
Abstract
Background
To determine the serum levels of endoplasmic reticulum (ER) chaperones, glucose-regulated protein 78 (GRP78), glucose-regulated protein 94 (GRP94), calnexin, and calreticulin in patients with lung cancer and in the control group and to evaluate the relationship between chaperone levels and clinical data and patient survival.
Methods
GRP78, GRP94, calnexin and calreticulin were measured in serum by ELISA. The serum chaperone levels of patients with lung cancer and the control group were compared. The relationship between serum chaperone levels and clinical data and patient prognosis was evaluated. The median survival time was calculated using the Kaplan-Meier method. Cox regression analysis was performed to determine the hazard ratio of ER chaperones considering prognostic factors.
Results
The serum levels of all ER chaperones GRP78, GRP94, calnexin, and calreticulin were higher in patients with lung cancer than in the control group and correlated with each other. Serum calreticulin levels were not affected by demographic and clinical characteristics. Serum levels of GRP78, GRP94, and calnexin were not associated with survival. However, median survival ± SE (95%CI) was 16.00 ± 1.72 (12.62–19.38) months in patients with serum calreticulin levels of 250.52 ng/ml and above, while it was 8.00 ± 1.38 (5.29–10.71) months in patients with calreticulin levels below the cut-off value (log-rank = 6.919; p = 0.009). Calreticulin impacted survival, even after adjustment for sex, histologic subtype, stage, treatment, and response to chemotherapy, which impacted survival [HR (95%CI): 0.656 (0.433–0.995); p = 0.047].
Conclusion
Calreticulin is promising for delineating risk groups in lung cancer screening studies, guiding treatment and monitoring outcomes.
Introduction
Lung cancer is the most common cause of cancer deaths worldwide. Its incidence continues to increase due to its etiologic link to tobacco and tobacco products.1,2 Two thirds of patients are diagnosed at a locally advanced/advanced stage and therefore have no chance of curative treatment. Despite staging and treatment efforts, the prognosis of locally advanced/advanced stage patients is poor and their five-year survival rate is between 31 and 7%. 3
In recent decades, research into new drugs based on the molecular pathogenesis of lung cancer has intensified, and some of these efforts have yielded results. These studies aim to transform lung cancer into a chronic disease by silencing the molecular signalling pathways that cause disease progression and prolonging survival as much as possible. Better results have been achieved with targeted therapies for non-small cell lung cancer (NSCLC), especially adenocarcinomas. These driver mutations are only detected in about 15–20% of patients. In small cell lung cancer (SCLC), these mutations do not work. 4 In recent years, immunotherapy has been shown to improve the survival rate of some patients with lung cancer. 5 However, there is currently no treatment modality that can be applied to large groups of patients with lung cancer, and there is still a need for studies on molecular signalling pathways and new therapeutics that can affect these pathways.
The endoplasmic reticulum (ER) is an important intracellular organelle involved in many cellular processes, especially protein synthesis and processing. 6 Misfolded polypeptides, excess subunits of oligomeric groups or incorrectly assembled oligomers are recognised and degraded by quality control systems. 7 In this way, the accumulation of misfolded proteins is prevented. When the capacity to correctly fold proteins or to degrade proteins that fail quality control is exceeded, misfolded proteins begin to accumulate in the lumen of the ER and ER proteostasis is disrupted. This situation is referred to as ER stress.8,9 After the occurrence of ER stress, the process known as Unfolded Protein Response (UPR), which allows the activation of some intracellular signaling pathways, is activated to restore the equilibrium and eliminate this situation in the cell.9,10 The UPR attempts to temporarily stop protein translation, induce molecular chaperones and enzymes in the ER that increase the folding capacity of proteins, activate a cascade of signaling molecules to initiate the process of detachment or degradation of misfolded proteins and restore ER equilibrium.11,12 In case of failure, the cell undergoes apoptosis.
Changes in the cell microenvironment during carcinogenesis cause ER stress and UPR. Cancer cells escape apoptosis, i.e. UPR does not act as a terminating effect, but plays a role in phases that contribute to tumor growth, such as angiogenesis, metastasis and chemoresistance. Uncovering the molecules and pathways involved in ER stress and UPR in lung cancer, which claims the lives of more than one and a half million people each year, linking these molecules to clinical patient data and targeting molecules involved in key pathways may offer new hope for treatment.
In this study, we aimed to determine the protein levels of ER molecular chaperones, glucose-regulated protein 78 (GRP78), glucose-regulated protein 94 (GRP94), calnexin and calreticulin in the serum of patients with lung cancer and in the control group by enzyme-linked immunosorbent assay (ELISA) and to investigate the relationship between the protein levels of the chaperones and the clinical data and survival of the patients.
Material and methods
Participants
A total of 140 patients with lung cancer who were diagnosed, treated and followed up between October 2017 and December 2018 at the Department of Chest Diseases, Faculty of Medicine, Eskisehir Osmangazi University were included in the study. All patients provided written informed consent for the study. Patients who had already received antitumor therapy and had a second primary cancer were not included in the study. The ethics committee of Eskisehir Osmangazi University approved the study (IRB number = 12.04.2018–12). In addition, 30 healthy volunteers who did not have cancer and had given their written consent were included in the study as a control group.
Sera from patients with lung cancer were collected before treatment and stored at −80°C in the biobank of the Lung and Pleural Cancers Research and Clinical Center of Eskisehir Osmangazi University until the time of analysis. The data including demographic and clinical characteristics and survival time of patients with lung cancer were obtained from the database of the same center. Age, sex, smoking history, concomitant diseases, histologic subtype, stage, type of treatment, response to chemotherapy, date of diagnosis and date of death of patients with lung cancer were recorded. The three most common histopathological subtypes, small cell carcinoma, adenocarcinoma and squamous cell carcinoma of lung cancer, were included in the study.
ER chaperones assays
GRP78, GRP94, calnexin, and calreticulin (ng/ml) were measured in serum using the Human ELISA kit (Bioassay Technology Laboratory, Shanghai, China). Assays were run according to the manufacturer's instructions, blinded to patient data. Absorbance was measured at 450 nm (ThermoFisher Scientific, Vartaa, Finland). Concentrations were calculated using the standard curves. The relationship between serum protein levels and clinical data and the patient prognosis was evaluated.
Statistical analysis
SPSS (version 15.0) and MedCalc Statistical Software (version 19.1.16, Medcalc Software Ltd, Ostend, Belgium) were used to analyze the data. Categorical variables were reported in the study with frequency and percentage. Continuous data were reported in the study as mean ± SD, median and min-max values. For continuous data, normality tests were performed and graphs were created. The data with abnormal distribution were converted to a normal distribution by logarithmization. Parametric tests (t-test and one-way ANOVA) were performed to compare the data. The Pearson correlation test was used to test the relationship between the parameters.
The median survival time and the 95% confidence interval were calculated using the Kaplan-Meier method. Survival time was defined as the time between the date of pathologic diagnosis and the date of death or last visit. The median value of the control group was used as the cut-off value for ER chaperones. A log-rank test was performed to determine the significance of ER chaperones for survival. A Cox regression analysis was performed to determine the hazard ratio (HR) and 95% confidence intervals of ER chaperones, adjusting for prognostic factors.
Results
The mean age of the 140 patients with lung cancer was 64.37 ± 9.11 years, that of the 30 control group 56.97 ± 9.81 years. The ratio of female to male was 14/126 and 5/25, respectively. Table 1 shows the demographic and clinical characteristics of patients with lung cancer.
Demographic and clinical characteristics of patients with lung cancer.
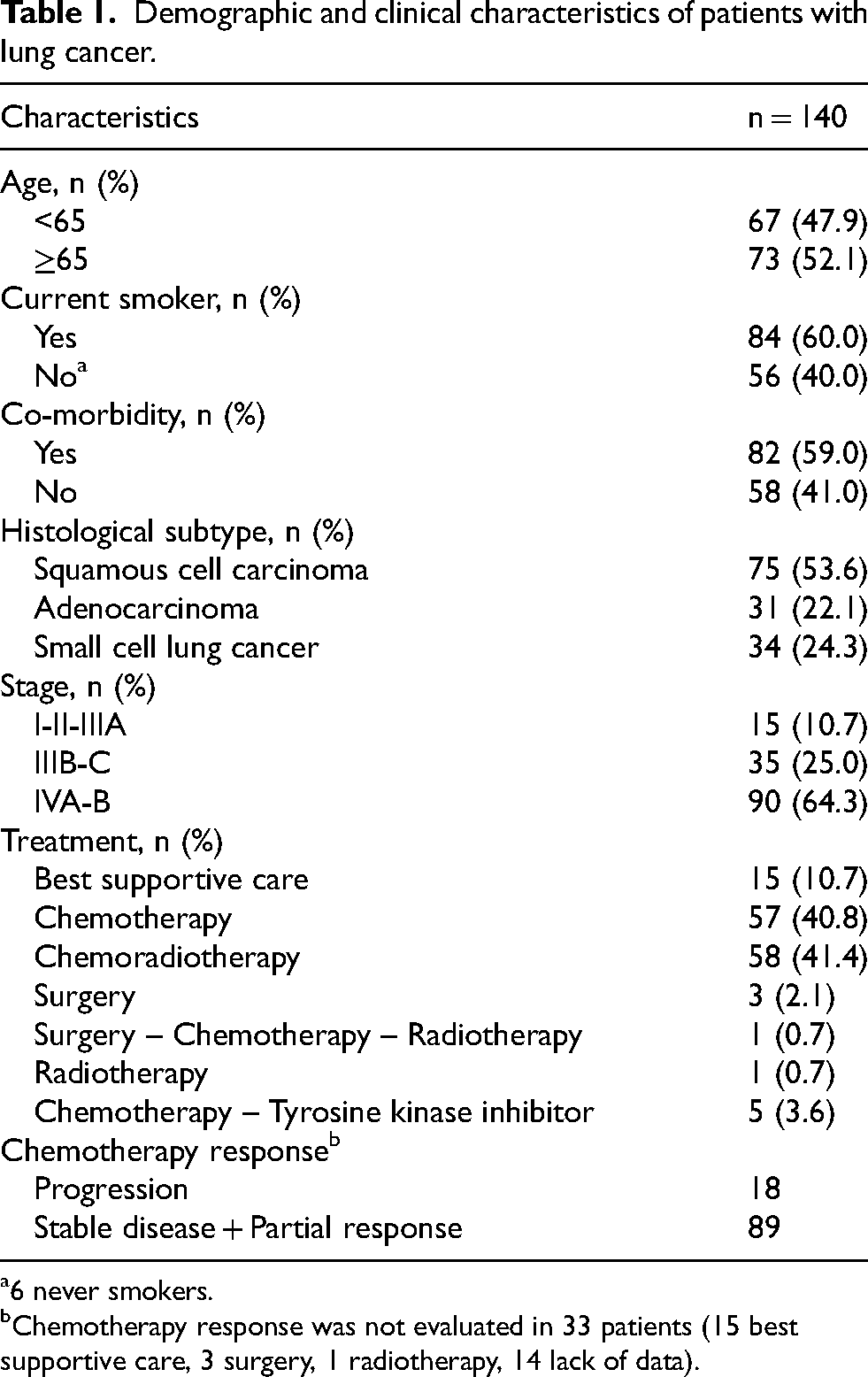
6 never smokers.
Chemotherapy response was not evaluated in 33 patients (15 best supportive care, 3 surgery, 1 radiotherapy, 14 lack of data).
The comparison of serum levels of GRP78, GRP94, calnexin and calreticulin in the patients with lung cancer and the control group is shown in Table 2. Serum levels of GRP78, GRP94, calnexin and calreticulin were significantly higher in patients with lung cancer than in the control group (Table 2).
Comparison of GRP78, GRP94, calnexin, and calreticulin levels of lung cancer patients with those of control group.
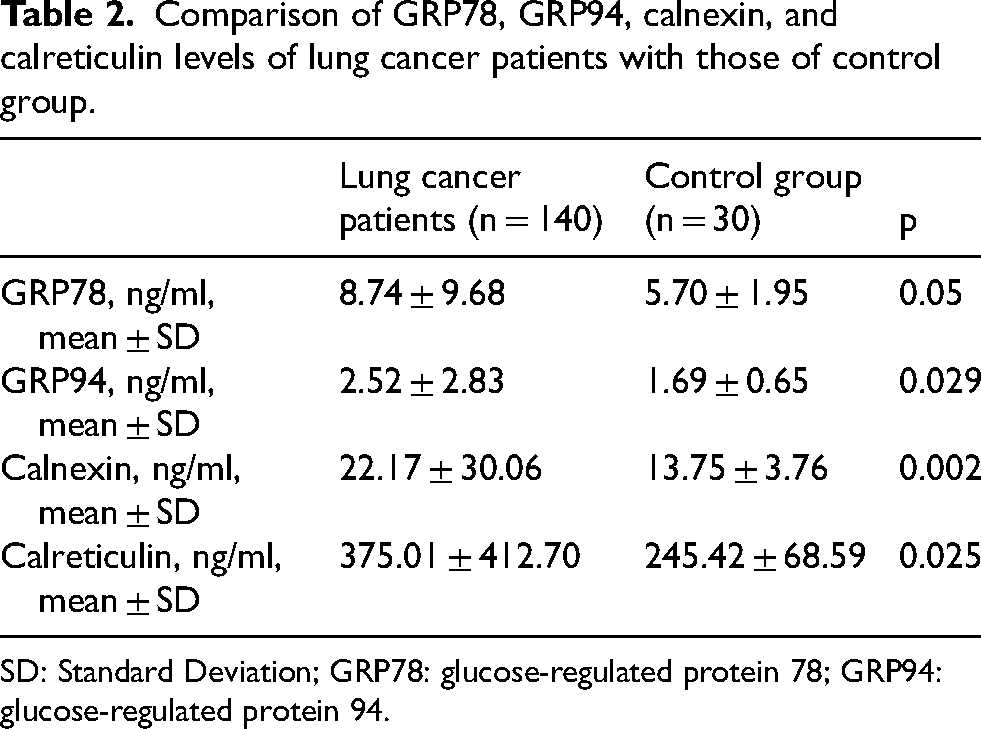
SD: Standard Deviation; GRP78: glucose-regulated protein 78; GRP94: glucose-regulated protein 94.
The correlation between the serum levels of GRP78, GRP94, calnexin and calreticulin in patients with lung cancer was investigated (Figure 1). In lung cancer patients, serum levels of GRP78, GRP94, calnexin and calreticulin were positive and strongly correlated (p < 0.001 for all).
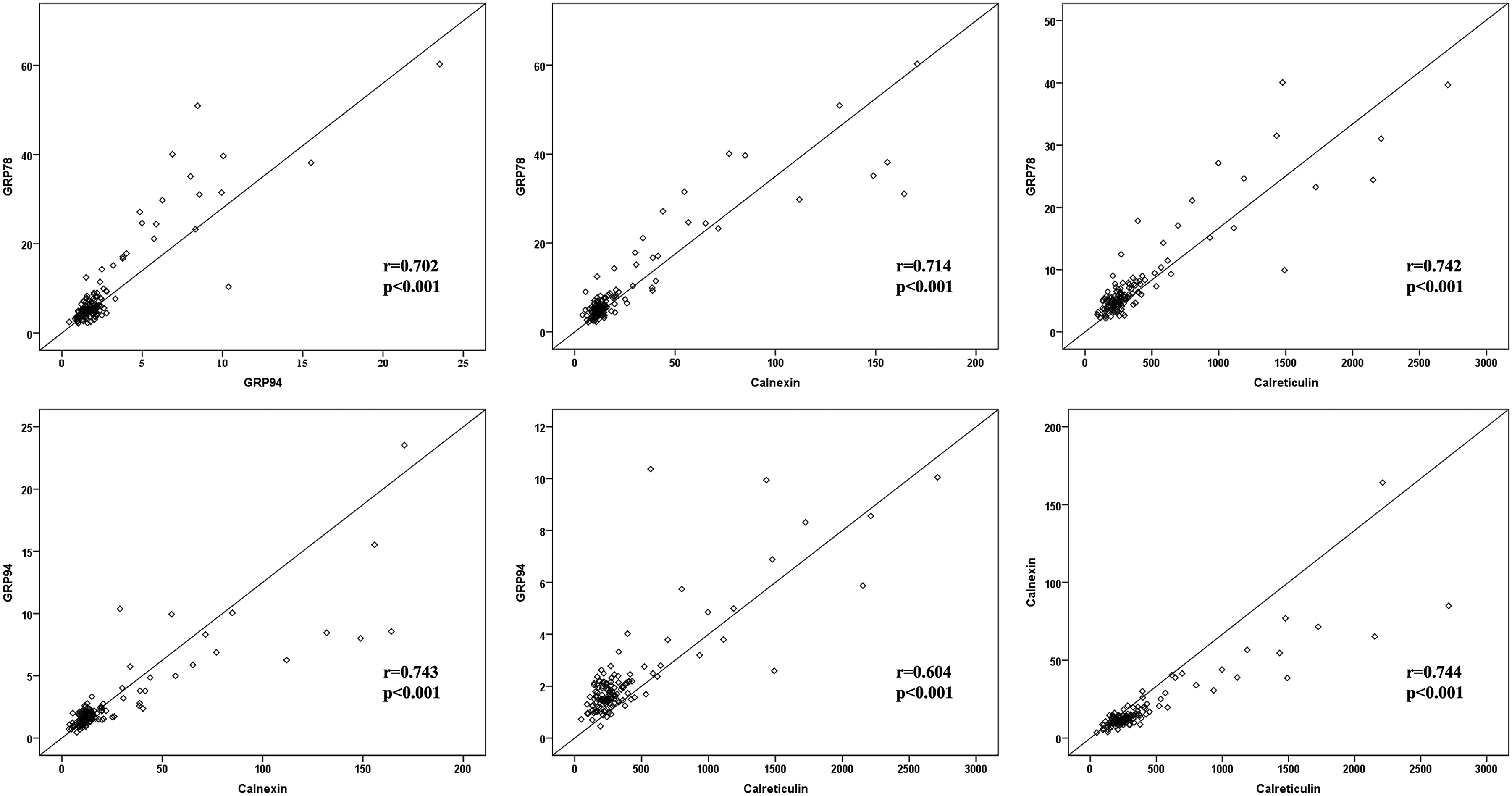
Correlation between serum levels of GRP78, GRP94, calnexin and calreticulin in patients with lung cancer. a-correlation of GRP78 with GRP94; b-GRP78 with calnexin; c-GRP78 with calreticulin; d-GRP94 with calnexin; e-GRP94 with calreticulin; f-calnexin with calreticulin. GRP78: glucose-regulated protein 78; GRP94: glucose-regulated protein 94.
The distribution of serum levels of GRP78, GRP94, calnexin and calreticulin in lung cancer patients according to age, sex, active smoking, comorbidity status, histologic subtype and stage is shown in Table 3.
Comparison of serum levels of GRP78, GRP94, calnexin, and calreticulin by demographic and clinical characteristics of lung cancer patients.
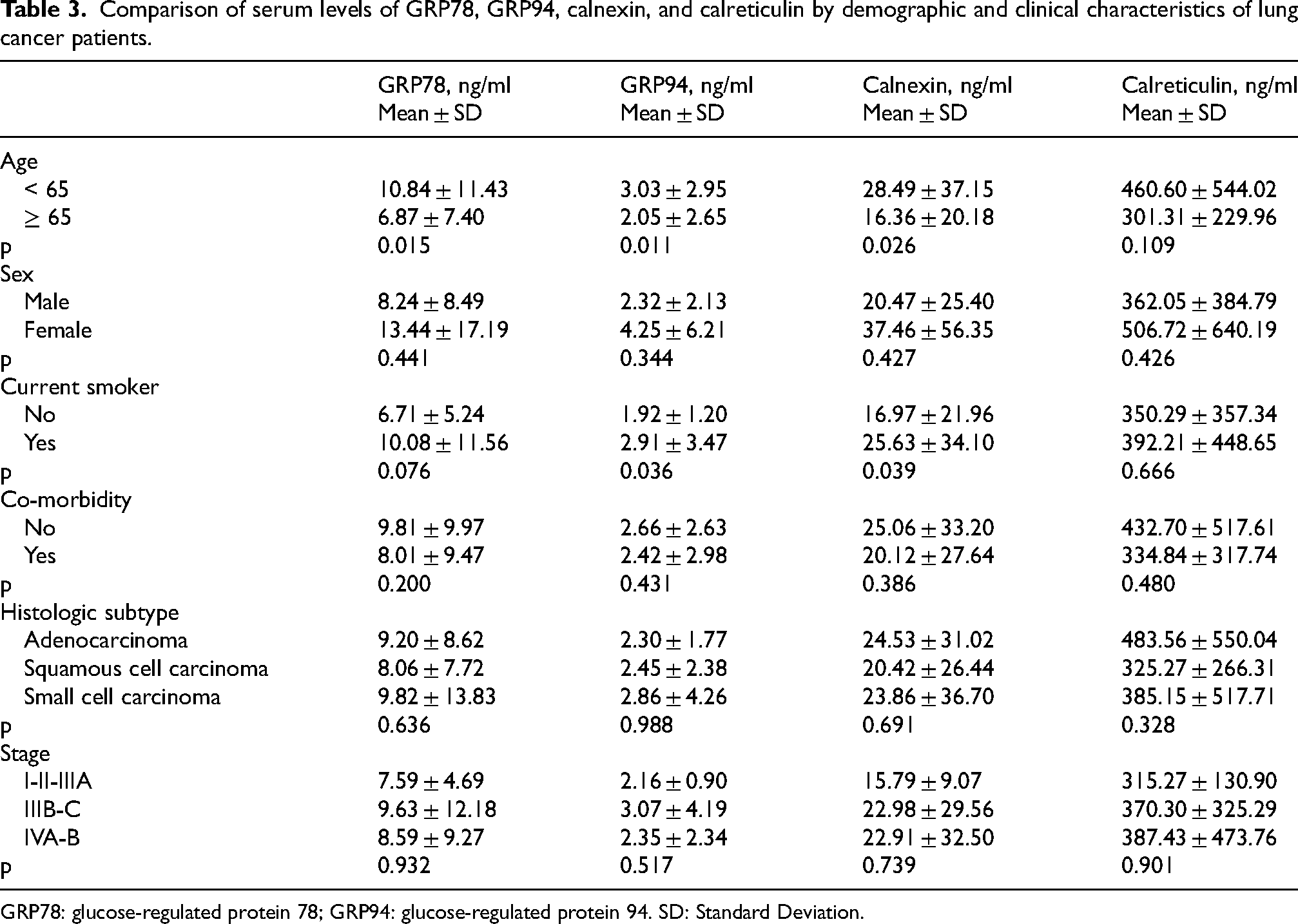
GRP78: glucose-regulated protein 78; GRP94: glucose-regulated protein 94. SD: Standard Deviation.
Serum levels of GRP78, GRP94 and calnexin were significantly higher in patients younger than 65 years (p = 0.015, p = 0.011 and p = 0.026, respectively), while the increase in calreticulin levels was not statistically significant (Table 3). Serum levels of GRP78, GRP94, calnexin and calreticulin were similar in both sexes.
Current smokers had significantly higher serum levels of GRP94 and calnexin than those who had never smoked or had quit smoking (p = 0.036 and p = 0.039, respectively). The increase in serum GRP78 and calreticulin was not statistically significant.
There was no significant difference between the serum levels of GRP78, GRP94, calnexin and calreticulin according to concomitant diseases, histologic subtypes and stages of patients with lung cancer.
The median survival time of patients with lung cancer was 11.0 ± 1.25 (95%CI: 8.54–13.46) months. A total of 26 patients were still alive at the end of the study. The mean follow-up time of surviving patients was 35.81 ± 12.42 months and the median follow-up time was 31.50 (26–75) months.
The relationship between serum levels of GRP78, GRP94, calnexin and calreticulin in patients with lung cancer and survival was evaluated. The results of the analysis based on the median values of the control group are shown in Table 4.
Comparison of survival of lung cancer patients according to serum levels of GRP78, GRP94, calnexin and calreticulin.
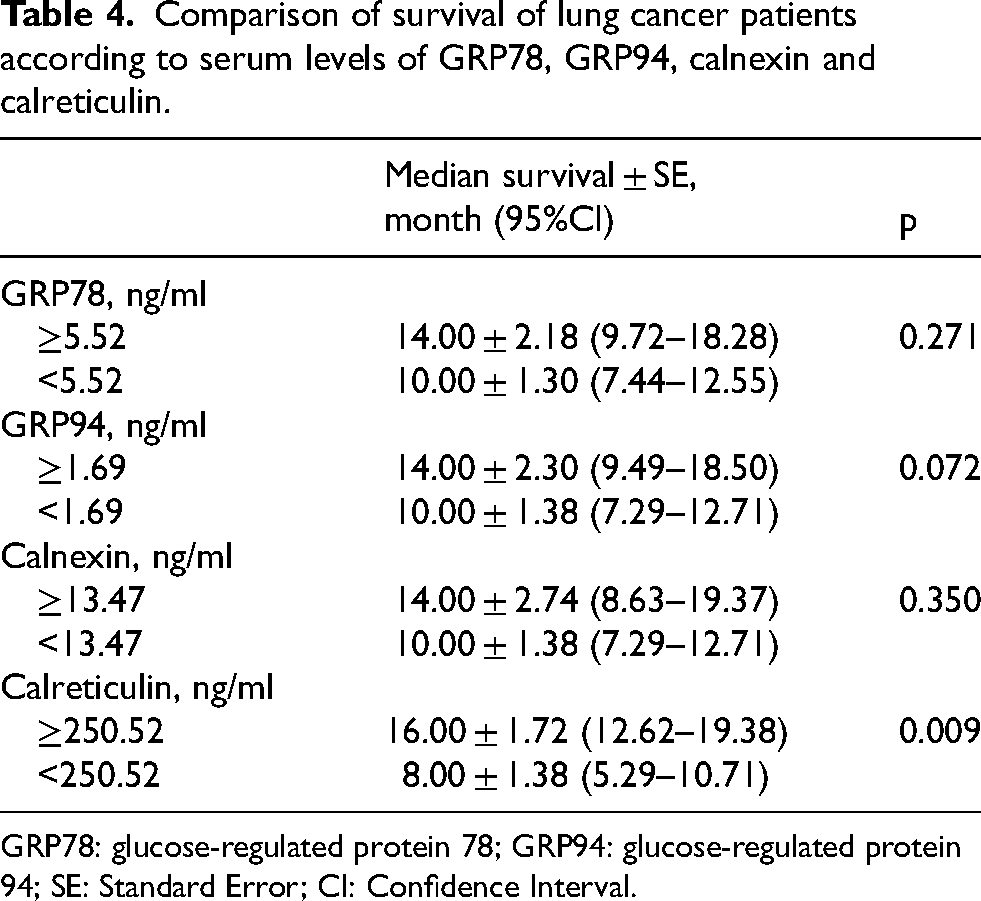
GRP78: glucose-regulated protein 78; GRP94: glucose-regulated protein 94; SE: Standard Error; CI: Confidence Interval.
Serum levels of GRP78, GRP94 and calnexin were not associated with survival. However, median survival ± SE (95%CI) was 16.00 ± 1.72 (12.62–19.38) months in patients with calreticulin serum levels of 250.52 ng/ml and above, while it was 8.00 ± 1.38 (5.29–10.71) months in patients with calreticulin levels below the cut-off value (log-rank = 6.919; p = 0.009) (Figure 2).
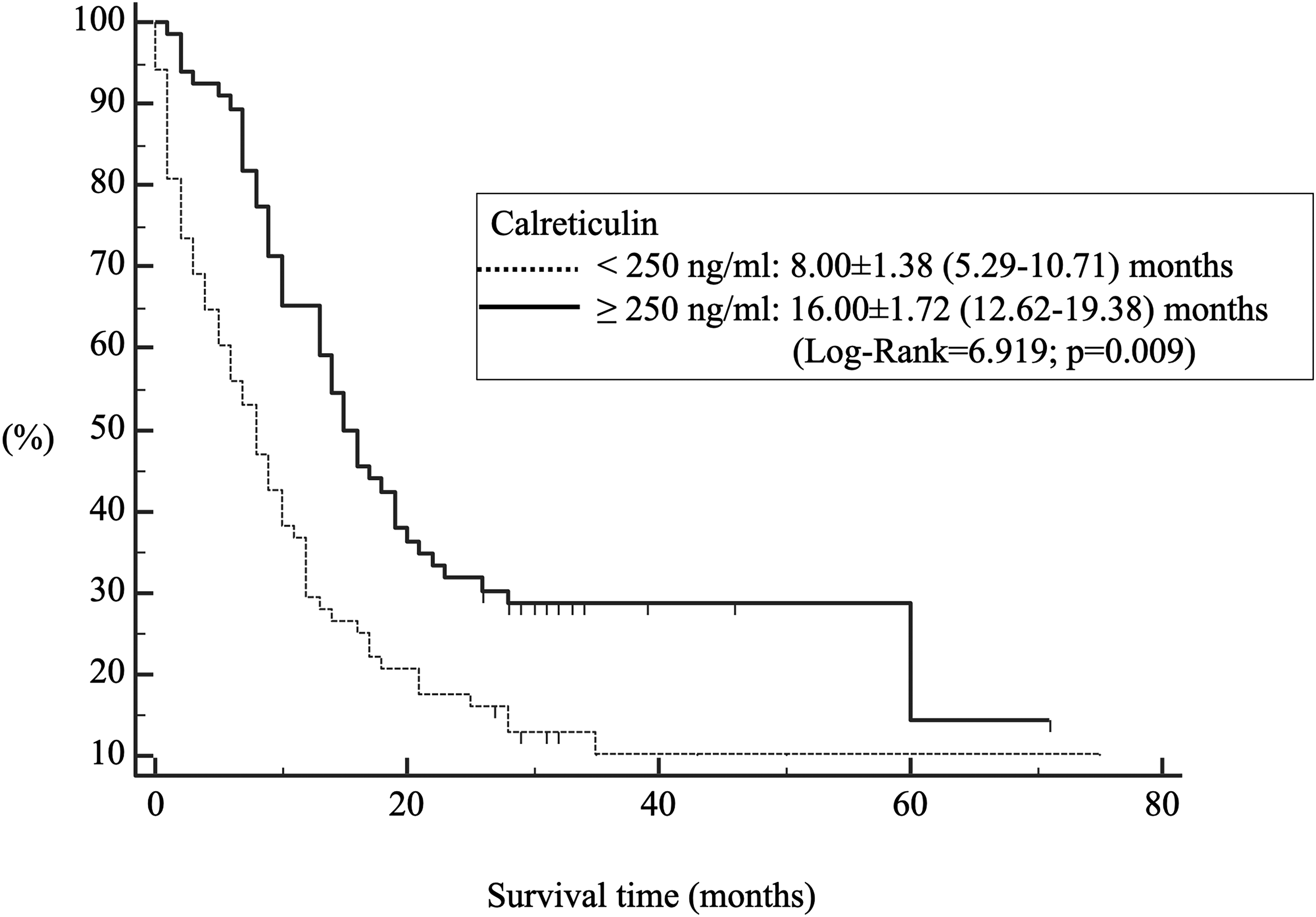
Kaplan-Meier survival curve according to serum calreticulin levels of patients with lung cancer.
The effect of calreticulin on survival was assessed by adjusting with a multivariable Cox regression analysis for sex, histologic subtype, stage, treatment, and response to chemotherapy, which are the variables that influence survival.
In the multivariate Cox analysis, female sex, stage IV patients and patients with small cell lung cancer had significantly higher mortality, while patients who responded to chemotherapy and had high calreticulin levels had significantly lower mortality. Calreticulin had an effect on survival, even after adjustment for variables affecting survival [HR (95%CI): 0.656 (0.433–0.995); p = 0.047] (Figure 3).
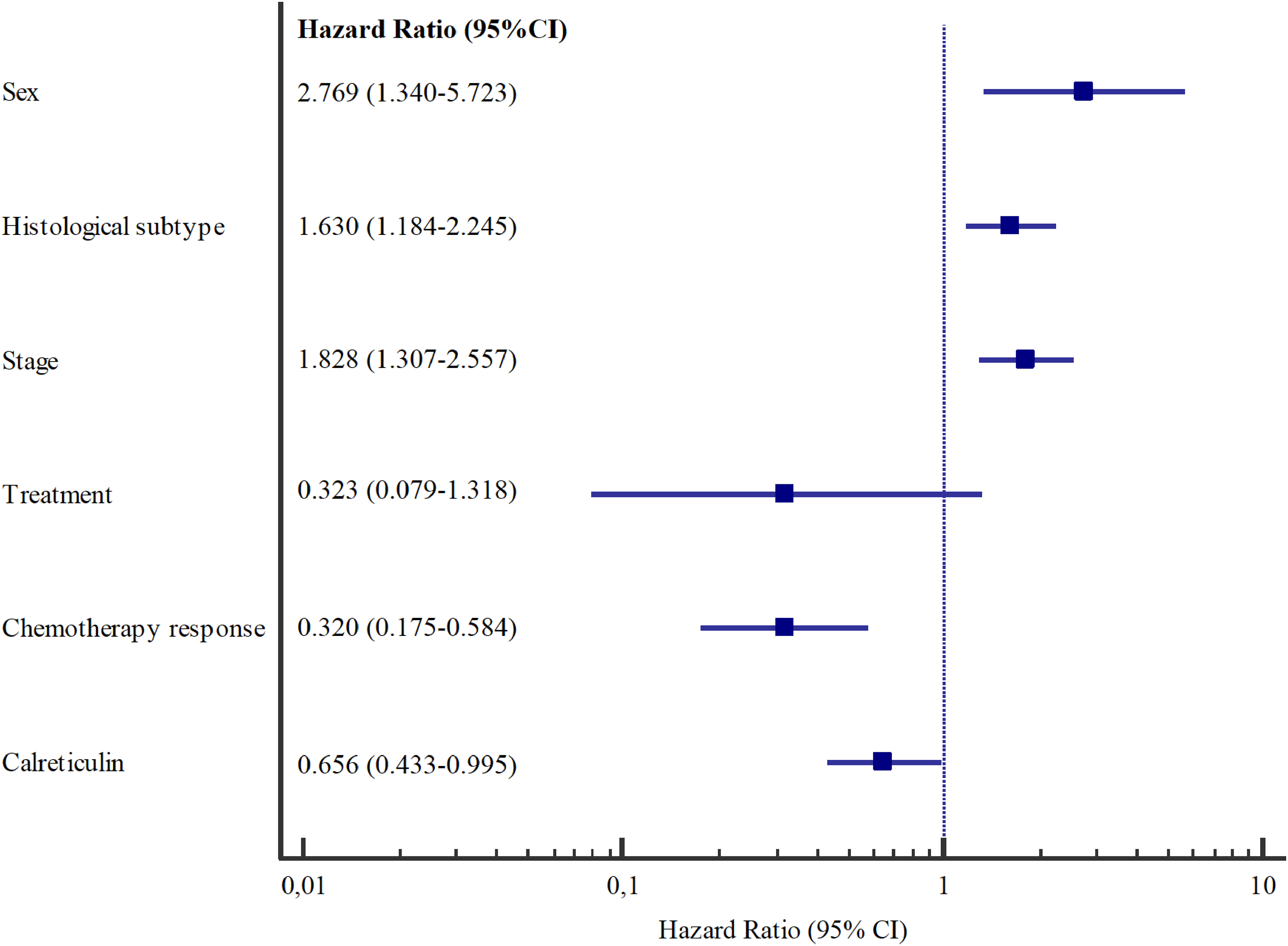
A forest plot showing the hazard ratio and 95% confidence intervals associated with variables considered in the multivariable analyses with survival time as the dependent variable. HR: Hazard Ratio; CI: Confidence Interval.
Discussion
We demonstrated that the serum levels of all ER chaperones GRP78, GRP94, calnexin and calreticulin were higher in lung cancer patients than in healthy subjects and correlated with each other. Regarding the association with demographic and clinical characteristics, we found that calreticulin serum levels were not influenced by demographic and clinical characteristics, that survival was better in patients with high calreticulin levels, and that this effect persisted after adjusting for factors influencing survival.
In recent years, there have been encouraging developments in the treatment of lung cancer. Unfortunately, despite all these developments, no significant improvements have been made in terms of ‘early diagnosis’ and ‘effective treatment’ that can prolong survival. As the majority of patients with lung cancer are diagnosed at a locally advanced/advanced stage, they have no chance of curative treatment. Screening studies with low-dose computed tomography continue in order to diagnose the disease at an early stage and treat it more effectively. However, in the studies on lung cancer screening with low-dose computed tomography, there are uncertainties regarding the “risk groups” and the “frequency and duration of screening”. 13 In addition, screening with low-dose computed tomography has disadvantages such as radiation exposure, false-positive results and high costs. A cost-effective screening program can be established by narrowing down the risk groups to be screened with molecular tests.14–16 On the other hand, efforts have been made in recent years to prolong the survival of lung cancer patients with treatments developed for molecular and immunologic mechanisms without compromising quality of life. However, only a minority of patients are suitable for these treatments. Research into new molecules that can predict the outcome of the disease and guide treatment is therefore being intensively pursued.
In our study, which is consistent with previous studies, serum levels of GRP94, calnexin and calreticulin were higher in patients with lung cancer than in the control group, in addition to GRP78, which has been extensively studied in the literature. These results suggest that chaperones may be useful in the diagnosis of patients with lung cancer.
The UPR is a signal transduction pathway that is activated when the cell is unable to maintain proteostasis within the ER. Depending on the tumor model, UPR activation has been shown to regulate cell survival, angiogenesis, inflammation, invasion, metastasis, and chemoresistance. 17
Previous studies have shown that ER chaperones are overexpressed in patients with lung cancer compared to control subjects.18–23 Wang et al. found that the mRNA and protein levels of GRP78 and GRP94 were overexpressed in tumor tissues from 54 patients who had undergone surgery compared with adjacent normal tissues, and their expression was stronger in poorly differentiated tumors. The authors noted that both chaperones could be useful for differential diagnosis and clinical follow-up. 18 Another study reported that the expression of GRP78 was higher in a larger group of patients than in normal tissue examined by immunohistochemistry. 19
Huang et al. investigated the role of GRP78 in the early detection of lung cancer. They determined the GRP78 level by ELISA in the plasma of 251 patients with lung cancer and 105 healthy controls and reported that the GRP78 level in the plasma of lung cancer patients was higher than in the control group. The sensitivity of GRP78 in distinguishing early-stage patients was 80% and the specificity was 69%. The authors commented that GRP78 could be used as a circulating biomarker for the early diagnosis of lung cancer. 20
Duan et al. investigated the role of GRP94 in the progression and prognosis of lung cancer. The authors first examined 13 data sets and analyzed GRP94 immunohistochemically in the tissues of 80 lung adenocarcinoma patients and the corresponding normal tissues according to the results obtained. The mRNA (encoded by HSP90B1) and protein levels of GRP94 were higher in lung adenocarcinomas compared to normal tissues. 21
Kobayashi et al. determined calnexin in their preliminary study to develop a serodiagnostic marker for lung cancer. After the initial phase, the researchers performed reverse-phase protein array analysis in samples from 195 lung cancer patients and 100 healthy controls. They showed that calnexin expression levels can distinguish lung cancer patients from healthy controls with a sensitivity of 99% and a specificity of 97%. Since calnexin is also detected in stage I disease, serum calnexin levels were interpreted as a marker that could be useful in the detection of early-stage lung cancer. 22
Liu et al. demonstrated that the level of soluble calreticulin in serum samples from 58 lung cancer patients was significantly higher than that of 40 healthy subjects using the chemiluminescent enzyme immunoassay system. 23 Immunohistochemical evaluation revealed that calreticulin expression is only present in trace amounts in normal lung cells, whereas calreticulin is highly expressed in both the membrane and cytoplasm of lung cancer cells. In their study, the researchers emphasized that the concentration of calreticulin in the serum of lung cancer patients is higher than that in the serum of healthy people, and that the expression level of calreticulin in the cell membrane of lung cancer is related to the pathological classification and grade of the tumor, and found that calreticulin can be used as a biomarker in lung cancer. 23
In our study, we investigated the association between age, sex, smoking, comorbidity, histopathological subtype and stage – factors that influence the treatment and clinical outcomes of patients with lung cancer – and ER chaperones. Serum levels of GRP78, GRP94 and calnexin were higher in patients younger than 65 years than in the 65 years and older group. The protein levels of GRP94 and calnexin were higher in current smokers. No association was found between other variables and chaperone levels. Calreticulin was not related to the demographic and clinical characteristics of the patients. This indicates that calreticulin could be effective for screening, treatment response and predicting prognosis in all lung cancer patients, which is discussed below.
Previous studies have shown that calreticulin is not influenced by demographic and clinical characteristics.24,25 In their study, Fucikova et al. found no association between age, sex, smoking history, histologic types and stage and calreticulin levels. 25 The fact that calreticulin levels are not influenced by age and smoking history, which are among the inclusion criteria in lung cancer screening studies, could be helpful in narrowing down the ‘risk group’ for radiological screening studies.
Most studies evaluating ER stress and UPR were conducted in surgical series and mostly included patients with early-stage NSCLC. In this sense, it is important that our study included patients with locally advanced/advanced stage and SCLC. In our study, we found no association between the stages of lung cancer patients and ER chaperones. In other words, the level of ER chaperones was not different in stages I- II-IIIA, which we can call early stage, from other stages. As Kobayashi et al. suggested, this was considered a promising result for screening studies.
In our study, we found a significant association between serum calreticulin levels and the survival of patients with lung cancer. Calreticulin was found to be an independent variable influencing survival after multiple regression analysis, including histopathologic subtype and response to chemotherapy, which are thought to influence patient survival.
The relationship between the ER chaperones GRP78, GRP94 and calnexin and prognosis has been the subject of numerous studies, the results of which are contradictory.21,26,27 However, calreticulin has been associated with a good prognosis in many studies.24,25,28
Fucikova et al. investigated the prognostic potential of calreticulin in two independent cohorts of patients with NSCLC. In the first case, they determined calreticulin levels in 270 patients with NSCLC by immunohistochemistry. Early-stage patients with high calreticulin levels had the best survival rate; conversely, advanced-stage patients with low calreticulin levels had the worst survival rate. On the other hand, advanced-stage disease with high calreticulin levels was more favorable than early-stage disease with low calreticulin levels. In the second phase, the authors confirmed the impact of calreticulin on survival in 125 stage III patients who received platinum-based neoadjuvant chemotherapy prior to surgery. Calreticulin levels in tumor cells were reported to correlate with EIF2a phosphorylation, which has a positive impact on clinical outcomes of NSCLC. The multivariate Cox model was performed in 395 patients considering both cohorts. Calreticulin, pathologic stage and age were found to be significant predictors of overall survival, independent of histopathologic subtype and chemotherapy. Higher expression of calreticulin in tumor cells was associated with a higher density of infiltrating mature DC and effector memory T cells. From this, the authors concluded that calreticulin triggers the activation of the adaptive immune response in the tumor microenvironment. Accordingly, patients with high calreticulin expression and extensive intratumoral infiltration by DC or CD8+ T lymphocytes were found to have the best prognosis. It was concluded that calreticulin expression could be a novel and useful prognostic biomarker reflecting an enhanced local antitumor immune response in the lung. 25
Another study showed that low expression of calreticulin in the tumor tissue of 88 NSCLC patients was associated with a poor overall survival rate. The 5-year survival rate was 12% in patients with low calreticulin levels and 35% in patients with high calreticulin levels. Stage and calreticulin-PDIA3 combination were found to be independent prognostic factors by Cox regression analysis. 24
It has been reported that calreticulin levels may also indicate response to antitumor treatment, and in some studies, calreticulin levels were higher in patients who responded to treatment.23,29 When tumor cells undergo immunogenic apoptosis, calreticulin is transported from the ER membrane to the cell surface. 30 Garg et al. reported that lung cancer patients with high levels of calreticulin responded better to radiotherapy and paclitaxel. 29 Yamamura et al. observed surface expression of calreticulin and HLA class I in cells treated with chemotherapeutic agents compared to untreated cells. The authors concluded that chemotherapeutic agents can enhance the immunogenicity of cancer cells in a cell-specific manner through the translocation mechanism of calreticulin. 28 In a recent study, Tsutsumi et al. investigated the relationship between response to treatment and levels of various DAMPs in patients with non-small cell lung cancer undergoing combination therapy of immune checkpoint inhibitors and chemotherapy. They showed a significant correlation between the maximum fold-change of CRT levels and progression-free survival. Median PFS and overall survival (OS) were higher in patients with a ≥ 2-fold increase in CRT plasma levels than in those with a < 2-fold increase (PFS, 14.9 versus 6.0 months; OS, not reached versus 21.6 months). They concluded that monitoring CRT plasma levels has the potential to predict the efficacy of an ICI combination. 31
The evaluation of our results together with the literature revealed that lung cancer survival can be determined by monitoring calreticulin. In addition, the signaling pathways in which calreticulin plays a role and related molecules could be used to develop potential targeted therapies.
In conclusion, one of the major findings of our study was that serum levels of GRP78, GRP94, calnexin and calreticulin were higher in lung cancer patients than in healthy volunteers, and there were no differences according to histopathologic subtype and stage that affected clinical outcome. Since calreticulin is not influenced by demographic and clinical data, it could be particularly useful to delineate risk groups for lung cancer screening studies. In addition, due to its positive effect on prognosis, calreticulin could be useful in the development of treatments for a larger patient population if targeted.
Footnotes
Acknowledgements
We thank all our patients.
Author contributions
Conception: G.A., S.M, M.M., H.V.G. Interpretation or analysis of data: G.A., S.M., H.V.G., D.T.C., H.K., S.Y., M.M. Preparation of the manuscript: G.A., S.M., M.M. Revision for important intellectual content: G.A., M.M., S.M. Supervision: S.M., M.M., H.V.G.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been supported by Eskisehir Osmangazi University Scientific Research Projects Coordination Unit under grant number 201946E04.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data for this study are available from the corresponding author upon request.