
Abstract
Purpose
Children with disabilities benefit from physical, occupational, and speech therapy, but families identify unmet needs for these services. The purpose of this study was to audit access to therapy services in a tri-state region. It was hypothesized that children who were publicly insured and children from minoritized identity groups would face greater access barriers and longer wait times than children covered by private insurance and non-minoritized White children.
Methods
This prospective audit study utilized callers who posed as mothers seeking outpatient therapy services for their child. Access difficulties were identified based on the number of phone calls required to obtain an appointment or determine if services would be obtained at all, as well as the number of days to the earliest available appointment.
Results
Therapy appointment access was a problem for 47.4% of simulated families. After 251 phone calls, 91 simulated families were able to schedule appointments in 76 clinics. Black and Hispanic simulated families had a harder time getting appointments, but days to appointment did not differ by telegraphed minoritized identity (F(3,88) = 1.474, p = .227).
Conclusion
Simulated families experienced substantial barriers to arranging therapy appointments with Black and Hispanic families experiencing more barriers than their White and Muslim peers.
Introduction
Children with disabilities benefit from occupational, physical, and speech therapy services to improve function. 1 Accessing care is a national problem with many families experiencing unmet rehabilitation needs for their children with disabilities.2–4 These rates of unmet and underrecognized therapy needs significantly increase among poor children and those with more severe disabilities. 3 Inadequate insurance coverage, high out-of-pocket costs, geographical barriers, and institutional racism further restrict access to equitable, quality, and efficient healthcare.5,6
This study evaluated pediatric therapy access in the tri-state area of Western Pennsylvania, Eastern Ohio, and West Virginia. It sought to determine if there were differences in access to therapies and wait time to first available appointment between privately and publicly insured children and children of different minoritized identities. The hypothesis was that publicly insured children and mothers of children with minoritized identities would face greater access barriers and longer wait times.
Methods
Study design
This prospective audit study was conducted using callers who posed as mothers seeking outpatient therapy services for their simulated three-year-old child with cerebral palsy over an eight-week period. The protocol and scripts were developed based on clinical expertise in conjunction with the model developed by Fuentes et al. 7
Outcome measures
Access difficulty was assessed by ability to make an appointment, determining the number of calls required to obtain an appointment when an appointment was obtained, and the wait time for obtained appointments (recorded as the number of days to earliest available appointment for pediatric rehabilitation therapy services).
Sampling method
Three hundred thirty four rehabilitation therapy clinics in the tri-state region of Western Pennsylvania, Eastern Ohio, and West Virginia were identified and organized into a database by their state, US Census population density (rural versus non-rural), type of population served (lifespan versus pediatric only), and contact information. The clinics were obtained using a Google Maps search with the parameters restricting locations to a 150-mile radius from the UPMC Children's Hospital of Pittsburgh, and the search terms were “occupational therapy,” “physical therapy,” “speech therapy,” “rehabilitation,” and “clinic.”
Four simulated family units were created to represent different minoritized identities – White, African American, Hispanic, and Muslim. These identities were chosen because individuals from these backgrounds face interpersonal and structural discrimination and are therefore minoritized compared to those who solely identify as White.8,9 Names were chosen for simulated families based on internet searches that revealed the popularity and frequency of the name within respective cultures to ‘telegraph’ or ‘signal’ identity.10,11 Each family type was then paired with public or private insurance providers creating eight patient identity/insurance profiles (Figure 1). These patient profiles were then randomized to one of the four clinic types (rural versus non-rural by lifespan versus pediatric only) and within the three states using a SAS-V-9.4 random number generator.
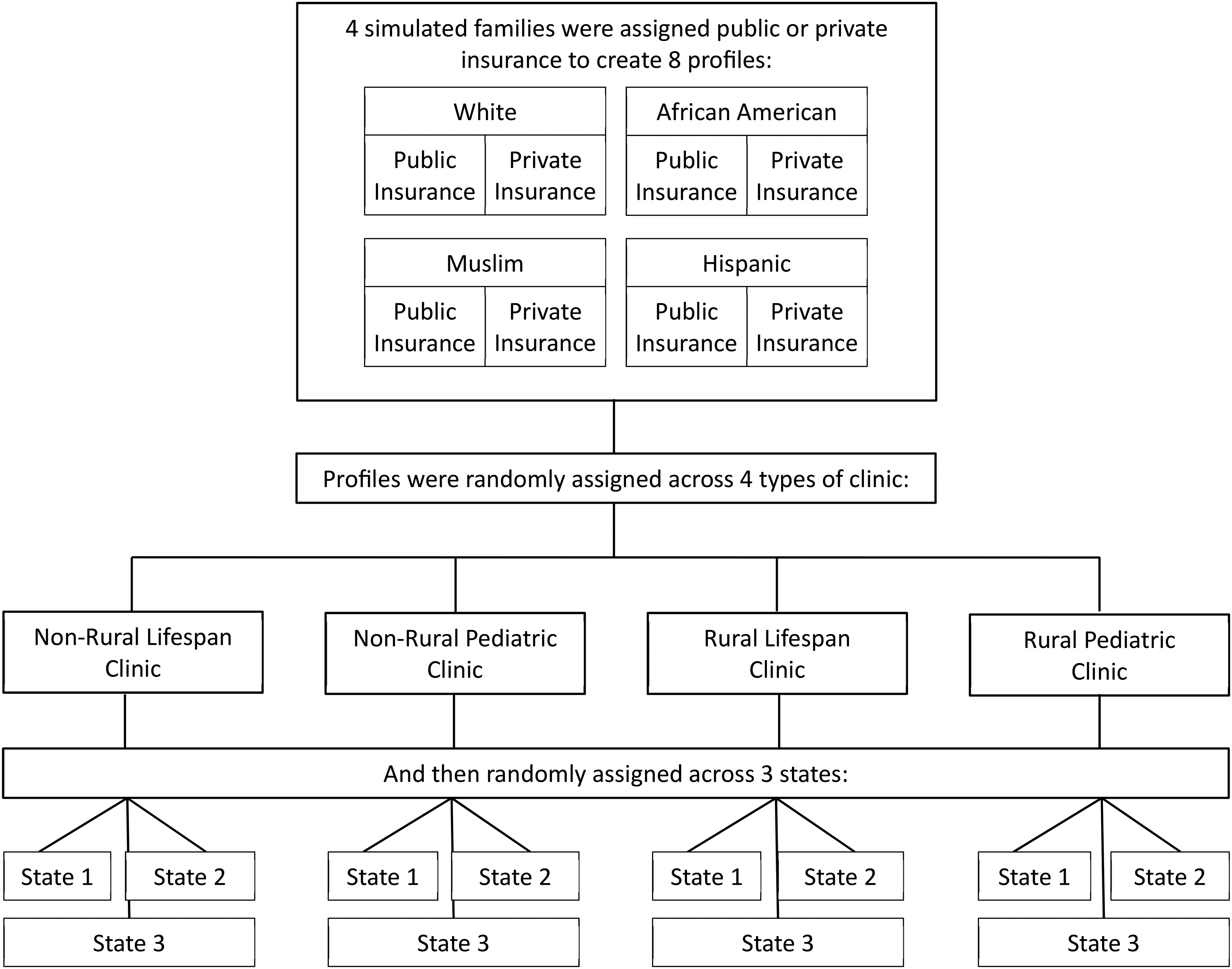
Randomization schedule.
The callers obtained information regarding services provided (occupational therapy, physical therapy, and speech therapy), accepted insurance type (private or public), and wait time to the first available appointment (measured in days) for each of the clinics called. Protocol required simulated family callers to make five call attempts, leaving a message after the second if phone calls went unanswered. Voicemails included the mother's first name and child's full name and phone number. When no outcome was reached after five call attempts, callers replaced the clinic with a substitution that matched all profile characteristics (identity, insurance type, rurality, population served, and state). A substitution was only to be used if (1) calls went unanswered after five attempts, (2) the clinic did not provide pediatric services, (3) the clinic number was no longer in service, or (4) multiple clinics used a centralized scheduling system. The a priori estimate of simulated families required to complete the calling process to ensure representation of the possible combinations of clinic type, child profile, and state was 109. A call was considered completed when it had reached its final conclusion: (1) an appointment date was provided, (2) the family was turned down due to insurance type, or (3) the family was told that the clinic was fully booked or not taking new patients.
Statistical analysis
Chi-square analysis (p < 0.05 as statistically significant) was used to determine the relationship of call outcomes with simulated family and clinic factors. To identify the importance of each factor on call outcomes and explore significant interactions between these factors, tree diagrams were created using chi-square automatic interaction detection (CHAID). CHAID incorporates chi-square to analyze all predictors and determine which of these has the strongest association with the dependent variable (i.e., call outcomes). 12 The top node of the classification tree starts out with all possible cases included. The tree is then split by whichever predictor was found to show the most differentiation on the dependent variable, and results in new nodes on the classification tree which are subsets of the original. The process is then repeated on these new nodes and continues until chi-square fails to find a significant relationship between a predictor and the dependent variable.13,14 Two tailed t-tests were used to determine the effect of clinic type and rurality, while one-way ANOVA was used to analyze the effect of state and identity on wait times. IBM SPSS version 26 was used for these analyses.
Results
Call outcomes: appointment access
Access to appointments was a problem for 47.4% of the simulated families. Out of 173 simulated families attempting to schedule appointments with 140 clinics, 91 (52.6%) successfully obtained appointments in 76 clinics (54.3%) with a total of 251 calls made (see Figure 2). An additional 21 simulated families (12.1%) were unable to schedule services for their child due to calls going unanswered, having insurance that was not accepted, or because the clinic reported being fully booked. Based on the sampling protocol, 31.2% of simulated families sought out alternative clinics. Of those substitutions, 68.5% of simulated families were told the service was not provided, 11.1% were met with nonworking numbers, 9.3% did not receive a response within five call attempts, and 11.1% were not provided a date for other reasons.
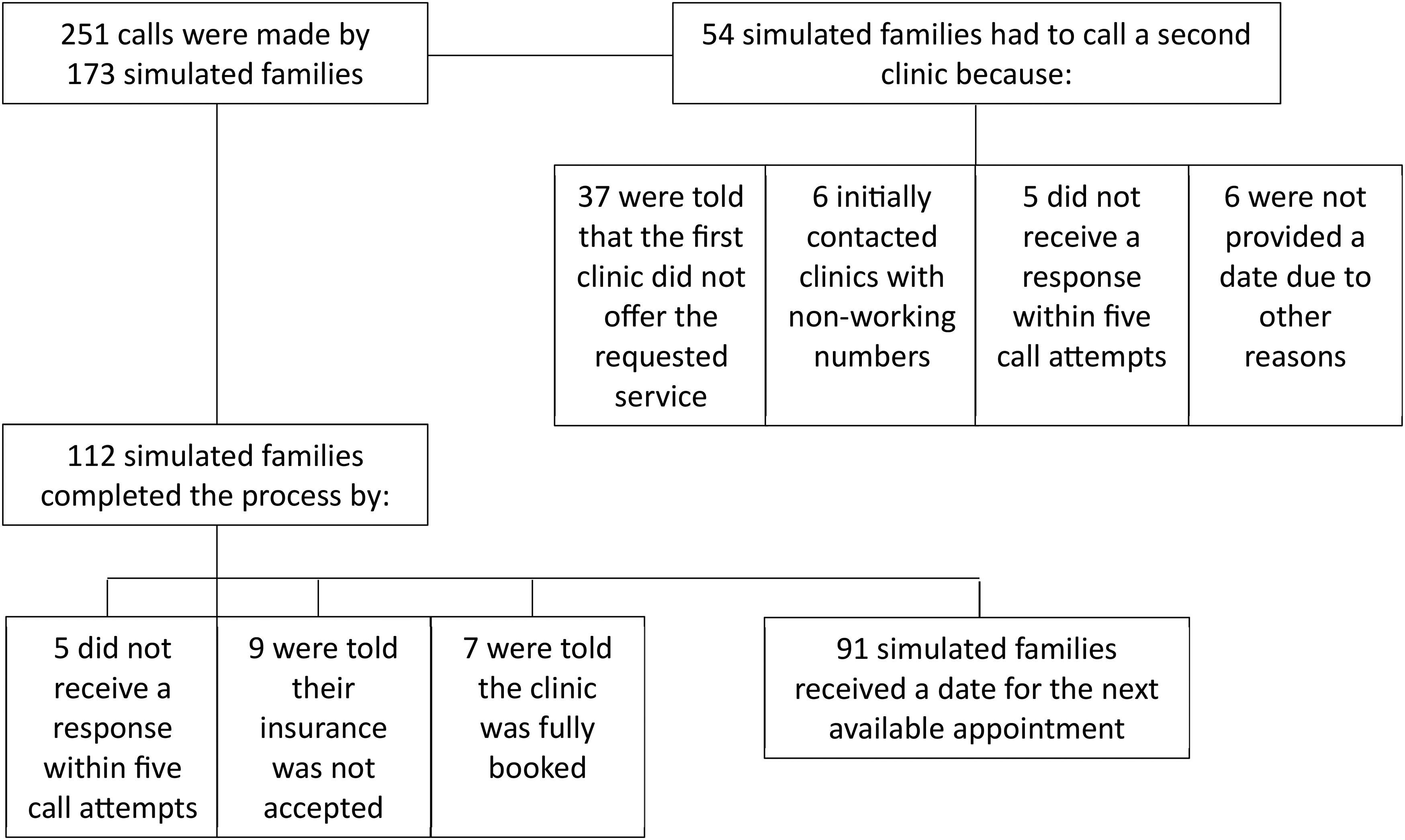
Overall call outcomes.
For approximately every three calls placed, one appointment was successfully booked (36.6%). In total, 70.3% of simulated families received an appointment date on their first call attempt with 18.7% of appointments made after two attempts, while 11.0% had to make three or more calls to the same clinic before being able to obtain an appointment for their child.
For appointment attainment, CHAID indicated that the state was the most important variable. Simulated mothers who contacted Pennsylvania and Ohio clinics received an appointment 40.9% of the time, while those who contacted clinics in West Virginia received an appointment 24.3% of the time, p < 0.05. The final split in the tree separated the Ohio and Pennsylvania node by the child's identity. Statistically fewer Hispanic and Black simulated families in Ohio and Pennsylvania were able to receive an appointment (34.3% compared 50.7% for White and Muslim families, p < 0.05). Insurance type was not a predictor of appointment attainment.
Wait times
T-tests determined that clinic type (lifespan versus pediatric only) did not significantly affect wait times (t = .125, p = .901) for the 91 appointments obtained, but the rurality of clinics did significantly affect the patient wait times (t = 3.397, p = .001) with wait times being longer for non-rural versus rural clinics. The results of the ANOVAs showed that state did not have a significant effect on wait times (F(2,88) = .930, p = .546). On average, Black families had to wait 9.2 days (confidence interval [CI] 6.6–11.8) for an appointment and Hispanic families 8.0 days (CI 5.5–10.5), while the Muslim families had to wait 5.9 days (CI 3.8–8.0), and White families 6.5 days (CI 3.8–9.1). The child's identity was not found to have a significant effect on wait time (F(3,87) = 1.474, p = .227).
Discussion
The hypothesis that children with minoritized identities and public insurance would face more barriers to accessing rehabilitation services was found to be partially true. While public insurance was not a predictor of reduced access, Black and Hispanic families had a harder time getting appointments than White and Muslim families. These findings are dissimilar to the findings of Fuentes et al. who found longer wait times for children with public insurance. 7 Overall, simulated families experienced substantial access barriers regardless of telegraphed minoritized identity or insurance type. Simulated mothers had to make multiple call attempts because no one answered the phone, the clinic did not take their insurance, or because appointments were not available. Nearly a third of the simulated sample had to seek an appointment at an alternative location. Appointment availability was worse in West Virginia than in Eastern Ohio and Western Pennsylvania. Poor access to therapy services is a long-standing well-known problem nationally, and children with disabilities (especially those with other minoritized identities) tend to face more barriers to care than their non-disabled peers.15–18 This speaks to the importance of addressing equity for those minoritized identities that intersect with disability and chronic health care needs. 19
This study has notable limitations. First, the results are limited to the geographies of the tri-state area of Western Pennsylvania, Eastern Ohio, and West Virginia, similar to the Fuentes et al. study. 7 Second, some of the therapy clinics required completion of intake forms and proof of a prescription before offering an appointment opportunity which, notably, would pose an added challenge to families seeking care. And third, due to the requirement to seek substitutions, some clinics were called more than once by different simulated families. Lastly, while names do ‘telegraph’ or ‘signal’ identities, the recipient of the signal may not interpret it as it was intended and may also ascribe social status to the name.11,20 Despite these limitations, this audit study demonstrates the substantial challenges families face in accessing rehabilitation therapy care for their children with disabilities and highlights the intersecting impact of disability, race and ethnicity, and socioeconomic status on healthcare access and health outcomes. Clinical programs should be aware of inequities in access for their patients with disabilities and should develop strategies to reduce them.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.