
Abstract
For almost all Americans, having affordable access to quality health care in the United States requires health insurance. Inadequate insurance is more common among children with disabilities and complex health conditions than other children. For children, insurance is considered adequate if the benefits must usually or always meet the child's needs and usually or always allow the child to see needed providers and the family reports no out-of-pocket expenses or out-of-pocket expenses deemed usually or always reasonable. After the CEO of UnitedHealthcare was killed in front of a Manhattan hotel on his way to his annual investor conference in December 2024, there was an outpouring of stories on social media about how people felt their loved ones were harmed by health insurance companies denying care that their doctors recommended. While murder as a form of vigilante justice should not be condoned, this event highlighted how angry Americans are at health insurance companies. Pediatric rehabilitation medicine physicians are no strangers to the frustrations of insurance denials for their patients and feel the strain of having to work through prior authorizations and peer-to-peers just to get their patients what they deem important for their health and functioning. The national data confirms what pediatric rehabilitation medicine physicians knew from collective experience - millions of children with more complex health care needs have inadequate insurance.
Keywords
When I was in my combined Pediatrics/Physical Medicine and Rehabilitation residency, our pediatric rehabilitation medicine clinic on Wednesday afternoons occasionally included calling insurance companies for peer-to-peer discussions about equipment denials. I remember one that I did while Dr. Doug Kinnett was listening and coaching me. It was for a head support on a child's wheelchair. The child obviously needed the head support, as the clinical documentation made clear. This was a school-aged child with cerebral palsy with a Gross Motor Function Classification System level of V. With Doug's coaching, I handled the peer-to-peer and the head support was approved. The whole thing seemed like a waste of time and energy. We knew what the child needed; the insurance company did not. In part because of situations like this, while I was in residency, I opted to also pursue a Master of Public Health degree in health policy and management. I did my thesis on health insurance for children with special health care needs. What I learned is what I already knew anecdotally: insurance was not always covering what children needed.
After the CEO of UnitedHealthcare was killed in front of a Manhattan hotel on his way to his annual investor conference on Wednesday, December 4, 2024, there was an outpouring on social media. Some applauded the killer's actions, some hoped the killer would avoid capture, many (and I mean many) shared their stories about how they or their loved ones were harmed by health insurance companies denying care they and their doctors felt was needed. As Dr Glaucomflecken eloquently said in his video, “two things can be true, one is that murder is bad, that even people who do bad things don’t deserve to be executed… it can also be true that UnitedHealthcare is an evil corporation that has caused pain and suffering to millions and millions of people over the years.” 1 But let this event galvanize us to move forward as a nation to improve financing, access and equity in health care.
As patients and families took to social media to share their own horror stories of fighting insurance companies for what they needed, physicians were doing the same. Simultaneously, insurers were posting about the “good” work insurers are doing by keeping patients from harmful, wasteful care. I guess it is all a matter of perspective…. but it is not. Of course, wasteful care should be avoided. But the insurers are in the business of making money and one obvious way they make money is by denying diagnostic tests and treatment that benefit people's health. If they didn’t make money doing it, they wouldn’t. According to their financial statements UnitedHealthcare made $23 billion in profits in 2023 with a 33% claim denial rate.2,3 Real people are harmed when denied the care they need, real people have died, real people have been bankrupted by out-of-pocket medical expenses. Medical debt impacts 19% of households and is associated with poor health outcomes and premature death.4,5 This is no secret; insurance companies know this.
Insurance is not covering what children need. From my vantage point, the situation has gotten worse, and the data concur. For children with more complex health care needs (the children we often see in our clinics), health insurance adequacy has, in fact, declined in recent years (see Figure 1). A million more children experienced inadequacy in 2022–23 than in 2011–12.6,7 Publicly available data from the National Survey of Children's Health (NSCH) demonstrates that increasingly more families of children with more complex health needs reported that their child's insurance was inadequate (see Table 1).6–10 To have adequate insurance, the insurance benefits must usually or always meet the child's needs
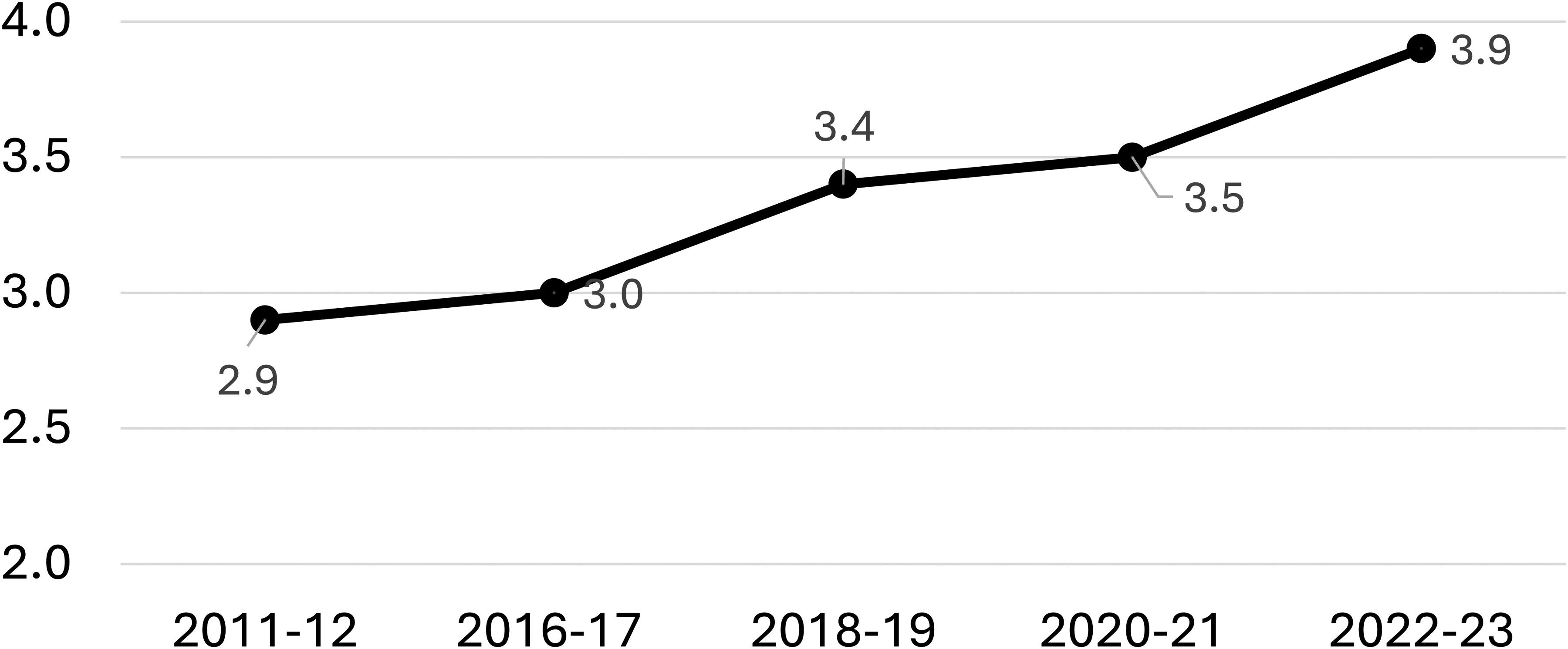
Millions of children with more complex health care needs without adequate insurance (2011–2023). Note time gap between 2011–12 and 2016–17 when the National Survey of Children's Health was being revised. Data publicly available from childhealthdata.org.
Percentage of children with more Complex health care needs without adequate insurance (2011–2023).
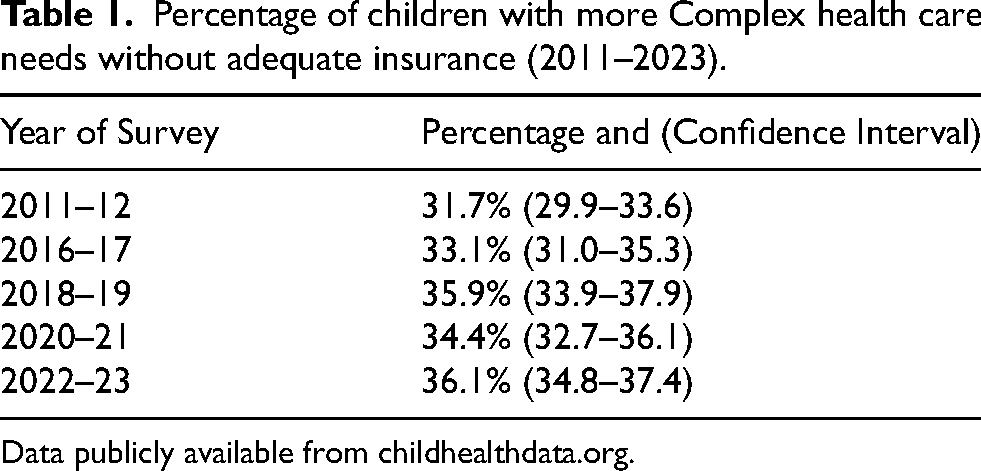
Data publicly available from childhealthdata.org.
Pediatric rehabilitation medicine physicians know what is like to have to fight insurers to get our patients what they need. On our private Facebook group, colleagues have shared how they spend hours stuck in phone trees, how insurance companies manipulate the process by offering a time window for a peer-to-peer that has already passed by the time the prescribing physician is alerted by mail of a denial, how they never actually get to talk to a peer, how much time and energy they spend dealing with insurance companies instead of providing actual patient care. See Table 2 for examples of denials.
Examples of denials for pediatric rehabilitation medicine patients.
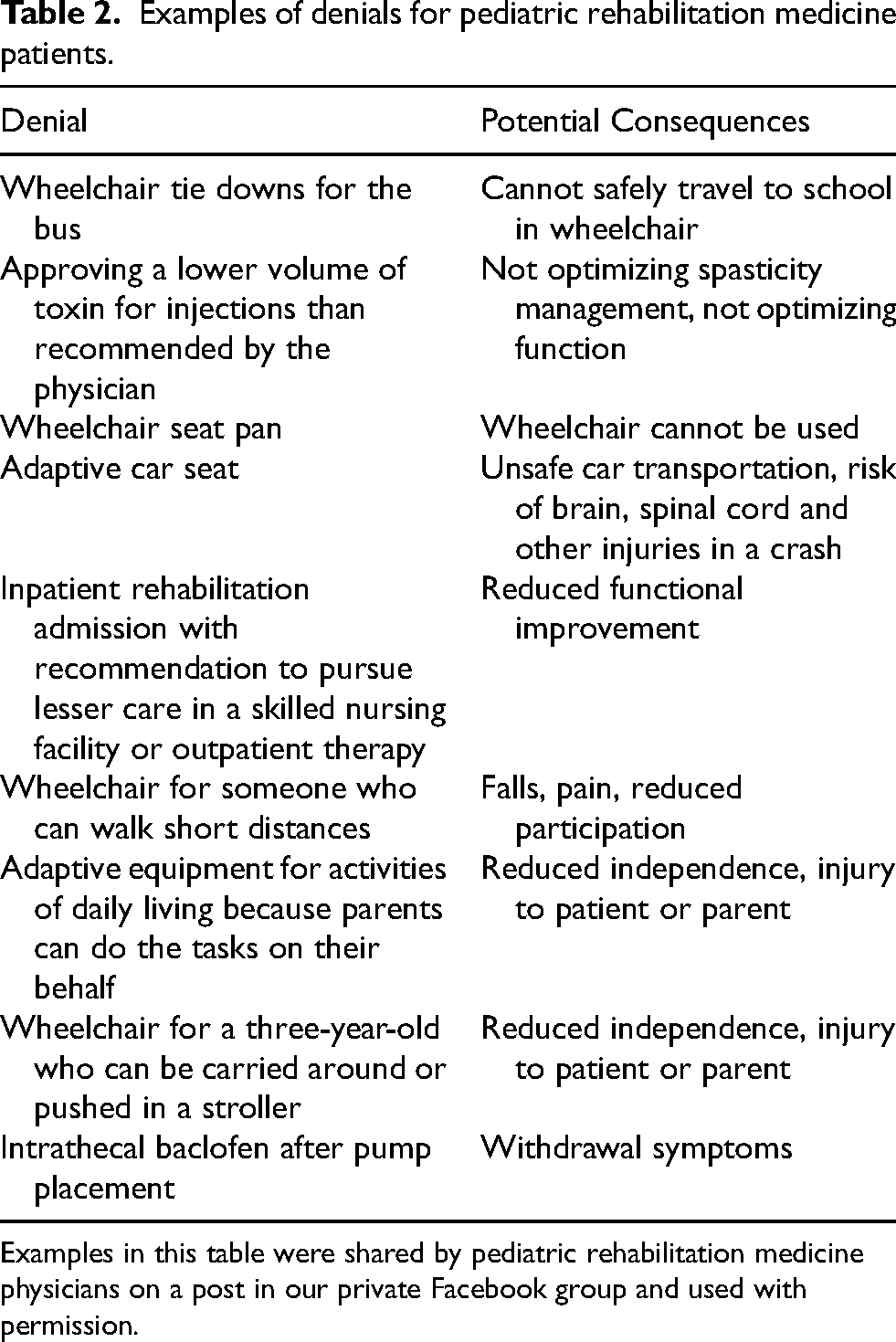
Examples in this table were shared by pediatric rehabilitation medicine physicians on a post in our private Facebook group and used with permission.
Appealing denials is associated with administrative burden for patients and families, not just health care providers. 12 The appeal process can worsen inequities for those already marginalized. 12 Health insurance companies utilize various tactics to shift losses to their covered population. 13 Artificial intelligence (AI), when used to deny claims or prior authorization requests, can cut costs for health insurers and wreak havoc upon patients and providers. A class action lawsuit filed in 2023 against UnitedHealthcare charged that their AI algorithm denied and overrode claims for older patients with a 90% error rate. 14
I have anticipatory frustration when I am alerted to the need for a peer-to-peer. Once, I had to do a peer-to-peer for wheels for a wheelchair. Yes, you read that correctly: wheels for a wheelchair. I explained that, without wheels, a wheelchair is just a very expensive chair and my paralyzed patient needed mobility. “Wheels are an essential component of a wheelchair, hence the name,” I harshly noted. The wheels were approved. But I was so angry. Seething, really. What a colossal waste of time. It was a waste of my time. But more importantly, it was a waste of my patient's time. Time that he could have had independent mobility in a chair that was custom made for him. It is morally injurious to me when I cannot assure that my patients get what they need to be as functional as possible and engage in life events as they desire. 15 Adding weeks to a process of getting a new wheelchair is burdensome to the family and limits the child unnecessarily. I do not want this for my patients. I want to help them thrive. This means that I will do the peer-to-peers and that I will advocate for my patients’ needs. But what I do and what I know my colleagues are doing is not enough. We need systems-based solutions. We need policies to assure that people are put above profit. And now we need our legislators to know how important health insurance is to the children we care for in our clinics.
Pediatric physiatrists can advocate for better coverage for the children we serve because underinsurance is a known problem and will become a bigger problem if cuts are made to Medicaid funding.11,16,17 Optimizing Medicaid and the Children's Health Insurance Program, as detailed by the American Academy of Pediatrics (AAP), is a strategy for which advocacy efforts are needed. 18 In their Principles of Health Care Financing policy statement, the AAP asserts that “(1) coverage with quality, affordable health insurance should be universal; (2) comprehensive pediatric services should be covered; (3) cost sharing should be affordable and should not negatively affect care; (4) payment should be adequate to strengthen family- and patient-centered medical homes; (5) child health financing policy should promote equity and address longstanding health and health care disparities; and (6) the unique characteristics and needs of children should be reflected.” 19 This is an envisioned future worth advocating for regardless of how out of reach it seems. All children deserve this. Unfortunately, health insurance adequacy is likely to worsen substantially if proposed cuts are signed into law.17,20 With political threats to Medicaid, advocacy on behalf of children's health is increasingly important. 21 It is time for all of us to raise our voices, whether on the phone to our congressional representatives, in letter writing campaigns, correcting disinformation on social media, or with our signs during peaceful protests. When we advocate for our patients one by one as we do in peer-to-peers or when we advocate for the needs of our patients with disabilities more generally, our voices are valued in the chorus of advocacy to help children with disabilities thrive.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.