
Abstract
Purpose
Twenty percent of childhood cancer survivors experience physical function impairments, and ∼75% develop a chronic health condition. Physical and occupational therapists (PT/OTs) can mitigate these late effects, yet few children receive cancer rehabilitation (CR). This research aimed to identify provider attitudes and perspectives towards CR services for children across inpatient and outpatient settings at a cancer center.
Methods
Three cardiac rehabilitation instruments were adapted to evaluate knowledge, attitudes, and perceptions regarding CR delivery. Descriptive statistics were used to summarize participant survey results.
Results
Twenty administrators, 20 physicians/advanced practice providers (APPs), and 20 PT/OTs completed surveys. All disciplines strongly agreed on the value of CR for patient outcomes and care quality. Barriers to CR access included insurance models that disincentivize healthcare systems from providing CR, lack of a standardized screening and referral process, and inconsistent patient participation. Physicians/APPs (81%) endorsed clinical practice guidelines (CPGs) to promote CR referrals, and 90% of PT/OTs agreed hybrid CR delivery, which includes both supervised and unsupervised exercise, would increase patient participation.
Conclusion
This study identified opportunities to increase CR access for childhood cancer survivors, including CPGs, streamlining referral processes, hybrid CR delivery, and closing insurance gaps. Future research should address these factors to improve CR access and ultimately improve outcomes for pediatric survivors.
Background
Advances in the treatment of children/adolescents with cancer have significantly improved the five-year post-diagnosis survival rate, now exceeding 80%. 1 However, despite these improvements, 62–74% of survivors will develop a chronic health condition related to the adverse effects of cancer and its treatment. 2 Survivors are also five times more likely than their healthy siblings to experience difficulties in participating in activities of daily living. 3 Notably, 20% of survivors have significant physical function impairments affecting their neurologic, musculoskeletal, and cardiopulmonary systems 4 and up to 32% experience symptoms of prefrailty or frailty during young adulthood, comparable to the rates in the geriatric population. 5
During cancer treatment, children/adolescents often begin to experience reduced physical activity compared to their peers, 6 and the effects of chemotherapy and radiation on cardiac and skeletal muscle further hinder the return to physical activity post-treatment. 4 This reduction in physical activity further compounds the risks of cancer-related late effects such as obesity, metabolic syndrome and low mineral bone density. 7
Cancer rehabilitation (CR) refers to a comprehensive, multidisciplinary program of care focused on restoring and maintaining function and health-related quality of life in cancer patients and survivors throughout the continuum of care, allowing for transitions between inpatient and outpatient treatment. 4 CR can alleviate functional impairments caused by peripheral neuropathies, sensory loss, neurocognitive impairment, chronic fatigue, chronic pain, muscle atrophy, and bone loss.3,8 An essential component of CR is combined resistance training and aerobic exercise which has been shown to improve fatigue, cardiorespiratory fitness, physical activity levels and health-related quality of life in children and adolescents with cancer. 9
Physical and occupational therapists (PT/OTs) play a crucial role in CR, developing goal-oriented plans with patients aimed at restoring function when full recovery is expected and optimizing adaptations when full recovery is not. 4 Early CR interventions can boost motivation to participate in personal care, leisure activities, school-based tasks, and vocational pursuits. 8 Participation in CR can also mitigate cognitive decline and promote an active lifestyle. 10 Rehabilitation provided to children/adolescents with cancer results in improvements in strength and flexibility of the musculoskeletal system 11 and improves pain, functional abilities, sensory motor function and quality of life. 12 It can also increase self-efficacy and physical activity expectations, helping children/adolescents avoid the sedentary lifestyles that contribute to secondary cancers and comorbidities post-treatment. 13
Despite the benefits of rehabilitation, research has shown that CR utilization is limited among childhood cancer survivors. A large retrospective cohort study of more than 5000 children with leukemia revealed that less than 30% received physical therapy within the first year after diagnosis and only 55.7% of those subsequently diagnosed with a neuromuscular condition received it. 14 In a prospective study of over 9000 childhood cancer survivors, less than 9.2% reported physical therapy utilization. 15
Recent studies have identified significant obstacles to rehabilitation utilization in children/adolescents with cancer. A survey of Children's Oncology Group member institutions revealed that 76% did not have established rehabilitation programs for children/adolescents with cancer, and 48% did not conduct any prospective surveillance for rehabilitation needs. 16 Additionally, 65% of participating physicians cited a lack of education regarding CR during medical training. 16 A survey of Canadian pediatric PTs and oncology providers found inadequate delivery of rehabilitation services at half of the programs, especially in outpatient settings. 17 This may partially explain why many children with cancer have identified functional needs but are not referred for CR.
In the absence of available CR programs, alternative approaches to increase physical activity in cancer patients have been developed and studied. 18 These too have demonstrated benefits in cardiovascular fitness and body composition.19,20 This is significant since adult survivors of childhood Hodgkin's lymphoma who adhered to vigorous activity guidelines had a 51% decrease in cardiovascular events compared to those who did not meet the guidelines. 21 However, these programs are rare, with only 46 identified across 10 countries (of which 21 were in Germany), and only 3–5 identified in the U.S. 22
The period during and following cancer therapy may be a critical window for childhood cancer survivors to regain or maintain physical function through CR programs. Preserving physical function might significantly impact long term functional independence, increase participation in leisure and work-related activities, and reduce cancer treatment late effects. However, many children/adolescents with cancer do not have access to CR programs that support physical activity. Barriers to CR access for children/adolescents with cancer are also underexplored. Thus, to improve CR access for children/adolescents with cancer during both inpatient and outpatient treatment, further research is needed to elucidate the barriers to pediatric CR access at the level of providers and healthcare systems. This report describes the results of a cross-sectional survey investigating attitudes and perspectives of pediatric oncology providers and hospital administrators towards CR delivery as part of a larger study on disparities in access to pediatric rehabilitation at a cancer center.
Methods
Study design
The surveys selected for this study included cardiac rehabilitation instruments adapted by the study team for use with cancer providers as there were no published surveys focused on system-level CR service delivery.22–25 Specifically, the word “cardiac” was changed to “cancer,” and all other aspects of the scales were largely unchanged from the original versions. The use of surveys originally intended to assess cardiac rehabilitation programs to evaluate a CR program is based on the applicability of the cardiac rehabilitation model to the CR context. Specifically, cardiac rehabilitation is characterized by a multimodal care delivery model that integrates prescriptive exercise, medical evaluation, risk mitigation, education, counseling and behavioral management. 26 Both types of rehabilitation incorporate regular aerobic and resistance training and have demonstrated positive outcomes in cancer patients. 27 In fact, the success of cardiac rehabilitation has led to the development of cardio-oncology rehabilitation programs that leverage the infrastructure and success of cardiac rehabilitation programs to manage cardiovascular outcomes in cancer patients. 27 The surveys were chosen for their strong face validity; the questions directly reflected the information relevant to study objectives. Following approval by the Institutional Review Board (IRB#2021-0893), participants were recruited from the cancer center to complete surveys between December 2021 and April 2022. All surveys contained an informed consent statement requiring agreement by the participant prior to beginning survey questions. All data were kept strictly confidential and de-identified prior to analyses.
Study population and procedure
Previous research has identified that barriers to adult CR occur at patient, provider, healthcare system, payor, and policy levels. 28 Thus, this study recruited three separate groups of healthcare staff (e.g., stakeholders) that work with children/adolescents with cancer or make decisions that affect this population at the cancer center in the inpatient and outpatient settings. 29 This study included these three unique groups to gain an understanding of facilitators and barriers to rehabilitation services from employees in the healthcare system with a wide variety of perspectives and job priorities. These groups included healthcare administrators (n = 20), physicians/advanced practice providers (APPs; n = 20), and PT/OTs (n = 20).
The cancer center employs approximately 20,000 staff members. During the study period, there were 233 employees in the Division of Pediatrics (73% female, 37% White, 16% Black, 17% Hispanic, 29% Asian) and the mean age was 46. Of these, 22 were pediatric clinical oncologists and 12 were pediatric APPs. In the Rehabilitation Department, there were 13 pediatric PT/OTs at the time of this study and an additional 100 adult PT/OTs, some of whom floated to pediatrics to cover service gaps. There are approximately 12,000 pediatric CR encounters per year.
The study used purposive, convenience sampling and snowball sampling techniques. Eligible hospital administrators included employees that held executive administrative or leadership positions and were involved in inpatient or outpatient hospital operational decisions regarding pediatrics, survivorship, rehabilitation, cancer control or health policy. Since many administrators were from outside the Division of Pediatrics, eligible administrators were initially referred to the study by the Division of Pediatrics Administrator and by the Executive Director from the Office of the Chief Operating Officer. Subsequent participants referred additional participants until target enrollment was achieved. Pediatric oncology staff physicians and APPs were eligible if their primary role involved the inpatient or outpatient clinical care of children/adolescents with cancer. Recruitment continued until 20 participants were enrolled. Due to the small number of designated pediatric PT/OTs, participants were also recruited from the pool of adult PT/OTs who floated to pediatrics until 20 therapists were enrolled.
The study investigators made initial contact through email invitations, including the use of group emails that included all physicians/APPs in the Division of Pediatrics and all PT/OTs employed in the institution. Additional announcements regarding study participation were made at Division of Pediatrics and Rehabilitation Department meetings. Potential participants identified through all sampling techniques were re-contacted up to five times, through all routes of published contact information including email, business phone, and appropriate administrative assistant contact. After-hour study visits were offered to enhance recruitment and retention.
In appreciation for their time, the healthcare administrator or clinical provider was given the option to be recognized for their participation by receiving an “Awesome Job Award” through the institution's internal recognition system. This non-monetary award is a brief written “shout-out” that is emailed to the recipient and their manager and highlights their participation in the study's initiative to improve rehabilitation access for cancer patients at their institution. Efforts were made to purposefully recruit staff representing widely divergent backgrounds that included ethnicity, race, gender, sexual orientation, minority groups, and persons with disabilities to be fully inclusive of a variety of cultural and social perspectives. Demographic information including age, gender identity, educational level, race, ethnicity, and occupation were collected from all participants. Survey instruments were administered based on self-reported occupation. Descriptive statistics were used to summarize cohort characteristics and survey outcomes.
Outcome measures
Healthcare administrator survey of attitudes towards CR
The survey instrument for healthcare administrators used in this study was adapted from a published survey by Grace et al. that assessed healthcare administrators’ perceptions and attitudes towards cardiac rehabilitation. 24 This revised survey elicited health administrators’ attitudes towards CR services for children/adolescents with cancer. The survey contained four knowledge items (response range: 1 = poor to 5 = excellent), five perception items (response range: 1 = not even considered to 5 = extremely important), and 14 attitude items (Likert response: 1 = strongly disagree to 5 = strongly agree). A high summary score was suggestive of more positive knowledge, perceptions, and attitudes toward rehabilitation.
Physician/APP attitudes toward CR and referral
The physicians/APPs completed the Physician Attitudes toward Cardiac Rehabilitation and Referral (PACRR) scale, which the study team adapted for cancer providers. 23 The PACRR scale was chosen because it specifically surveyed clinician attitudes towards rehabilitation within domains that could affect patient access at their institution. The PACRR is a 19-item scale that uses a Likert response format (response range: 1 = strongly disagree to 5 = strongly agree). 23 It includes four categories: referral norms (six items), referral process (two items), preference to manage patients independent of rehabilitation (seven items), and perceptions of program quality (four items). A higher score indicated a more positive attitude toward rehabilitation and referral to rehabilitation services.
Perceptions of PT/OTs on CR delivery
A previously published survey by Servio et al. measuring rehabilitation providers perceptions of cardiac rehabilitation service delivery was adapted for use with PT/OTs delivering CR. 25 This adapted survey assessed PT/OTs’ perceptions of delivering CR to children/adolescents with cancer. It had 12 items and used a Likert response format (response range: 1 = strongly disagree to 5 = strongly agree). The survey included three domains: facilitators (three items), barriers (five items), and delivery of comprehensive CR (four items). A higher score meant more positive perception within each domain.
Results
Overall, all eligible administrators approached through snowball sampling agreed to participate in the study as well as 59% of the physicians/APPs and 100% of pediatric PT/OTs working in the Division of Pediatrics. Table 1 provides a summary of the participant characteristics. The average age of healthcare administrators (n = 20) was 49.95 years (standard deviation [SD] = 7.7). Females comprised 65% of this group, and 65% of administrators reported being non-Hispanic White. Physicians/APPs (n = 20) had an average age of 43.4 years (SD = 8.5). Females comprised 65% of the physician/APP group, and 75% self-reported as non-Hispanic White. PT/OTs (n = 20) had an average age of 38.3 years (SD = 11.4), and 85% were female; 65% of PT/OTs were non-Hispanic White. The study participants’ mean age (43.8 years) and majority female gender (72%) were representative of the Division of Pediatrics; however, they were less racially and ethnically diverse than the division as a whole (68.3% vs. 37% non-Hispanic White).
Demographic characteristics.
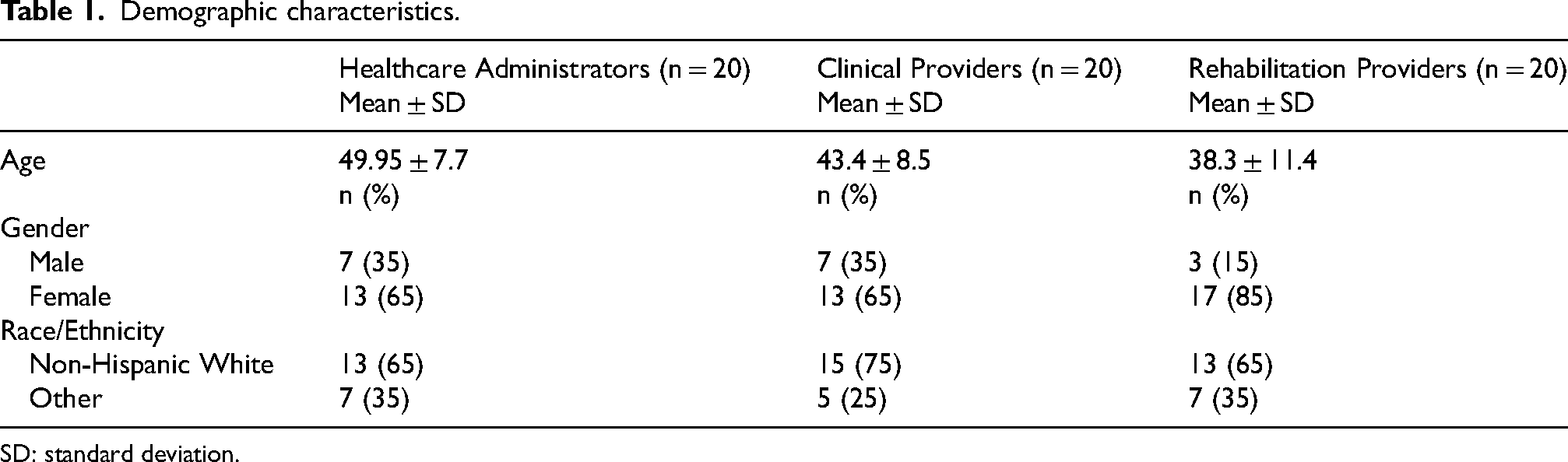
SD: standard deviation.
System-level perspective (healthcare administrators and CR)
Administrators reported a “good” level of CR knowledge on average (Table 2, section A). Components of the CR knowledge assessment included knowledge of what CR entails, rates of patient participation in CR, personal CR awareness, and perceived knowledge by their colleagues. Administrators reported knowledge in each of these components as “good”.
Healthcare administrator cancer rehabilitation (CR) survey results.
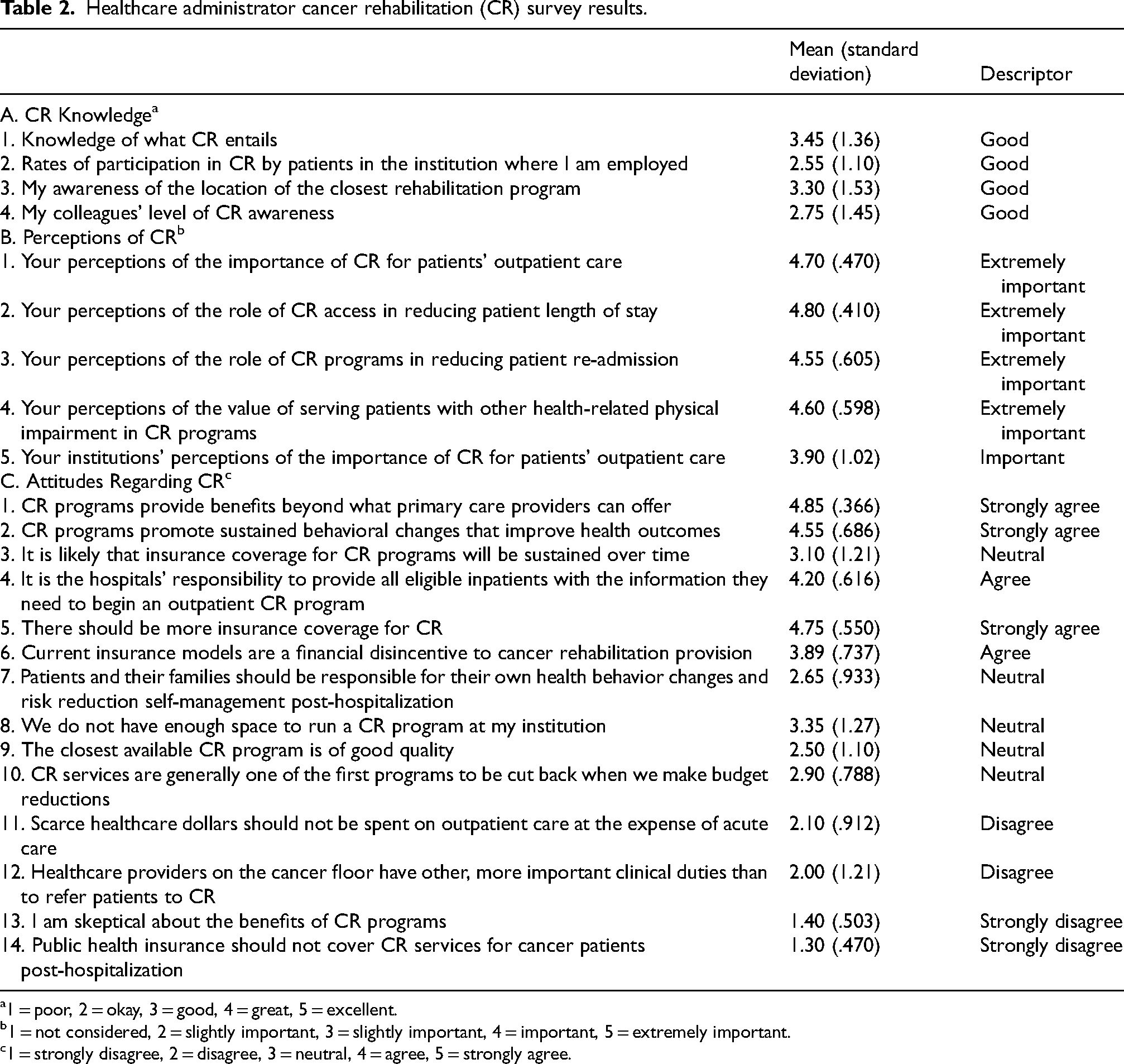
1 = poor, 2 = okay, 3 = good, 4 = great, 5 = excellent.
1 = not considered, 2 = slightly important, 3 = slightly important, 4 = important, 5 = extremely important.
1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree.
Additionally, administrators perceived CR to be “extremely important” on average. Administrators reported the value of CR as “extremely important” for general outpatient care, reducing length of stay and readmissions, and serving children/adolescents with cancer with other health-related impairments. They also reported that the institution perceived CR as “important” (Table 2, section B).
There was consensus (100% marked “agree” or “strongly agree”) that CR programs provide benefits beyond those that primary care providers can offer a patient, and no administrators reported skepticism about the benefits of CR (Figure 1 and Table 2, section C). Administrators “agreed” that hospital staff should educate inpatients on how to enroll in outpatient CR programs, “disagreed” that inpatient providers were too busy to refer to CR, and were neutral on whether children/adolescents with cancer and their families should be responsible for their own health behavior changes post hospitalization. They had neutral responses towards the quality of the closest available CR program and whether there was enough space to run a CR program in their institution. There was “strong agreement” that more insurance coverage is needed for CR, “agreement” that current insurance models disincentivize hospitals from providing CR, and “strong disagreement” that public health insurance should deny outpatient CR services. There was a neutral response regarding whether insurance coverage for CR would be sustained over time. Table 2 summarizes responses to each survey question.
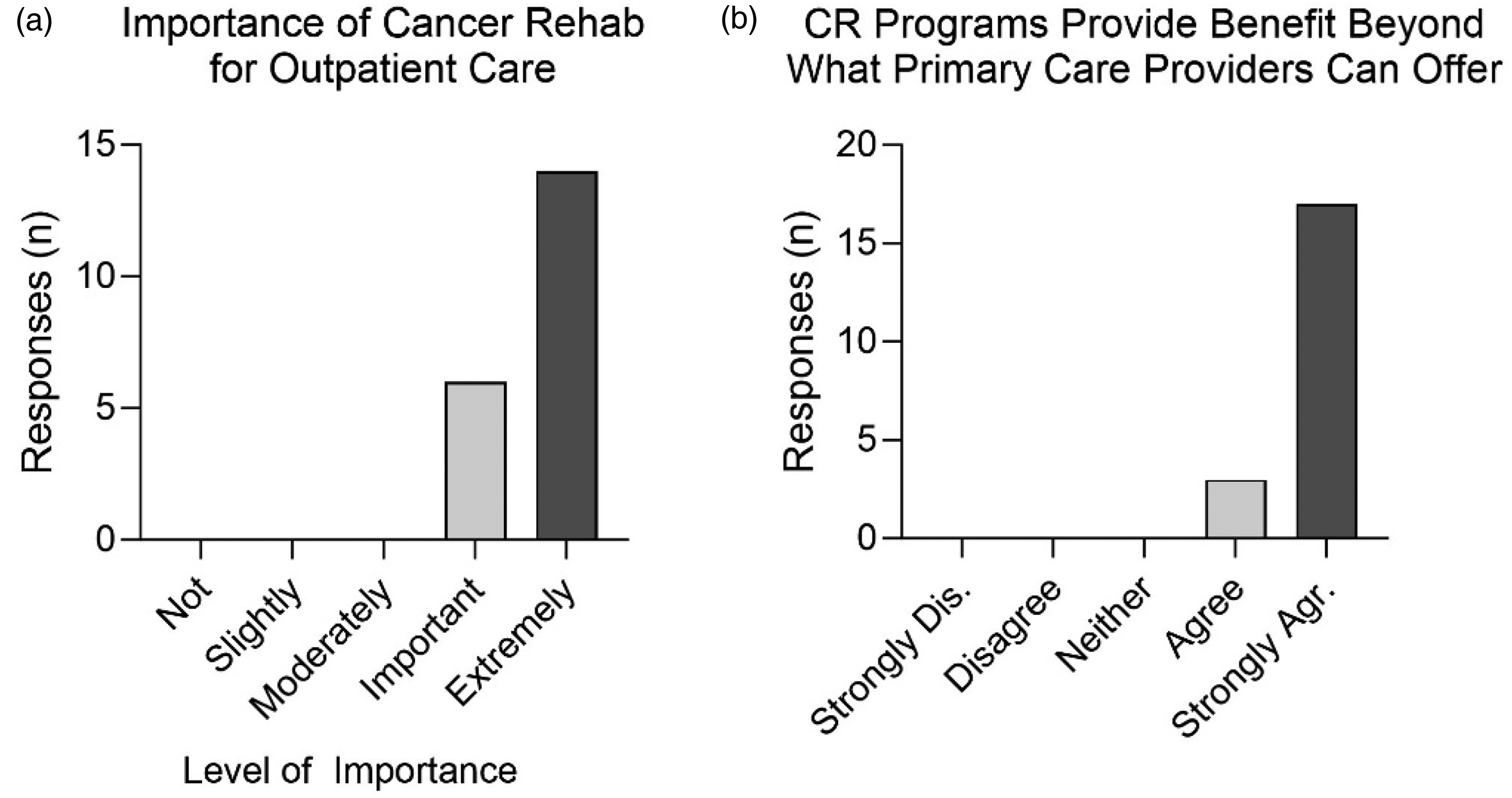
Administrators perceive value in cancer rehabilitation (CR). Administrators’ responses to (a) “Your perceptions of the importance of CR for patients’ outpatient care” and (b) “CR programs provide benefits beyond what primary care providers can offer.” N = 20 responses to each survey question. Dis.: disagree; Agr.: agree.
Physicians/APPs attitudes toward CR and referral
Physicians and APPs were surveyed on referral norms. Eighty-one percent of them “agreed” or “strongly agreed” that clinical practice guidelines (CPGs) promote CR referrals, 95% “agreed” or “strongly agreed” that they generally intend to refer children/adolescents with cancer to CR, and 81% “agreed” or “strongly agreed” that their colleagues generally refer children/adolescents with cancer to CR (Figure 2(a)). Most of the physician/APPs (71%) did not believe that referrals were inconvenient to make, though results were mixed as to whether there is a standard referral form for CR (Table 3, sections A and B).
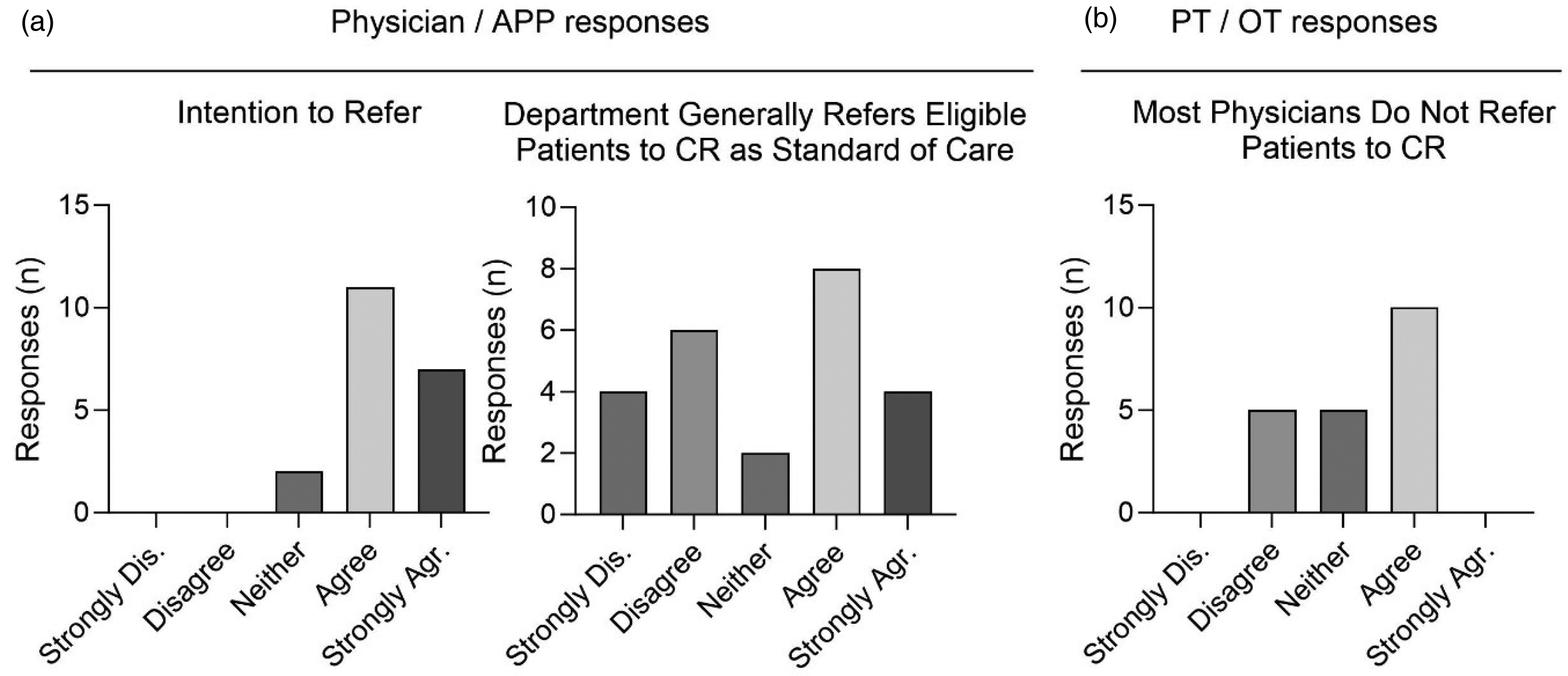
Attitudes toward referral to cancer rehabilitation (CR) varied among clinical providers. (a) Physicians’/advanced practice providers’ (APPs’) responses to “I generally intend to refer patients to CR” and “My department generally refers all eligible patients to cancer as a standard of care”. (b) Physical therapists’/occupational therapists’ responses to “Most physicians do not refer patients to CR.” N = 20 responses to each survey question. Dis.: disagree; Agr.: agree.
Physicians’/advanced practice providers’ attitudes toward cancer rehabilitation (CR) and referral.
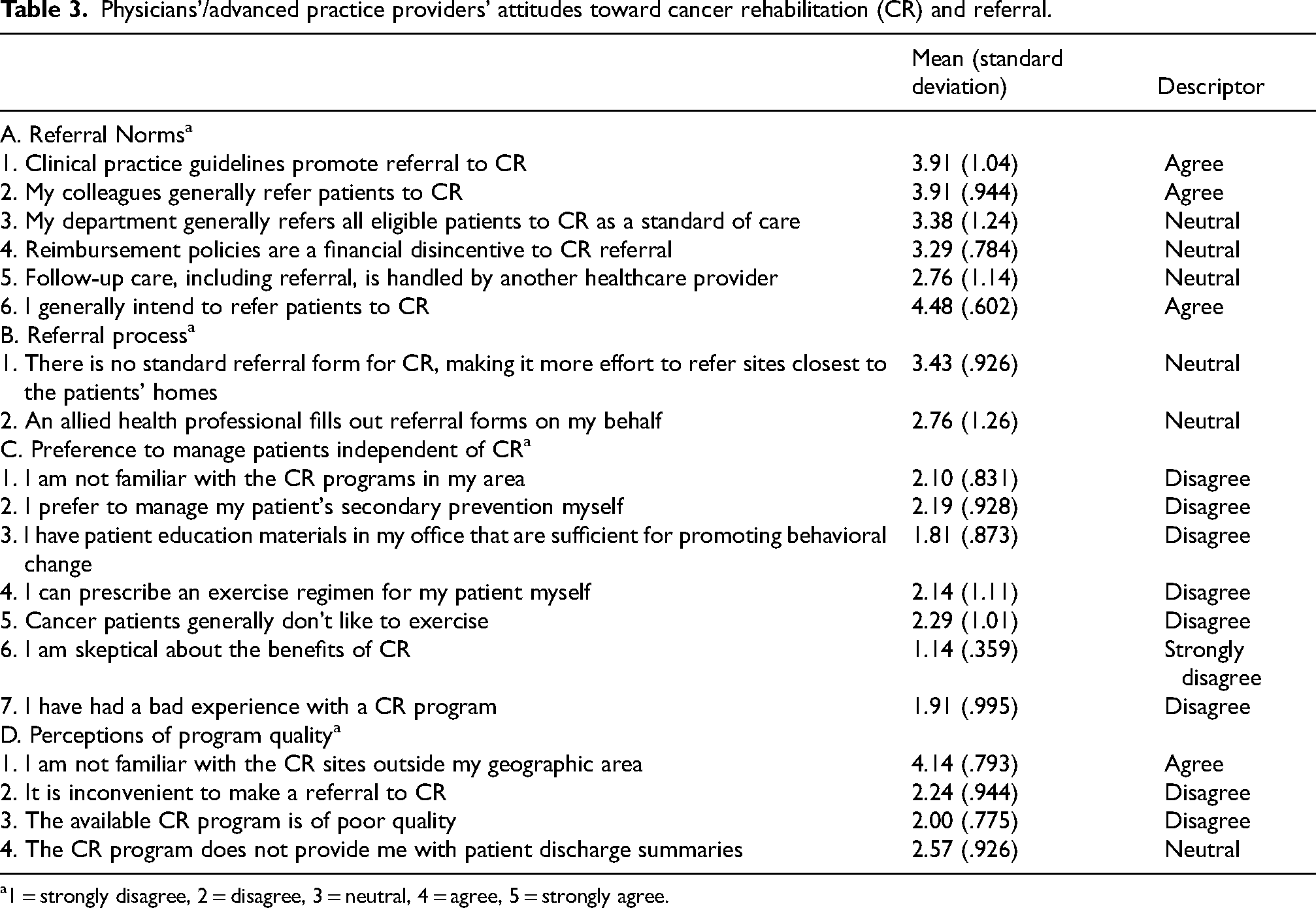
1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree.
Physicians/APPs did not indicate a preference to manage patients independent of CR (Table 3, section C). Ninety percent of this group “disagreed” or “strongly disagreed” that they had sufficient resources to promote behavioral changes. They also “disagreed” with personally managing children/adolescents’ secondary cancer prevention and exercise regimens. Notably, none of the physician/APPs were skeptical of the potential benefits of CR.
Not surprisingly, physicians/APPs were familiar with CR programs within their geographic area, but not outside of their area (Table 3, section D). They “disagreed” that the cancer center CR program was of poor quality and were “neutral” about whether the CR program provided patient discharge summaries.
Perception of CR staff on CR delivery
PT/OTs agreed that CR participants were aware of the benefits of participation (Table 4, section A). The rate of absenteeism might be an obstacle to facilitating CR, as PT/OTs were neutral when asked whether the rate of absenteeism was low. Notably, 90% of PT/OTs “agreed” or “strongly agreed” that hybrid CR delivery, which includes a combination of both supervised and unsupervised exercise, could increase participation to facilitate CR.
Perception of cancer rehabilitation staff on delivery.
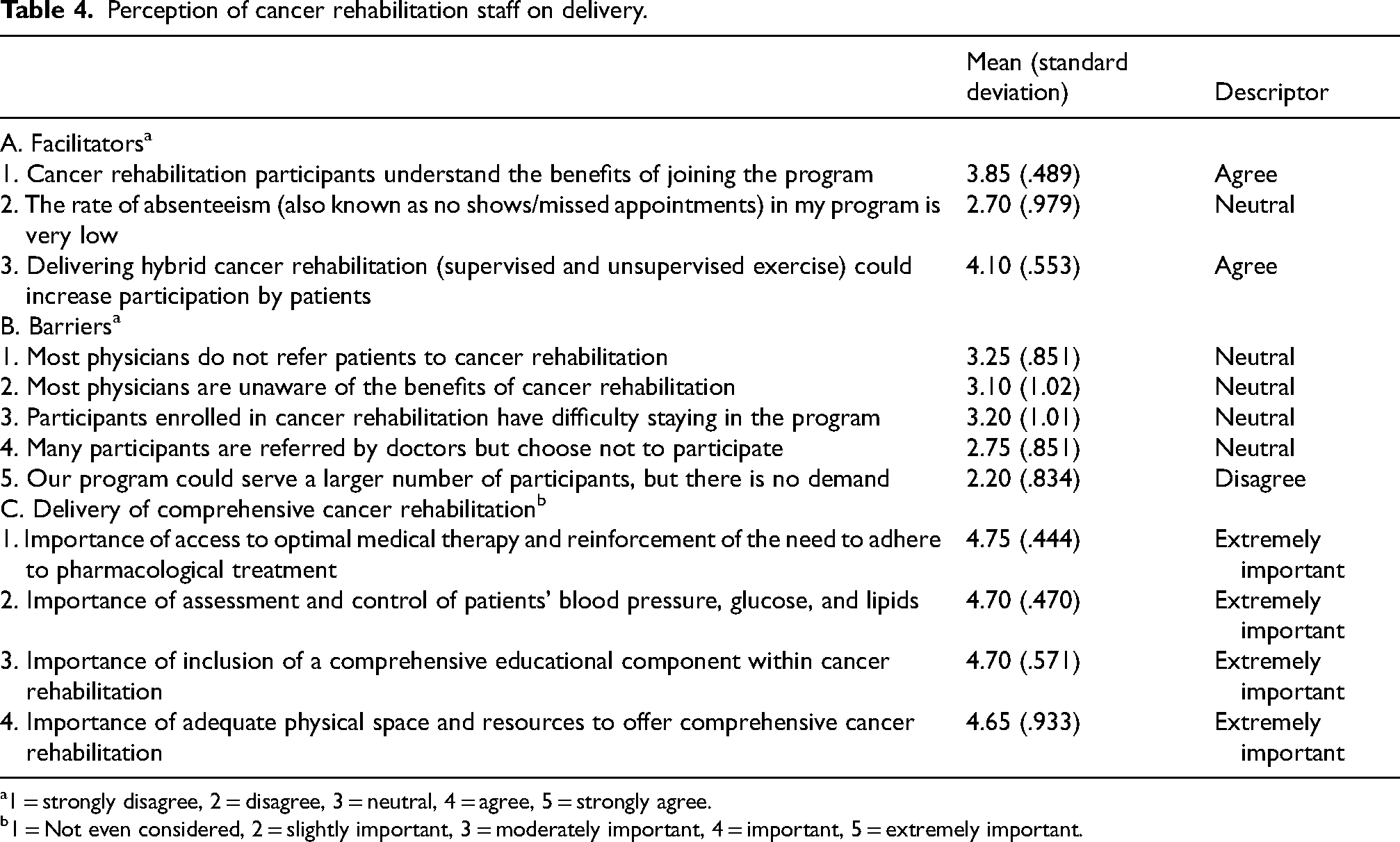
1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree.
1 = Not even considered, 2 = slightly important, 3 = moderately important, 4 = important, 5 = extremely important.
Some potential barriers to CR were identified (Table 4, section B). There were mixed beliefs on whether physicians refer children/adolescents with cancer to PT/OT (Figure 2(b)) and whether physicians were aware of the benefits of CR. There were also mixed responses on CR program retention. PT/OTs denied a lack of demand for CR programs, with 90% responding “disagree” or “strongly disagree.”
All components of ‘delivery of comprehensive CR’ were deemed extremely important by PT/OTs (Figure 3 and Table 4, section C). Participants believed that including comprehensive health education components into CR and having adequate physical space and resources for a comprehensive CR program were important.
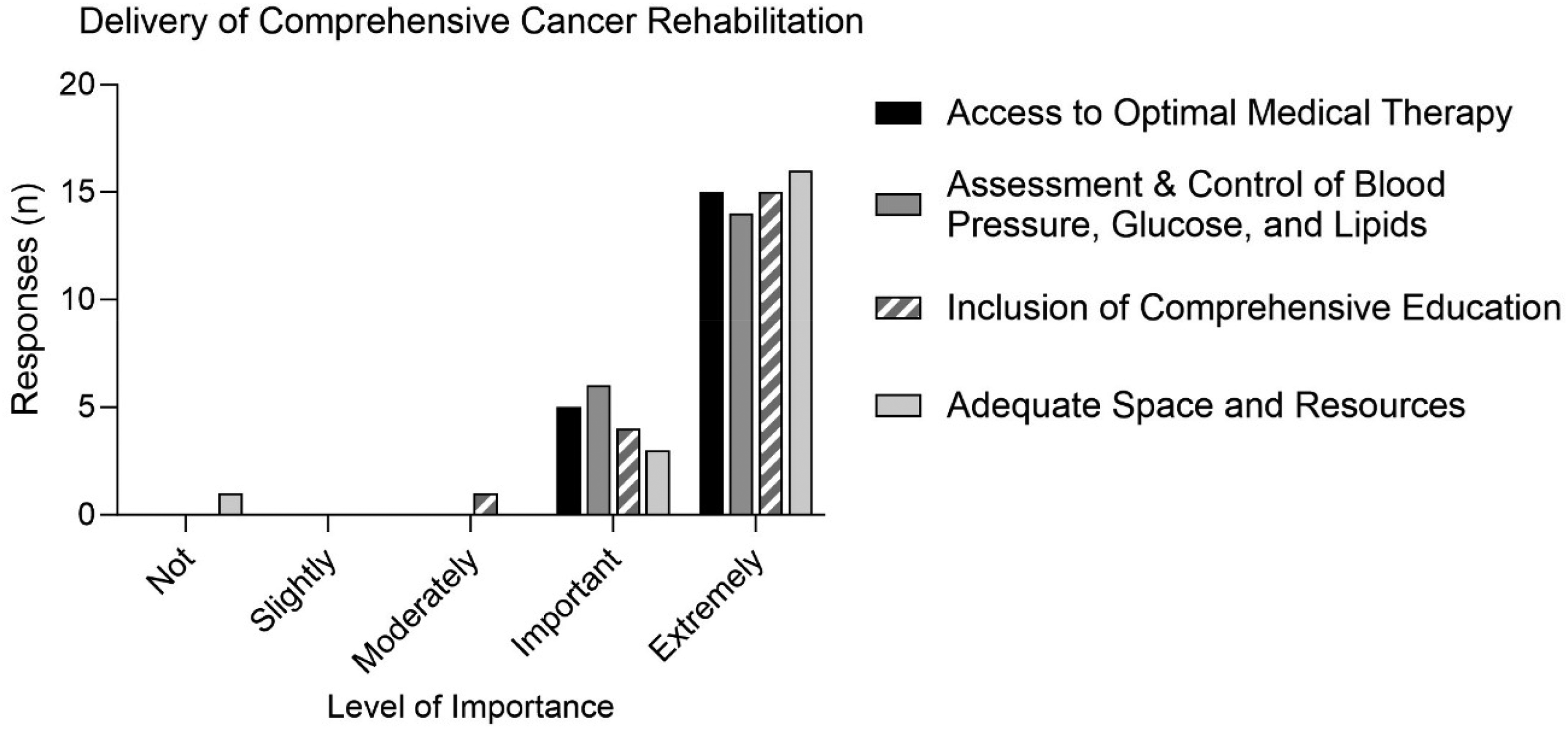
Physical therapists (PTs) and occupational therapists (OTs) agree that delivery of comprehensive cancer rehabilitation is extremely important. PT/OTs ranked perceived importance of four categories: access to optimal medical therapy and reinforcement of the need to adhere to pharmacological treatment; assessment and control of patients’ blood pressure, glucose, and lipids; inclusion of a comprehensive educational component within cancer rehabilitation; adequate physical space and resources to offer comprehensive cancer rehabilitation. N = 20 responses to each.
Discussion
The integration of CR into comprehensive cancer care across settings is necessary to ensure optimal functional outcomes for children with cancer.13,30 Despite its recognized value, many children/adolescents do not have access to CR and barriers to accessing these services for children/adolescents with cancer are underexplored. 16 The current study provides novel insight into the current barriers to pediatric CR access and potential solutions at the health care system level. Through the inclusion of administrators, oncology providers and PT/OTs, a broader array of barriers to rehabilitation care was more likely to be identified than if the study had been limited to only one discipline since each group had different job-related priorities, knowledge and experience impacting their perspectives on rehabilitation barriers. This approach also facilitated the development of comprehensive solutions that encompassed the provider referral process, therapist accessibility, and care access within the cancer system.
Across all three disciplines surveyed (administrators, PT/OTs, and physicians/APPs), there was strong endorsement for the value of CR in both inpatient and outpatient settings to improve patient outcomes and key quality indicators. Administrators also supported investment of health care dollars in outpatient CR. This consensus suggests that the culture at the health care system studied is conducive to enhancing CR delivery. Evidence suggests that multidisciplinary collaboration is key to optimizing CR delivery in both children and adults with cancer.31–33 Collaboration between PT/OTs and physicians/APPs is fostered by an increased awareness of CR benefits and a shared understanding of the value of CR in the oncology population. 31 This study illustrated that OT/PTs, physicians/APPs, and administrators agreed on the importance of CR and were aware of the benefits of CR, suggesting that multidisciplinary collaboration is within reach.
This study also identified opportunities to improve CR delivery in both inpatient and outpatient settings at the cancer center. For example, physicians/APPs believed CPGs promote CR referral. These findings are comparable to those of a similar survey study of PTs in Canada. 17 When implemented as part of a multidisciplinary collaboration between PT/OTs and physicians, CPGs have been shown to improve referral rates of children with cancer to CR substantially. 32 Interestingly, physicians/APPs strongly agreed that they and their colleagues intended to refer children/adolescents with cancer to CR, but they had divergent opinions on whether referring to CR was a pediatric standard of care. Similarly, PT/OTs were split on whether they thought the physicians were making CR referrals. This suggests that despite the enthusiasm for CR, the process for CR referrals needs improvement. The development of a standardized CPG-driven referral process would optimize the timing of referrals to CR. In particular, the use of CPG-driven consultations for newly diagnosed children/adolescents with cancer upon hospital admission can be a vital way to connect patients to inpatient CR services and facilitate outpatient CR referrals. 16 Streamlining the referral process may minimize the burden on providers and lead to increased participation rates in CR. 34
Given the challenges identified in the CR referral process, the prospective surveillance model (PSM) has been proposed as an option to increase CR utilization without the requirement for oncologist-driven referrals. 16 This approach is an alternative to the traditional symptom-based or CPG-based referral system that relies on oncologists to identify patients with rehabilitation needs. It standardizes screening of all patients by rehabilitation specialists. The Stoplight Program at Children's Hospitals and Clinics of Minnesota is an example of an evidence-based PSM implemented for children with leukemia, in which baseline screening is used to grade impairments and rehabilitation needs. 35 Participants who completed the graded CR intervention demonstrated better body coordination, strength, agility, and speed compared to controls. 35 Another PSM implemented at the Huntsman Cancer Institute in the University of Utah Health system imbeds PTs in adult oncology clinics to provide ongoing patient monitoring using a mobility questionnaire to stratify and stage patients. Based on the stratification and staging, patients receive a targeted functional assessment and intervention. These programs illustrate the feasibility of prospective monitoring of function through repeated assessment as a standard of cancer care. 36
Integration of a CR patient navigator into the cancer care system is yet another way to ensure that patients are screened at the appropriate time and referred to CR. Cancer centers have used patient navigators to improve care coordination and decrease disparities in access to cancer treatments. 37 A CR patient navigator could also facilitate referrals to rehabilitation. As an example, patient navigators have been successfully integrated into cardiac rehabilitation programs and have been proven effective for promoting utilization of cardiac rehabilitation in patients after hospitalization for a cardiac event. 38 A CR patient navigator with a rehabilitation therapy background implemented in a large southeastern cancer center was shown to improve timely identification and management of adults with functional deficits and improved patient participation in CR 39
Rehabilitation providers at the institution were split on whether patients have difficulty adhering to CR programs. Hospitalized children with cancer have demonstrated non-adherence to 15–24% of physical therapy sessions. 18 Hybrid delivery, which was strongly endorsed by the PT/OTs to improve patient participation in CR, allows flexibility in CR delivery mode and could increase CR utilization and adherence. And, in adult cancer patients, when given a choice to do their exercises asynchronously (on their own time), the added flexibility has been shown to improve participation rates in CR programs. 40
PT/OTs strongly agreed that space was a critical component to a comprehensive CR program, yet administrators were mixed about whether there was adequate space for CR at the cancer center. Lack of or inappropriate space for rehabilitation was often noted by pediatric oncology rehabilitation therapists across Canada.17,41 The CREATE (collaboration, rehabilitation/research, education, assessment, treatment, and evaluation) team at Children's Hospitals and Clinics of Minnesota found that placing a rehabilitation space within the pediatric oncology clinic significantly increased provision of pediatric CR services. 32 Specifically, outpatient physical therapy utilization increased from 41% to 61%, and outpatient occupational therapy utilization increased from 6% to 23%. Having the space available for on-site CR would improve patients’ experience and make treatment more accessible. Furthermore, since most PT/OTs receive no training or education specific to pediatric oncology, 16 collocating PT/OTs within cancer centers could facilitate oncology education of these professionals. Similarly, this arrangement could facilitate education of oncologists about CR, as it did in Minnesota. 35
Telehealth CR delivery is a novel solution for limited available space for CR at a cancer center and/or lack of sufficient community resources. The utilization of telerehabilitation grew substantially during the COVID-19 pandemic and demonstrated feasibility and acceptability for children with chronic health conditions including cancer.42,43 Training programs for PT/OTs to use telerehabilitation with children have been published and trialed successfully.42,44 Research indicates that both patients and providers approve of telemedicine visits as a delivery mode for CR. 45 However, for patients without internet access, electronic devices, English language proficiency, or an insurance plan that will cover telerehabilitation, this option may widen existing disparities in CR access related to social determinants of health.39,46,47
In this survey, the administrators noted that current insurance models provide inadequate coverage for CR. In the outpatient population, high copays, no coverage, and Medicaid's “optional” rehabilitation benefits which limit annual visits and require referrals are all potential insurance barriers to CR access.48,49 In addition to providing timely screening and referrals, CR navigators can also address some insurance coverage barriers.38,39,50,51 A navigator can clarify insurance benefits, determine in-network CR providers, assist with getting prior authorization, and identify resources when coverage is inadequate or completely lacking. 37 Cancer treatment navigators have been shown to reduce disparities in care, expedite time to treatment, and improve care coordination among uninsured adults. 37 CR navigators may be able to provide a similar pathway to improve access for uninsured and underinsured children/adolescents to CR.
Other initiatives to improve health insurance coverage for CR will depend upon accumulated research and evidence on the impact of CR on morbidity and mortality, national consensus guidelines on clinical practice, and ultimately health policy changes that bolster the provision of CR for children with cancer. 48
The study had several limitations. The study team adapted a cardiac rehabilitation survey for use with cancer providers and used a closed-ended survey format. Nevertheless, the results aligned with the findings from other studies that surveyed cancer providers.16,41 Also, many survey items yielded neutral responses and reflected divergent opinions, precluding firm conclusions. Qualitative data would enrich the information gleaned from the surveys, and the study team plans to complete a qualitative interview study of the participants as a next step. The surveys across disciplines differed; therefore, the study team was not able to directly compare responses to survey questions or collapse results across disciplines. The non-probability method of participant recruitment also could have biased the results by potentially enrolling similarly minded employees. The participants were also not as racially and ethnically diverse as the overall employees of the Division of Pediatrics, which may have skewed the results. The study findings are also limited by the small sample size and inclusion of a single cancer center, which limits generalizability of the results.
Conclusion
Overall, survey results suggested that CR services for childhood cancer patients are highly valued by healthcare administrators and clinical providers, and the culture is ready for a full-scale multidisciplinary collaboration to promote CR. However, key opportunities were identified to improve pediatric CR service delivery that require action from all three stakeholder groups. These included (1) developing a standardized CPG-driven referral process, (2) identifying outpatient clinic space and leveraging hybrid rehabilitation and telerehabilitation to increase CR participation, and (3) implementing a plan (such as the patient navigation model) to overcome insurance-related barriers. Although this study was performed at a single cancer center, the results have broader applicability to other pediatric oncology centers, particularly those with nascent CR programs or even those without CR programs. That is because the need for CPGs to direct referrals, access to rehabilitation specialists, and advocacy for insurance coverage are needed universally. Future studies should evaluate the impact of these interventions on CR utilization and clinical outcomes for children with cancer, potentially setting new standards for pediatric oncology care.
Footnotes
Acknowledgments
Support provided by an NIH/NCI Cancer Center Administrative Supplement Grant (P30CA016672-454S PI Moody, MDACC). Additional salary support was provided by the UTHealth Houston-Cancer Prevention Research Institute of Texas Innovation for Cancer Prevention Research Pre-Doctoral Fellowship (RP210042). We also want to thank our survey participants for completing the surveys to help us improve access to pediatric cancer rehabilitation services.
Ethical considerations
This study was approved by the Institutional Review Board (IRB# 2021-0893) and informed consent from participants was obtained.
Author contributions
Conception and design: Karen Moody, Maria C. Swartz, Donna Kelly, Keri Schadler, Clark Andersen. Administrative support: Alakh P. Rajan, Stephanie J. Wells, Eduardo Gonzalez Villarreal, Amy Heaton .Provision of study materials or patients: Karen Moody, Maria C. Swartz, Donna Kelly, Keri Schadler . Collection and assembly of data: Stephanie J. Wells, Karen Moody, Maria C. Swartz, Clark Andersen, Shiming Zhang . Data analysis and interpretation: Maria C. Swartz, Eduardo Gonzalez Villarreal, Keri Schadler, Alakh P. Rajan, Donna Kelly, Clark Andersen, Shiming Zhang, Amy Heaton, Karen Moody . Manuscript writing: All authors . Final approval of manuscript: All authors . Accountable for all aspects of the work: All authors
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for the authors was provided by an NIH/NCI Cancer Center Administrative Supplement Grant (P30CA016672-454S PI Moody, MDACC). Additional salary support was provided by the UTHealth Houston-Cancer Prevention Research Institute of Texas Innovation for Cancer Prevention Research Pre-Doctoral Fellowship (RP210042) and MD Anderson's Cancer Center Support Grant (CA016672).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Previous presentations
Abstract was previously presented at the General Poster Session at the 2022 ASCO Quality Care Symposium by Maria C Swartz.