensure all the critical topics are covered during training.”
The majority of respondents (98.5%, n = 64) felt that PM&R residency programs should be required to provide formal education on disability and likewise regarding PRM training programs (86.2%, n = 56). Of those who felt disability education should be required, respondents felt 20 h or less across residency and fellowship would be sufficient. “We are the experts in disability, and it should be part of any physiatrists [sic] education.” “We are the experts on the subject matter and should lead this educational initiative.” “This is the heart of PM&R.” “PRM is a natural leader that other specialists can and likely will look to for leadership in taking care of those with disabilities.”
To address the lack of standard education, respondents suggested disability education be required through the ACGME and a focus of sessions at major conferences. Very few respondents (under 4%) anticipated lack of interest in disability education to be a concern for either the PRM or PM&R training programs. All respondents felt there is a need for formal education; however, the two largest barriers to curricula development for both PM&R residency programs and PRM training programs were felt to be developing content and time constraints.
Respondents indicated that individuals with disabilities should be highly integrated into disability education programs. When asked about the recommended format for formal curricula, the majority 61.9% (n = 39) of respondents recommended a variety of delivery methods including didactic lectures, standardized patient encounters, and organized community outings (Figure 6). The free text comments overwhelmingly indicated the importance of didactic content led by those with disabilities, community outings, and interaction with parents/caregivers of those with disabilities. “There is room for significant didactic content that centers disabled voices.” “There should be patient centered experiences and presentations rather than just theoretical demonstrations.” “…As an important part of the movement says, ‘nothing about us without us’.” “…there should be experiential components as well, such as participation in/attendance of support groups and/or adaptive activities (such as summer camps etc).”
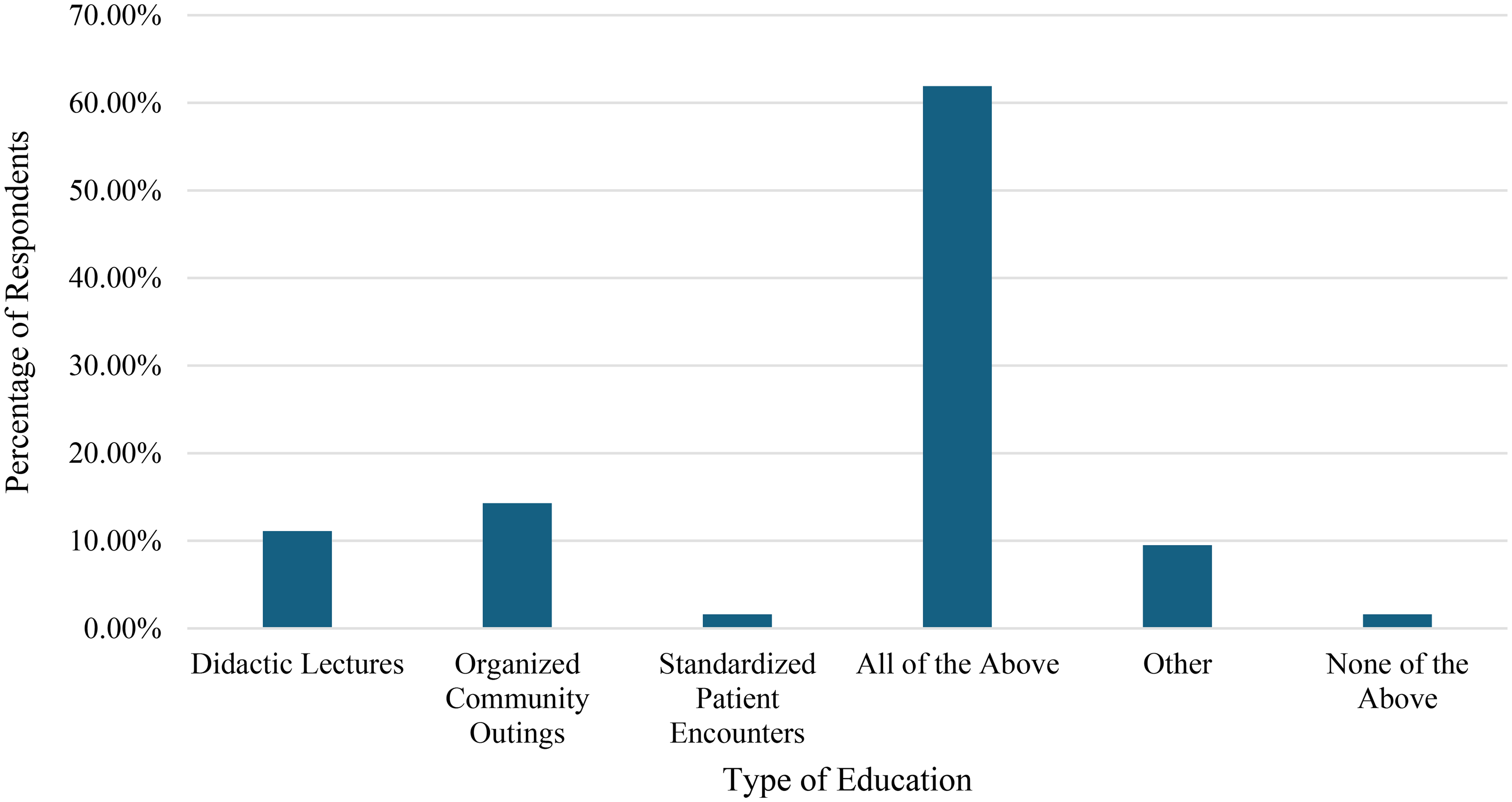
Recommended educational content.
Many PRM physicians view advocacy as a key component of their role in caring for children with disabilities. While a specific survey question was not asked related to this topic, a consistent theme among the survey respondents via open text boxes was that knowledge regarding disability history, disability legislation, and the lived experience is crucial for PRM physicians to be effective advocates. “Advocating for disabled patients is (should be?) central to our role as rehab physicians. This is a heavy lift and deserves more formal education.” “Part of being a PRM physician is to be an advocate for the children/adults we care for. You can not do that without a good understanding of disability rights and its history.” “We are not only physicians but advocates and need a comprehensive education to be the best advocates we can.” “As integral players in the clinical care and advocacy for persons with disabilities, physiatrists should have ample exposure for formal education regarding disability.”
Discussion
Despite being well-poised to serve as leaders in advancing the health and functioning of children with disabilities, this study revealed that the current amount and type of disability education received by PRM physicians is highly variable. The ACGME-required milestones for PM&R residents and fellows do not explicitly cite specific skills or knowledge pertaining to disability. It may be helpful to consider more specific verbiage in the milestones given that these requirements often guide program directors when creating and updating curricula within their programs.
Inadequate training of healthcare professionals has been cited as a factor that leads to healthcare disparities in those with disabilities; thus, the Institute of Medicine, the Surgeon General of the United States, the Association of American Medical Colleges, and several other academic policymaking institutions have identified a need for widespread disability-based education.1,5,21,22 This survey as well as data reported from other specialties3,4,11,12,14 serve as potential examples to bolster the argument that, if disability education is not a requirement, it is less likely to be implemented in graduate medical education.
While a multi-faceted approach is likely needed to fill this educational gap, developing graduate medical education-level concentrations in disability care is likely to be an important component of this effort. 8 Previous publications have noted that PRM physicians in particular are primed to improve health and functioning for those with disabilities. 17 Furthermore, PRM physicians in this study indicated that they view themselves as leaders in this arena and wish to be knowledgeable about this topic. A nationally standardized curriculum for PRM training could be one way to support PRM physicians in this goal. Respondents in this survey confirmed their support of a more formal curriculum and felt that the curriculum should include information on disability history, legislation, culture, advocacy, and interactive experiences with individuals with disabilities. These topics align with disability curricula advocacy efforts across specialties and health education.3,23,24 Each individual's lived experience is complex and unique and will benefit from providers who are trained and knowledgeable in these topics.
A standardized disability education curriculum, as supported by the results of this survey and previously advocated for by PM&R physicians, 8 could be introduced during residency and/or fellowship training to allow trainees a strong foundation upon which to build their practices. However, it is also clear that many PRM attendings already in practice may benefit from access to a disability curriculum, given that one-third of faculty respondents in this study reported receiving less than 10 h total of disability education thus far. One way to move forward with this goal would be to partner with national organizations that provide continuing medical education (CME) credits at little to no cost.
Similar to reported challenges in other fields, the lack of time for further required education, the extra time and work required for curriculum development, and the ongoing efforts to maintain an updated and accurate curriculum were identified as potential barriers and will need to be addressed.11,24,25 Protected time for residency and fellowship program leadership has been well-documented as declining. 26 However, recent efforts by the ACGME have attempted to improve this balance and will be a critical piece for development of disability education at the graduate medical education level. 27
One limitation of this study was the small sample size. Additionally, it is unknown exactly how many individuals received the survey so the response rate may be an under- or overestimate. While there is not one agreed-upon ideal response rate in medical survey research, one meta-analysis suggests aiming for an absolute response rate of 67% to minimize non-response bias. 28 While the response rate of this study was lower than that, the addition of a thematic analysis of qualitative data (i.e., a mixed-methods study) provides added validity and increases the ability to draw meaningful conclusions. 19
Conclusion
Current experiences with formal disability education are variable amongst PRM physicians. PRM providers are often viewed as leaders and experts in caring for those with disability, and this survey suggests support for a more formalized curriculum and/or requirements related to disability education for PRM physicians. PM&R residencies and PRM fellowships are urged to incorporate formal education on disability into their curricula.
Supplemental Material
sj-pdf-1-prm-10.1177_18758894261439983 - Supplemental material for Disability education in pediatric rehabilitation medicine physicians: A survey study
Supplemental material, sj-pdf-1-prm-10.1177_18758894261439983 for Disability education in pediatric rehabilitation medicine physicians: A survey study by Rebecca Caine, Caitlin Chicoine and Ashlee Bolger in Journal of Pediatric Rehabilitation Medicine
Footnotes
Ethical considerations
This study received Institutional Review Board Approval on March 17, 2022, IRB ID 2022-0032.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.