
Abstract
Purpose:
In Argentina, there is no consensus on the functional assessment of children with cerebral palsy (CP). The International Classification of Functioning, Disability and Health (ICF) Core Sets for children with CP are tools that standardize clinical functional assessments. The aim was to build functioning profiles of children with CP aged 2 to 18 years in eight Argentine cities, to identify their functional needs and contribute to improving assessment processes.
Methods:
Cross-sectional study, developed in stages. This article describes the last stage, the creation of the functional profile of a sample surveyed in eight cities. Twenty-five categories established in the common abbreviated core set of CP were evaluated through the application of a protocol called PC-CIFuncional (previously created). This protocol consists of scales or culturally sensitive instruments, assessed through clinical evaluations and questionnaires for children and families.
Results:
One hundred thirty-three functioning profiles were built using the previously developed PC-CIFuncional protocol. Of the participants, 52.7% had severe motor compromise with Gross Motor Function Classification System (GMFCS) levels IV and V. In children at GMFCS level IV-V, most categories in activities and participation—including recreation, communication and physical activity—showed severe limitations and restrictions, compared with their peers. The use of technology for daily living and mobility in children with less motor compromise (GMFCS level I-III) was neither a facilitator nor a barrier, but in children with greater compromise it was a complete facilitator.
Conclusions:
Differences in functional needs were identified in children with CP according to motor involvement. This project standardizes the identification of functional needs and therapeutic goals based on ICF language, creating novel functioning profiles in Argentina.
Introduction
Cerebral palsy (CP) is the most frequently occurring disability in the pediatric population. 1 Its consequent clinical manifestations are as diverse as the children who present them. The estimated incidence of CP ranges from 1.4 to 1.8 per 1000 live births in industrialized countries,2,3 with a prevalence of 2.95 to 3.4 per 1000 live births in low- and middle-income countries,4,5 where diagnosis and initiation of therapy occurs later than in high-income countries.6,7 Although confirming a diagnosis of CP is important, it does not provide much information about a child's functional characteristics. Diagnoses are associated with symptomatology, but do not predict function. 8
Adopting a global assessment of functioning would provide an ecological and integrated perspective on the interaction between body functions and structures, as well as environmental factors. 9 Factors such as family, friends, social attitudes and health systems have a significant influence that must be systematically measured. In Argentina, only 60.3% of individuals with disabilities have health coverage through employment-based social security systems. 10 Consequently, just over three in 10 people rely exclusively on the public health system. 11 Previous studies have shown that children with CP in Argentina who lack social security coverage receive fewer and shorter duration of therapies compared to their peers. 12
Assessing functioning supports the therapeutic team in identifying meaningful goals and engaging children, adolescents, and their families in the rehabilitation process. The International Classification of Functioning, Disability and Health (ICF) offers a structured framework for this purpose.13,14 Since the ICF includes over 1400 categories, developing Core Sets with the most relevant ones for each condition became essential. In 2014, Schiariti et al. introduced the first ICF Core Sets for children and youth with CP, along with guidelines for global implementation. 15 Various initiatives have supported the implementation of ICF Core Sets across contexts. These initiatives have been used to assess activity, participation, and functioning profiles in CP populations across various countries, and even in other conditions such as Zika.16–19
In Argentina, there is no national-level information on the functioning of this population. In a previous stage of this project, the PC-CIFuncional protocol was developed for Argentina (the Spanish translation of CP-ICFunctional). 20 Using this created protocol, this work aimed to 1) create functioning profiles of a nationally representative sample of children with CP according to the Common Brief ICF Core Set and 2) analyze differences in the functioning profiles of children with CP according to their motor compromise. It was established that a minimum number of 100 participants would be required. It is believed that this methodology can be replicated in other countries.
Materials and methods
This study was part of a cross-sectional study, developed in five stages. Stage 1: ICF formation process. Stage 2: Consensus for the definition of instruments to apply the common abbreviated set of CP (creation of the PC-CIFunctional protocol). Stage 3: Level of intra-interobserver agreement prior to protocol application. Stage 4: Pilot test and protocol adjustments. Stage 5: Construction of the performance profile. This article describes the results of Stage 5. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies was followed.
This multicenter study was carried out in 10 rehabilitation centers in eight cities in Argentina (San Salvador de Jujuy, Mendoza, Córdoba, Rosario, Reconquista, Ciudad Autónoma de Buenos Aires [CABA], La Plata, General Pacheco). Thirteen professionals comprised the panel of experts who participated in the course, protocol creation and application. They had to be graduates, have training in pediatric rehabilitation and have more than six years of experience in working with the CP population.
Participants
A functioning profile was developed based on a sample of children and adolescents aged two to 18 years. Participants included children and adolescents with CP receiving care at health and rehabilitation centers in eight cities across Argentina. The largest number of cases possible at each institution were included. All children and adolescents had a confirmed diagnosis of CP and represented all Gross Motor Function Classification System (GMFCS) classification levels. 21 All children who gave consent were included. Children whose families did not wish to participate or did not give their assent were excluded, which resulted in the exclusion of 29 children. The aim of the recruitment strategy was to obtain a sufficient sample of children with CP, according to the specifications of the Consensus-based Standards for the Selection of Health Measurement Instruments. It was established a minimum number of 100 participants. 22
This study was approved by the ethics committee of the Hospital Nacional de Clínicas de Córdoba (REPIS N° 3262/3764) and had the informed consent of fathers, mothers, guardians and/or caregivers and the assent of children over 13 years of age.
Measurements
The PC-CIFuncional protocol derives its name from the abbreviations ‘PC’ for parálisis cerebral (cerebral palsy in Spanish) and ‘CIF’ for the Spanish term for the ICF. This protocol provides guidelines for the development of functioning profiles. 23 To create the functioning profiles, the Common Brief ICF Core Set for CP was used, which consists of 25 categories to assess the four domains of the ICF. For each category, the instruments previously established in the protocol developed by a team of experts were used. These instruments corresponded to clinical evaluations or questionnaires given to families (Table 1). The instruments used included the Cerebral Palsy Quality of Life (CPQOL) questionnaire, language items from the Functional Independence Measure for Children (WeeFIM) cognitive domain, the Peabody Developmental Motor Scales-Second Edition (PDMS-2), the Gross Motor Function Measure (GMFM-88), goniometric assessments, and the Modified Ashworth Scale. For categories without existing scales, custom questions were developed and validated by experts. Each evaluation was carried out across two sessions of approximately 40 min, amounting to a total of one hour and 20 min on average for completion.
Tools proposed to apply the Brief Common ICF Core Set for CP according to the PC-CIFuncional protocol.
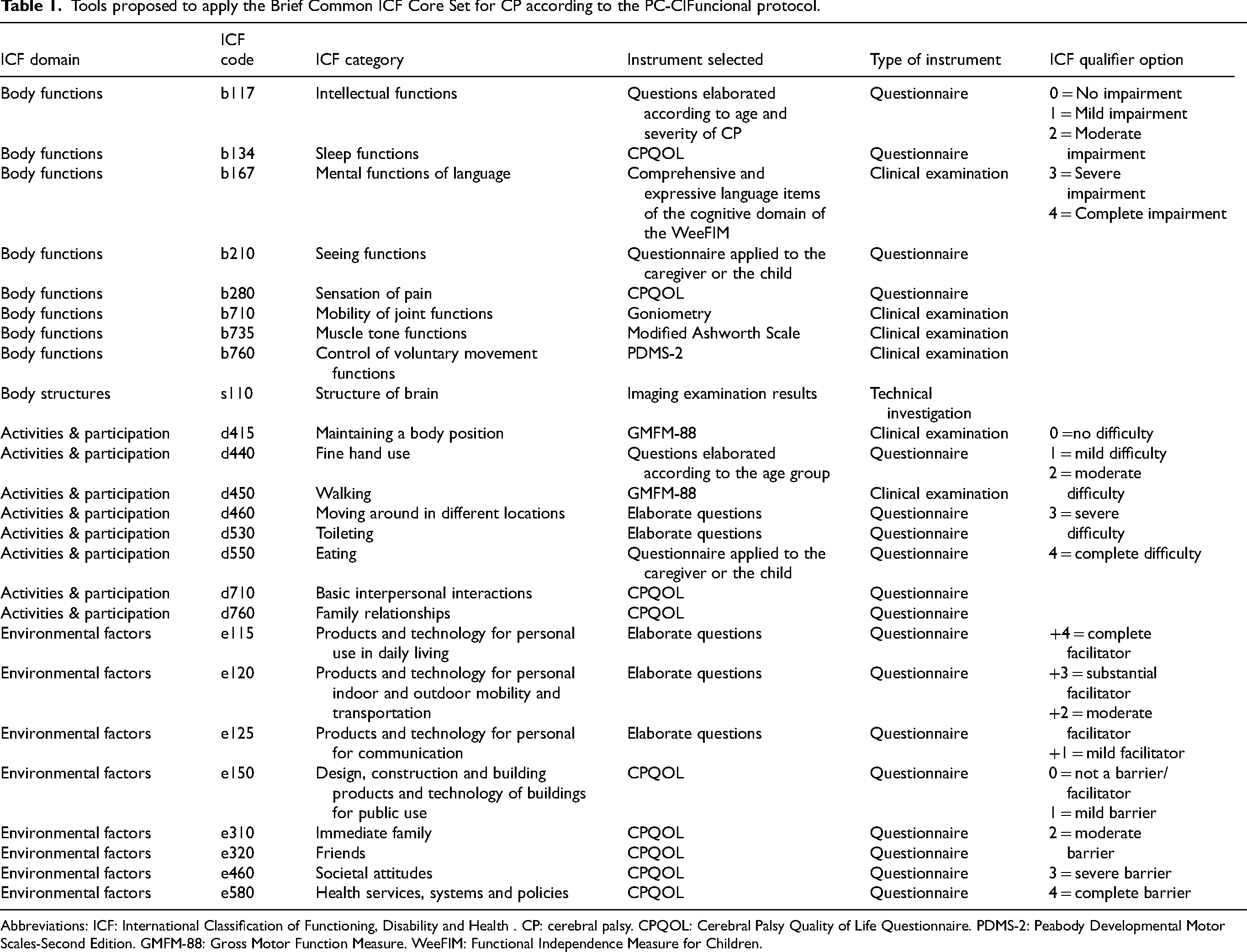
Abbreviations: ICF: International Classification of Functioning, Disability and Health . CP: cerebral palsy. CPQOL: Cerebral Palsy Quality of Life Questionnaire. PDMS-2: Peabody Developmental Motor Scales-Second Edition. GMFM-88: Gross Motor Function Measure. WeeFIM: Functional Independence Measure for Children.
Statistical analysis
For the analysis of quantitative data, continuous variables were described as means with their respective standard deviations (SDs) or medians with interquartile range according to their distribution. Discrete variables were presented as percentages with a 95% confidence interval (CI). Statistical calculations were performed using the statistical software MedCalc 18.2.1.
Results
A total of 133 functioning profiles were created. The mean age of the children was 7 ± 4 years. Most of them, 85.7% (n = 114), had social security. Sixty-nine participants (52.7%) were at GMFCS levels IV and V. According to the Surveillance of Cerebral Palsy in Europe (SCPE) classification, 24 the predominant type of CP was bilateral spastic in 52.3% (n = 69). All the participants’ characteristics are described in Table 2.
Clinical and sociodemographic characteristics of the population evaluated (n = 133).
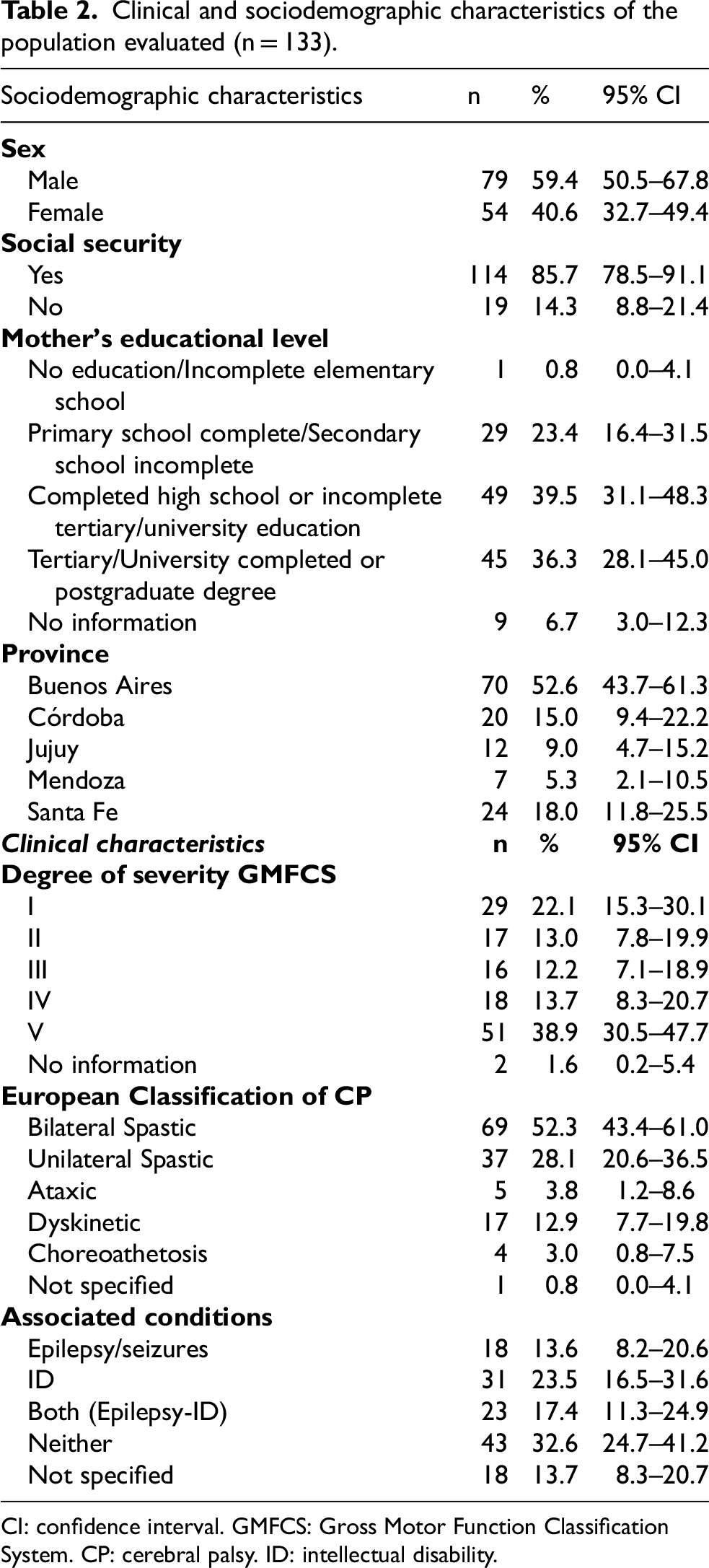
CI: confidence interval. GMFCS: Gross Motor Function Classification System. CP: cerebral palsy. ID: intellectual disability.
The functioning profiles described the functional abilities and challenges and the impact of environmental factors on a child's daily performance. As shown in Tables 3 and 4, the population can be grouped based on GMFCS levels. Children with mild to moderate motor compromise (GMFCS levels I-III) are presented in Table 3 and those with severe motor compromise (GMFCS levels IV and V) in Table 4. Figures 1 and 2 were created based on the highest prevalences in Tables 3 and 4.
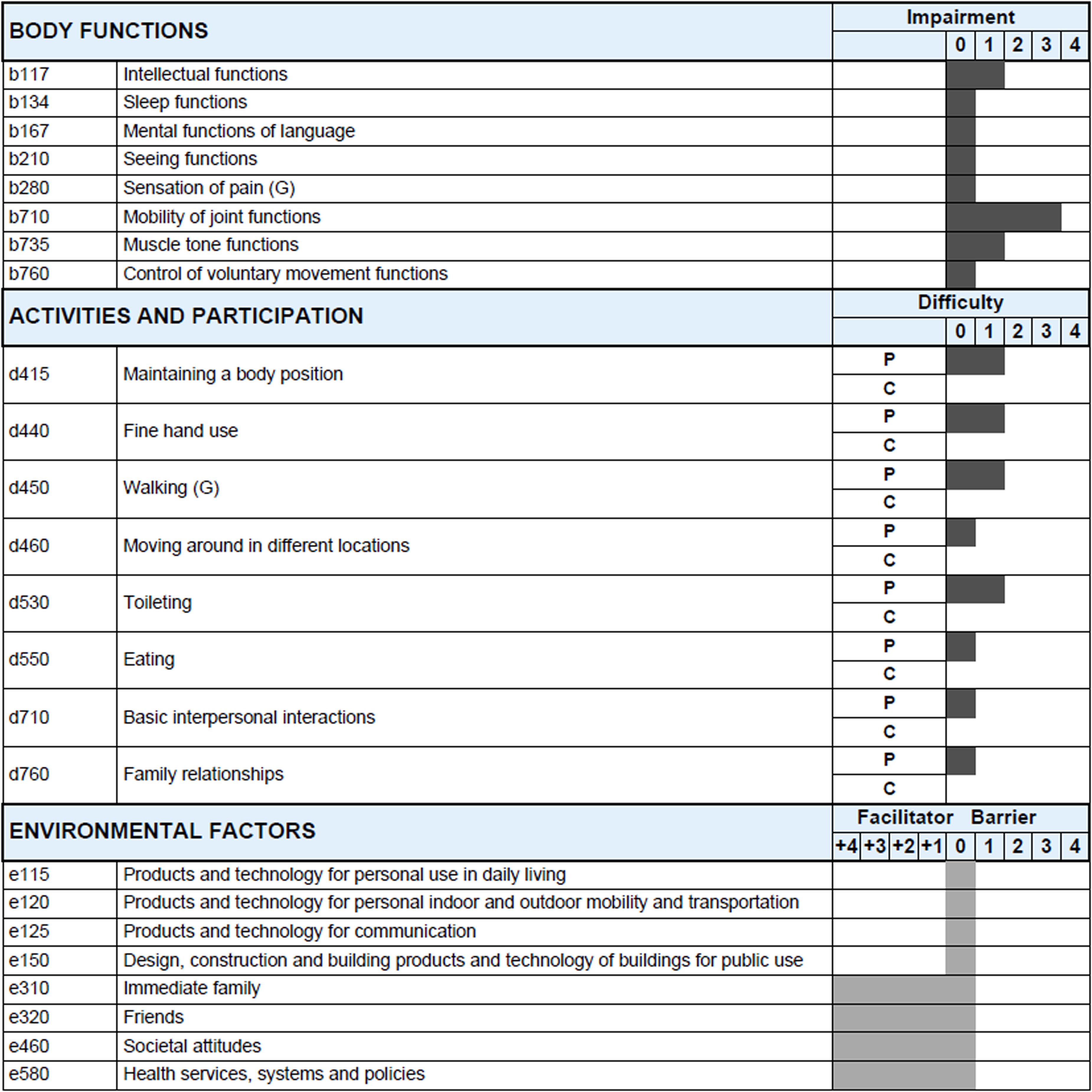
Functioning profile of children with cerebral palsy GMFCS level I–III.
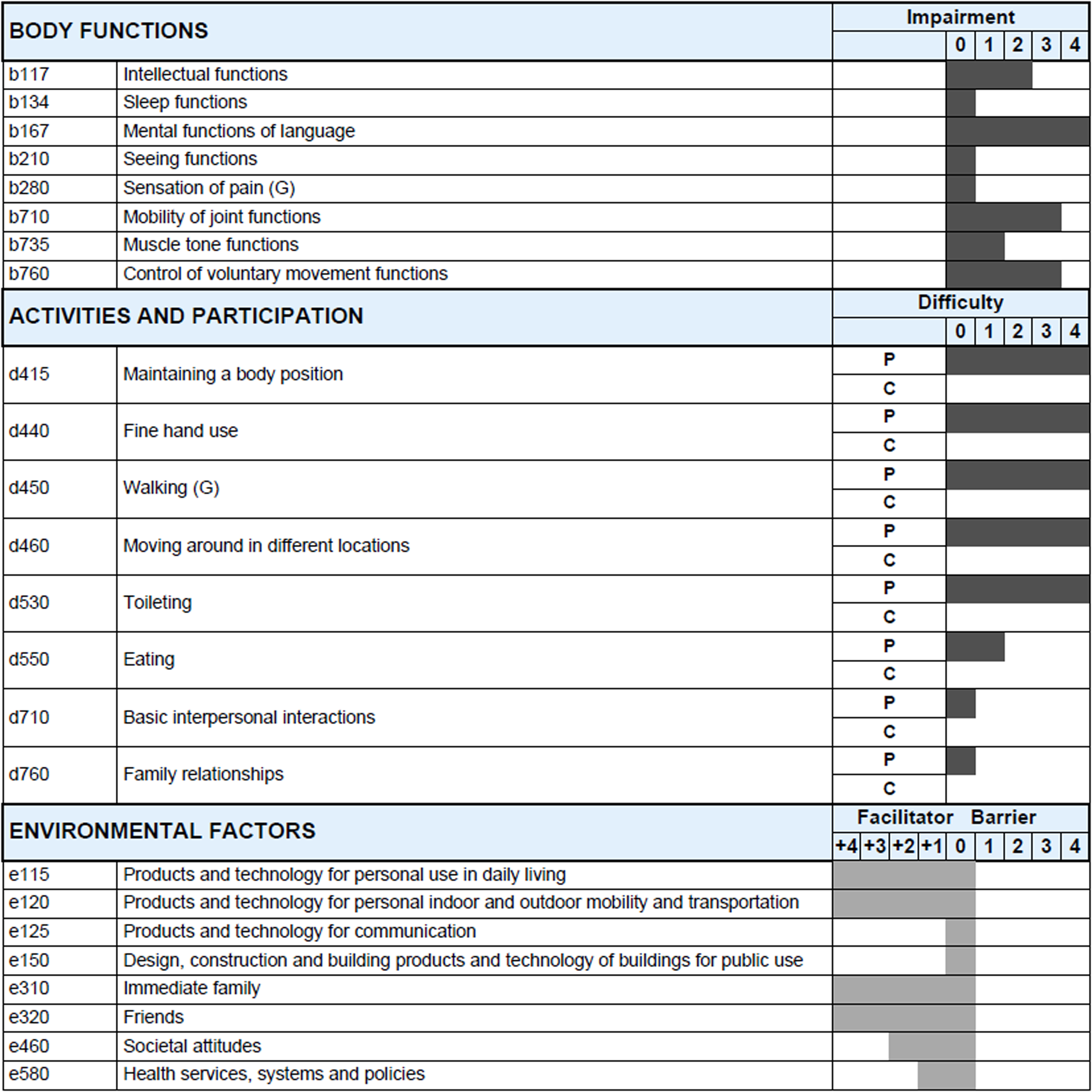
Functioning profile of children with cerebral palsy GMFCS level IV–V.
Table of relative frequency (%) describing the functioning profile of children with cerebral palsy GMFCS level I–III (n = 62).
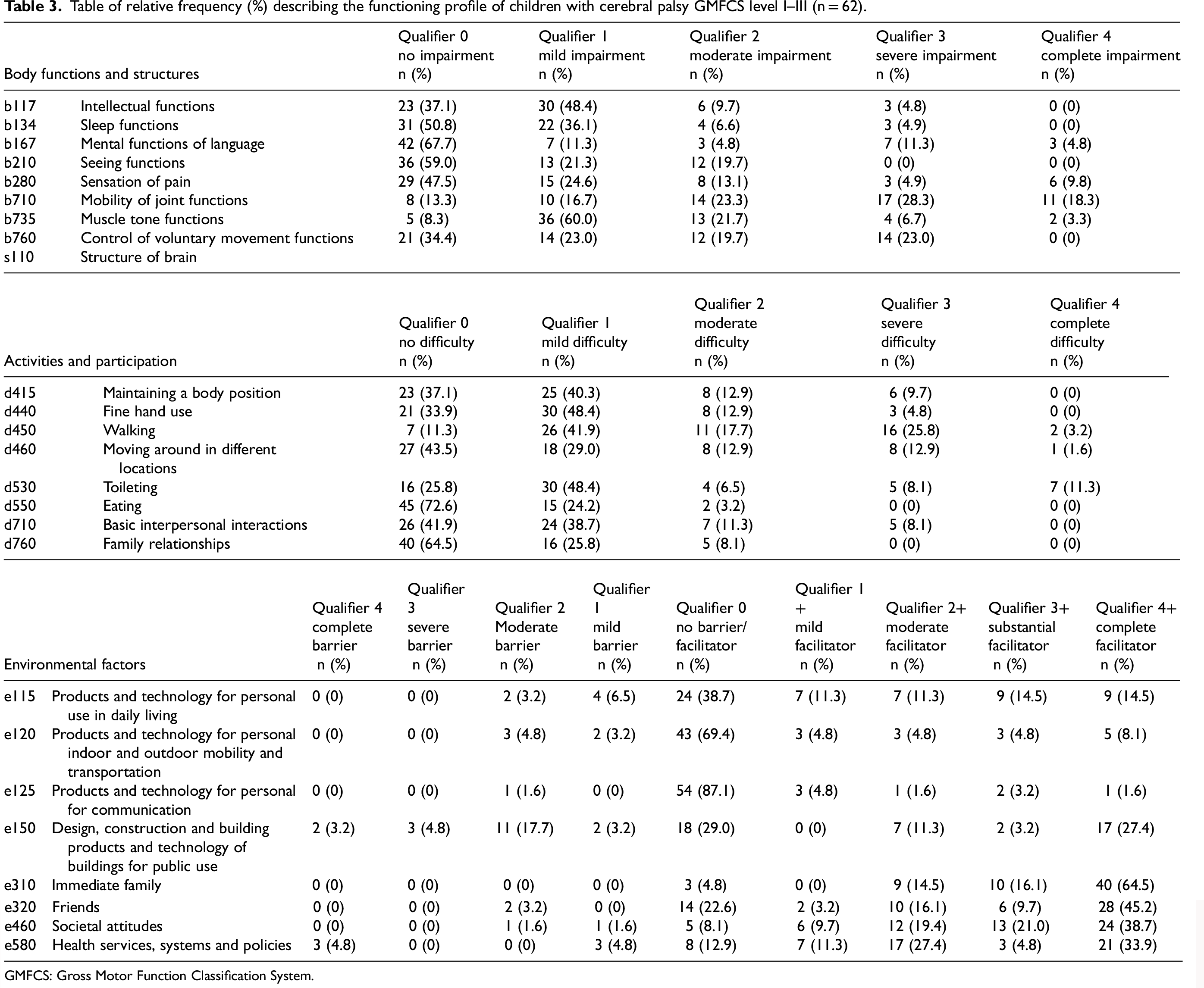
GMFCS: Gross Motor Function Classification System.
Table of relative frequency (%) describing the functioning profile of children with cerebral palsy GMFCS level VI–V (n = 69).
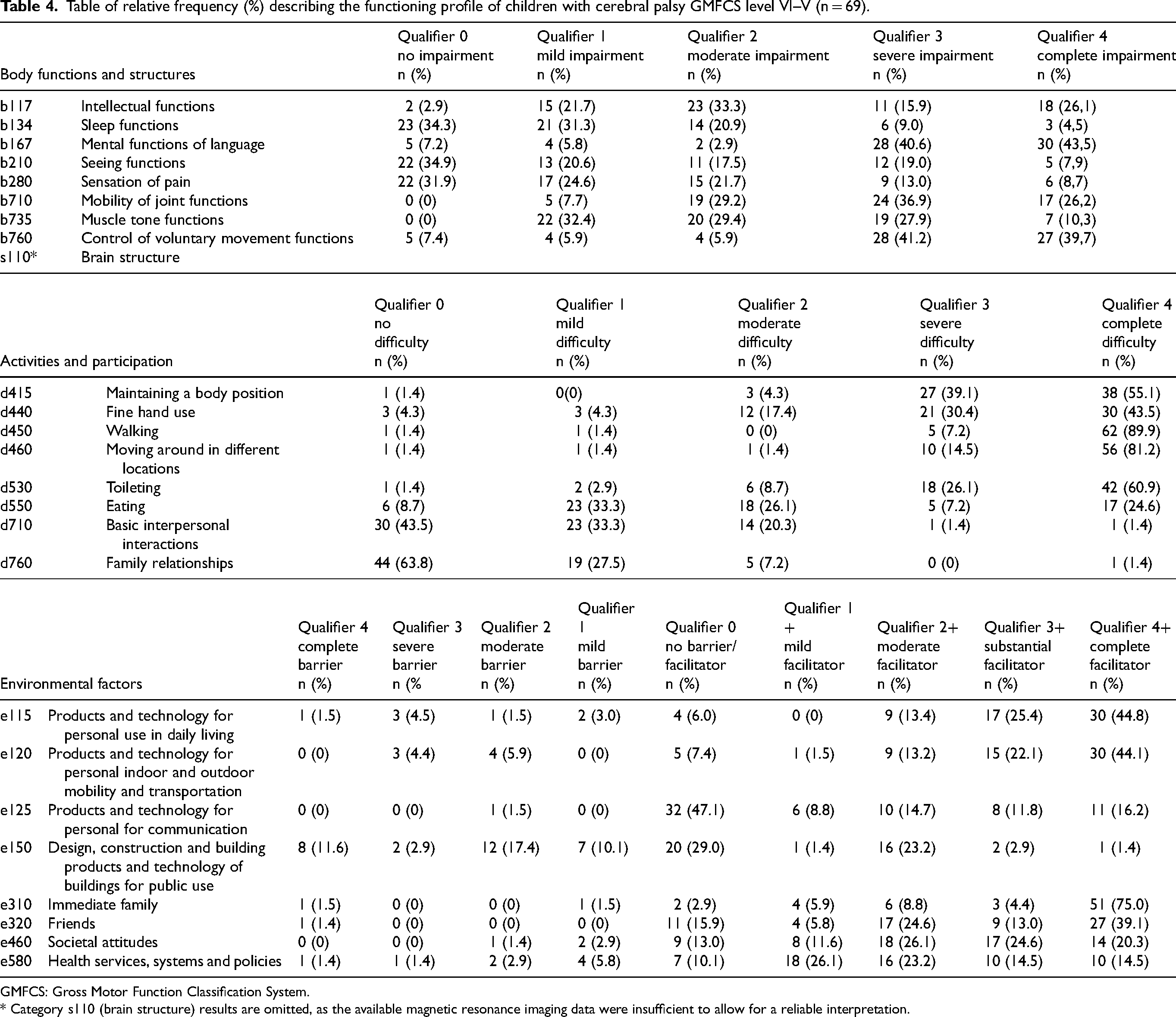
GMFCS: Gross Motor Function Classification System. * Category s110 (brain structure) results are omitted, as the available magnetic resonance imaging data were insufficient to allow for a reliable interpretation.
Figures 1 and 2 show the functioning profile of the total population according to GMFCS level groups. Regardless of the GMFCS level, categories such as sleep functions (b134), visual functions (b210) and pain sensation (b280) presented no difficulties (score 0).
In bodily functions, children at GMFCS level I-III presented severe impairment (score 3) in the category of joint mobility functions (b710), and mild impairment (score 1) in intellectual functions (b117) and muscle tone functions (b735). In activity and participation, no category presented severe restrictions (Figure 1).
In terms of components of bodily functions, children with GMFCS IV-V levels presented complete impairment (score 4) in the category of mental functions of language (b167) and severe impairment (score 3) in functions related to joint mobility (b710) and control of voluntary movements (b760). In the activities and participation dimension, children with GMFCS IV-V presented complete difficulties (score 4) in most categories, except basic interpersonal interactions (d710) and family relationships (d760) (Figure 2).
Differences in environmental factors were observed according to GMFCS level. In terms of technology use—both for daily life and mobility—children at GMFCS level I-III generally did not perceive it as either a facilitator or a barrier (score 0). In contrast, for children with GMFCS IV-V levels, technology was considered a full facilitator (score +4) (Figure 1 and 2). Among children with GMFCS I-III levels (Figure 1), several environmental factors were reported as full facilitators (score +4): immediate family (e310), friends (e320), social attitudes (e460), and health services, systems, and policies (e580). However, for those with severe motor impairments, only immediate family and friends were consistently identified as full facilitators (score +4) (Figures 2).
Category s110 (brain structure) results are omitted, as the available magnetic resonance imaging (MRI) data were insufficient to allow for a reliable interpretation.
Discussion
This study describes the process of applying a culturally sensitive ICF-based tool to operationalize the pediatric ICF Core Sets for the population with CP in Argentina. Not only did this process enable the creation of the first national functioning profile of this population, it also made other relevant contributions, such as 1) raising awareness about the importance of investing in professional ICF training in clinical settings; 2) implementing a unique protocol to standardize functional data collection and the creation of ICF-based functioning profiles; and 3) providing concrete functional information that could guide therapeutic interventions for children and adolescents with CP in Argentina. Overall, the protocol called PC-CIFuncional made it possible to identify functional needs and relevant environmental factors, contributing to the standardization of the assessment process. Although all team members were qualified to administer the various scales and instruments used to develop the functioning profiles, in practice, the professionals most frequently involved were physiatrists, physiotherapists, and/or occupational therapists. It is important to note that the specific professionals participating in the process varied depending on the resources and composition of the health and rehabilitation teams at each center.
Regarding the clinical characteristics of the sample, a high prevalence of cases of children with severe motor disability with GMFCS levels IV and V attending rehabilitation centers in Argentina was observed. This may be due to data collection in institutions specialized in motor disabilities; however, the proportions align with previous Argentine studies on CP. 25 This sample was also similar in its distribution according to levels of gross motor function to those previously described in underdeveloped or low-income countries, such as Bangladesh, and developing countries, such as other Latin American countries, with a higher prevalence of more severe cases.26,27 In contrast, in developed countries, such as Australia and the United States, mild levels of CP (levels I-II) constitute 40 to 60% of the population.6,28 These differences in severity could be explained by the types of centers included which, being specialized in motor disability, are likely to have treated more severe cases, but could also be due to other factors such as lack of early detection and intervention, access to treatment or support equipment, and fewer children with CP diagnosed with mild motor impairment.
Functional profiles based on GMFCS level make it possible to identify needs more specifically, not only for each group but also for each individual. Previous studies have demonstrated that functional profiles are valuable tools for designing intervention strategies tailored to the unique abilities and limitations of each child with CP or another disability.23,29
The findings of this study confirm that children with severe motor impairments (GMFCS levels IV–V) experience greater functional limitations, particularly in the domains of body functions (three out of the eight components) and activities and participation (five categories). These results are consistent with previous research. For instance, studies conducted in Russia, Brazil, and Turkey have reported similar patterns of severe impairment, especially in areas related to voluntary movement, muscle tone, intellectual functions, and gross motor performance.16,18,30 This aligns with studies showing that nearly all CP Core Set parameters correlate with poor GMFM-66 outcomes in children with GMFCS IV-V levels, highlighting the broad impact of severe motor impairment. 16 These converging findings reinforce the importance of early identification and intervention strategies aimed at minimizing the effects of motor impairment on overall functioning. Furthermore, they highlight the need to tailor rehabilitation approaches to better support children with high levels of motor involvement.
Regardless of GMFCS level, there tended to be fewer impairments, limitations, or restrictions in the following categories: seeing functions (b210), sleep functions (b134), sensation of pain (b280), basic personal interactions (d710), and family relationships (d760). Although some studies report that more than 50% of children with CP have some visual impairment, 10 this was not the case in the present study population. With respect to sleep functions (b134), Espinosa and Ortiz reported that only 16.7% of a sample of children with CP reported some sleep disturbance, 31 which coincides with the current study. As for the categories of basic personal interactions (d710), the results reinforce the importance of a social and family network for the child with disabilities, and of further research on its evaluation in rehabilitation processes.
Among the environmental factors, the use of technology for both daily life and mobility was neither a facilitator nor a barrier for children with less motor compromise, while it was a complete facilitator for children with greater motor compromise. It is important to mention that, although most children participating in the study need an assistive device for communication, many do not have one, making it a major barrier to communication. Inequalities in access to assistive devices between individuals with and without social security should continue to be investigated in order to highlight these disparities and propose targeted solutions. In a study on the use of assistive technology to promote adaptive skills in children with CP, 32 Stasolla et al. found that various assistive technologies were effective in fostering independence and self-determination among children with CP, regardless of their levels of intellectual and motor functioning. Technologies for the activities of daily living, mobility and communication provide autonomous access to request and choice processes. These results continue to show the impact that assistive devices have in facilitating the participation of children with CP and the impact on their quality of life. 32 For this reason, it is necessary to identify the causes of the difficulties in accessing them and ensure that everyone, according to their particular needs, is in a position to gain access.
By promoting participation, family, friends, and health services are a fundamental support network for people with disabilities; child- and family-centered care in particular are indispensable in the rehabilitation process of children with disabilities.33,34,35 Many families rated health services as facilitators simply because they had access to them, even if the quality was suboptimal or not family centered. It is essential to investigate health disparities among individuals with CP in Argentina, with particular attention to the quality of and access to rehabilitation services. In Argentina, Law 24.901 (1997) establishes the system of basic benefits for the comprehensive habilitation and rehabilitation of persons with disabilities, including the provision of assistive devices. 36 The law designates the social security system as the primary payer of these benefits. Consequently, children with CP who are not covered by a social security scheme often experience severely limited or precarious access to rehabilitation services and assistive technologies. Future studies should explore access to communication devices and opportunities for community-based participation, such as recreation, music, and arts, both inside and outside school.
This study had limitations. The sample was drawn exclusively from rehabilitation centers, so children with mild motor impairments and without social insurance may be underrepresented. Therefore, the results should be interpreted in this context and not extrapolated to the whole population of children with CP. As participation in the study was voluntary, no data were collected from individuals who declined to participate. Therefore, it was not possible to assess potential differences between participants and non-participants, which may have introduced a degree of selection bias.
One of the strengths of the present study is its multicenter and multidisciplinary nature. This was the first collaborative initiative, which described functioning profiles, in rehabilitation centers in different provinces of Argentina that are recognized for their work with people with CP. The unique perspectives of the team made it possible to obtain adequate representativeness in the creation and application of the protocol of this first version of PC-CIFuncional. In addition, due to the success of the ICF educational course, this project has enabled hundreds of professionals in the country to receive training in ICF. The research team has provided four additional courses and continues to provide ICF education, with an emphasis on ICF-based tools for clinical practice.
Future directions
Due to the success of the collaboration working with professionals across the country, the study team is creating a network of centers to apply PC-CIFuncional to gain full representation of provinces. Importantly, the project recently received funding from a federal agency (PICT RAICES 2022–2024) to carry out the multicenter implementation of PC-CIFuncional in the next three years.
Conclusion
This project standardizes the identification of functional assessments and therapeutic goals using ICF language. Different functional needs were identified in children with CP depending on their level of motor commitment. This suggested that the functional profiles might be influenced by different factors that must be considered when thinking about therapeutic goals. This novel protocol called PC-CIFuncional facilitates the creation of much-needed functional profiles of children with CP in Argentina, filling an important gap in national disability data. The systematic application of PC-CIFuncional in this country will contribute to individual assessments in rehabilitation centers, and comparisons of functional needs at the provincial and national levels, ultimately guiding appropriate services and interventions for children and adolescents with CP.
Footnotes
Acknowledgments
We thank all the participants, researchers and collaborators who participated in the study for their effort and contribution. The authors thank the collaborators in the different phases of the study. In the PC-CIFuncional creation stage, we would like to thank Mariana Melaragno, Agustina Fabbro, Úrsula Ivancic, Maria Laura Mammana, Geraldina Morganti, Andrea de los Ríos, Lourdes Graffigna, Romina Vera, Valeria Menéndez, Silvana Domínguez, Federico Ángel Benito, and Alejandra Capone for their participation. In addition, in the process of making the performance profiles, we appreciate the collaboration of Sandra Schenfelt, Sonia Spiazzi, Mayra Rossetti, Mailen Cernadas, Roxana Ramírez, Cielo Frangi, Carolina Zinni, Cecilia Lucentini, Jackie Ducoté, Verónica Parareda, Juan Zamora, and Mariana Stoisa.
Ethical considerations
This study was approved by the Health Research Ethics Committee CIEIS- Hospital Nacional de Clínicas FCM (REPIS N° 3262/3764) and had the informed consent of fathers, mothers, guardians and/or caregivers and the assent of children over 13 years of age.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Material resources were provided by the Institute for Clinical and Epidemiological Research (INICyE). The National University of Córdoba funded the work through a grant from SECyT (Resolution SECyT N.° 411/18). The Cerebral Palsy Alliance Research Foundation supported this work through grant PRG10321. In addition, it was carried out with the support of the SALUD INVESTIGA 2020–2021 grants, awarded by the Ministry of Health of Argentina through the Directorate of Health Research, and a grant through a PICT project awarded by the Fund for Scientific and Technological Research FONCyT (PICT-2021-III-A-00062).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.