
Abstract
Purpose
Rocking in a rocking chair may facilitate trunk muscle activation in children with spinal cord injury (SCI). To assess this, children with SCI and typically developing (TD) children were evaluated for increases in trunk muscle activation, muscle activation patterns, and correlation of trunk muscle activation with trunk control during rocking.
Methods
Eleven children with SCI and 10 TD children aged 1–12 years rocked while surface electromyography activity in arm, leg, and trunk muscles was captured. Mean muscle activity during rocking and at baseline were compared for each muscle. Temporal activation patterns of SCI and TD groups were compared using cluster analysis. Correlation of trunk control and trunk muscle activation was assessed.
Results
Significantly higher muscle activity was found during rocking versus quiet sitting for each muscle (p < 0.05). Cluster analysis of temporal muscle activation patterns revealed two disparate SCI groups; one SCI group's muscle activation timing was similar to the TD group. Correlation analysis indicated greater trunk muscle activation in lower trunk muscles for participants with better trunk control.
Conclusion
Rocking activates the neuromuscular system and is feasible for children with trunk impairment due to SCI, suggesting its potential as a home-based activity for extending practice beyond the clinic.
Introduction
Pediatric spinal cord injury (SCI)
SCI is a debilitating condition that significantly impacts quality of life. Children with SCI in particular face numerous physical, emotional, and psychological challenges that often impede their overall development and well-being. 1 SCI is known to cause long term complications including negative effects on respiration, bladder and bowel control, cardiovascular function, and head/trunk control. 2 Moreover, SCI in children is more likely to result in secondary conditions, such as scoliosis, respiratory complications, hip dysplasia, and pressure ulcers,2,3 and the incidence of these conditions is greater for children injured at younger ages.3–6
Activity-based therapy (ABT)
With currently available treatments unable to correct for paralysis associated with SCI, traditional rehabilitation approaches focus on compensating for paralysis through use of assistive devices, behavioral strategies, and environmental adaptations to support mobility, function, and activities of daily living. 7 However, researchers have recently demonstrated that ABT is an effective intervention for at least partial restoration of intrinsic trunk control, as measured by the Segmental Assessment of Trunk Control (SATCo), in children with SCI. 8 The purpose of ABT is to activate the neuromuscular system below the level of injury, and to promote the restoration of neuromuscular capacity. ABT interventions include treadmill training with partial body weight support, which aims to mimic typical standing/walking patterns and reinforce appropriate trunk, pelvis, and lower extremity alignment, providing locomotor-specific sensorimotor input to the neural axis.9,10 Off-treadmill interventions encourage activation of trunk muscles through task-specific motor activities such as reaching, standing, and sit-to-stand. 8
ABT also focuses on home and community integration by giving children opportunities to utilize their new abilities and practice in a variety of everyday and functional activities. 11 From that perspective, rocking in a rocking chair was explored in a case report by Argetsinger et al. 12 This report described the trial of a pediatric rocking chair adapted for use by a child with SCI as an activity intended to support gains in trunk postural control outside of the clinic. Rocking in this chair created a self-initiated activity that promoted an upright posture and engaged trunk and arm muscles with little to no assistance from caregivers. A critical next step to inform clinical decision-making is to validate the effectiveness of using this approach to apply the gains acquired through locomotor training.
To better understand the effectiveness of rocking in the context of pediatric SCI, this study aimed to answer the following research questions: 1) Does rocking in a rocking chair activate trunk muscles in children with SCI and in typically developing (TD) children? 2) What are typical temporal muscle activation patterns during a rocking cycle in children with SCI, and how do these patterns differ from those seen in TD children? 3) Is there a correlation between intrinsic trunk control, as measured by SATCo, and trunk muscle activation during rocking?
In addition to these specific technical questions, it is important to investigate practical factors that impact the rocking experience, including the child's enjoyment of rocking, and the safety and functionality of the rocking chair prototype.
Materials and methods
Rocking chair design and fabrication
A thorough examination of the concept, design methodology, fabrication, and safety testing of the rocking chair have been described previously. 13 Briefly, to develop new technology for accomplishing the goals of this study, a custom rocking chair specifically designed for children with SCI (Figure 1) was fabricated. The chair was based on a glider style rocking chair to ensure stability and safety, and the base was assembled using Baltic birch plywood, a well-known furniture material which provided durability, cost-effectiveness, and ease of assembly. Seats from commercially available pediatric rocking chairs of two different sizes were adapted to attach interchangeably to the custom base to accommodate children of varying sizes. An adjustable height footrest was also included in the design of the rocking chair base to accommodate taller children.
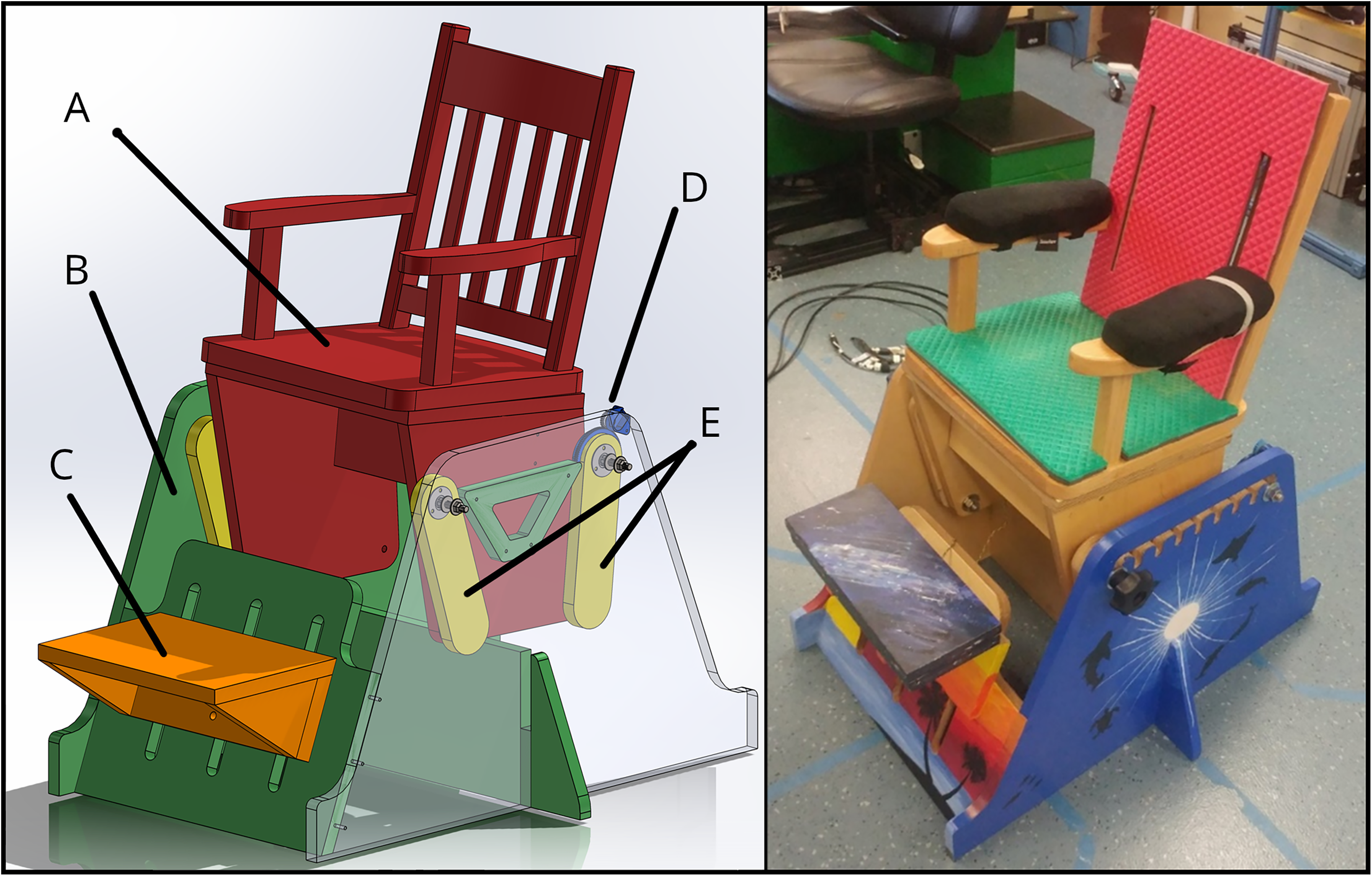
Left: A – Seat assembly; B – Chair base assembly; C – Footrest; D – Position sensor; E – Suspension arms; Right: Fabricated rocking chair.
To quantify the amplitude of rocking and to enable tracking of the temporal location of muscle activation in the rocking cycle, a custom chair position sensor was incorporated into the design. This included a shafted potentiometer configured so that the rotational position of the shaft was adjusted by the angular movement of one of the chair suspension arms as the seat assembly moved back and forth during rocking. This sensor generated a dynamic voltage which corresponded to the position of the seat as it was moved through the rocking cycle by the user.
Participant recruitment
The current study was performed under an Institutional Review Board approved protocol for parental/caregiver informed consent and assent for children older than seven years. Two cohorts were enrolled: children with SCI and TD children, based on specific eligibility criteria. Children with SCI were eligible if they were between the ages of 1–12 years and were either currently participating in locomotor training or recently discharged within the last month. Children discharged between one and 24 months prior were required to undergo a medical screening to determine health status and safety concerns before being deemed eligible. TD children between the ages of 1–12 years were eligible if they had no history of SCI or neurological disorder, musculoskeletal disease, or cardiovascular, pulmonary, or respiratory condition that would affect typical function; For both cohorts, children needed the ability to follow age-appropriate instructions, and those with a physical condition or recent illness that would prevent participation in rocking (identified via medical screen) were excluded.
Participant characteristics
A total of 11 children with SCI and 10 TD children were enrolled over a 22-month period. Age and height at time of testing and sex were recorded for all participants in both groups. American Spinal Injury Association (ASIA) Impairment Scale (AIS) 14 was recorded for participants in the SCI group whose age and etiology allowed it to be determined. Injury level, time since injury, etiology, and SATCo scores were also recorded for participants in the SCI group. SATCo score is an indication of a child's capacity to sit upright in both static and dynamic conditions with a facilitated neutral pelvis position and varying biomechanical levels of trunk support, and represents the patient's inherent, uncompensated level of trunk control. 8 Scores range from zero to 20, with higher values indicating better trunk control. SATCo was the primary measure of trunk control impairment and a primary descriptor of the population with SCI participating in this study.
Chair functionality assessment
To validate the basic operation of the chair, a TD child first evaluated the chair by sitting in it to test its balance, followed by rocking to assess both comfort and function. Once basic chair operation was verified, those with SCI were allowed to rock in the chair. Children were asked to rock in several different ways to evaluate which muscles they were capable of using to rock the chair: 1) Free rocking, allowing participants to rock in any manner of their choosing; 2) arms off armrests, to promote use of trunk muscles; 3) leg-only rocking, restricting trunk motion to assess the contribution of leg muscles to rocking; and 4) footrest removed, so that only upper body muscles contributed to rocking. Results from these modes of rocking were noted and compiled to better understand muscle use strategies.
During rocking sessions, children were observed closely while technicians engaged with them in conversation to understand their experience. Enjoyment of rocking, difficulties with making the chair rock, methods of initiating and maintaining rocking, and any potential safety or practical issues were observed and noted. Additionally, parents, children, engineers, and therapists engaged in debriefing conversations after each rocking session to obtain reactions and feedback, and to suggest possible improvements to the chair and protocols. Videos of rocking sessions were also reviewed to ensure that all data pertaining to chair use had been captured.
Surface electromyography (sEMG) data acquisition
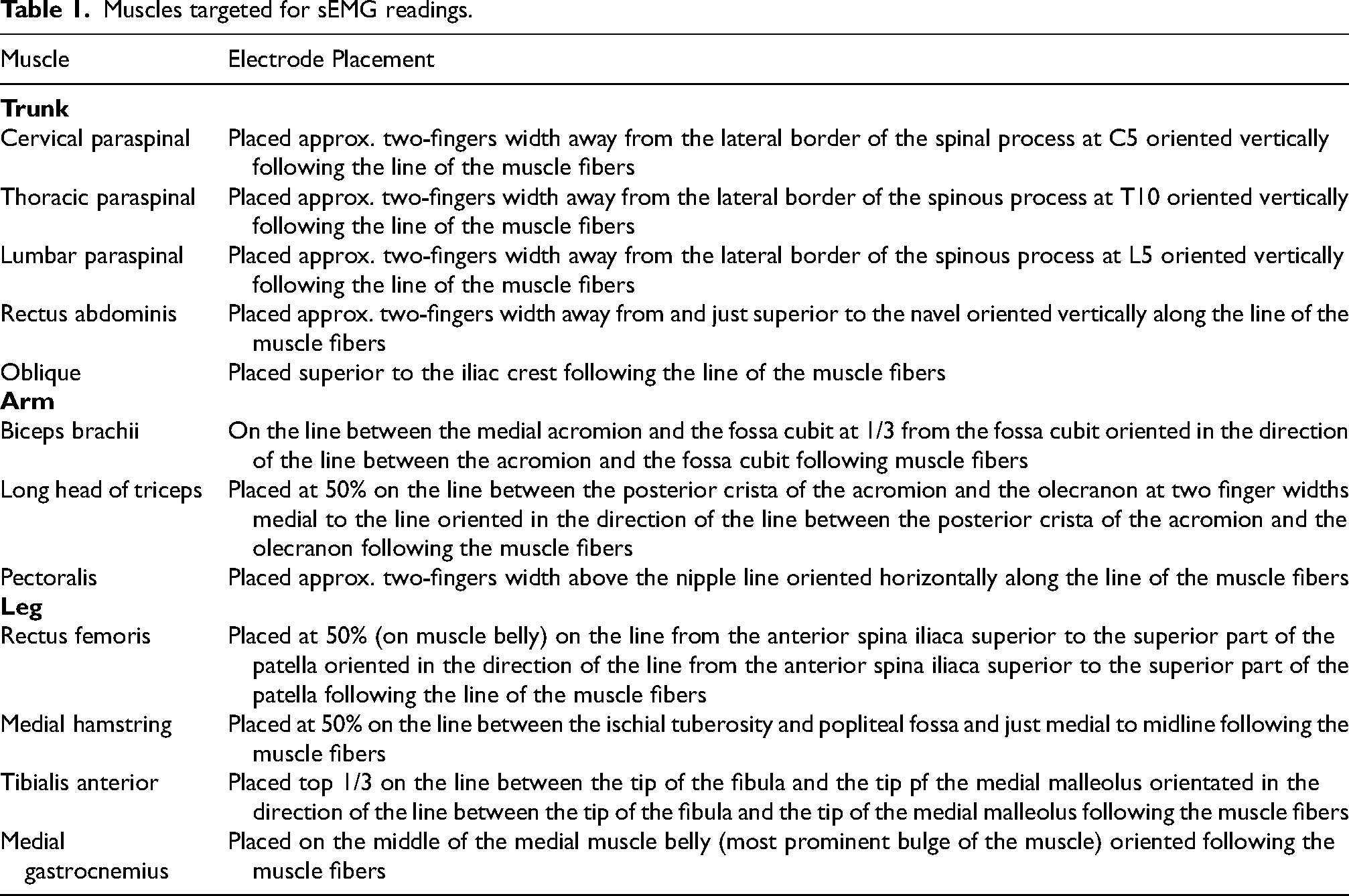
sEMG signals from muscles in the arms, legs, and trunk of both TD and SCI groups were recorded in microvolts (μV) at a 2000 Hz sampling rate and with a bandpass filter of 10—500 Hz. Wireless, pre-amplified, bipolar electrodes with 29 mm electrode spacing (Cometa Pico EMG, Cometa SRL, Milan, IT) were used. The skin over the muscle belly was prepared by cleaning with alcohol swabs, and self-adhesive 1.25” disposable electrodes were placed over each muscle while the child was seated on a stationary table. Electrode placement details are shown in Table 1. 15 Participants were then asked to sit in (TD) or were placed in (SCI) the chair (examples in Figure 2). A safety strap was placed around the waist, and additional straps placed higher on the trunk, if necessary, for support. Each child was instructed to sit quietly for one minute while sEMG was recorded to establish baseline muscle activation. All children were then instructed to rock in the chair using whatever methods were most natural to them. Once the child was accustomed to rocking and was observed to be rocking in a regular rhythm, sEMG was recorded for one minute. sEMG data was then imported into MATLAB where data offset was removed by subtracting the mean value of all data points from each data point and a 300-point moving window root mean square (RMS) was calculated for all datasets using custom MATLAB scripts. In addition, the sEMG and chair position sensor signals were synchronized using a pulse input to both data acquisition programs.

A participant with spinal cord injury using the custom rocking chair prototype. Note strap around chest for support, and footrest raised to support feet. Photo used with permission.
Muscles targeted for sEMG readings.
Rocking cycle
For this study, a single rocking cycle was defined as the position of the chair as it swung from the extreme front position to the extreme rear position and back to the front. Thus, the beginning and end of the cycle was defined as the point at which the chair reversed direction at the front of the cycle. As shown in Figure 3, the cycle was broken into two phases: Phase 1 was backward (BW) motion, starting with the chair all the way forward, and lasting while the chair swung backward to the farthest back point in the cycle. Phase 2 was forward (FW) motion, starting with the chair at the farthest back point, and lasting until the end of the cycle with the chair again at the farthest forward point. Each of these phases was divided into early (EBW, EFW) and late (LBW, LFW) stages. Accordingly, the chair rocking direction reversed from forward to backward at the end point of the cycle, and reversed from backward to forward at the midpoint of the cycle.
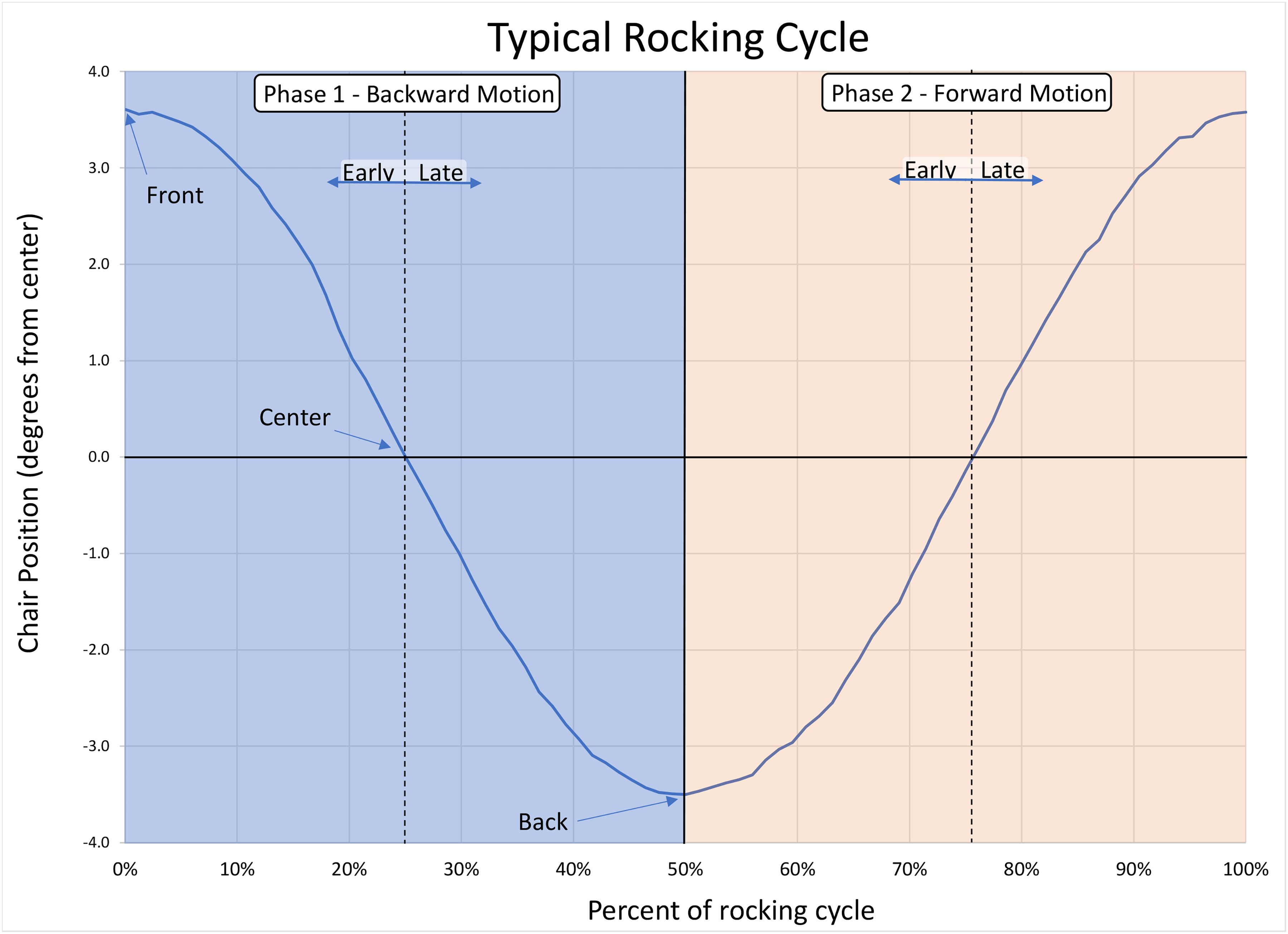
Sample position sensor data from one rocking cycle, to highlight cyclical phase of rocking; center vertical line marks change in direction; left quadrant is backward motion, right quadrant is forward motion.
Artifact removal in sEMG data
As is common with sEMG data, many of the trunk muscle data sets were contaminated with cardiac artifacts. To remove this interference, two methods were used. First, for analyses that looked at sEMG amplitude during rocking, it was possible to average the uncontaminated data between heartbeats to calculate the magnitude of the sEMG signal. To delete the contaminated data, a custom MATLAB script was used to identify the interfering signals and delete them from the dataset. Before running this script, each dataset was manually inspected to determine an appropriate threshold for detecting heartbeats. Typically, the cardiac signal was strongest in the left pectoral sEMG; therefore, this signal was used initially to locate the heartbeats, and the start and end points of each heartbeat were identified. The erroneous data was then deleted from all data streams and the mean of the remaining data was calculated for each muscle during rocking and during quiet sitting.
Second, for analyses of the timing of muscle activation during rocking, it was necessary to use a method of cardiac contamination removal that preserved the time-dependent nature of the data. Similar to the previous method, this involved identification and deletion of the contaminated data. However, to preserve the time-dependent nature of the data, a custom MATLAB script was used to replace the deleted data with the averaged data from the same point in the other rocking cycles.
In addition to the cardiac contamination, there were also two other, less prevalent sources of data contamination. First, to capture data from the desired muscles, some sEMG sensor bodies were required to be positioned in locations that brought them into contact with the seat during rocking, potentially introducing artifacts into the recorded data in the event of a collision. Second, extraneous movements on the part of the child, such as a hand gesture, could introduce a signal unrelated to the rocking cycle into the data. These were identified and removed manually by inspecting the sEMG data and cross-referencing with the corresponding video recording of the data collection session. Removed data was replaced with averaged data from other rocking cycles, similar to the procedure described above for cardiac artifact removal.
Muscle activation amplitude calculation
For each participant, the mean sEMG (RMS) amplitude during rocking was calculated for each muscle. Baseline amplitude was also calculated by taking the three second period with the lowest mean sEMG (RMS) amplitude during quiet sitting for each muscle. Normalized activation amplitude for each muscle was calculated by subtracting the baseline amplitude from the mean amplitude during rocking of the corresponding muscle.16–18 Normalized activations were then plotted in a heatmap.
Prototype cycle creation
To determine the timing of muscle activation within the rocking cycle, an average or “prototype” rocking cycle was created for each muscle. To do this, a custom MATLAB script was used to break the sEMG data from each participant into rocking cycles using the peaks in the position data from the position sensor mounted on the rocking chair to identify the beginning and end of each rocking cycle, as shown in Figure 3. These activation cycles for each muscle were time-normalized by linear interpolation to 1000 points per rocking cycle, and averaged for each participant.
19
The resulting average cycles were normalized to a scale of 0 to 1 using the formula:
Statistics
To address the first research question, “Does rocking in a rocking chair activate trunk muscles in children with SCI and in TD children?”, the mean sEMG (RMS) amplitude during rocking was calculated for each muscle activity recorded. Baseline amplitude was also calculated by taking the three second period with the lowest mean sEMG (RMS) amplitude during quiet sitting for each muscle. Data was tested for normality, and since data for many muscles failed these tests, one-sided signed-rank tests were selected to test the hypothesis that, for both SCI and TD groups, sEMG amplitude (RMS) for each muscle during rocking would be greater than baseline sEMG amplitude (RMS) for the same muscle during quiet sitting. To quantify the increase in muscle activation, a non-parametric effect size (ES) equivalent to Cohen's d was calculated using equation 2:
To address the second research question, “What are typical temporal muscle activation patterns during a rocking cycle in children with SCI, and how do these patterns differ from those seen in TD children?”, cluster analysis was used to investigate how the timing of muscle activation in the SCI group compared to those observed in the TD group, and to determine if different rocking styles contributed to different muscle activation patterns in trunk muscles. To achieve this, the rocking cycle was subdivided into four segments, as described previously and shown in Figure 3: EBW (first 25% of the cycle), LBW (26–50%), EFW (51–75%), and LFW (76–100%). Muscle activation for each child was normalized to a scale of 0 to 1 using Equation 1, and the mean normalized muscle activation within these segments was calculated for each participant and each trunk muscle. This data was aggregated and used to perform cluster analysis. Cluster analysis was performed in MATLAB, using the ‘linkage’ function with the ‘average’ distance method to find clusters of participants who used similar temporal muscle activation patterns while rocking. After clusters were identified, distance between each SCI participant and the TD cluster was calculated using the formula:
Two-sided t-tests were used to test for differences in activation in each segment between the TD group and each of the SCI clusters, and significant differences were noted on plots.
To examine the third research question, “Is there a correlation between intrinsic trunk control, as measured by SATCo, and trunk muscle activation during rocking?”, Spearman correlation analysis was performed to assess the correlation between SATCo scores and trunk muscle activation amplitude. For purposes of this analysis, two children with acute flaccid myelitis (AFM) were excluded as their impairment presentations were atypical, not uniform across spinal cord levels, and reflected greater to lesser impairment in a cephalad-caudal direction. In contrast, other participants demonstrated higher SATCo scores with greater control and activation of lower thoraco-lumbar muscles. Results were compiled in a table and significant correlations were noted.
All confidence levels were set at 95% (p < 0.05). Prism 10 (GraphPad Software, San Diego, CA, USA) was used for the analysis.
Results
Participant characteristics
Characteristics of participants are shown in Table 2. The SCI group included seven males and four females between three and 11 years of age (mean = 7.1, standard deviation [SD] = 2.7), and heights ranging from 77 to 142 cm (mean = 120, SD = 22). SATCo scores ranged from zero to 19 out of 20 (mean = 13.1, SD = 5.8). ASIA grade was A for five children and B for one child; five children were not assessed for ASIA grade due to age (< 5 yo) or diagnosis of AFM. All were non-ambulatory. Two children presented with cervical SCI, six with thoracic SCI, and one with lumbar SCI. Time since injury ranged from 1.5 to 6.5 years (mean = 4.1, SD = 1.7).
Participant characteristics.
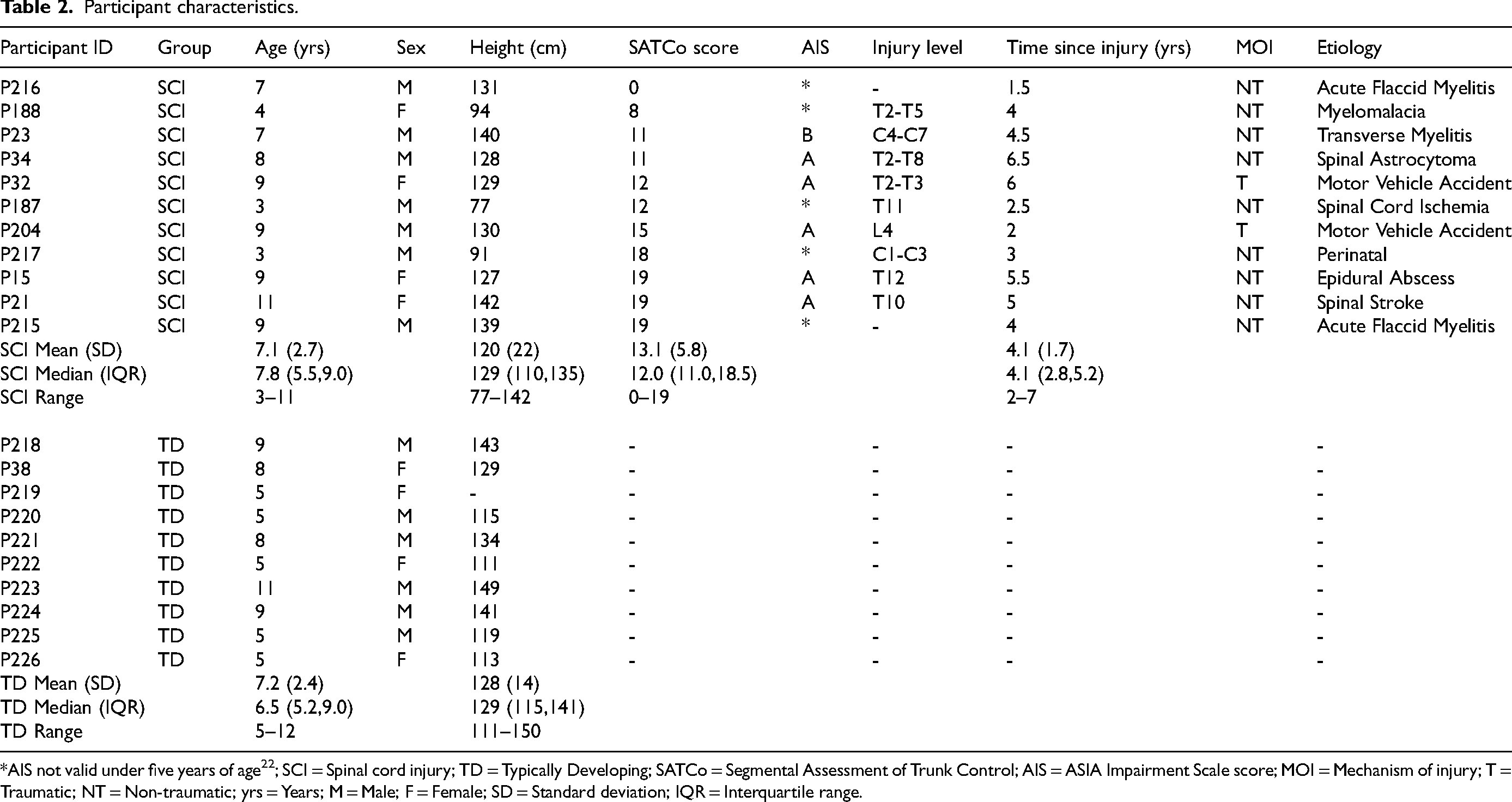
*AIS not valid under five years of age 22 ; SCI = Spinal cord injury; TD = Typically Developing; SATCo = Segmental Assessment of Trunk Control; AIS = ASIA Impairment Scale score; MOI = Mechanism of injury; T = Traumatic; NT = Non-traumatic; yrs = Years; M = Male; F = Female; SD = Standard deviation; IQR = Interquartile range.
The TD group included six males and four females with ages ranging from five to 11 years (mean = 7.2, SD = 2.4), and heights from 111 to 143 cm (mean = 128, SD = 14).
Safety, functionality, and enjoyment
Data from observation of rocking sessions are summarized in Table 3.
Participant experience while rocking.
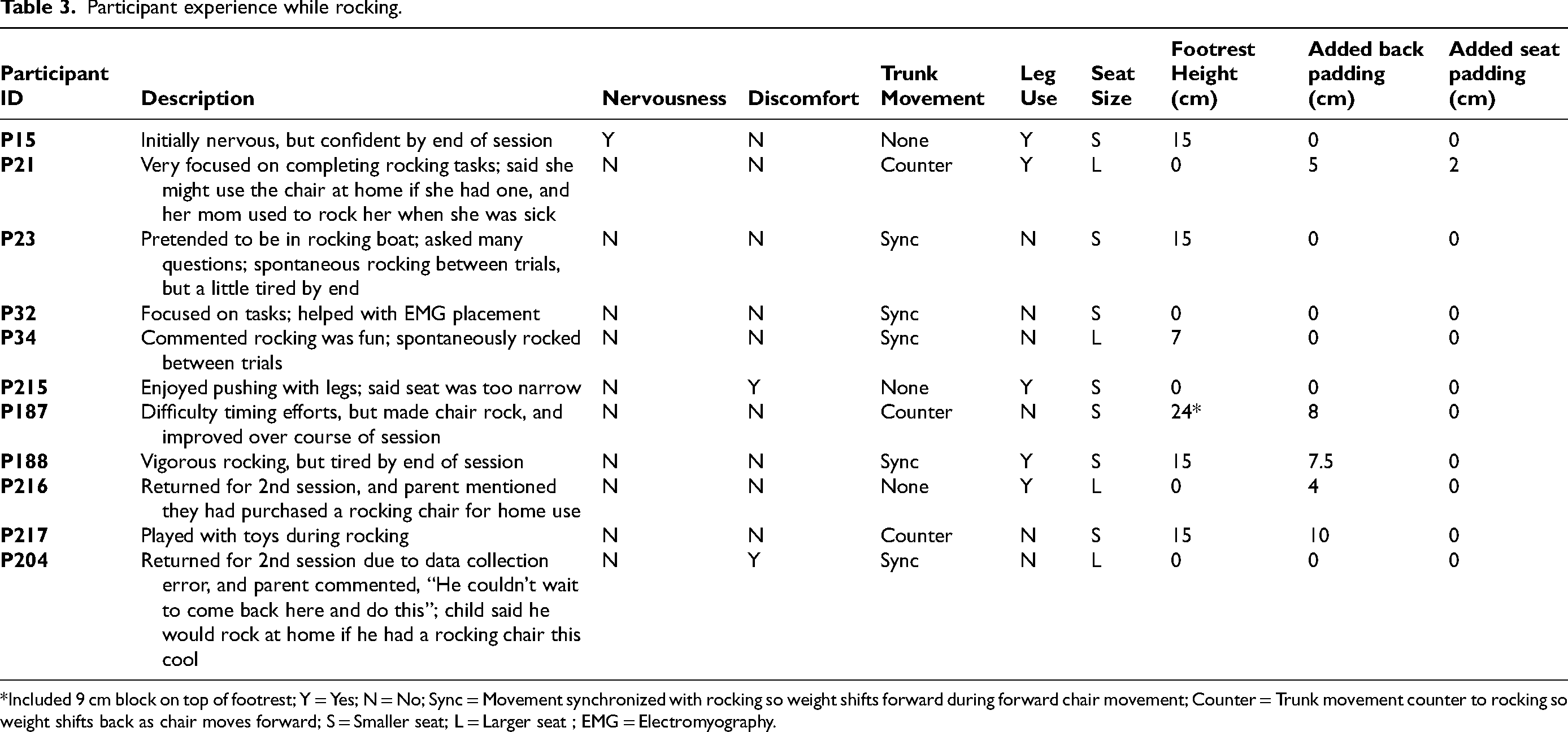
*Included 9 cm block on top of footrest; Y = Yes; N = No; Sync = Movement synchronized with rocking so weight shifts forward during forward chair movement; Counter = Trunk movement counter to rocking so weight shifts back as chair moves forward; S = Smaller seat; L = Larger seat ; EMG = Electromyography.
Safety: No adverse safety events or injuries were experienced during trials with children in the rocking chair. However, it was observed that a cross brace under the seat could create a potential pinch point for smaller children.
Functionality: Regardless of previous experience with rocking or degree of impairment, all children in both groups were successful at making the chair rock. The two youngest children (both three years old) had some difficulty timing their efforts but were able to make the chair rock. After some practice, their timing improved, but the amplitude of rocking remained well below the chair's full range of motion.
All children in both the SCI and TD groups were able to fit in the rocking chair. The interchangeable seats and adjustable footrest accommodated most children without alteration, but for those with shorter legs, it was necessary to insert padding between the child and the seat back and, in one case, to place foam blocks on the footrest to enable their feet to reach comfortably. This adjustment allowed them to engage in rocking but made it more challenging to position them correctly.
Debriefing discussions following rocking sessions provided suggestions for functional improvements to the rocking chair. These suggestions included a larger footrest with straps and a non-slip surface to keep feet in place, and a lock to prevent rocking during transfers or other activities.
Enjoyment: During conversation, several of the children specifically said they enjoyed rocking in the rocking chair, and two who had to return for a second session due to problems with data collection expressed their eagerness to return. Another indication of enjoyment was that many of the children rocked spontaneously while not specifically engaged in a rocking task, and in some cases, it was difficult to convince them to sit still.
There were no major negative reactions to the rocking chair. One of the children did initially express some apprehension that the chair would tip over but was reassured when the safety stops which limit chair tilt were demonstrated and quickly gained confidence as they rocked. Two rocked vigorously at first but expressed that they were feeling tired toward the end of the rocking session.
Observed trunk motion during rocking
The majority of children in the SCI group moved their trunk and/or head in time with the rocking cycle. Of these, five leaned their head and upper trunk, shifting their weight forward while the seat moved forward, and shifting their weight back while the chair moved back. In contrast, three children instead moved their trunk in a counterbalance rocking strategy, leaning forward from the waist as the seat of the chair moved back. This effectively kept the center of mass of the seat/child in approximately the same place but moved the seat back and forth. Finally, three children maintained a mostly stationary trunk.
Increase in muscle activation during rocking
Mean RMS muscle activation during rocking was significantly higher than during quiet sitting (p < 0.05) for all twelve muscles tested in both SCI and TD groups (see Tables 3 and 4, respectively). Muscle activation was measured by the increase from baseline of sEMG amplitude (μVRMS). Due to discomfort, cervical paraspinal sensors were not used on several participants in each group leading to a smaller n for this muscle, and a different confidence interval. Median increase and confidence interval are shown for all muscles.
Increase in muscle activation while rocking for children with SCI.
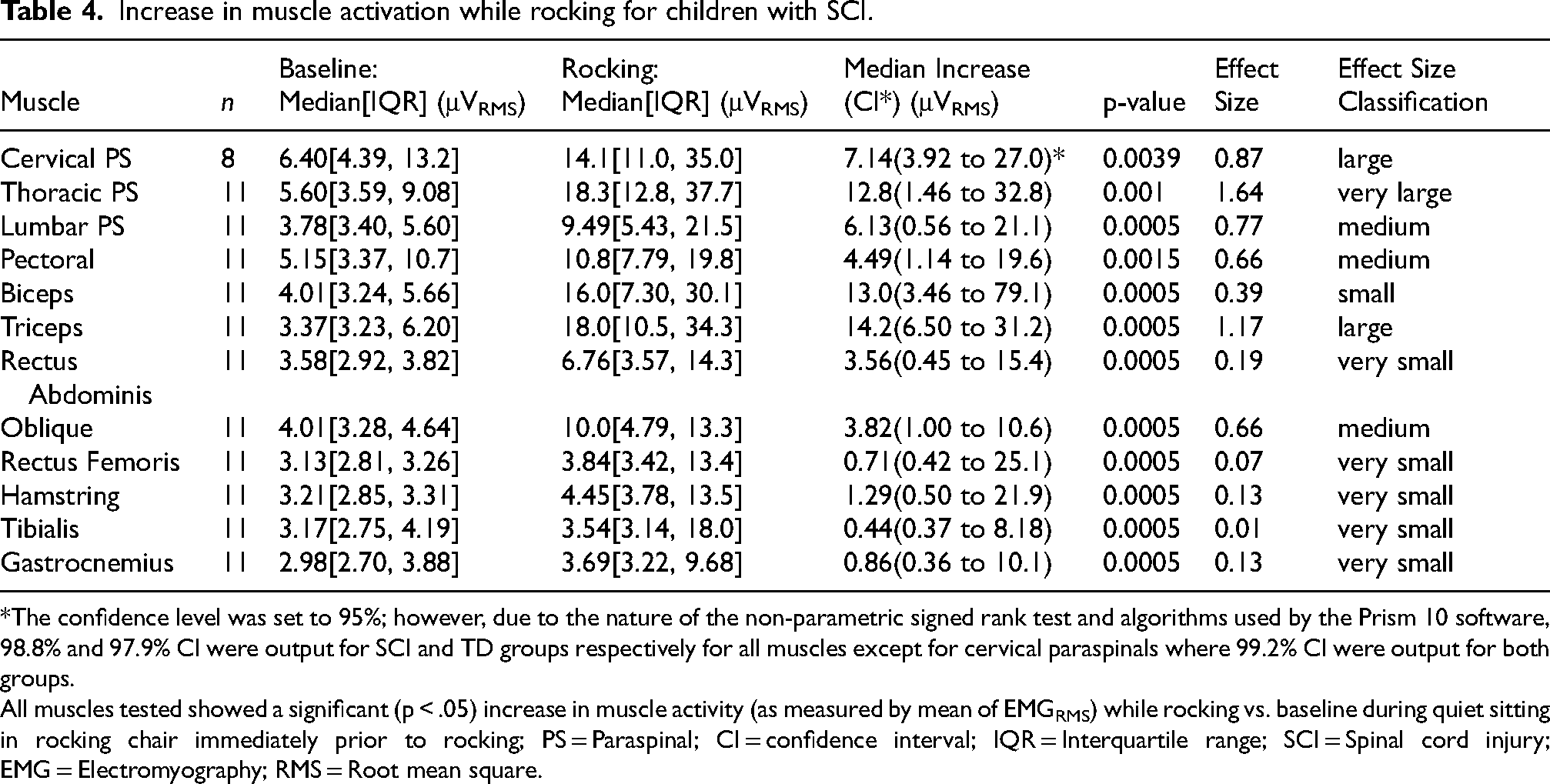
*The confidence level was set to 95%; however, due to the nature of the non-parametric signed rank test and algorithms used by the Prism 10 software, 98.8% and 97.9% CI were output for SCI and TD groups respectively for all muscles except for cervical paraspinals where 99.2% CI were output for both groups.
All muscles tested showed a significant (p < .05) increase in muscle activity (as measured by mean of EMGRMS) while rocking vs. baseline during quiet sitting in rocking chair immediately prior to rocking; PS = Paraspinal; CI = confidence interval; IQR = Interquartile range; SCI = Spinal cord injury; EMG = Electromyography; RMS = Root mean square.
ESs for muscle activation during rocking are reported in Tables 4 and 5 for SCI and TD groups, respectively. ESs for trunk muscles in the SCI group were all medium or larger with the exception of rectus abdominis which was very small. All ESs for leg muscles in the SCI group were very small. In the TD group, all were medium or larger with the exception of pectoral, rectus femoris, and gastrocnemius, which were small.
Increase in muscle activation while rocking for TD children.
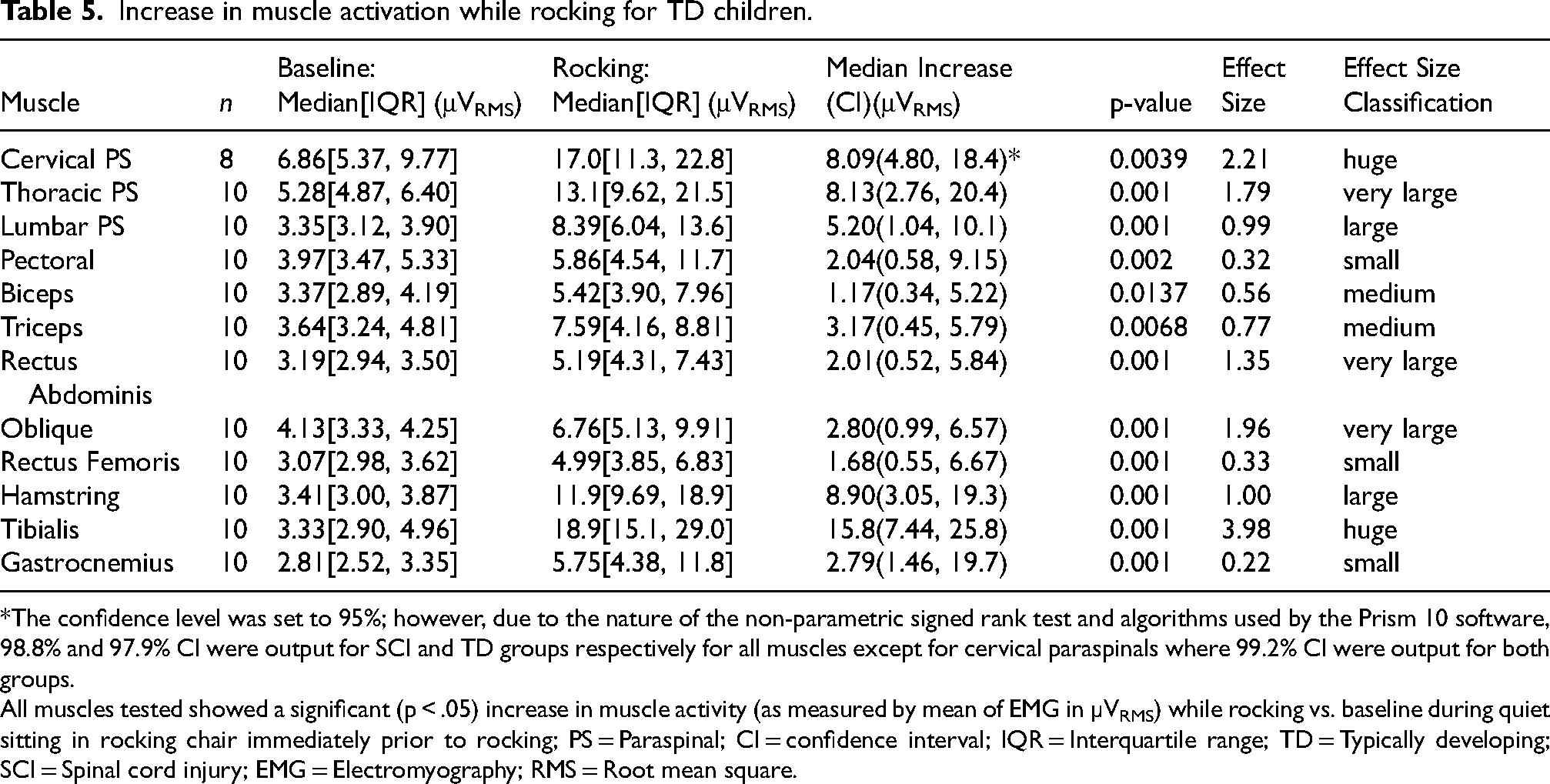
*The confidence level was set to 95%; however, due to the nature of the non-parametric signed rank test and algorithms used by the Prism 10 software, 98.8% and 97.9% CI were output for SCI and TD groups respectively for all muscles except for cervical paraspinals where 99.2% CI were output for both groups.
All muscles tested showed a significant (p < .05) increase in muscle activity (as measured by mean of EMG in µVRMS) while rocking vs. baseline during quiet sitting in rocking chair immediately prior to rocking; PS = Paraspinal; CI = confidence interval; IQR = Interquartile range; TD = Typically developing; SCI = Spinal cord injury; EMG = Electromyography; RMS = Root mean square.
Observed actions of muscles during rocking in children with SCI.
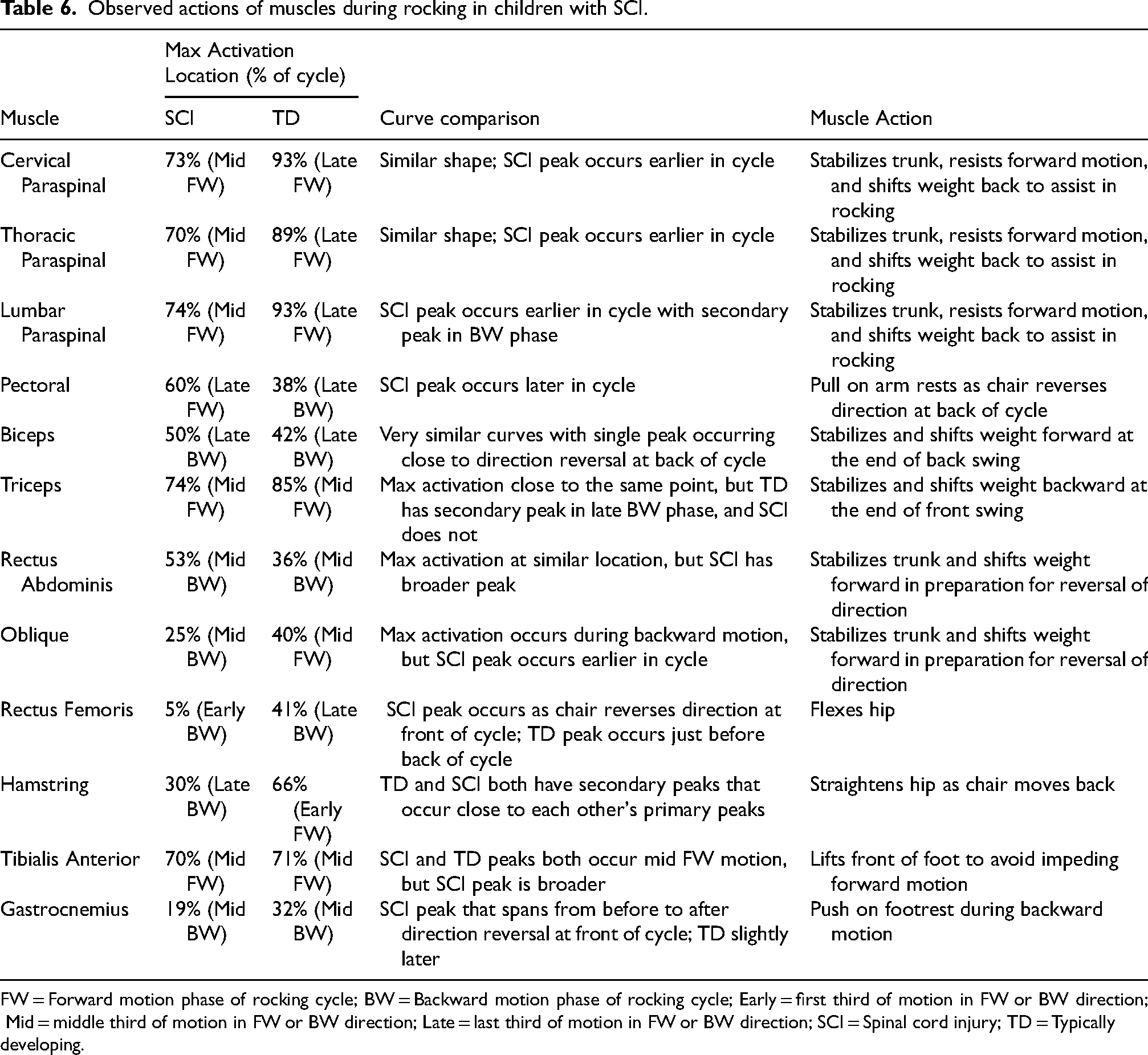
FW = Forward motion phase of rocking cycle; BW = Backward motion phase of rocking cycle; Early = first third of motion in FW or BW direction; Mid = middle third of motion in FW or BW direction; Late = last third of motion in FW or BW direction; SCI = Spinal cord injury; TD = Typically developing.
Temporal muscle activation patterns
Typical temporal muscle activation patterns during the rocking cycle for both SCI and TD groups are shown in Figure 4. General trends indicated that many of the muscles exhibited similar activation patterns between the groups but were often out of phase with each other. For instance, cervical and thoracic paraspinals showed very similar activation curves, but in the SCI group, the peak activation occurred earlier in the rocking cycle. Other muscles had maximum activations that occurred close to the same point in the rocking cycle but exhibited different shaped curves. For example, both the SCI and TD groups showed maximum activation of the rectus abdominis at the same point in the rocking cycle, but the SCI group had a much broader activation peak than the TD group. Table 6 describes the observed locations of peak muscle activation and the effects of muscle activation with respect to the rocking cycle in SCI and TD groups.
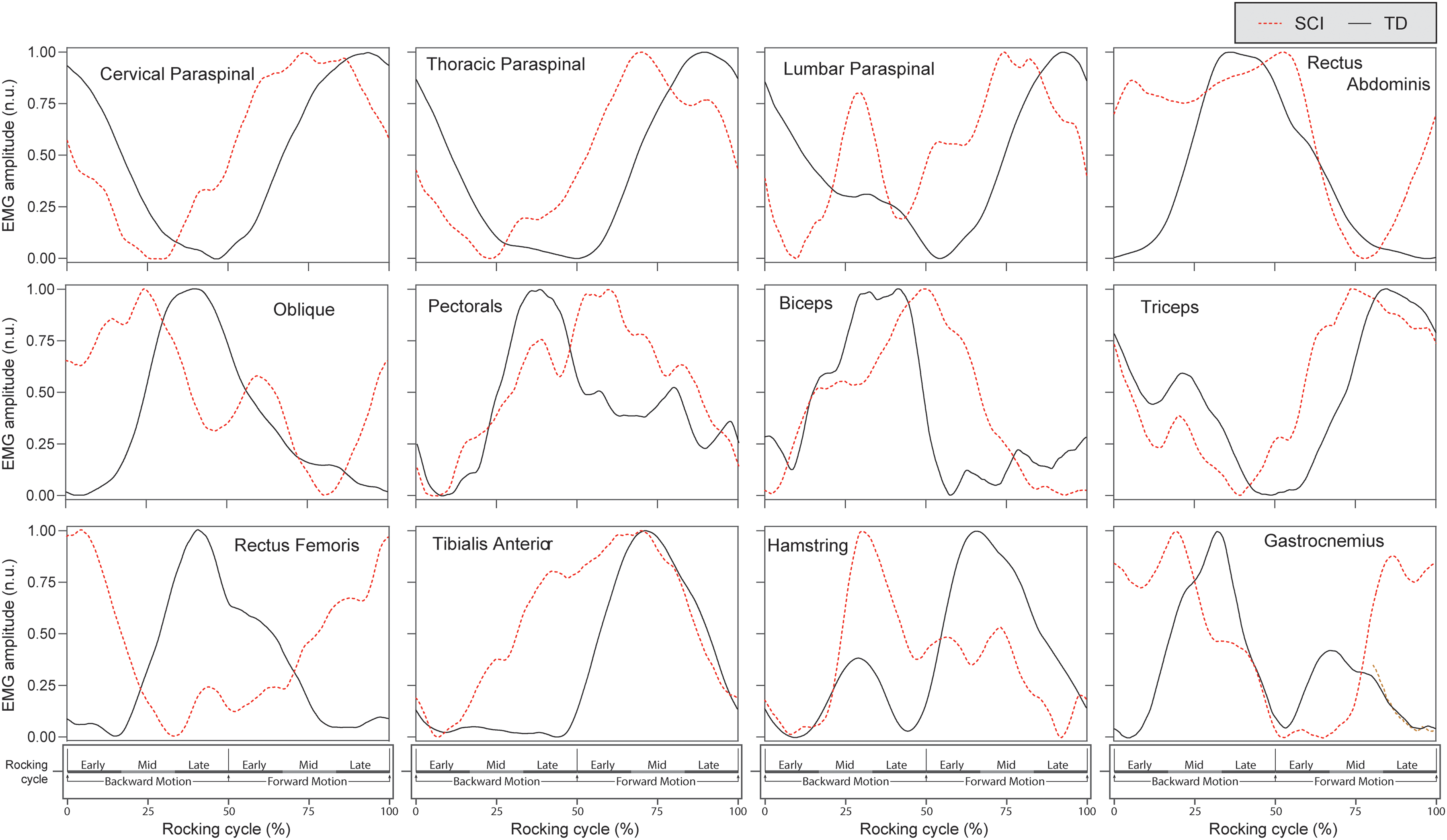
Averaged muscle activation during rocking in children; x-axis is one full rocking cycle; y-axis is normalized to the amplitude of EMGRMS in the rocking cycle; n.u. = Normalized units; EMG = Electromyography; RMS = Root mean square; SCI = Spinal cord injury; TD = Typically developing.
Cluster analysis based on the timing of muscle activation divided the SCI group into two clusters of seven and four participants as shown in the dendrogram in Figure 5. The average calculated distance from the seven- and four-participant clusters to the TD group was 0.78 and 1.16 respectively. Thus, the seven-participant cluster was labeled the “TD-similar cluster,” and the four-participant cluster was labeled the “TD-dissimilar cluster.” Plots of the clustering data for the trunk muscles are shown in Figure 6. This figure illustrates that, for most trunk muscles, the temporal activation patterns in the TD-similar cluster were closely comparable to those of the TD group, whereas the patterns of the TD-dissimilar group were not.
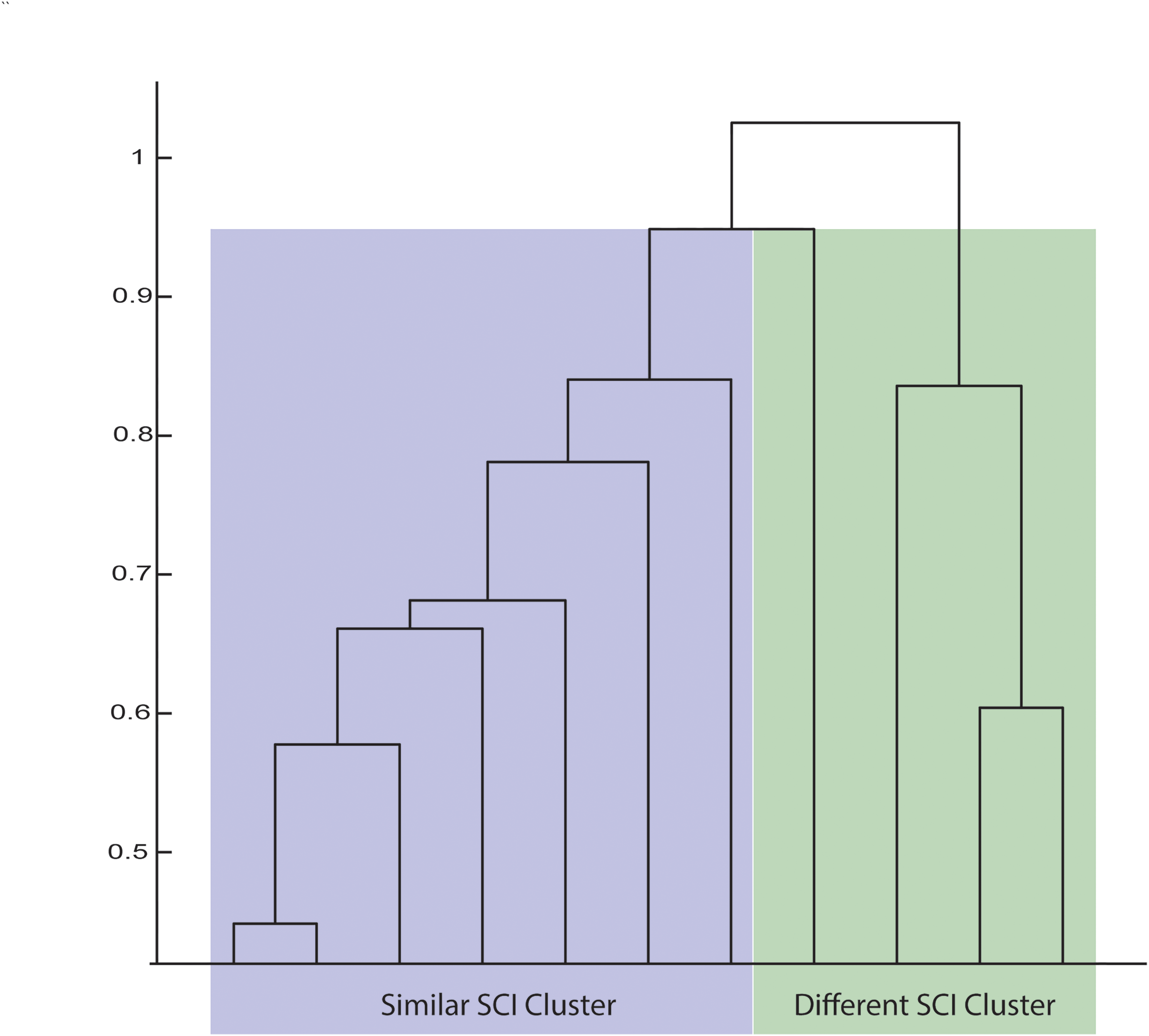
Dendrogram showing clusters based on average normalized EMG amplitude in each rocking cycle quartile for all muscles; EMG = Electromyography; SCI = Spinal cord injury.
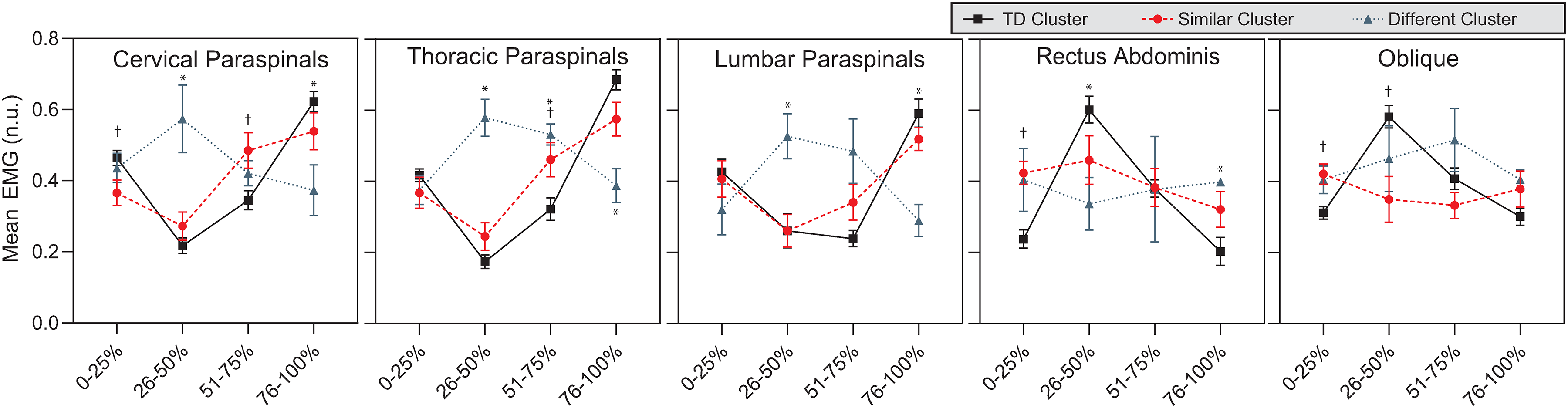
Average EMG amplitude in trunk muscles during each quarter of the rocking cycle for the typically developing (TD) cluster and two spinal cord injury clusters; n.u. = Normalized units; EMG = Electromyography.
Muscle activation amplitude
Figure 7 shows a heatmap of muscle activation in each muscle as measured by mean sEMG amplitude (μVRMS) during rocking. Each row represents one child, and each column represents one muscle. Muscles are sorted from left to right in a cephalocaudal direction. For children with SCI, the rows are sorted by SATCo score.
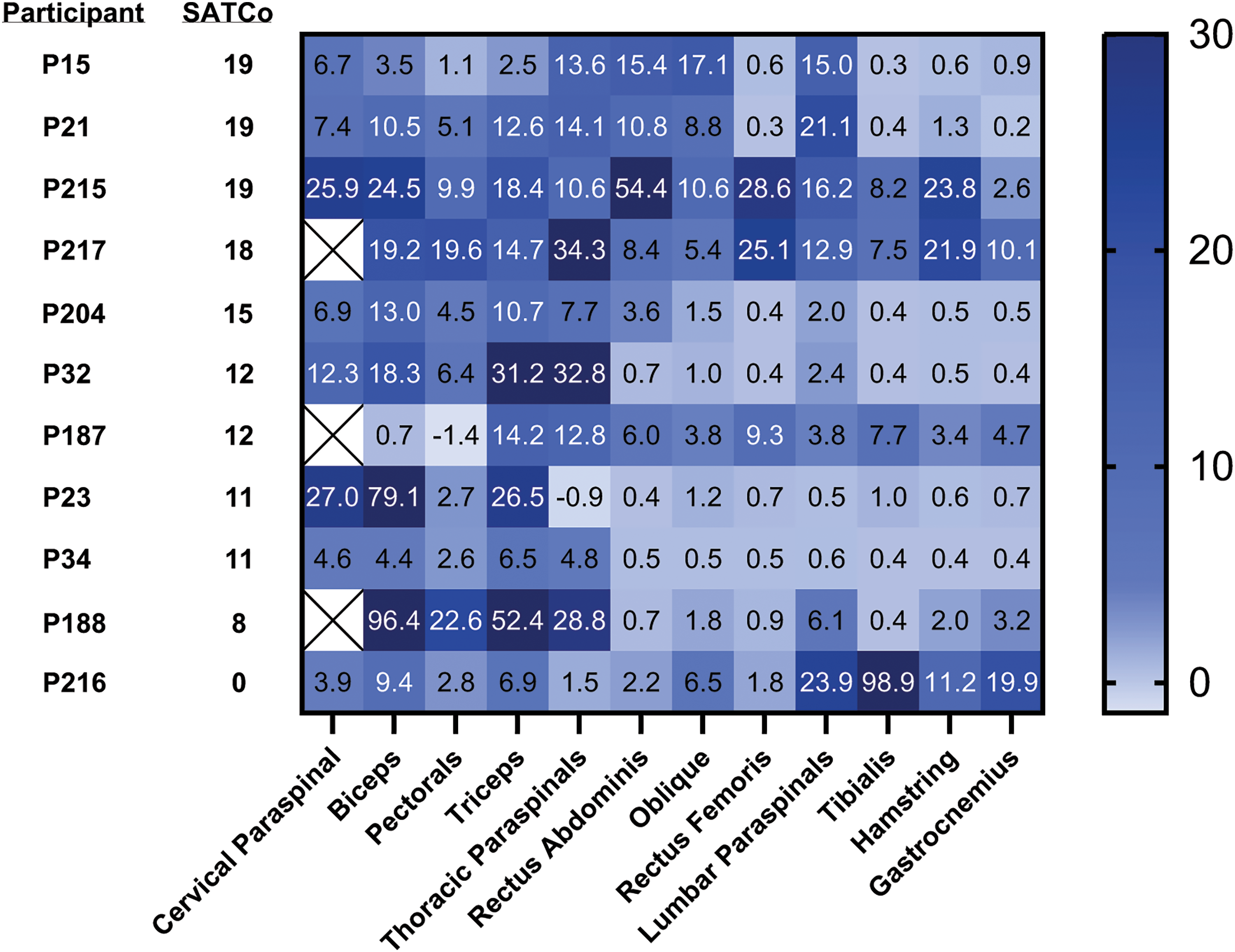
Muscle activation (µVRMS) heatmaps for spinal cord injury group; Higher numbers and darker colors represent higher activation; muscles are on x axis, sorted by spinal cord level of nerve roots. Y axis shows SATCo score, representing trunk control. SATCo = Segmental Assessment of Trunk Control; RMS = Root mean square.
Results of Spearman correlation analysis of SATCo vs. muscle activation amplitude for the SCI group are presented in Table 7. No significant correlation was observed for cervical or thoracic paraspinals; however, a significant positive correlation was observed for rectus abdominis (r = 0.89, p = 0.003), oblique (r = 0.73, p = 0.03), and lumbar paraspinals (r = 0.68, p = 0.05), indicating that participants with higher SATCo scores showed higher activation in muscles lower on the trunk than those with lower SATCo scores.
Activation amplitude during rocking vs. SATCo score.
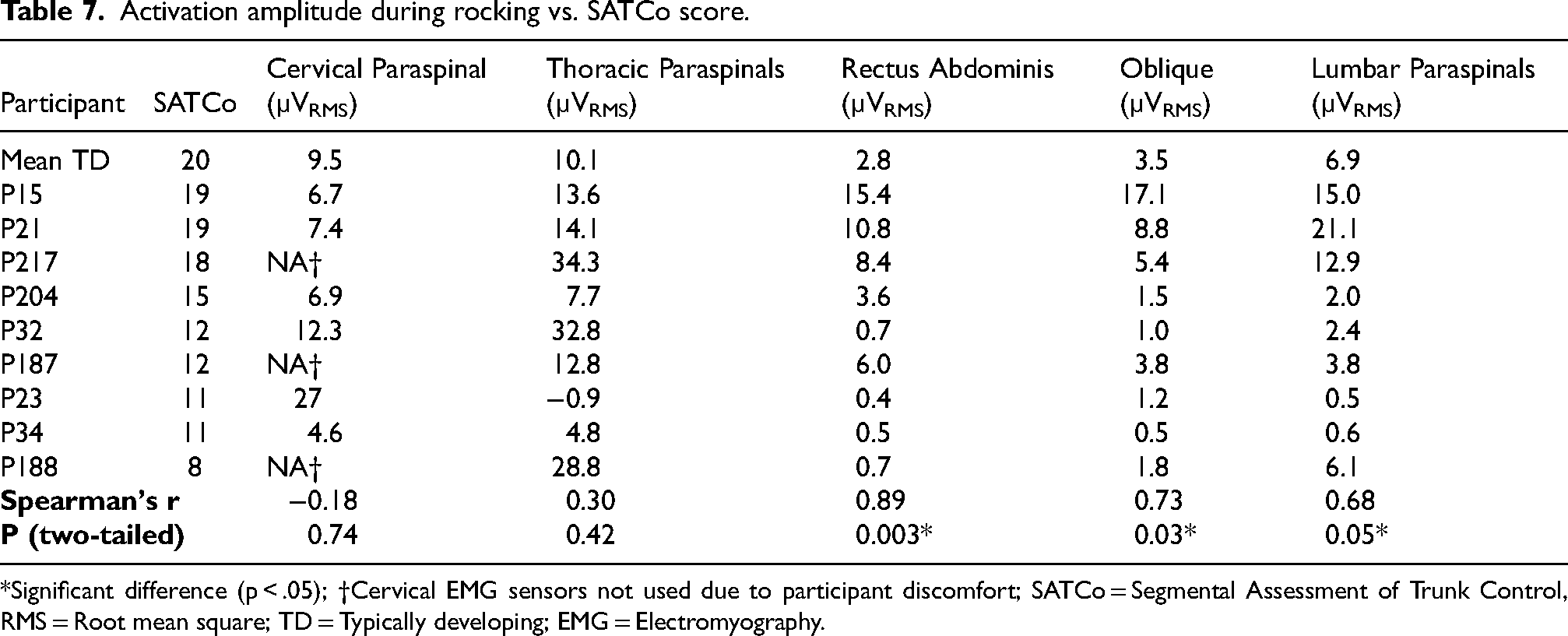
*Significant difference (p < .05); †Cervical EMG sensors not used due to participant discomfort; SATCo = Segmental Assessment of Trunk Control, RMS = Root mean square; TD = Typically developing; EMG = Electromyography.
Discussion
Of primary importance, the results confirmed the first hypothesis that trunk muscle activation would increase above baseline during rocking. In fact, all muscles tested in both TD and SCI groups showed significantly higher levels of activation during rocking than at baseline. Additionally, ES calculations showed that trunk muscle activations, with the exception of rectus abdominis, had an ES of medium or larger, confirming that activation levels are meaningful.
These results indicate that, in addition to activating trunk muscles and being helpful for children with poor trunk control, rocking may also facilitate leg muscle activation in those with SCI. Some who can activate leg muscles may remain non-ambulatory due to factors such as muscle weakness, poor balance, or the inability to manipulate an assistive device. Although ESs for leg muscle activation were low, even small activations in the context of rocking can be significant, as they can contribute to rocking motion. In the context of ABT, the primary goal is to achieve movement, and the permissive nature of the rocking environment allows for the activation of muscles that are otherwise rarely used. Over time, engaging in this activity may improve endurance due to the actual use of these muscles. Thus, rocking may serve as an accessible and enjoyable form of voluntary movement that utilizes available trunk and leg muscles.
The second research question asked whether there were differences between trunk muscle activation during rocking by children with SCI and TD children. Cluster analysis of temporal activation of muscles during the rocking cycle revealed two muscle activation patterns, a pattern similar to TD and a pattern dissimilar to TD, providing insights into the motor strategies employed by children with SCI during rocking. One notable finding was the higher variability in muscle activation patterns in the SCI group, and the presence of synchronous and counterbalance rocking strategies employed by the children with SCI. These different rocking strategies were at least partially reflected in the cluster analysis. For instance, three of the four participants in the “TD-dissimilar” cluster used the counterbalance strategy to rock, while none of those in the “TD-similar” cluster used this strategy.
Other potential reasons for the different cluster seen within the SCI group include differences in height between the SCI and TD groups and differences in previous experience with rocking. While the two groups were well-matched in other respects, they were unbalanced in height with a standardized difference score (SDS) of 0.399. The heights in the “TD-dissimilar” cluster were even farther (SDS = 0.964) from the TD group, raising the possibility that at least some of the differences between the groups may have been due to participant height. Additionally, while previous experience with rocking was not tracked, it is likely that the TD group tended to have more rocking experience than those in the SCI group. This was especially apparent in two of the youngest children with SCI who, as noted earlier, struggled initially with rocking and improved notably over the course of the rocking session. Another difference in experience was caused by repeat testing in two of the children due to technical problems with data collection in their first session.
A significant association was observed between trunk control, as measured by SATCo score, and activation of muscles lower on the trunk. This matched expectations, since higher SATCo scores reflect greater control and activation of trunk muscles in lower thoraco-lumbar areas. It should be noted that the two children with AFM were excluded from this analysis, since there is not a clear, level-dependent pattern of impairment with this etiology.
Primary motivations for investigating the use of a rocking chair in this population included accessibility and enjoyment. Importantly, there were no injuries during testing, and the identified safety concern has been addressed by repositioning a cross brace so that it no longer presents a potential to be a pinch point. It was found that all children included in the study were able to make the chair rock, regardless of previous experience or impairment. Feedback from children and parents during rocking also demonstrated that the children enjoyed rocking in the chair and were motivated to use their muscles to make it rock. These factors demonstrate that rocking gives children with SCI an enjoyable opportunity to move independently, which may be rare outside use of a wheelchair for mobility and thus particularly motivating for them.
Limitations
The results highlighted in this study should be interpreted considering identified limitations. As noted previously, there were several sources of noise in the sEMG data used for this analysis. While all of these were addressed, it is important to acknowledge that this does introduce some additional uncertainty regarding the accuracy of some of the source data.
Additionally, the SATCo scores of the participants, which indicated their inherent trunk control, ranged from zero to 19. However, the distribution skewed towards higher SATCo scores. Ideally, a more balanced distribution of SATCo scores would have been preferred to ensure a broader representation of participants across the entire spectrum of trunk control abilities.
As noted previously, confounding factors that may have influenced the results include differences in participant height between the SCI and TD groups, and lack of previous experience with rocking in some of the children with SCI. These may have contributed to differences in rocking between the SCI and TD groups; differences in rocking experience within the SCI group may have contributed to different rocking strategies, especially since two children returned for second rocking sessions due to technical issues in their initial session. These factors may have affected the temporal muscle activation patterns, which would in turn affect the clustering results.
Future work
To alleviate concerns about these potential confounding factors, several changes should be made in future work. Differences in experience with rocking could be accounted for and, to some extent, mitigated by surveying children on how much previous experience they have with rocking. Providing participants with substantial time to practice rocking would reduce the confounding effects of previous experience and allow muscle activation patterns to more closely resemble the patterns that would be seen with long term use of the rocking chair. Data on muscle activation patterns could also be taken before and after practice in the rocking chair, to study learning effects early in the experience with rocking.
Defining typical muscle patterns for the SCI group and how they differ from TD patterns is complicated by the wide variety of impairments, capabilities, and compensation strategies in the SCI group, and by differences (particularly height in this study) between the TD and SCI groups. To address this, future studies should focus on the ways that muscle activation patterns in specific children with SCI differ from the typical muscle activation patterns seen in TD children. Knowledge of these differences will help therapists to understand how children with SCI are compensating for impairments and may allow them to formulate strategies to help them activate muscles in patterns that more closely resemble TD patterns.
Future research should also aim to enroll children with a greater range of SATCo scores to better define the relationship between trunk control and muscle activation patterns during rocking, and allow for exploration of additional strategies to activate the desired muscles for rocking. For example, redesigning the footrest to attach to the seat of the chair instead of the base could target the use of trunk muscles, as it would prevent use of leg muscles initiating rocking by pushing the footrest. Additionally, asking children to take their arms off the armrests could encourage the use of trunk muscles for weight shifting stabilization during the FW and BW phases the rocking cycle.
Investigating the long-term use of rocking chairs in the home would be valuable to understand the different rocking strategies employed by children with SCI and the progression of neuromuscular activation and capacity. Chairs could also be equipped with sensors to monitor rocking performance, including parameters such as time spent and amplitude of rocking. Sensors could also be installed to detect forces applied to the rocking chair and provide valuable information about the muscles being utilized by the child during rocking. Other possible uses of sensor data would be to adjust the difficulty of rocking depending on the needs of the child, or to provide feedback in the form of a game to encourage the use of target muscles.
Conclusions
Rocking in this prototype glider rocking chair activates the neuromuscular system and is an accessible activity for children with varying degrees of trunk impairment due to SCI. Additionally, the study provides the first examination of the timing and amplitude of muscle activation during rocking, and the differences between TD and SCI groups. These results, combined with the observation that the rocking chair prototype is safe and enjoyable for children with SCI, highlight its potential as an effective tool for trunk muscle activation. This approach could extend ABT beyond the clinic, offering promising opportunities for use at home and in the community.
Footnotes
Acknowledgements
The authors would like to express gratitude to the children and families who participated in this study. Additionally, we would like to acknowledge the contributions of the research staff of the Kosair for Kids Center for Pediatric NeuroRecovery including Molly King, Research Manager; Lisa Clayton, Research Manager; Parth Parikh, Biomedical Engineer; the activity-based technicians at the Pediatric Neurorecovery clinic at Frazier Rehab Institute; Goutam Singh, PhD, Assistant Professor, Spalding University; and the Kentucky Spinal Cord Injury Research Center.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The National Science Foundation under Cooperative Agreement No. 1849213.