
Abstract
Background:
Women’s role as patients is associated with power relationships embedded in society. Although trust in the health care system is a general prerequisite for positive health outcomes, practices regarding women’s agency in healthcare systems in Southeastern Europe reinforce women’s passivity. Most of the current psychological measures of trust have been constructed and validated in “WEIRD” (samples that are drawn from populations that are White, Educated, Industrialized, Rich, and Democratic) countries, thus having a limited application in other social contexts.
Objectives:
We aimed to construct an instrument for assessing women’s trust in healthcare systems to describe the structure of trust: Women’s Trust and Confidence in the Healthcare System scale.
Design:
Two independent samples (N1 = 329; N2 = 333) of adult women in Serbia voluntarily completed an online questionnaire. The questionnaire comprised 20 trust-related items which were selected from an extensive collection of women’s experiences in the healthcare system and evaluated by experts on a 5-point Likert-type scale.
Methods:
We used exploratory factor analysis of the Women’s Trust and Confidence in the Healthcare System scale to analyze the structure of trust in the first sample data set and validated it with the second sample using confirmatory factor analysis. We tested concurrent validity by exploring how women’s trust in the healthcare system predicts health-related behaviors (multigroup structural equation modeling). All analyses were conducted using R statistical software.
Results:
The Women’s Trust and Confidence in the Healthcare System scale (Cronbach’s alpha = 0.86) indicated a three-factor structure of trust in the healthcare system: trust in healthcare professionals, distrust in the public healthcare system, and confidence in healthcare system. This was validated using an independent sample. Interpersonal trust positively predicted women’s desirable health behaviors, while trust in the system had a negative impact.
Conclusion:
The Women’s Trust and Confidence in the Healthcare System scale captures women’s trust in a paternalistic healthcare system, is reliable, and has a stable three-factor structure. The study’s findings reveal the relationship between women’s trust and health-related behavior: in paternalistic environments, trust reinforces women’s passivity.
Keywords
Introduction
Trust in the healthcare system: definition and conceptualizations
Patient trust is the foundation of each interaction within healthcare systems and essential for positive treatment outcomes. 1 Trust between a patient and physician in a medical context can be defined as follows: The expectations of the public that those who serve them will perform their responsibilities in a technically proficient way, that they will assume responsibility and not inappropriately defer to others, and that they will make their patients’ welfare their highest priority.2,3 On a psychological level, trust requires relinquishing control over future actions performed by the agent (i.e. the physician), in whom patients place their trust, meaning that the certain level of trust always precedes, and, as previous research shows, shapes1,4–6 health-related interactions. Therefore, trust is a set of inter-dependable behaviors and beliefs that a person will act in certain ways and a complex neural process that binds diverse representations into a semantic pointer that includes emotions. 7 Trust can be generalized or particularized. 8 The former is social trust toward a relatively large circle of unfamiliar elements (e.g. healthcare system), whereas the latter is contingent on a particular situation, relationship, or person (e.g. healthcare provider). Whether generalized or particularized, trust serves as a heuristic decision-making rule, 9 enabling patients to navigate the complexities of medical information that would otherwise require unachievable knowledge for lay people. A distinction also exists between trust and confidence within the social work system 10 from which an analogy with the healthcare system can be drawn. For example, one can believe that a recommended therapy and medication are reliable, indicating confidence, while simultaneously not believing that the prescribing physician is sufficiently dedicated or trustworthy for any other aspect of life, indicating a lack of trust. Confidence in the healthcare system comprises assurance that the system is functional, evidence-based, and impersonal, which may be considered a foundation of the system’s structural and technological aspects; however, trust is personal and based on beliefs about and faith in other people (physicians) and their actions.
Correlates of trust in the healthcare system
Empirical findings show a strong consensus that trust in the healthcare system and physicians is associated with various patient health behaviors.3,11,12 Physicians’ cooperation with trusting patients is easier; patients’ trust in physicians is associated with their satisfaction, continuity of care and adherence to treatment, self-reported health improvement, and self-reported ability to manage chronic conditions. It facilitates healthcare access and the disclosure of relevant information and aids in making timely diagnoses.5,13–16 Patients are more likely to be open and disclose information if they trust their healthcare professional, and higher-quality interactions result in greater patient autonomy, patient agency, and shared decision-making.16–18 Essentially, trust increases patients’ involvement in their own treatment. Better medical outcomes, satisfaction, and reduced costs are achieved when healthcare providers form partnerships with their patients. 19 The patient’s involvement in treatment is a critical aspect of safe and sustainable people-centered health services and is recognized by the World Health Organization (WHO) as a key component of the physician–patient relationship. 20 Patients who are actively involved in their treatment are more likely to adhere to the prescribed treatment and less likely to be subject to exploitation, 21 which empowers them to better manage their health, and have trust in the healthcare system and providers supporting their health-related behavior.10,22
Conversely to the outlined benefits of high trust levels, low levels of patient trust are related to decreased doctor–patient interactions, suboptimal and unstable relationships with clinicians and the system, decreased adherence to physicians’ advice, worse self-reported health, and overall decreased use of healthcare services.5,13–15 Previous findings have also shown a strong relationship between trust and power, with less empowered people being significantly more trusting than those with greater power. 23
Women as patients within a paternalistic healthcare system
High trust appears to be the main factor to be nurtured to enhance the healthcare system, and this has been considered when developing interventions for increasing trust. 24 However, socialization as a female patient is associated with other power relationships embedded in society and the healthcare system where similarly women confront structural impediments that hinder their full participation in different aspects of society and are typically underrepresented in positions of power and decision-making roles. Social roles and power guide the direction and strength of trust relationships, 23 and trust precedes women’s health behavior.1,4 The trust relationship is always between at least two persons engaged in a psychological interaction in which the trustor (e.g. patient) is willing to rely on the actions of the trustee (e.g. physician). Trust generally serves as this mechanism, and is, therefore, always psychologically the same; however, the power dynamics within healthcare systems and the roles of patients, especially women, within those systems differ. The four main models of the physician–patient relationship are outlined in the seminal work by Emanuel and Emanuel: 25 the paternalistic, informative, interpretative, and deliberative models. Subsequent literature on this categorization has further emphasized individual patients’ independent expression of values and autonomy and included patient education.26–29 Over the past few decades, emphasizing patients’ roles in both literature and public policies, particularly their values, autonomy, and education, has led to a gradual shift from the paternalistic approach toward the deliberative model in healthcare systems. Unlike the recommended deliberative model, the paternalistic model, which represents the context of our study, aims to impose physicians’ power and neglect patients’ agency. 25 With power as an inexorable aspect of all social relationships, the paternalistic model forms “an adult–child relationship” that deteriorates women’s agency and autonomy. This is especially notable among women in Southeastern Europe, where the paternalistic model of the physician–patient relationship remains the dominant social norm despite being abandoned in official health policies (e.g. Article 51 of the Ethical Codex of Medical Chamber of Serbia states that, to increase patient involvement in treatment: “Doctor–patient relations must be based on mutual trust and responsibility, so that the patient actively participates in her treatment. Doctor must advocate for the respect of patient’s rights. Patient has the right to full loyalty of the doctor and all possibilities of his/her knowledge and skills” 30 ). Contingent on women’s treatment within healthcare systems, even those (more) deliberative ones, research on women’s roles as patients in Serbia paints a bleak picture. For example, birthing women’s passivity (as opposed to agency) is normalized to such an extent that old-fashioned practices (e.g. unnecessary episiotomy or induced labor) that define a woman as an inactive agent are frequent and not even subject to critical re-examination. 31 Women who dare speak out about their negative experiences are considered spoiled and ungrateful. Society teaches women that it can “always be worse” (sic.). When women are passive, disengaged, and lack a sense of agency or power, they will not fulfill their responsibilities, make informed decisions about their care options, or report symptoms until given permission and will thus endure more pain. As a consequence of the social structure of power and culture and access to healthcare, women in Serbia do not fully rely on the healthcare system. 31 For example, distant and cold relationships with healthcare providers that add to feelings of isolation and abandonment and lack of insight into and control over the birthing process when managed in the hospital without women’s subjective involvement have been reported to be particularly distressing aspects of the institutional environment during most childbirth experiences. 32 When interacting with the healthcare system, women experience feelings of isolation and abandonment and perceive a lack of communication, a caring relationship, and control and agency. 32 The paternalistic model emphasizes the repeatedly registered influence of gender on healthcare-seeking behavior.1,33,34 Gender stereotypes reduce women’s ability to challenge and assess their physicians’ competency, and women are more likely to be disregarded by physicians and have their experiences of medical symptoms discounted. 35 Even when they believe they have adequate information, women may not be fully informed about existing contraceptive options, indicating that women may not be actively involved in their own contraception choices. 36 Women are also subject to medical gaslighting, which includes misdiagnoses; denial of needed tests, medications, and treatments; dismissal from clinical care settings; and blame for “not trying hard enough” to recover. 37 For example, women may have their reported pain symptoms disregarded with psychological support recommended instead of pain medication. 38 Furthermore, greater trust in physicians was found to be related to increased blame of the doctor for other negative events that had occurred during the treatment, illustrating the complex interplay of agency, trust, and outcomes. 39 Thus, the patient role is shaped by societal norms and determines patients’ expectations of physicians and their own behavior, which is mediated by women’s trust in both healthcare providers and the system.15,35
Problem in this study
The conflict between the various psychosocial aspects of the patient role, such as women’s expected trust and responsibility on one side and reduced power and agency on the other, could cause women’s well-being to decline. 40 In Serbia, a disparity exists between the purpose of the healthcare system and the requirements for women’s behavior that the very same system imposes, which is enabled by the paternalistic model of the physician–patient relationship. In paternalistic systems, women’s trust in healthcare, both generalized and particularized, could be positively associated with their passive behavior (or even obedience) as patients, rather than with agency and autonomy, which are officially recommended. As almost all measures of trust in the healthcare system and/or physicians have been constructed and validated in the United States 41 and women’s diminished agency in paternalistic healthcare systems has been empirically established, 36 the role of women’s trust could differ from the data obtained in other societal contexts. The inappropriate conceptualization of trust could lead to errors in the assessment of trust in the healthcare system by emphasizing only the positive influence of trust on women’s health-related behavior while omitting the possible moderating effects of the healthcare system on the relationship between trust and women’s agency. This could lead to oversight of the possibility that women’s trust in paternalistic healthcare systems can be misused, as paternalistic treatment compromises patient autonomy and can result in patients being exploited. 4 For example, using a scale developed in the United States where the healthcare system is financed through compulsory payroll taxes and formally available to everyone, 42 to measure trust in the healthcare system among women in former Yugoslavian countries, could mask important aspects of the interplay between trust and health behavior. In short, inadequate measurements of trust could provide misleading findings and conceptualizations about the function of trust in the healthcare system and ultimately lead to public policy interventions being shaped without regard for possible misuse. Thus, in this study, we developed and validated a scale that measures women’s trust in the healthcare system in the Serbian context.
We derived an operational definition of trust in the healthcare system based on conceptual definitions outlined above, all of which include the interdependent behaviors, expectations, and intentions of two healthcare agents,1–7 and on empirical correlates of trust, such as power23,39 and health-related behavioral outcomes.1,3,11,12 Women’s trust in the healthcare system comprises beliefs in the good intentions and common goals of healthcare agents (regardless of whether they are persons or systems), which results in the adjustment of women’s power, control, and behavior.
Considering the lack of adequate instruments for measuring women’s trust in the healthcare system, paternalistic relationships within the Serbian healthcare system, and the possible influence on women’s diminishing agency as patients, our aim was threefold. First, we constructed the Women’s Trust and Confidence in the Healthcare System (WITCH) scale measuring women’s trust in the healthcare system in the context of the paternalistic system in Serbia. Second, we confirmed the factorial validity of the WITCH scale. Third, we explored the influence of women’s trust in the healthcare system on desirable health-related behavioral outcomes (e.g. adherence to physicians’ advice).
Method
Study design
We used a cross-sectional self-report survey design. The data were collected in two periods: directly prior to the onset of the COVID-19 pandemic and during the first year of the pandemic.
Sample
Samples were collected from two different participant groups, both comprising adult women from Serbia. Participants in Sample 1 (n = 329) were recruited before the first registered case of COVID-19 in Serbia (January–February 2020), while the data for Sample 2 (n = 333) were collected during the first year of the pandemic (March 2020–March 2021). The target sample size for each group ranged from 180 to 360, corresponding to the recommended ratio of N > 5–10:1 (i.e. ratio of the number of participants to the number of items on the scale). The sample structure based on participants’ number of children, socioeconomic status, employment status, and education level is presented in Supplemental Appendix A, Table A1.
Procedure
Participants were recruited online via Facebook advertisements and using the snowball method. After providing written informed consent, participants evaluated items related to women’s subjective perceptions of real and potential experiences in the healthcare system, their experiences during, receiving, or upon hearing their diagnosis, related privacy issues, and perceptions of the behavior of medical workers. Subsequently, participants answered questions that were part of the WITCH project but were not analyzed in this study. At the end of participation, they were presented with demographic questions, followed by a thank you note.
As this study is part of a larger research project dedicated to exploratory research on women’s experiences with the healthcare system in Serbia in general, all participants responded to a comprehensive list of items concerning different aspects of women’s experiences in and perceptions of the healthcare system, including trust. All items included in the analyses in this study were evaluated on a 5-point Likert-type scale (1—completely agree; 5—completely disagree).
Scale construction and content validity
To ensure content validity and adequately demarcate trust in the healthcare system and of medical workers, four independent evaluators indicated which items were most representative, based on the operational definitions in the Introduction. The sample comprised 36 items in total across categories that partly represented different aspects of trust: 24 items concerning women’s subjective perceptions of real and potential experiences in the healthcare system (e.g. “I trust that my doctor will tell me if he/she makes a mistake during the course of my treatment”); four items describing women’s experiences regarding receiving or hearing a diagnosis (e.g. “When a doctor tells me my diagnosis, I ask questions until I’m completely clear on what is going on with my body”); four items about privacy issues (e.g. “If a nurse loudly told me my diagnosis over the counter, I would feel ashamed”); and four items regarding women’s perceptions of medical workers’ behaviors (e.g. Doctors and medical staff ask if there is anything else I want to know regarding my health status). The initial pool of items presented to evaluators is found in Supplemental Appendix B, Table B1.
Each evaluator was asked to mark the items that resemble trust (1—resembles trust; 0—does not resemble trust) according to its definition. Only items for which at least two evaluators (50%) reached a consensus were analyzed. (Although some authors propose a higher degree of agreement for content validity assessments, we opted for a more liberal criterion of 50% consensus to ensure no potentially relevant facets of trust were omitted.) Based on the evaluation results, we constructed the WITCH scale comprising 20 items (Supplemental Appendix B, Table B2).
Statistical analyses
We first explored the factor structure of trust in the healthcare system using an exploratory factor analysis (EFA) in Sample 1. Second, we tested the factorial validity of the scale on Sample 2 using a confirmatory factor analysis (CFA). Third, we tested the invariance of trust in two periods (before and during the pandemic), using a multigroup CFA. Finally, we tested for concurrent validity using a multigroup structural equation modeling (SEM) analysis, with the trust dimensions as predictors and desirable health behavior as the outcome. All analyses were conducted using R statistical software 43 with the packages jmv 44 and lavaan. 45 Path models were reproduced using the SemPlot package. 46
Results
To test the factor structure of the WITCH scale, we conducted an EFA on Sample 1 (pre-pandemic data set, n = 329), using the principal axis extraction method with Promax rotation. According to Horn’s parallel criterion, four factors were extracted (scree plot, Figure 1). Factor intercorrelations (Table 1) indicated that the four dimensions are distinct but mutually related. Factor loadings (Table 2) revealed that the first factor (seven items, α = .81) captures interpersonal trust in medical professionals, defined as an expectation that healthcare workers will perform their responsibilities proficiently and responsibly making patients’ welfare their highest priority. 14 This factor mirrors what Schilke et al. 8 refer to as particularized trust, which we labeled as trust in healthcare professionals. The second dimension (five items, α = .68) represents what Schilke et al. 8 refer to as generalized trust; however, because it is reverse coded, we labeled it distrust in the public healthcare system. The third dimension assesses confidence (i.e. participants’ expectations that they will typically receive appropriate care and treatment; four items, α = .67). Finally, the fourth extracted dimension captures behavioral aspects of trust (i.e. adherence to physicians’ advice; two items α = .58). Therefore, we used it as an outcome of trust in further analyses. Two items (MG01_15 and MG01_09) did not have any factor loadings equal to or above .30 and were excluded from further analyses.

Scree plot.
Intercorrelations between the factors obtained using EFA.

p < .001, **p < .01.
Factor loadings of the Women’s Trust and Confidence in the Healthcare System scale.

The principal axis factoring extraction method was used in combination with Promax rotation. For clarity, loadings below .30 are not shown. F1: trust in healthcare professionals; F2: distrust in the public healthcare system; F3: confidence; and F4: behavioral aspects of trust. Items MG01_03 and P101_04 should be re-coded prior to score calculation.
The first three factors represent different beliefs about the healthcare system and satisfy the criterion of having at least three items per factor. 47 In contrast, the fourth factor captures behaviors and includes only two items. Therefore, we decided to retain the three factors that represent trust in the healthcare system and workers: (1) trust in healthcare professionals, (2) distrust in the public healthcare system, and (3) confidence in the healthcare system. The fourth factor was used as a behavioral outcome of trust. The three-dimensional WITCH scale was found to be highly reliable (Cronbach’s alpha = .85).
Model validation: CFA of the WITCH scale
To validate the three-factor model of trust in the healthcare system, we conducted a CFA (maximum likelihood method) using the data collected during the first year of the COVID-19 pandemic (Sample 2, n = 333). A total of 16 items were included in the model and distributed across the dimensions as suggested by the EFA results: (1) trust in healthcare professionals—seven items, (2) distrust in the public healthcare system—five items, and (3) confidence—four items. The data fit the model well (χ2 (101) = 275.448, χ2/df = 2.727, CFI = .895, TLI = .875, RMSEA = .072, SRMR = .066), with all factors significantly loaded by the respective variables (Supplemental Appendix C, Table C1). However, modification indices suggested that three items should be rearranged across the factors (Supplemental Appendix C, Table C2). Moving item MG01_18 to Factor 1 (trust in healthcare professionals) and item MG01_19 to Factor 3 (confidence) resulted in a better fit (χ2 (101) = 241.925, χ2/df = 2.395, CFI = .915, TLI = .899, RMSEA = .065, SRMR = .060). The remaining modification index suggested that item P101_04 (due to the unavailability of medicines, equipment, and staff in our healthcare system, patients do not receive adequate care) should be moved to Factor 3. However, moving this item resulted in a negatively definite covariance matrix. Therefore, we did not make this change. Factor loadings and intercorrelations followed the pattern obtained in the EFA (Table 3 and Figure 2). The detailed factor loadings, variances, and covariances can be found in Supplemental Appendix C, Table C3. The CFA results confirm the three-factor structure of the WITCH scale (Table 3). The internal consistency of the complete scale was almost the same as that in the pre-pandemic data set (Cronbach’s alpha = .86).
Correlations between the three dimensions of the WITCH scale (Sample 2).
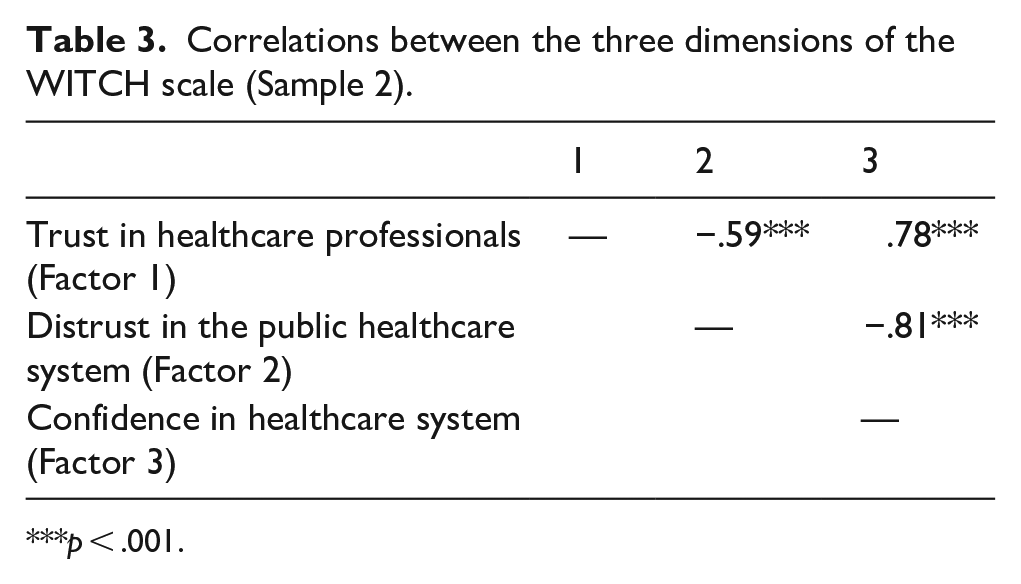
p < .001.
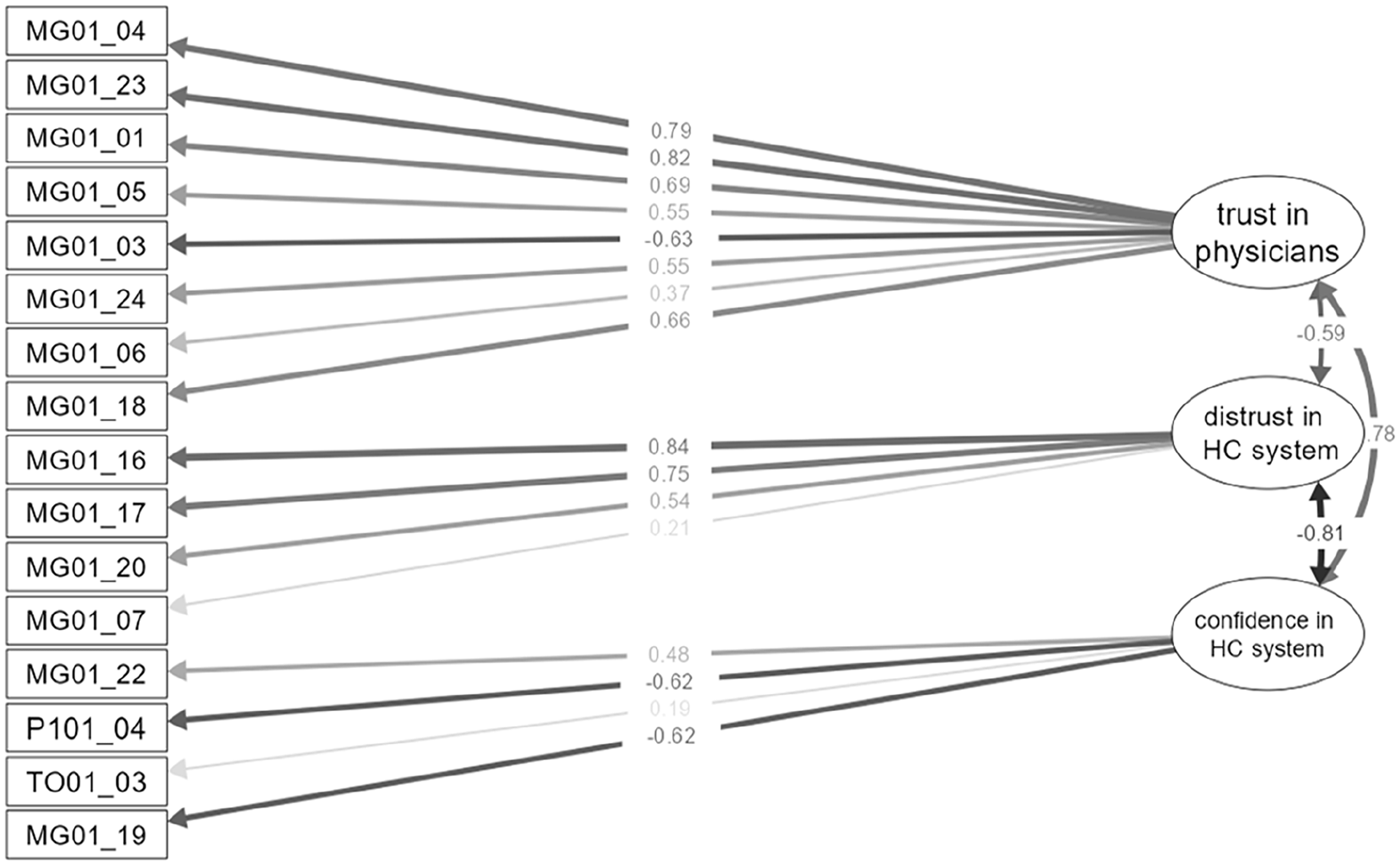
CFA model of the Women’s Trust and Confidence in the Healthcare System scale.
Concurrent validity of the WITCH scale: predicting behavioral outcomes of trust
To test the concurrent validity of the WITCH scale, we used SEM analyses with three interrelated dimensions of trust as latent predictors and the desirable health behaviors (Factor 4 obtained in the EFA: taking the prescribed therapy and following the physicians’ advice regarding preventive measures) as a latent criterion (to ensure the stability of the results, we re-ran the analysis using the mean of these two items as a manifest criterion. The values and directions of the coefficients did not substantively differ between the two models (see Supplemental Appendix C, Table C6 for details)). To conduct the analysis, we merged the data from two samples (N = 662), and the model showed a good fit (χ2 (129) = 370.449, χ2/df = 2.872, CFI = .928, TLI = .915, RMSEA = .053, SRMR = .046). The three trust dimensions explained 36% of the variance in trust-related behaviors (R2 = .364). The first trust dimension (particularized trust) positively predicted desirable health-related behaviors. Notably, the second dimension capturing distrust in the healthcare system also positively predicted desirable behaviors, indicating that individuals who do not trust the system are more likely to adhere to prescribed treatments and preventive measures. Although seemingly paradoxical, this finding suggests that distrust in a paternalistic healthcare system is related to agency regarding one’s own health. The third dimension did not significantly contribute to the prediction of desirable health-related behaviors (Table 4 and Figure 3). The detailed SEM analysis results are presented in Supplemental Appendix C, Table C4.
Regression coefficients for the dimensions of the WITCH scale predicting desirable health-related behaviors.
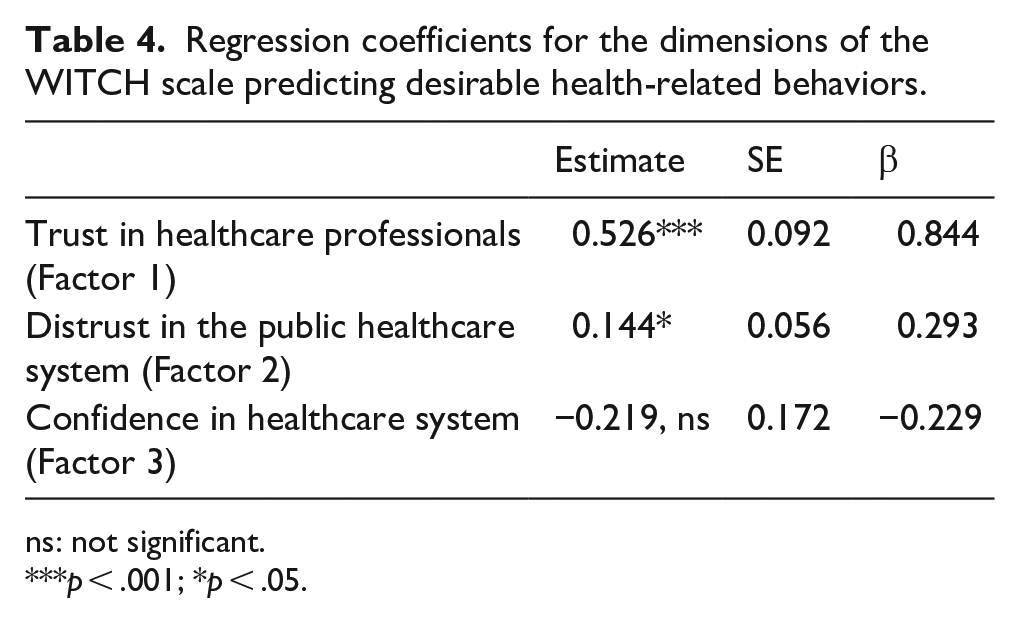
ns: not significant.
p < .001; *p < .05.

Dimensions of the WITCH scale predicting adherence to desirable health behaviors.
Testing the invariance of the WITCH scale
To compare the structure of women’s trust in the healthcare system before and during the COVID-19 pandemic, we used a multigroup CFA. The results indicated that the model had residual (strict) invariance across the two groups (Δχ2 = 155.56, Δdf = 143, p = .223); thus, the structure of trust in the healthcare system did not change due to the COVID-19 pandemic. The detailed measurement invariance testing results are found in Supplemental Appendix C, Table C5.
We further analyzed the structural differences before and during the pandemic regarding predictors of desirable health-related behaviors between the two groups. We observed residual invariance, in that the model was the same for both groups (Δχ2 = 202.72, Δdf = 175, p = .074; fit indices are detailed in Supplemental Appendix C, Table C6). However, the behavioral predictors were found to differ. Before the pandemic, both interpersonal trust in medical professionals and distrust in the public healthcare system predicted behavior, whereas only trust in medical professionals was a significant predictor of behavior during the pandemic (Table 5).
Prediction of desirable health behaviors using the dimensions of the WITCH scale before and during the COVID-19 pandemic.
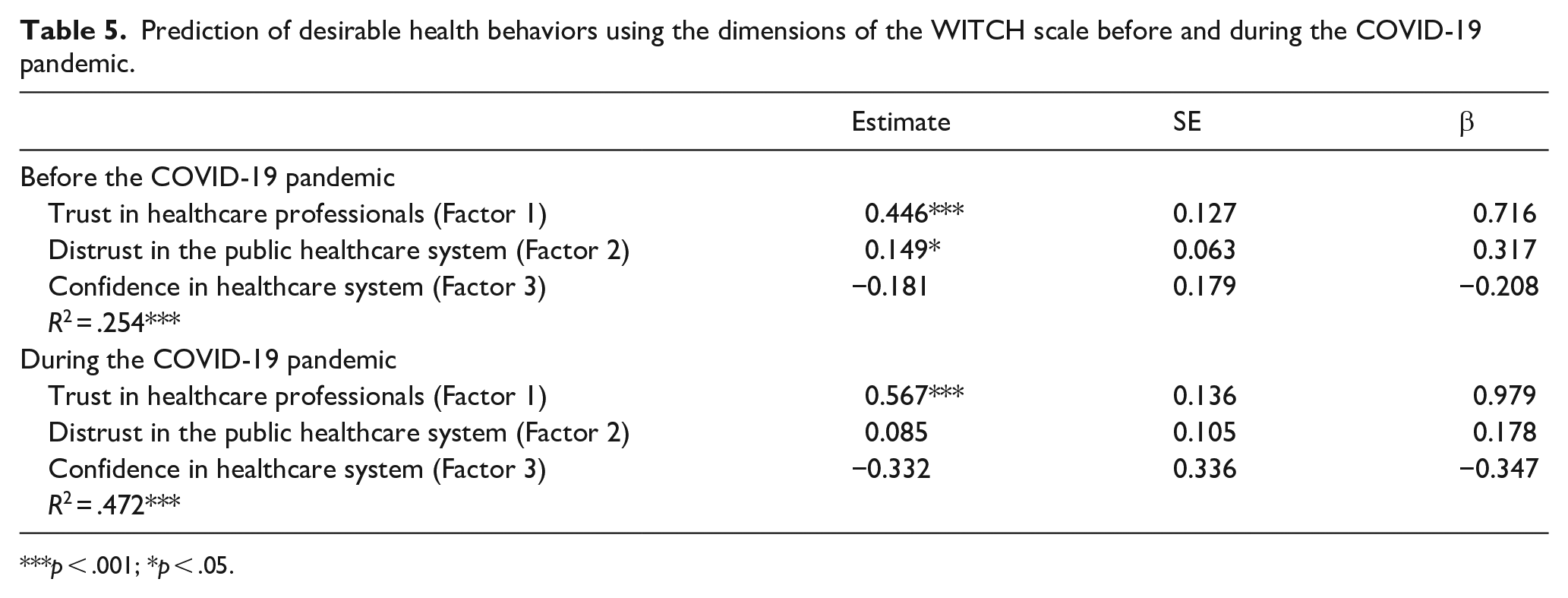
p < .001; *p < .05.
Discussion
This study aimed to construct and examine a scale to measure women’s trust and confidence in the healthcare system in the context of the de facto paternalistic model of doctor–patient relationships in Serbia. We first used the WITCH scale to explore the factorial structure of trust and confidence and then further validated the structure using another sample.
Using a bottom-up approach, we first selected the items from the initial pool that represent trust in the healthcare system. Then, four independent experts assessed the items’ content validity against the operational definition of women’s trust in the healthcare system. This comprises beliefs in good intentions and common goals of healthcare agents (regardless of whether they are people or systems), which results in the adjustment of women’s power, control, and behavior preceded by trust. Those items were used to construct the scale, the factor structure of which was then explored. The three-dimensional structure of the WITCH scale was confirmed across two independent samples of women. The scale showed high reliability in both samples, with Cronbach’s alphas of .85 and .86. Finally, we provided support for the scale’s concurrent validity using self-reported desirable health behaviors as outcomes of trust.
Dimensions of women’s trust in the healthcare system
The EFA results suggest that women’s trust in the healthcare system encompasses three distinct and interrelated dimensions: (1) trust in medical professionals, (2) distrust in the public healthcare system (reverse coded), and (3) confidence (i.e. women’s expectations that they will receive appropriate care and treatment). The first two factors mirror Schilke et al.’s 8 concepts of particularized and generalized trust, respectively. Specifically, trust in medical professionals (particularized trust) pertains to a particular situation, relationship, or person, which in this study are healthcare providers and includes the expectation that they will perform their responsibilities proficiently and responsibly, making women’s welfare their highest priority. 14 The second dimension, distrusts in the public healthcare system, mirrors Schilke et al.’s 8 generalized trust, which pertains to trust toward a relatively large circle of unfamiliar others (i.e. the healthcare system). Finally, we observed a distinction between trust and confidence, as confidence that the system is functional, evidence-based, and impersonal emerged as a distinct (third) factor, which is a pattern noted in previous literature on trust in the context of social work. 10 Furthermore, the three dimensions of the WITCH scale were interrelated with absolute values of Pearson’s correlations ranging from .50 to .81, indicating that the scale measures a single construct consisting of the three interrelated dimensions.
Finally, our results suggest that the structure of women’s trust in the healthcare system remains stable over time. We conducted a CFA on data collected from women who participated in the study during the first year of the COVID-19 pandemic. All observed parameters mirrored the pattern identified in the EFA, confirming the scale’s three-factor structure. Thus, the factorial structure of trust measured using the WITCH scale was not only stable over time but also remained constant despite the large-scale healthcare crisis that emerged during the pandemic.
Trust, but also distrust, predicts desirable health behavior
We tested the concurrent validity of the WITCH scale using SEM analysis with the trust dimensions as predictors and desirable health behaviors (adherence to physicians’ advice) as a latent criterion. The rationale behind this decision was that individuals who trust the healthcare system and workers are more likely to adhere to their physician’s advice.3,11,12
Supporting our previous findings, trust in healthcare professionals positively predicted desirable health-related behaviors. Notably, distrust in the public healthcare system (Factor 2) also predicted higher rates of desirable health behaviors. This indicates that patients who do not trust a paternalistic healthcare system still very much trust their doctors and are even more prone to adhere to advice from their medical professionals. Although this finding appears paradoxical, it reflects the complex interplay between trust and behavior in a transitioning healthcare system that is officially deliberative (Ethical Codex of Medical Chamber of Serbia, Article 51, states that “Doctor–patient relations must be based on mutual trust and responsibility, so that the patient actively participates in her treatment. Doctor must advocate for the respect of patient’s rights. Patient has the right to full loyalty of the doctor and all possibilities of his/her knowledge and skills.”) but remains paternalistic in practice. 31 In short, different aspects of trust divergently influence health-related behavior. Finally, we observed that this pattern was present only before the COVID-19 pandemic, whereas only trust in healthcare professionals predicted women’s health behavior during the pandemic. This finding suggests that, owing to the major health crisis of the pandemic, interpersonal trust emerged as the only trust-related antecedent of health behavior. Our results also indirectly imply what has already been proposed in previous research on trust: that trust in medical professionals is primarily based on the relationship between the trustor and trustee and is not significantly influenced by changes in social and institutional frameworks. 13
Limitations and future directions
In this study, we developed a scale to measure women’s trust and confidence in the healthcare system and tested its factorial and concurrent validity. We focused particularly on the context of Southeastern Europe where the transition from a paternalistic to a deliberative model of physician–patient relationships has been officially designated but not yet put into actual practice. Although we observed a replicable factorial and concurrent validity of the WITCH scale, evidence is still needed to validate its convergent and discriminative validity. Therefore, further validation of the WITCH scale should include at least one other well-established scale of trust in the healthcare system and/or providers; correlates of trust, such as self-reported health and well-being; and broader outcomes of trust, such as adherence to professional medical recommendations. The data in this study were collected using the snowballing method and Facebook advertisements, resulting in a non-representative sample with a high proportion of highly educated participants (Supplemental Appendix A, Table A1). Although we do not expect that educational level would affect the scale’s factor structure, further research should include a broader sample of women with lower education levels and self-reported socioeconomic status. This study was exploratory and the first of its kind in the region; therefore, the sample size was calculated based on the rule of thumb, which estimates the number of participants based on the number of items. In future studies, and based on the present findings, researchers should aim to use power analysis for more precise sample size calculations.
Furthermore, how women’s trust in the healthcare system fits perceptions of their own health and observed agency within the healthcare system is vital to examine. Finally, the link between trust in the healthcare system and power relationships between patients and healthcare providers should be addressed, as this is essential for the further development of interventions that aim to facilitate the transition toward a deliberative model in the Serbian healthcare system.
Pathways to progress
Along with identifying three distinctive aspects of women’s trust and confidence in the healthcare system, and the role of interpersonal and social trust in shaping women’s health-related behavior, our findings provide directions for practical psychosocial interventions aimed toward implementing the deliberative model for patient–physician relationships. First, women, who comprise half of all patients, must receive the same quality of care and be treated as equally capable interlocutors as men, which is not currently the case.1,33,34 Second, women’s agency should be strengthened, while healthcare providers should be trained to adopt the deliberative model of physician–patient relationships as the norm. Communication with healthcare providers shapes the normalization of women’s passive role, such as during childbirth, 48 and, therefore, cannot be the only pillar of transition toward the deliberative model. In a paternalistic context, feeling pain and assuming the right to not feel pain are stigmatized. Moreover, the need to know what is happening with one’s own body is perceived as unnecessary, thus reinforcing and reproducing the metaphorical “adult–child” relationship between healthcare professionals and female patients. 49 Therefore, this transition must go beyond communication and encompass comprehensive empowerment of both women (patients) and healthcare providers. Thus, education for both parties along with the redistribution of power appears to be the most promising method for shifting to an “adult–adult” relationship in the healthcare context, as suggested by Goodyear-Smith and Buetow. 50
Summary
We have constructed a reliable and valid scale to measure women’s trust and confidence in healthcare systems in the Serbian context. We believe that with further validation, the WITCH scale can be used in other countries where the healthcare system is transitioning from a paternalistic to a deliberative model, especially in places where the most common public healthcare systems are financed by compulsory health insurance contributions, but with the option to pay for private healthcare facilities out-of-pocket. As our scale’s factor structure suggests, trust in a context such as this comprises three interrelated dimensions: trust in healthcare professionals, trust in the public healthcare system, and confidence in the healthcare system. The second dimension relates to a publicly funded healthcare system, indicating that a woman’s expectations for publicly funded healthcare differ from those for private healthcare. Thus, this context-specific scale allows researchers to measure trust more subtly than can be done with other scales. The WITCH scale is also focused on women’s trust only, considering that the content and structure of trust in healthcare systems and professionals might be gender-dependent.
The importance of having reliable measures of trust valid for use in a particular societal context is essential for studying health behavior. Trust in the healthcare system shapes patients’ health-related behavior, serving as a basis for heuristic decisions. 9 Research consistently shows that trust in healthcare providers shapes interactions within healthcare systems,1,4–6 which aligns with our findings. However, the influence of trust on women’s involvement within the paternalistic model depends on the object of trust. If a woman trusts the paternalistic system, she will be obedient. If she trusts the physicians within the same system, she will be an agent in caring for her own health. These findings represent the complex psychological interplay of involvement and trust in paternalistic healthcare systems. Women display both trust and adherence; however, such adherence is passive. In these systems, trust can also have unfavorable repercussions by reinforcing the social norm of women’s passivity, thus providing ample space for abuse. Paternalistic behavior toward patients is, to some extent, facilitated by patients themselves who often conceptualize the dynamics in patient–physician relationships as similar to those in parent–child dyads, in which all power, as well as all the responsibility, rests with the parent (physician). 39 Mutual trust should be established to increase women’s involvement and sense of responsibility in managing their own health and redistribute power, resulting in better medical outcomes overall for all parties involved, as previous research has demonstrated.10,18,19,22
Misuse of women’s trust within the paternalistic model
The positive relationship between distrust in the system and desirable high involvement implies two novel notions regarding trust. First, trust in the system, or generalized trust, can be observed as secondary to interpersonal trust, meaning that when generalized trust deteriorates, as the findings show it did during the pandemic,51,52 interpersonal trust (i.e. trust in physicians) can remain a resource for increasing women’s agency in the medical context. However, both “physician” and “patient” are social roles, and the stability of the healthcare system should not be reduced to or lean on personal trust toward a particular physician. If social or generalized trust continues to deteriorate, a negative impact on interpersonal trust and a sense of alienation are more probable than strengthening patient–physician trust, which is a relationship that should be further explored.
Second, we considered this diversion of contributions of interpersonal trust and generalized distrust through the lens of the de facto paternalistic model in Serbia. Our results suggest that the more a woman trusts the healthcare system, the lower her adherence to her physician’s advice will be, which could lead to a suboptimal and unstable relationship with the medical system and healthcare providers, and consequently, worse healthcare for women. This might further generalize women’s agency regarding their health: paternalistic systems enforce women’s acceptance of a passive role; thus, their passivity during treatment will be reinforced. Some initial studies on the relationship between trust and normalization of the passive role of women during childbirth support this, 48 indicating that paternalism in the healthcare system is flourishing and is facilitated by all parties involved. (An illustrative example is an excerpt from a text on obstetrical violence by medical doctor Zlatko Bokun: “. . . Pregnant women are automatically even in court automatically considered to be in state of ‘diminished responsibility’ and they (pregnant women) are in every regard vulnerable population and many of the misunderstandings during the hospitalisation comes from communication with scared and hormonal women and tired nervous routine-oriented healthcare provider . . .”)
Conclusion
Our study’s findings provide insights into the structure of women’s trust in a paternalistic healthcare system and provide insight into how to approach the issue of the interplay between women’s trust and the healthcare system, considering that trust can be misused in these types of systems. As trust works both ways, it is a common good for women to trust physicians, as it is for physicians to respect and rely on women’s agency.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241249864 – Supplemental material for Women’s trust in the healthcare system in Serbia: Validation of the Women’s Trust and Confidence in Healthcare System scale
Supplemental material, sj-docx-1-whe-10.1177_17455057241249864 for Women’s trust in the healthcare system in Serbia: Validation of the Women’s Trust and Confidence in Healthcare System scale by Milica Ninković, Sandra Ilić and Kaja Damnjanović in Women’s Health
Research Data
sj-txt-3-whe-10.1177_17455057241249864 – Women’s trust in the healthcare system in Serbia: Validation of the Women’s Trust and Confidence in Healthcare System scale
sj-txt-3-whe-10.1177_17455057241249864 for Women’s trust in the healthcare system in Serbia: Validation of the Women’s Trust and Confidence in Healthcare System scale by Milica Ninković, Sandra Ilić and Kaja Damnjanović in Women’s Health
Research Data
sj-xlsx-2-whe-10.1177_17455057241249864 – Women’s trust in the healthcare system in Serbia: Validation of the Women’s Trust and Confidence in Healthcare System scale
sj-xlsx-2-whe-10.1177_17455057241249864 for Women’s trust in the healthcare system in Serbia: Validation of the Women’s Trust and Confidence in Healthcare System scale by Milica Ninković, Sandra Ilić and Kaja Damnjanović in Women’s Health
Footnotes
Acknowledgements
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.