
Abstract
Purpose
Individuals with spina bifida (SB) often face substantial gaps in sexual and reproductive health (SRH) knowledge leading to low use of contraception, poor utilization of preventative sexual health care, unintended pregnancies, missed opportunities to pursue their SRH goals, and increased risk of abuse and coercion. Validated questionnaires are needed to reliably test and track the SRH and self-efficacy of adults with SB. This study aimed to develop a survey with content validity to assess five SRH domains in adults with SB.
Methods
An initial survey was informed by a targeted literature review as well as stakeholder and expert opinions. Social cognitive theory's self-efficacy concept, known for its predictive power in behavior change among those with physical disabilities, guided its development. The survey items were iteratively reviewed online by national sexual health experts using a modified Delphi method, assessing item clarity, relevance, and comprehensiveness. Then, cognitive interviews of the refined instrument were conducted with five adults with SB to analyze acceptance and understanding.
Results
Of the 26 potential panel members invited to participate, 22 (85%) responded and agreed to participate. There were seven urologists (two adult, five pediatric), six developmental pediatricians, six registered nurses from SB clinics, two physiatrists, and one medicine-pediatrics trained internist. Consensus was achieved after three rounds for 100 survey items. Following each round, items were refined through researcher consensus until the content validity index was met (agreement = 0.8–1.0) for each question, ensuring all domains were adequately represented. These domains included sexual knowledge/education, sexual practice, sexual safety/risk profile, history of abuse, and perceived self-efficacy.
Conclusion
Content validity, clarity, and functionality of a novel survey that probes five domains of SRH in adults with SB was established. The survey can be utilized in both research and clinical settings to assess baseline SRH knowledge, identify risky behaviors, and screen for sexual abuse.
Keywords
Introduction
Individuals with disabilities often face significant marginalization when it comes to accessing sexual and reproductive health (SRH) services. This marginalization can manifest in various ways, including limited access to information, stigma, and physical barriers to healthcare facilities.1–3 Evidence suggests that healthcare providers frequently view these individuals as asexual, leading to significant barriers in accessing SRH education and services. 4 Lack of SRH knowledge results in poor health outcomes and increases risk of abuse.4,5 Among adults born with spina bifida (SB), the most common and permanently disabling birth defect, only approximately 5% report discussing their sexual health with a healthcare professional.6,7 Despite medical advancements that have extended the lifespan of individuals with SB well into adulthood, there are still significant gaps in accessing SRH care, screening, and education.8,9
Adults with SB encounter unique challenges related to social opportunities, dating, and sexual health.10–12 Despite this, 50% of adults with SB report being sexually active by age 23, and nearly all express a desire for sexual intimacy by the same age. 13 However, these individuals often have limited knowledge about their reproductive health and pregnancy potential.14–16 Women with SB particularly report significant gaps in understanding these issues.15,16 Men with SB also face a notable deficiency in sexual education and approximately 75% experience erectile dysfunction, highlighting the urgent need for improved information on sexual health, function, and fertility.17,18 Both men and women with SB commonly show inadequate use of contraception (ranging from 9–43%), primarily due to a lack of awareness about how SB affects fertility and childbearing. 19 Additionally, low sexual self-esteem among individuals with SB can lead to sexual abuse, coercion, and avoidance of romantic relationships due to embarrassment over treatable sexual dysfunction.14,15
The Spina Bifida Association (SBA) has issued guidelines advocating for patient-centered SRH discussions for individuals with SB. 14 However, there are no standardized methods on how to deliver this information, what components should be included in the teaching, how individuals affected would like to receive the information, nor any outcome data that shows increased knowledge after teaching. Providers have expressed a desire to discuss these topics with their patients, but report a lack of knowledge and training in how to have these discussions.7,20 Developing a valid and reliable survey to measure sexual health literacy, self-efficacy, risky sexual behavior, and experiences of abuse will enhance SRH discussions in three key ways: 1) identifying knowledge gaps, 2) evaluating the effectiveness of SRH education interventions, and 3) serving as a clinical tool for providers initiating SRH conversations.
The primary objective of this study was to establish survey content validity utilizing a modified Delphi method as well as to examine clarity and functionality through cognitive interviews.
Methods
Preliminary survey development
The University of Alabama at Birmingham (UAB) Internal Review Board approval (IRB-161021001) was obtained to develop a 40-question deidentified sexual health survey on intimacy, sexual/reproductive knowledge, and sexual abuse by the multidisciplinary SB team at UAB and Children's of Alabama. A team of local survey experts and physicians specialized in SB care performed a targeted literature review and developed questions based on clinical expertise and published findings. After initial survey development, questions were vetted with a focus group comprised of local adults with SB and parents of children with SB. Due to the sensitive nature of this survey, a rigorous iterative process was used to design the questions and ensure tolerance and acceptability from potential participants. The questions were then sent to two national experts (pediatric urologist and adult psychiatrist) and revised at each step based on feedback. From March 2021 until April 2022, this survey was administered via phone call and during in-person UAB Adult Spina Bifida Clinic visits. These results were submitted for publication in a separate report (currently under review).
Conceptual framework
Theoretical frameworks, like social cognitive theory (SCT) introduced by Bandura in 1986, systematically explore the factors influencing specific behaviors. 21 SCT examines how past experiences, reinforcements, and expectations impact behavior and the motivations behind these actions. In SRH, SCT elucidates how observational learning, expectations, behavioral capability, and self-efficacy interact to influence behavior. Using SCT, a survey was created that could analyze how knowledge, skills, practice, and self-efficacy, coupled with access to information, predict health behaviors. 22 By using this framework in developing the survey, depicted in Figure 1, the relationship between SRH literacy levels and the risk and incidence of abuse and intimate partner violence can be examined. Additionally, the survey will evaluate self-efficacy in seeking SRH information and engaging in safe sexual practices, which will inform both the analysis of the data and the development of future interventions based on this research.
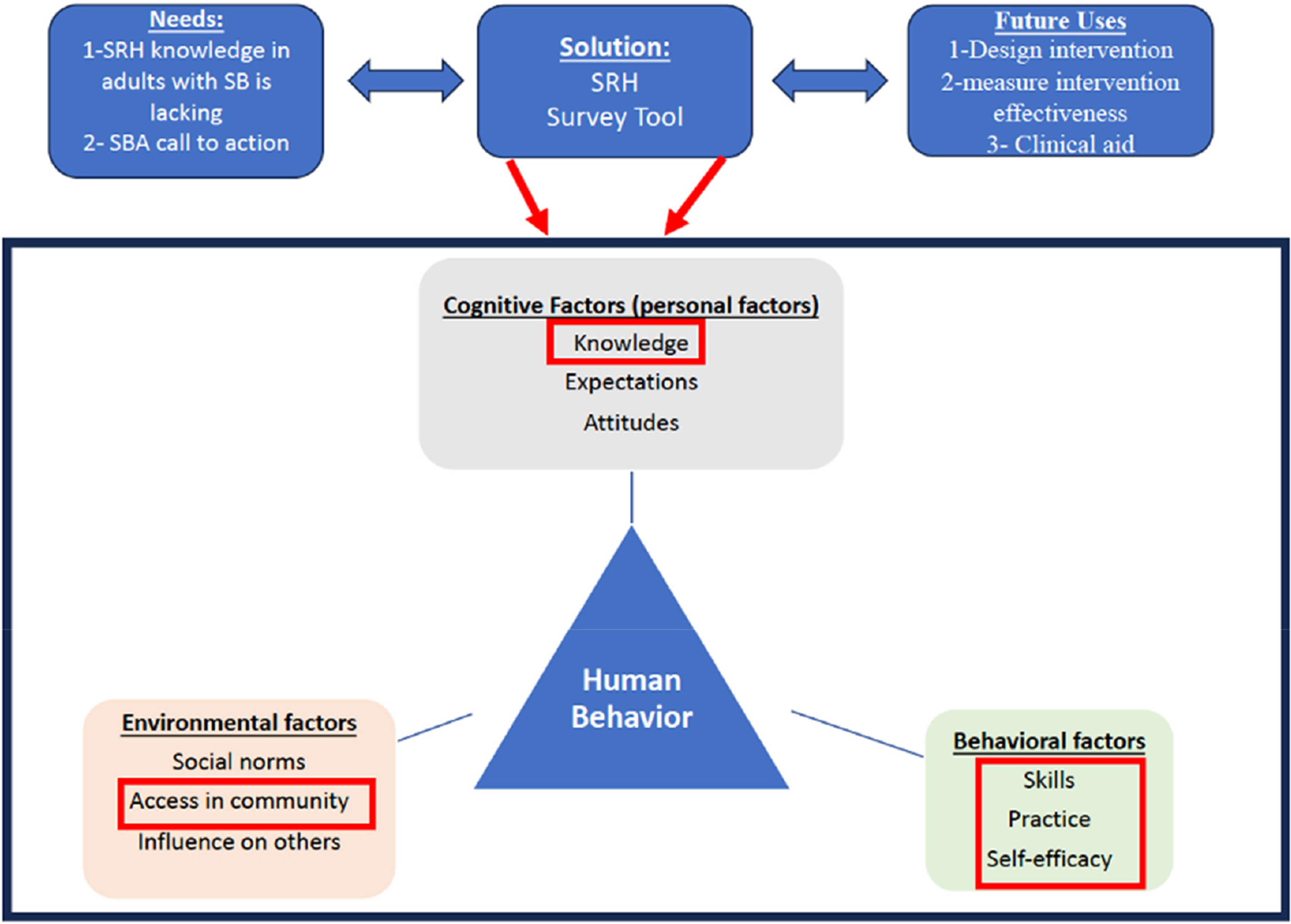
Conceptual framework. SB: spina bifida; SBA: Spina Bifida Association; SRH: sexual and reproductive health.
Survey instrument
Following the analysis of the preliminary data, a secondary target literature review, and application of the conceptual framework, the research team drafted a revised list of domains and survey questions. Based on this review, a section was added on baseline SRH knowledge and perceived self-efficacy to the previous survey. The development of the revised survey occurred by consensus among three investigators who had backgrounds in SB care and survey development. All domains and the items within the domains in the revised survey were discussed and kept if all three investigators involved in the revision reached unanimous agreement. These domains were 1) sexual knowledge/education, 2) current and past sexual practices, 3) sexual safety/risk profile, 4) current and past abuse, and 5) perceived self-efficacy.
Delphi method
A modified Delphi method was employed to establish content validity; this qualitative systematic approach includes quantitative components for measuring consensus and establishing the content validity index (CVI) with an expert panel. 23 This method is appropriate and particularly useful when empirical evidence is lacking, limited, or contradictory. 23 Potential expert participants who worked in large interdisciplinary SB clinics from geographically diverse locations across the United States and/or those who treated patients from across the lifespan were purposefully chosen to characterize the greatest background and knowledge of SRH in individuals with SB. These clinics were similar to the clinics that are represented in the National Spina Bifida Patient Registry (NSBPR) funded by the Centers for Disease Control. 24 By using these clinics, the likelihood that the providers selected had the most up-to-date information on research being done in SB care and had awareness of the SBA Guidelines, as well as that the clinics met the standards set forth by the NSBPR in size and diversity, was increased.14,24
An invitation email detailing the project's goals and requesting participation was sent to each potential participant, with consent implied upon survey completion. The invitations included information about confidentiality measures, the right to withdraw, and the removal of data. Privacy was maintained by anonymizing responses and storing data on encrypted, password-protected computers. While absolute anonymity was not possible due to email contact, strict measures were taken to protect data privacy, with only the lead author aware of participant identities, which were not shared with other panel members. The email invitation was sent in March 2023 and round 1 began April 2023 with data from round 1 analyzed in May 2023. Participants were given two weeks for each round. A total of three rounds were needed to achieve content validity of this survey. All of the steps of the Delphi process are described in Figure 2.
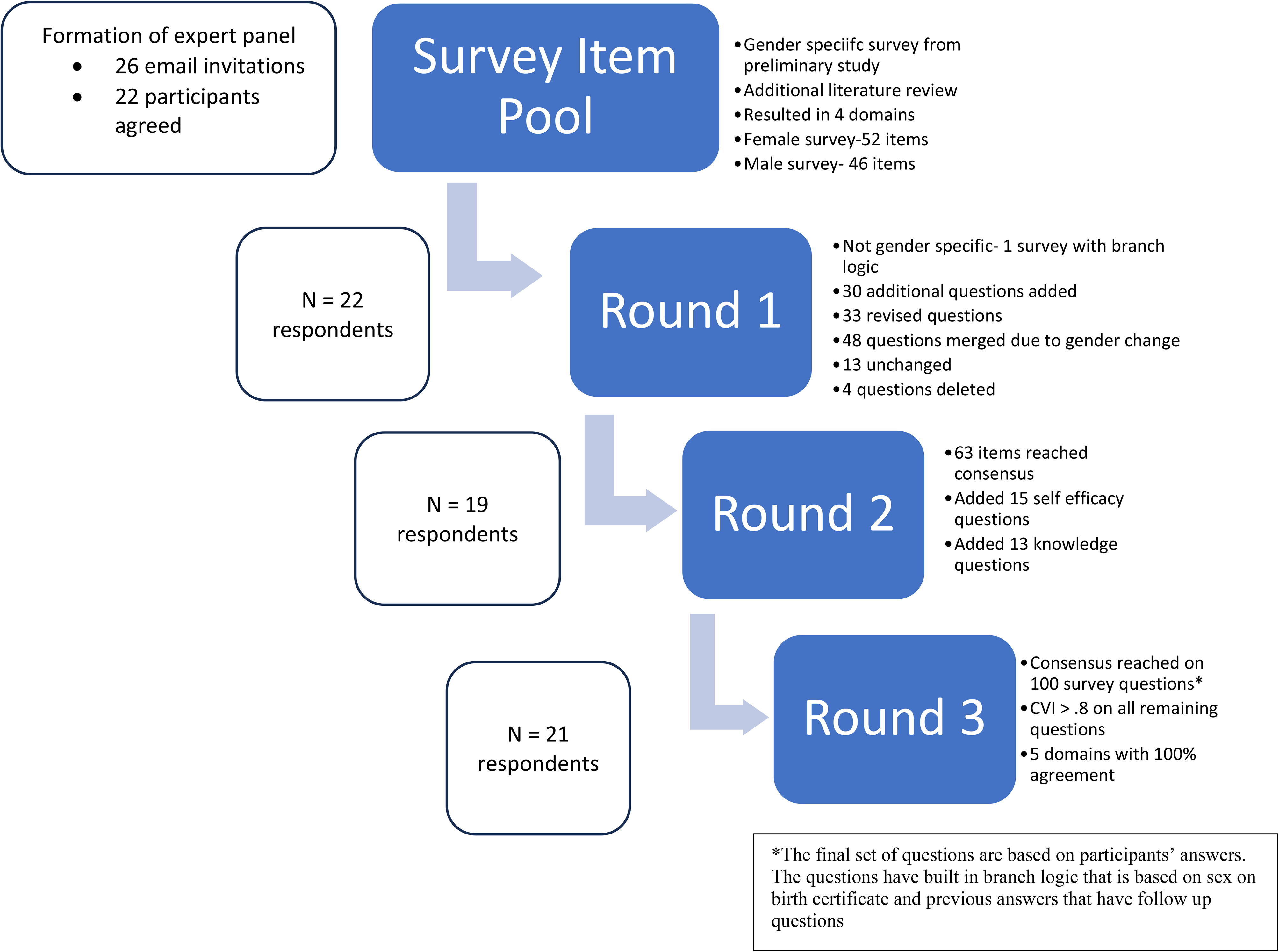
Steps of Delphi process. CVI: content validity index.
During each round, the survey questions were replicated in REDCap and for each survey question, respondents were asked to either select 1- keep question as written, 2- terminate question, or 3- revise question. In addition, at the end of each domain, respondents were asked to indicate if the questions in that section fully captured all aspects of the five domains of sexual practices of individuals with SB.
Delphi analysis
Content validity is the degree to which an instrument has an appropriate sample of items for the construct being measured. 25 The CVI is the most accepted and widely used measure for determining item agreement and relevance, noted for its advantages in ease of computation, understandability, and focus on agreement and consensus. 26 In this study, a CVI threshold of 0.8 was chosen to ensure that only items with substantial expert agreement were retained. The 0.8 cut-off is widely accepted in content validity studies as it reflects a high level of consensus among expert raters without being overly restrictive. 26 By setting the threshold at 0.8, it was ensured that each item demonstrated strong relevance and clarity, while still allowing for nuanced input and diverse perspectives from the expert panel. 26 To calculate the CVI of each item, the total number of individuals who selected either “keep as written” or “revise question” were totaled and divided by the total number of participants. A higher score indicated greater agreement amongst the expert panel. The formula of CVI is CVI = (Nk - Nt)/(N), in which the Nk is the number of panelists indicating “keep” or “revise,” Nt is the number of panelists indicating “terminate,” and N is the total number of panelists. If the question or domain had significant rewording based on the qualitative feedback from expert panelists, the research group (BH, DL, CT) voted to rephrase based on the recommendations of the panelists. If the item or section was reworded and this rewording was accepted unanimously by the research group, the item was placed into the next round of the Delphi process and a new CVI was calculated. The Delphi process was done, and agreement was achieved after three rounds. At the end of each round, items were revised by unanimous researcher consensus (BH, DL, CT), and the process was repeated until CVI was reached (agreement = 0.8–1.0) for each question and each of the five domains were stated to be adequately covered.
Cognitive interviews
After consensus was reached, cognitive interviewing was performed. Cognitive interviewing involves a semi-structured interview process that examines the ways in which people comprehend, process, and react to questions and their possible answers on a survey. This technique incorporates a “think aloud” approach, supplemented by probing questions, to assess respondents’ understanding of the questions, their ability to select appropriate answers from the given options, and their general emotions while completing the survey. 27 A cognitive interview guide was developed, informed by a tool created by Kolbe (Appendix 1: Cognitive Interview Guide). 28 Convenience sampling was used to pick five respondents from the adult SB clinic at UAB. In conducting cognitive interviews, participants’ informed consent, confidentiality, and voluntary participation was ensured. Data was securely handled, and findings were reported accurately, respecting participants’ autonomy and minimizing harm. The emotional impact of the study was considered, and participants were given the opportunity to opt out at any time. Respondents were asked to complete the survey during a recorded, online Zoom session while the interviewer (BH) asked probing questions about the respondents’ choices, actions, thoughts, and experiences as they were completing the survey. The probes targeted comprehension of the questions, ability to recall information, and response to determine how respondents chose their answers. Respondents were sent the survey before interviews and asked to review the survey in advance. At the conclusion of the cognitive interviews, suggested revisions were determined unanimously by members of the study team (BH, DL, CT) for each variable. These changes focused on rewording and reordering questions for improved understanding and acceptability of the survey by adults with SB.
Cognitive interview analysis
Interviews were transcribed using Zoom software, producing qualitative data for each question. This data was then organized into three key categories: 1) the respondent's understanding of the question's meaning and purpose, 2) their ability to recall the necessary information to respond accurately, and 3) their emotional reaction during the response process. The frequency of issues identified was calculated for each question and category by dividing the number of instances of a problem by the total number of interviews, and then multiplying the result by 100 to yield a percentage. Any issue with a frequency exceeding 20% was marked for potential revision. Revisions were reviewed by members of the study team (BH, DL, CT) for each affected variable.
Results
Expert panel and response rates
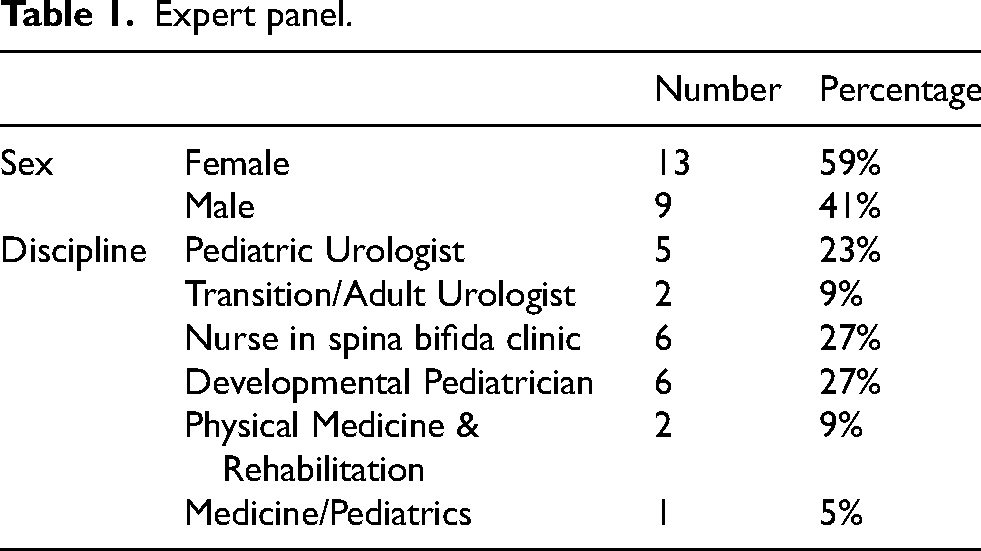
Of the 26 potential panel members invited to participate, 22 (85%) responded and agreed to participate. There were seven urologists (two adult, five pediatric), six developmental pediatricians, six registered nurses from SB clinics, two physiatrists, and one medicine-pediatrics trained internist. Round 2 was completed by 19 participants (86% of round 1 participants) and round 3 was completed by 21 participants (95%) (Table 1). The cognitive interviews were completed by five participants. Demographic data of these participants is in Table 2.
Expert panel.
Cognitive interview participants.
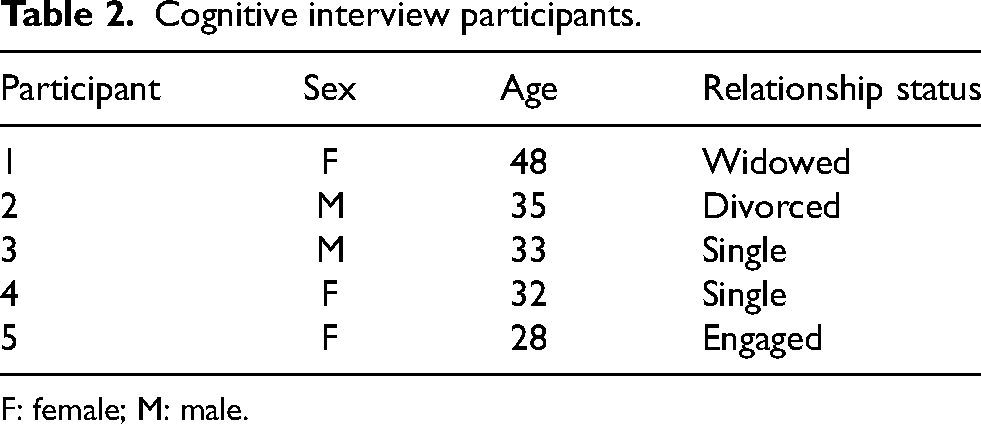
F: female; M: male.
Round 1
In the first round, there was a female survey that had 52 questions and a male survey that had 46 questions. The primary change in this round involved removing the gender-specific survey and instead creating one survey with branch logic built within the design of the survey.
Of the original 98 questions, after round 1 48 questions were merged due to the transition from a gender-based survey, 33 questions were revised, 13 questions remained unchanged, and four questions were deleted. Thirty additional questions were added based on free text revisions from the expert panel. Appendix 2 provides a complete summary of the recommended revisions. All revisions made were unanimously accepted by study team members (BH, DL, CT) and then became part of the survey for the next round.
Round 2
There was significant revision between round 1 and round 2 based on expert panel feedback. Therefore, most of the survey was placed into round 2 except where clear consensus had been reached in round 1. For each question, participants were shown the revised question and a new CVI was calculated based on their responses. Some overall feedback during round 2 included a desire to assess self-efficacy and baseline SRH knowledge. The research team conducted an additional focused literature review and added 13 additional questions on SRH knowledge and 15 questions on perceived self-efficacy to round 3. At the conclusion of round 2, consensus was reached on 63 survey questions.
Round 3
Only the added questions, the survey questions that did not reach consensus in round 2, or questions that had significant revisions based on qualitative responses were added to round 3. After round 3, all 100 questions had reached greater than 0.8 CVI. This comprised all questions regardless of sex and included all possible questions based on branch logic. There were questions related to pregnancy and fertility that were based on the respondents’ indicated sex on their birth certificate. There were also follow-up questions based on some responses. Therefore, a single participant would not answer 100 questions, but the total questions that reached a CVI of 0.8 or higher was 100. At the conclusion of the final round, the total CVI for each domain was as follows: Demographics- 0.82, Sexual Knowledge and Education- 0.94, Current Sexual Practice- 0.83, Sexual Safety/Risk Profile- 0.94, Sexual Coercion/Abuse- 0.94, Perceived Self-Efficacy- 0.95. Appendix 3 includes the final full version of the survey.
Cognitive interviews
The cognitive interviews did not yield a problem frequency higher than 20% on any given survey question; however, there were minor suggestions made related to word choice or order of questions. This feedback was recorded and reviewed with members of the study team. Based on this feedback, the research team unanimously decided to reorder two questions and provide additional description of the potential responses on one question.
Discussion
In this study, a comprehensive survey was developed using mixed methods aimed at assessing sexual health literacy, current sexual practices, risky behaviors, perceived self-efficacy, and the risk or presence of abuse among adults with SB. This survey resulted in a high average CVI, suggesting that it had good content validity and all domains had been adequately addressed. A CVI of 0.80 or higher with three or more experts was evidence of good content validity. 26 In addition, cognitive interviewing led to very few changes in the survey, suggesting that it is understandable and acceptable to adults with SB. To the authors’ knowledge, this survey is the first developed to assess SRH in adults with SB.
This survey could be an important first step in meeting the guidelines for patient-centered SRH discussions for individuals with SB set forth by the SBA. 14 This survey could be used by clinicians to examine SRH knowledge and practice in adult patients with SB and allow a mechanism to open discussions surrounding these topics. However, because providers have reported that they lack the knowledge and training in how to have these discussions with adults with SB, this survey could also be used to evaluate the success of education programs while training providers on how to have these important discussions and teaching which domains are relevant.7,20 Regardless of whether this survey is being used to evaluate SRH issues in patients or SRH education programs for patients, it could help start the process of addressing the knowledge gaps14–19 and lack of screening for abuse/coercion14,15 reported by adults with SB.
The survey's development spanned several years and was informed by input from a wide range of stakeholders, including local experts at a large multidisciplinary SB clinic, individuals with lived experience, and a national panel of experts. This survey was also informed at each step by recent literature and the collective wisdom of the research group. The significant revisions made between rounds 1 and 2 of the Delphi method highlight the importance of incorporating insights from an interdisciplinary panel of experts. Moreover, the blinding and separation of the Delphi experts allowed all voices to be heard and limited any one person's opinion. 23 Prior to this study, the survey was tested in a sizeable and diverse adult SB clinic, and the findings from that experience were integrated into the initial round of this study (with results pending publication). This prior work, along with the diverse representation from the expert panel, contributes to the robustness of this study. Additionally, the inclusion of free-text responses for the suggested revisions of each question greatly enhanced the survey's clarity, relevance, and overall effectiveness. Finally, cognitive interviewing was used to ensure that adults with SB found the survey was understandable and acceptable. Since little change was required, it can be safely assumed that they understood and accepted this survey. Cognitive interviewing has been successfully used to ensure that surveys and interventions are understandable, likable, and easy to use. 27
In this survey, additional questions were incorporated to assess both baseline knowledge and self-efficacy. The research team identified a gap in the previous format, which focused on the history of educational exposure but lacked direct measures of knowledge. Consequently, specific knowledge assessment items were added. Recognizing that knowledge alone does not necessarily translate into behavior change or adherence to safe sexual practices, self-efficacy measures, a well-established predictor of health behaviors, were included. 21 These additions enabled the survey to evaluate participants’ confidence in seeking health information from providers and in practicing or advocating for safe sexual behaviors.
Furthermore, individuals with SB face unique health challenges that make them particularly vulnerable to sexual abuse and misconduct. These challenges include conditions such as neurogenic bladder, often managed by clean intermittent catheterization performed by a caregiver, precocious puberty, and early caregiver dependence. According to the World Health Organization, sexual health is defined as a state of physical, emotional, mental, and social well-being in relation to sexuality—not merely the absence of disease or dysfunction. 29 This definition emphasizes a positive and respectful approach to sexuality and sexual relationships, ensuring that individuals can experience pleasurable and safe sexual experiences free from coercion, discrimination, and violence. Sexual well-being is crucial for reducing stress, regulating sleep, and maintaining overall physical and mental health through various psychological and biological processes. 30 Given these considerations, this survey offers a tool for clinics to begin assessing the risk of abuse and misconduct while promoting positive sexual well-being among individuals with SB. As clinics implement this survey, it will be essential to have a plan in place for responding to positive abuse screenings.
While adding another survey to a busy clinic could pose challenges, this tool was designed for both research and clinical use. Although the survey may appear lengthy, it employs branch logic to tailor questions based on prior responses, reducing respondent burden. In clinical settings, many demographic questions can be omitted, and administering the survey early in the visit on iPads or other electronic devices is recommended, as these clinics often have downtime between providers. The survey is organized by domain, allowing clinics the flexibility to administer only the most relevant sections based on patient needs or specific clinical goals. Recognizing that individuals with SB may have cognitive deficits, the survey begins with a question to indicate whether it is being completed independently or with support. When interpreting results, it is important to consider how the survey was completed, as caregiver assistance could introduce bias.
Limitations and future directions
A limitation of this study is that the survey may not be suitable for individuals with low literacy or those with high caregiver dependence, as these factors could impact their ability to independently complete the survey. Additionally, due to the sensitive nature of the questions, some participants may be reluctant to engage with the survey in a clinical setting, potentially affecting response rates. As a result, the findings may not be fully generalizable to all adults with SB. However, by selecting experts from diverse regions across the United States with experience in both pediatric and adult SB clinics, and conducting comprehensive cognitive interviews, the survey was ensured to be both appropriate and applicable for its intended population.
Although the survey was specifically designed and validated for adults with SB, the insights gained will be invaluable in identifying knowledge gaps that can inform interventions in pediatric clinics. Administering the survey to patients aged 18 and older enables clinics to pinpoint critical areas where education is most needed, facilitating the development of targeted interventions based on these findings. The goal is for this survey to become a tool in interdisciplinary SB clinics, with the potential to inspire the development of a pediatric version and inform interventions to enhance SRH knowledge in individuals with SB.
Conclusion
Using a modified Delphi technique, content validity was established for a survey to assess five domains of SRH in adults with SB. This survey represents a valid tool that could be used for both clinical or research purposes to 1) determine gaps in knowledge, 2) evaluate the effectiveness of SRH education interventions by providing a baseline for knowledge, 3) screen for abuse and risky behavior, and 4) serve as a clinical aid for providers when initiating SRH conversations with their patients. Evaluating the psychometric properties of this survey will be an important next step.
Supplemental Material
sj-pdf-1-prm-10.1177_18758894241304357 - Supplemental material for Development and content validation of a survey assessing domains of sexual and reproductive health in adults with spina bifida
Supplemental material, sj-pdf-1-prm-10.1177_18758894241304357 for Development and content validation of a survey assessing domains of sexual and reproductive health in adults with spina bifida by Betsy Hopson, Ching Man Carmen Tong, Courtney Streur, Brandon G Rocque, Jeffrey Blount, Nataliya Ivankova and Donald H Lein Jr in Journal of Pediatric Rehabilitation Medicine
Supplemental Material
sj-pdf-2-prm-10.1177_18758894241304357 - Supplemental material for Development and content validation of a survey assessing domains of sexual and reproductive health in adults with spina bifida
Supplemental material, sj-pdf-2-prm-10.1177_18758894241304357 for Development and content validation of a survey assessing domains of sexual and reproductive health in adults with spina bifida by Betsy Hopson, Ching Man Carmen Tong, Courtney Streur, Brandon G Rocque, Jeffrey Blount, Nataliya Ivankova and Donald H Lein Jr in Journal of Pediatric Rehabilitation Medicine
Supplemental Material
sj-pdf-3-prm-10.1177_18758894241304357 - Supplemental material for Development and content validation of a survey assessing domains of sexual and reproductive health in adults with spina bifida
Supplemental material, sj-pdf-3-prm-10.1177_18758894241304357 for Development and content validation of a survey assessing domains of sexual and reproductive health in adults with spina bifida by Betsy Hopson, Ching Man Carmen Tong, Courtney Streur, Brandon G Rocque, Jeffrey Blount, Nataliya Ivankova and Donald H Lein Jr in Journal of Pediatric Rehabilitation Medicine
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.