
Abstract
FOXP1 syndrome is a neurodevelopmental disorder caused by mutations or deletions in the Forkhead Box Protein 1 (FOXP1) gene. It is characterized by intellectual disabilities, language difficulties, autism spectrum disorder, congenital anomalies and motor impairments.
Walking difficulties have been reported, but specific gait impairments have not previously been described. In this case series, specific gait abnormalities, and how they were managed, are reported in three children with FOXP1 syndrome. The most prominent clinical abnormalities in their gait and gait analysis were toe walking with increased plantar flexion, and knee and hip flexion in midstance. All children had premature activation of the calf muscles. In two of the three children, spasticity in the calf muscles and contractures of ankles and knees were found, which could explain these abnormalities in their gait.
Introduction
FOXP1 syndrome is a neurodevelopmental disorder caused by mutations in the Forkhead Box Protein 1 (FOXP1) gene. This gene encodes a transcription factor important for the early development of many organ systems, including the brain. Children with FOXP1 syndrome often have a combination of intellectual disabilities, language difficulties, autism spectrum disorder, congenital anomalies and motor impairments. 1 Hypertonia, spasticity and contractures of the lower limbs have been reported, as well as walking difficulties, but specific gait impairments have not previously been described in the literature. 2
It is important to better understand the gait abnormalities and underlying motor impairments in FOXP1 syndrome to be able to allocate the correct treatment to improve or preserve mobility.
Clinical gait analysis (CGA) provides a quantitative description of gait patterns by combining data from different sources, such as kinematic and kinetic data, and surface electromyography (sEMG).
Gait abnormalities found using CGA can be related to underlying impairments identified with physical examination, such as spasticity, muscle weakness, reduced selective motor control, muscle contractures and bony deformities.
Here, three children with FOXP1 syndrome who were referred because of walking problems are presented. The purpose of this study was to describe their gait abnormalities and the chosen treatments aimed at improving gait.
Case study
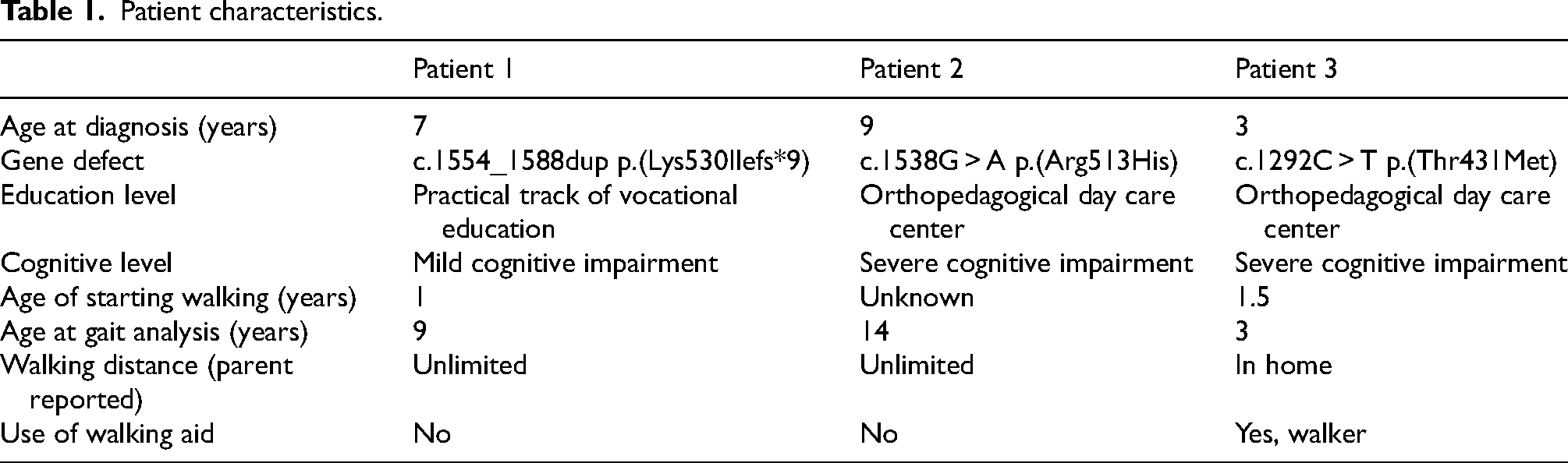
Three children with FOXP1 syndrome are presented. Patient characteristics are listed in Table 1. Table 2 gives an overview of the mean outcome values of joint range of motion (ROM), spasticity, foot deformity and functional strength in the three children. The cases are reported following the CAse REport (CARE) guidelines checklist. 3
Patient characteristics.
Overview of the mean outcome values of joint range of motion (ROM), spasticity, foot deformity, and strength.
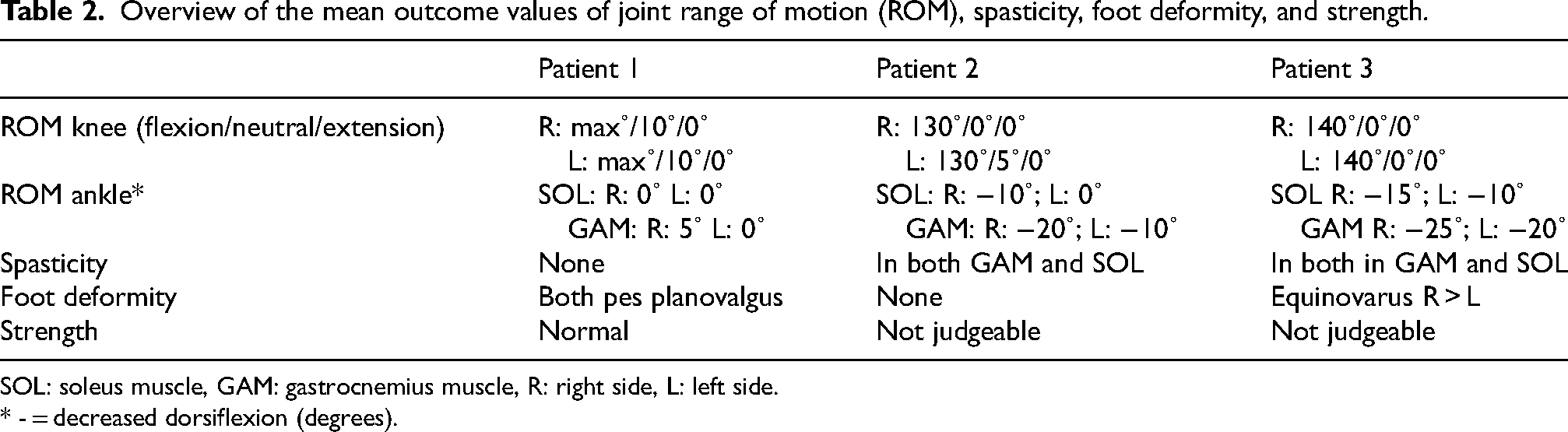
SOL: soleus muscle, GAM: gastrocnemius muscle, R: right side, L: left side.
* - = decreased dorsiflexion (degrees).
Patient 1 was a male, age nine years, with mild cognitive impairment, autism spectrum disorder, attention deficit/hyperactivity disorder (ADHD) and a phonological disorder. He started walking at the age of 12 months. With age, he developed gait deviations characterized by bilateral toe walking and increased knee flexion in stance phase. Physical examination revealed knee flexion contractures and reduced ankle ROM on both sides (see Table 2). His resting muscle tone was normal and no spasticity was found in the lower limbs. Clinical gait analysis showed that kinematics were comparable on both sides, demonstrating ankle plantar flexion and increased knee flexion in midstance.
To increase the ankle ROM and reduce toe walking, serial casting of the ankle was initiated. The casts were changed weekly with a total duration of two weeks. After this treatment, the soleus and gastrocnemius muscle length improved on both sides.
Following this, ankle-high shoes with stiff insoles were advised in order to force heel strike at initial contact by reducing foot drop during swing, and apply dynamic stretch to the calf muscles during the stance phase. The toe walking improved slightly, with better foot contact and improved knee extension during the stance phase, and better clearance in initial swing. With shoes, the position of the feet at initial contact improved.
Patient 2 was a male, age 14 years with autism spectrum disorder and a severe cognitive impairment. From the moment he started to walk, at two years and 11 months, he was bilateral toe walking with increased knee flexion during the stance phase. At presentation, he had an unlimited walking distance. Clinical examination revealed a reduced ankle ROM bilaterally with plantar flexion contracture with extended leg of 20 degrees on the right and 10 degrees on the left. This implied gastrocnemius muscle contractures on both sides. His resting muscle tone was high and spasticity was found in both legs in the soleus and gastrocnemius.
CGA showed forefoot contact and increased knee and hip flexion in midstance on both sides.
He was treated with botulinum toxin A injections in the soleus and gastrocnemius muscles of both legs, followed by serial casting and intensive physiotherapy. After this treatment, the soleus and gastrocnemius muscle length improved bilaterally. Toe walking decreased slightly, and prepositioning improved with improved knee extension at initial contact and better clearance. The patient was advised to continue stiff insoles in combination with ankle-high shoes in order to force heel strike and maintain the ROM of the ankles.
Patient 3 was a male, age three years, with severe cognitive impairment. He was a toe walker since he started walking at the age of 18 months and could walk only with a walking aid or two hands for support. Clinical examination revealed a plantar flexion contracture both with knee flexion (soleus) and knee extension (gastrocnemius) in the right and left ankles. (Table 2) He had an equinovarus foot, right more than left, and there was spasticity in gastrocnemius and soleus on both sides. Gait analysis showed forefoot contact with knee flexion in midstance on both sides.
To increase walking distance, reduce toe walking and increase the ROM, he was treated with botulinum toxin injections in gastrocnemius, soleus and tibialis posterior muscles followed by serial casting and intensive physiotherapy. In addition, he was prescribed ankle-foot orthoses to maintain calf muscle length and to correct varus foot deformity. After treatment, ROM of the ankle and toe walking were slightly improved, as were the walking speed and timing of activation of the calf muscles. Knee flexion during midstance remained the same. The maximal walking distance did not change.
Discussion
To the authors’ knowledge, this case series reports, for the first time, specific gait abnormalities in three children with FOXP1 syndrome. The most prominent clinical abnormalities in their gait and the gait analysis were toe walking with increased plantar flexion, and knee and hip flexion in midstance. All had premature activation of the calf muscles. In two of the three children, spasticity in the calf muscles and contractures of ankles and knees were found which could explain these abnormalities in their gait. In the literature, one previous study described a case with FOXP1 syndrome and toe walking, but no previous studies have described underlying impairments. 4
The children in this report had different treatments in order to reduce toe walking and improve ankle ROM. Treatment goals were set using shared decision making with the parents. All children benefitted from the treatment, even if sometimes only slightly. Spasticity treatment in FOXP1 patients can consist of botulinum toxin A injections, and improvement of ankle ROM can be achieved with serial casting. When choosing the appropriate treatment strategy for these patients, it is important to take their cognitive functioning into account, to predict if they can handle casting treatment and benefit from physiotherapy.
Compared with the walking pattern of idiopathic toe walking patients, FOXP1 patients have more knee and hip flexion in midstance. 5 Also, spasticity of the calf muscles is abnormal for idiopathic toe walking patients.
In patients with cerebral palsy, specific gait patterns have been described in order to guide clinicians in developing appropriate treatment strategies to optimize functional outcomes. 6 Gait classification could also be useful in FOXP1 patients in order to recognize abnormal gait patterns earlier. Early recognition could potentially lead to earlier treatment, thereby preventing secondary problems such as knee flexion contractures. Such a classification system could also help clinicians and researchers to improve treatments. Although there are no specific registries for children with FOXP1 syndrome, by adding walking indicators to global registries for rare diseases, treatments can be improved over time. Therefore, more research is needed with larger numbers of children to be able to cluster specific gait abnormalities and standardize the appropriate treatment in FOXP1 patients.
Footnotes
Acknowledgements
The authors would like to thank the children and their parents for their contribution.
Ethical considerations
This study is approved by the Medical Research Ethics Committee of Amsterdam University Medical Center (nr 2022.0261).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.