
Abstract
Guideline-recommended screening programs exist for only a few single-cancer types, and these cancers represent less than one-half of all new cancer cases diagnosed each year in the U.S. In addition, these “single-cancer” standard of care (SoC) screening tests vary in accuracy, adherence, and effectiveness, though all are generally understood to lead to reductions in cancer-related mortality. Recent advances in high-throughput technologies and machine learning have facilitated the development of blood-based multi-cancer early detection (MCED) tests. The opportunity for early detection of multiple cancers with a single blood test holds promise in addressing the current unmet need in cancer screening. By complementing existing SoC screening, MCED tests have the potential to detect a wide range of cancers at earlier stages when patients are asymptomatic, enabling more effective treatment options and improved cancer outcomes. MCED tests are positioned to be utilized as a complementary screening tool to improve screening adherence at the population level, to broaden screening availability for individuals who are not adherent with SoC screening programs, as well as for those who may harbor cancers that do not have SoC testing available. Published work to date has primarily focused on test performance relating to sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). MCED tests will require approval through the pre-market approval pathway from the United States Food and Drug Administration. Additional studies will be needed to demonstrate clinical utility (i.e., improvements in health outcomes) and establish optimal implementation strategies, (i.e., testing intervals), follow-up and logistics of shared decision making. Here, we propose core attributes of MCED testing for which clinical data are needed to ideally position MCED testing for widespread use in clinical practice.
Introduction
Single-cancer screening tests
Cancer is a major public health concern worldwide, and the burden of cancer incidence and mortality is rapidly growing. 1 It is the second leading cause of death in the U.S., and the primary cause of death in individuals less than 80 years old.2,3 The United States Preventive Services Taskforce (USPSTF) recommends (Grade A/B) routine screening methods for four cancer types: breast, colorectal, cervical, and lung. Breast, colorectal, and cervical screening tests are intended for average-risk populations and lung cancer screening is recommended for individuals at elevated risk due to smoked tobacco use.4–7 The majority of cancer-related deaths occur in cancer types for which no recommended screening exists, including pancreatic, prostate, liver, bladder, esophageal, kidney, uterine, ovarian, and gastric cancers.3 Even though guideline-recommended SoC screening has improved mortality rates for breast, colorectal, cervical and lung cancers,9–12 screening adherence remains below national target goals, 13 and is especially poor for lung cancer. 8 This gap is even more pronounced in members of racial and ethnic minorities due to barriers at individual, societal and economic levels.13,14
While delivering high sensitivity, current single organ screening tests have moderate specificity, generating a substantial burden of false positive (FP) results. False positive rates for a single round of a single-cancer SoC test range from 11.1% for mammography, 15 12.8% for low dose computerized tomography (CT), 16 13.4% for stool-based colorectal screening tests, 17 to 14.5% for the Papanicolaou test and up to 7.4% for hrHPV screening tests.11,18 Since the probability of obtaining a FP result increases with each round of single cancer SoC screening, 19 the cumulative lifetime FP risk for individuals receiving recommended screening is considerable. 20 However, FPs resulting from SoC screening have clearly defined pathways for FP resolution (e.g., colonoscopy to resolve FP stool-based tests and biopsies to resolve suspicious mammogram results).
Biologic basis for multi-cancer tests
Advancements in cancer biology, genomic measurement technologies, and machine learning create an opportunity to measure tumor-derived nucleic acid and protein biomarkers in biofluids, most commonly blood, at low concentrations.21,22 Blood-based tests have been developed using these innovative technologies to detect minimal residual disease and monitor treatment and therapy selection in patients with known cancer diagnoses.23–25 These methodologies have also been leveraged for their ability to detect biomarkers from multiple types of cancers simultaneously using a single test, collectively known as multi-cancer early detection (MCED) tests. Several emerging MCED tests are currently in development for clinical use (Exact Sciences Corporation, Madison, WI; GRAIL, LLC, Menlo Park, CA; Adela, Foster City, CA and Toronto, Canada; DELFI Diagnostics, Baltimore, MD; Freenome, South San Francisco, CA; Quantgene Inc., Santa Monica, CA; Burning Rock Biotech, Guangzhou, China; Singlera Genomics, La Jolla, CA; Geneseeq Technology Inc., Jiangsu, China; Dxcover Ltd., Glasgow, UK). To date, cell-free DNA (cfDNA), which is released into the bloodstream through cellular processes, 26 is the most widely investigated biomarker for MCED assay development. Many MCED tests utilize single biomarker classes, such as cfDNA methylation (GRAIL, Burning Rock Biotech, Singlera Genomics),27–34 mutations (Quantgene Inc.), 35 fragmentation patterns (DELFI Diagnostics, Geneseeq Technology Inc.),36–39 or proteins (Dxcover Ltd.) 40 to detect cancers, and in some cases, predict the cancer signal's origin. High level summaries of completed, ongoing, and planned MCED studies are provided in Table 1.
Completed, ongoing, and planned MCED studies.
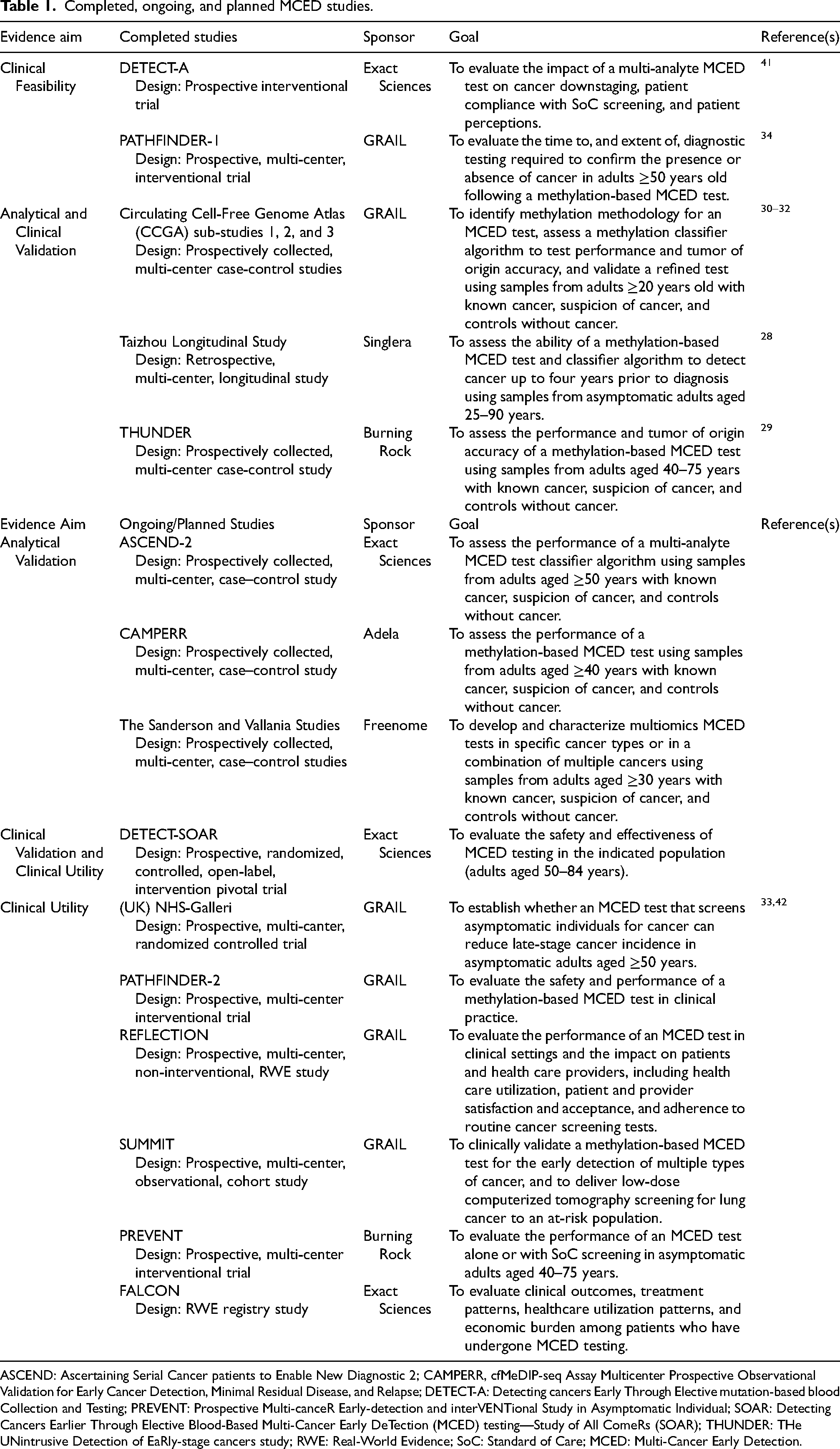
ASCEND: Ascertaining Serial Cancer patients to Enable New Diagnostic 2; CAMPERR, cfMeDIP-seq Assay Multicenter Prospective Observational Validation for Early Cancer Detection, Minimal Residual Disease, and Relapse; DETECT-A: Detecting cancers Early Through Elective mutation-based blood Collection and Testing; PREVENT: Prospective Multi-canceR Early-detection and interVENTional Study in Asymptomatic Individual; SOAR: Detecting Cancers Earlier Through Elective Blood-Based Multi-Cancer Early DeTection (MCED) testing—Study of All ComeRs (SOAR); THUNDER: THe UNintrusive Detection of EaRly-stage cancers study; RWE: Real-World Evidence; SoC: Standard of Care; MCED: Multi-Cancer Early Detection.
Clinical development of multi-cancer tests
GRAIL LLC's Galleri® test utilizes a single biomarker class, cfDNA methylation, to detect a shared cancer signal across a number of cancer types, while also predicting the source of this cancer signal. Galleri® was initially developed and validated in the case-control Circulating Cell-free Genome Atlas (CCGA) study (NCT02889978), 31 demonstrating an overall specificity of 99.5%. In addition to the case-control study, GRAIL LLC investigated the feasibility, safety, and perceptions of MCED testing for cancer screening by evaluating the Galleri® test in asymptomatic participants. The PATHFINDER study (NCT04241796), a prospective, interventional, single-arm trial, enrolled 6,622 average and elevated cancer risk participants across oncology and primary care outpatient clinics at seven U.S. health networks. The primary objective of PATHFINDER was to assess the extent of diagnostic testing needed to achieve diagnostic resolution (time to resolution, number/type of tests). Secondary endpoints included PPV, NPV, specificity, and cancer signal of origin accuracy.43–45 Median time to diagnostic resolution was 79 days in true-positive and 162 days in false-positive participants. Most participants had both laboratory tests (79% with true-positive results and 88% with false-positive results) and imaging (91% with true-positive results and 93% with false-positive results). 34 The overall PPV was 38%, NPV was 98.6%, specificity was 99.1%, and first cancer signal of origin prediction accuracy was 85% in true positive patients. 34 The PATHFINDER study was not specifically designed to assess the sensitivity or the breadth of cancer types detectable by the Galleri test. However, it is noteworthy that the study identified cancer types that currently lack standard screening methods. A number of cancer types were detected in the PATHFINDER study, including oropharyngeal, lung, breast, liver, intrahepatic bile duct, pancreas, small intestine, colon and rectum, uterus, ovary, prostate, bone cancers, lymphoma, Waldenstrom macroglobulinemia, lymphoid leukemia and plasma-cell myeloma. The ongoing PATHFINDER2 study (NCT05155605) is investigating test performance in a larger asymptomatic U.S. adult population.
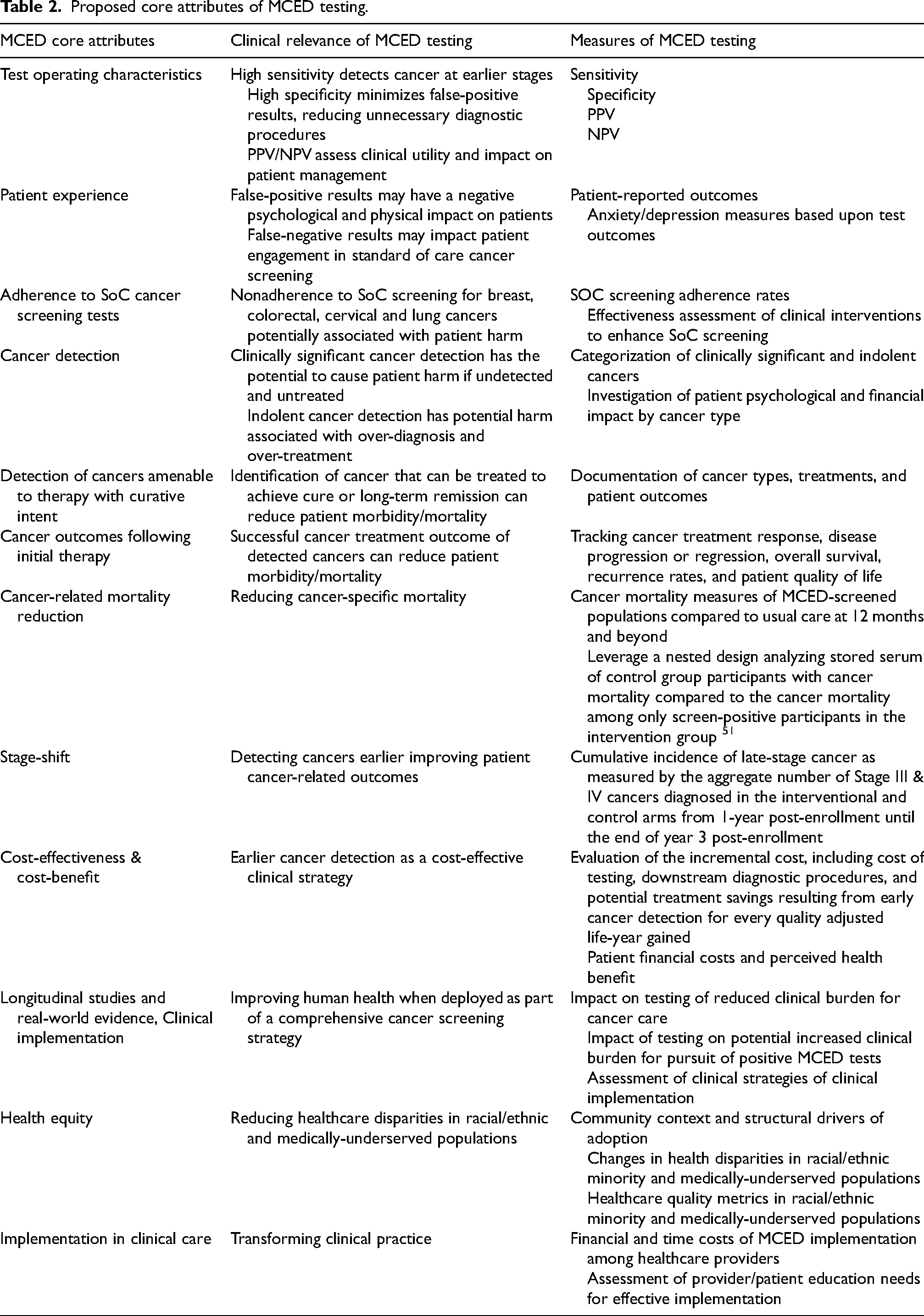
MCED tests incorporating multi-biomarker classes are also in development, including various combinations of fragmentations and methylation, with or without proteins (Freenome, Singlera Genomics),46,47 and cfDNA mutation, aneuploidy, and methylation biomarkers, together with cancer-associated protein quantification (Exact Sciences Corporation).41,48–50 The Detecting Cancers Earlier Through Elective Blood-Based Multi-Cancer Early DeTection (DETECT-A) study was the first prospective interventional trial to evaluate the feasibility and safety of an MCED blood test, enrolling 10,006 asymptomatic female participants with no known history of cancer. An early version of Exact Sciences’ MCED test (CancerSEEK) was used to detect a variety of cancer types, including cancers for which routine SoC screening modalities are not presently available. 41 In the DETECT-A study, CancerSEEK, together with diagnostic imaging, demonstrated an overall PPV of 40.6%, a NPV of 99.3%, and a specificity of 99.6%. 41 These results paved the way both for large case control studies evaluating new test versions and plans for additional studies. Here we propose core attributes of MCED tests that should be investigated to position MCED testing in clinical practice (Table 2 and Figure 1).
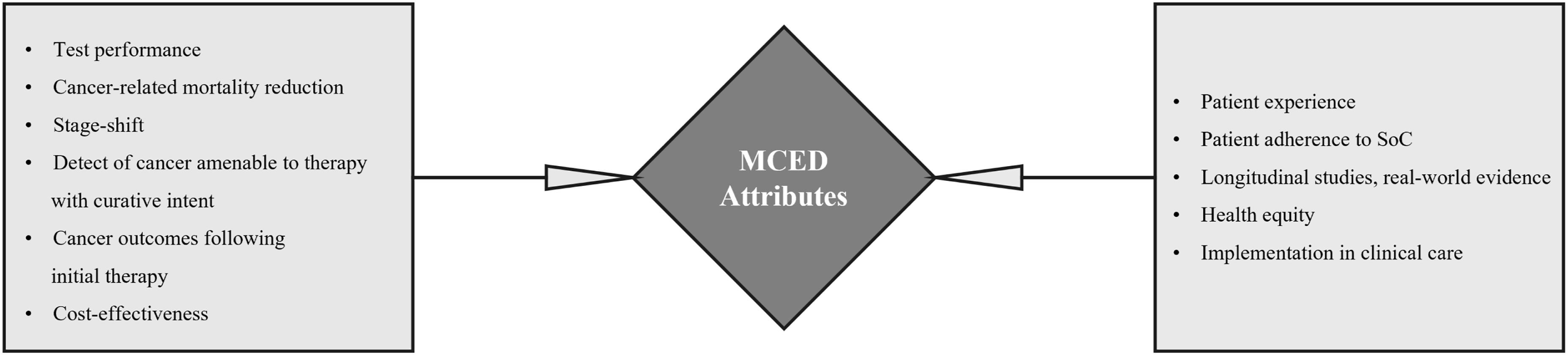
Core attributes of MCED testing illustration.
Proposed core attributes of MCED testing.
Test operating characteristics
MCED tests must balance sensitivity and specificity performance to provide optimal sensitivity for early cancer detection of many cancer types, while maintaining high specificity to minimize the risk of FP results. Like SoC screening tests, a positive MCED test result provides a suspicion of cancer signal that requires diagnostic workups to provide a definitive cancer diagnosis or rule out its presence. Unlike single cancer screening tests, MCED tests detect signals from multiple organ sites, and the diagnostic work-up after a positive MCED test may require a search for multiple cancer types. Thus, FP MCED results could trigger several follow-up diagnostic procedures that result in increased healthcare costs and, most importantly, may impose physical and psychological burdens on patients to definitively rule out cancer. MCED tests are being designed with high specificity to minimize the potential harms associated with FP results. Specificities of ≥99% were reported for both the PATHFINDER and DETECT-A studies, resulting in false positive rates of ≤1%.34,41 MCED tests may occasionally detect clinically significant pre-cancerous conditions amenable to intervention, although their sensitivity for such conditions appears limited to date. In the DETECT-A study, three pre-cancerous lesions were identified through positive CancerSEEK MCED. Subsequent imaging detected an ovarian mucinous cystadenoma, an appendiceal mucinous neoplasm, and colonic polyps with high-grade dysplasia. All three participants underwent successful surgery and remain cancer-free as of February 2023. 52
False negative results may also be considered as a potential harm inherently associated with all screening tests. False negative MCED test results are less concerning than false positive results, in that they do not trigger medical interventions, but some have raised concerns about false assurances that might lead individuals to forego proven single cancer screening tests. In the DETECT-A study, 70 cancers were diagnosed among 9,777 participants with negative test results (false negative rate of 0.72%), 41 and in the PATHFINDER study 86 cancers were diagnosed among 6,529 participants (false negative rate of 1.32%). 34 False negative risks may be mitigated by thoughtful interpretation of test results and bolstering clinician-patient education regarding the importance of adherence to SoC screening and annual physical exams. False negative results may be more common with MCED tests than the established, higher sensitivity single cancer tests However, the degree to which false negative MCED test results harm patients is not known. Ongoing and planned studies will evaluate adherence with SoC screening in MCED screening participants including those who received a negative result and help address this potential harm.
Patient experience and adherence to standard of care cancer screening tests
Low MCED FP rates reduce potential patient anxiety, limit unnecessary diagnostic workups, and control healthcare resource use and costs. MCED is complementary and additive to SoC screenings, however the tests are designed to detect, in aggregate, signals from cancers with and without SoC screening, as well as uncommon cancers. MCED tests with high specificity detecting cancers at an aggregate level would be expected to result in a higher cancer detection rate and PPV than is commonly seen with single cancer screening tests. 22 Studies of MCED tests should include monitoring of patient emotional and physical consequences of testing (e.g., morbidity associated with invasive diagnostics) to fully assess the risk/benefit of MCED testing. Implications of a negative MCED test result, such as continued engagement in unhealthy lifestyle choices, also require consideration.
MCED tests in development are intended to complement, not replace, SoC single cancer screening in asymptomatic individuals. Therefore, it will be imperative that negative MCED test findings do not steer participants away from continuing with established and recommended SoC cancer screening. Early preliminary evidence from a follow-up survey study of participants in the DETECT-A trial 41 was recently presented at the European Society of Clinical Oncology 2023 Congress. Survey results demonstrated that 3,820 of 3,870 (98.7%) DETECT-A participants who completed a survey expressed no change or a decrease in anxiety and depression as a result of DETECT-A participation. 53 Interestingly, participants with FP results were significantly more likely than participants with true negative results to report a decrease in anxiety resulting from study participation; 22.9% of FP respondents versus 7.7% of true negative respondents (p = 0.005) and were no more likely to report an increase in anxiety [5.7% of FP respondents versus 1.3% of true negative respondents (p = 0.07)]. Additional, prospectively collected anxiety data will be needed to fully understand the psychological impact of MCED testing and such studies are expected.
Similarly, PATHFINDER participant-reported data on anxiety, distress, uncertainty, and satisfaction with the Galleri® MCED test were presented at the European Society of Medical Oncology 2022 Congress. Although participant-reported distress and anxiety scores were low, participants with positive MCED test results reported greater distress and uncertainty upon receiving their test results compared to those with negative test results. Distress and uncertainty levels approached baseline levels by the end of study timepoint for participants with TP as well as FP results. Overall, high rates of satisfaction were reported with MCED testing irrespective of test result. 54
The DETECT-A survey results described above also revealed high levels of participant satisfaction and adherence to SoC screening. Amongst survey respondents eligible for mammography with available health records, 93.4% (n = 984) were adherent with mammography screening. 53 This survey is limited because is presents data on a subset of highly motivated study participants who voluntarily agreed to contribute to an extension study and were queried about their experience after a considerable amount of time had passed.
Cancer detection
Ideal clinical cancer screening programs maximize detection of clinically significant cancers and minimize over-diagnosis. Clinically significant cancers are those for which timely intervention improves patient outcomes. “Clinically insignificant” or “indolent” cancers are not universally understood nor defined, but in general, represent cancers that are usually small, slow growing, localized, and unlikely to significantly affect the patient's quality of life or lifespan. 55 Overdiagnosis is expected to be minimal for MCED testing, as DNA biomarkers appear to be released into the bloodstream preferentially by more aggressive and/or larger cancers 56 ; however, data obtained from future clinical studies will provide more information. Observation or active surveillance may be the initially recommended approach for such indolent cancers as earlier than necessary treatment may cause more harm than benefit by exposing patients to complications of unnecessary diagnostic procedures and treatments. Patients diagnosed with indolent cancer may also experience psychological harm from this new knowledge and negative financial impact through prospective monitoring for cancer progression. Measurement of the psychological and financial impact on patients of MCED diagnosis of clinically significant and indolent cancers will be important for understanding the impact of MCED screening when deployed in clinical practice.
Detection of cancers amenable to therapy with curative intent & cancer outcomes following initial therapy
Early cancer detection seeks to facilitate early and effective therapies. Although limited, data are emerging regarding outcomes following positive MCED test results. In the DETECT-A trial, 26 cancers were first identified by MCED testing (CancerSEEK), including six cancer types with no guideline-recommended screening (ovarian, thyroid, uterine, appendiceal, lymphoma, and kidney). Seventeen (65%) of the 26 cancers were localized or regional, including five participants with Stage I tumors, four with Stage II tumors, and eight with Stage III disease. 41 At a median follow up of 8.4 months following definitive diagnosis, 11 patients were in remission and 9 were undergoing treatment or had stable disease. 41 A follow up analysis at a median follow-up period of 4.4 years following DETECT-A study enrollment reported 13 of the identified 26 (50%) cancer-bearing participants were alive and cancer-free [ovarian (4), thyroid (1), uterus (2), breast (1), colorectal (2), and lung (3)]. All 8 treated stage I or II participants (8/8, 100%) and 12/14 (86%) surgically-treated participants were alive and cancer-free. 57 Additionally, within 12 months post-enrolment, 35 true positive cancers (28 had a new cancer, 6 had recurrent cancer, and 1 had both) were first detected by a positive MCED test in GRAIL's PATHFINDER study. Fourteen (48%) of the 29 new cancer cases were stage I–II, including 6 solid tumors and 8 hematological malignancies. GRAIL's MCED test identified cancers that do not have SoC screening in 26 (74%) of the 35 participants with true positive results. 34
Cancer-specific mortality reduction
Cancer-specific mortality reductions have been observed in screening trials for some, but not all, cancers. In the European Randomized Study of Screening for Prostate Cancer (ERSPC) trial, the cumulative incidence of advanced stage cancer was reduced by 48%, resulting in a 21% prostate cancer mortality reduction. 58 Similar results were reported from the National Lung Screening Trial (20% reduction in lung cancer mortality), 59 the UK Age Trial (17% reduction in breast cancer mortality), 60 and the Nurses’ Health Study/Health Professionals Follow-up Study (46% reduction in colorectal cancer mortality). 61
However, in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS) trial, a reduction in stage III or IV disease incidence did not translate into a mortality reduction. 62 The reasons for the failure of UKCTOCS to demonstrate a mortality benefit are not known. Potential contributors may include insufficient magnitude of “stage-shift” (i.e., detection at earlier stages) and/or insufficient efficacy of earlier interventions. The ability of stage-shift to serve as a surrogate for mortality reduction across a variety of cancers has recently been estimated in modeling studies. Using Surveillance, Epidemiology, and End Results (SEER) data for 17 cancer types, Clarke et al. projected a 15% reduction in cancer-related deaths would occur if all stage IV cancers were diagnosed at stage III. Assuming one third of metastatic cancers were diagnosed at stage III, one third diagnosed at stage II, and one third diagnosed at stage I, all cancer-related deaths would be reduced by 24%. 63
Mortality reduction given a specified stage-shift may vary across cancers. For example, a modeling study conducted by Owens et al. concluded that stage-shift does not appear to be a reliable basis for inference about mortality reduction across bladder, liver, lung, lymphoma, ovary, pancreas and stomach cancers. 64 Results of such analyses also depend on the quality of the data used in the models, the degree of stage-shift that a screening test may produce, the efficacy of earlier intervention when compared to later intervention in each cancer type, and the modeling methodology used. Hubbell et al., built upon single cancer models by implementing an interception (or state transition) model to understand the potential public health effects of adding a MCED test to standard cancer screening processes. 65 The model utilized published SEER incidence and 5-year survival data, MCED performance data across cancer types and stages, various cancer growth rate assumptions and multiple screening schedules to predict potential mortality benefit from stage-shift. When modeling for maximum benefit, 41% of all cancers would be intercepted by a MCED test; the remainder would be detected by SoC. Even the most aggressive growth rate scenario reduces deaths by 74 per 100,000, for a 19% relative mortality reduction in all-cancer mortality. Across all scenarios, this model predicted that MCED testing could substantially reduce overall cancer mortality if added to usual care. 65
Stage-shift
Stage-shift has been proposed and used as an early outcome measure that may predict the change in cancer mortality.66,67 Reduction in advanced stage disease may translate into a reduction in mortality from cancer and substantial cost savings among Medicare, Medicaid, TRICARE, CHAMPVA and commercially insured populations.68,69 While stage-shift and mortality outcomes have been studied in the context of single cancer screening programs, it is not known how well stage-shift predicts the impact of screening on mortality across the wide variety of cancers potentially detectable by MCED tests. The detection of a relationship between stage-shift and cancer-specific mortality requires that MCED studies include stage and mortality data. In order to demonstrate clinical utility, MCED tests must demonstrate utility in shifting cancer diagnoses to earlier stages. For earlier detected cancers, effective early interventions must be available and treatment must improve outcomes compared to patients whose cancers are detected without MCED testing. Modeling analyses combining data from multiple single cancer screening trials into a single analysis may enable us to estimate the potential impact of MCED testing on mortality.
Cost-effectiveness
MCED testing might increase detection of cancer at early stages, when survival outcomes are better and treatment costs are lower but may also increase diagnostic testing costs. Modeling studies can estimate the potential health benefits and harms, and economic consequences of MCED testing; approaches and considerations for such analyses have been outlined. 70 A quantitative framework for estimating potential benefits and harms of MCED has been proposed by Jiao, et al.. 71 The authors concluded that the potential population impact of MCED testing depends on the test characteristics, the cancers detected, as well as the efficacy of early treatment. Additional analyses are needed to fully understand the harm–benefit tradeoffs of MCED testing and how to utilize MCED tests to reduce the population cancer burden. In addition, a suggested framework has been developed illustrating decision modeling strategies that could be employed to predict the resulting effects on quality-adjusted life-years (QALYs) and medical care costs. The analysis conducted using modeling data yielded promising results for MCED testing which indicated that MCED testing is cost-effective, with an Incremental Cost-Effectiveness Ratio (ICER) of $22,494 per Quality-Adjusted Life Year (QALY). 72 This is well below the commonly accepted threshold value for decision makers’ willingness to pay for a QALY, set at $100,000. 72
A comprehensive, cutting-edge examination of cost-effectiveness would advance understanding about the impact of MCED testing on patient total cost-of-care if deployed across clinical practices. 72 Investigations of healthcare resource utilization can be built on modeling studies evaluating MCED testing in average-risk populations,63,65 patients with clinical risk factors for cancer such as smoking use and obesity, 73 and U.S. population subgroups defined by race/ethnicity and sex. 74 Additional analyses as more data becomes available from MCED testing implemented in the intended use population will further refine our estimates of the economic impact of MCED testing.
In addition to cost-effectiveness from a healthcare system perspective, measurement of patient costs and benefits could be considered. Costs related to out-of-pocket expenses, work absenteeism and presenteeism could be measured along with patient perceived health benefit of the testing specifically as it relates to earlier detection of cancer and management or reassurance that they do not have detectable cancer.
Longitudinal studies and real-world evidence, clinical implementation
Real-world evidence studies will test implementation, performance, and outcomes (including clinical validity and utility), as well as potential future uses for MCED-based screening and diagnostic tests. Utilizing real-world data (RWD) from real-world evidence studies offers several advantages compared to traditional methods. RWD studies have the potential to furnish extensive data over an extended follow-up period, allowing for the examination of long-term outcomes across a substantial sample of individuals in the target population, including those with rare cancers. Moreover, RWD offers insights into real-world scenarios, shedding light on factors such as diagnosis rates, screening frequencies, adherence, and evolving treatment patterns. 75 For future considerations, surveillance systems with the ability to aggregate data about clinical implementation of MCED testing would enhance our understanding of “best practice” implementation and optimization of clinical workflows.
Health equity
Disparities in SoC cancer screening and adherence exist for racial and ethnic minority groups and other medically underserved populations. Race/ethnicity, geographic location, education level, income, disability status, and access to insurance/healthcare influence screening adoption and SoC adherence over time.14,76 A recent modeling study using data from 2006 to 2015 observed a 3-fold difference in the rate of stage IV cancer between groups with the highest (non-Hispanic Black males) and lowest (non-Hispanic Asian/Pacific Islander females) incidence rates. 74 If all stage IV cancers were detected at stage III, an estimated 13%–14% fewer cancer-related deaths would occur. If one-third of metastatic cancers were diagnosed at each earlier stage (I, II, and III), a 21%–23% relative reduction in deaths has been estimated to occur. The model predicted that non-Hispanic Black males would benefit the most from improved cancer detection before metastasis, but it could reduce deaths across all populations. Deliberate, proactive efforts will need to be made to ensure access, knowledge, and trust in MCED tests among health care providers and all segments of the U.S. population. In addition, modelling and measurement of MCED adoption, changes in healthcare disparities and healthcare quality metrics in all underserved groups will be essential.
Implementation in clinical care
One consideration for the incorporation of MCED testing into clinical practice involves the diagnostic evaluation strategy following a positive MCED test result. Like all cancer screening tests, an abnormal MCED test requires a diagnostic work-up to rule in or rule out cancer. MCED tests also require localization of the suspected tumor. The optimal diagnostic strategy should be safe, widely accessible, and efficient, limiting unnecessary procedures, patient harm, and delivering timely diagnostic resolution. To date, prospective MCED studies have utilized two differing diagnostic resolution strategies.
The PATHFINDER study utilized molecular data obtained through MCED testing to predict the potential tissue of origin (TOO) of the suspected tumor. The DETECT-A study used an MCED test (CancerSEEK) to detect a suspected cancer and subsequent diagnostic imaging flourine-18 fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET-CT) to confirm and identify the location (TOO) of the suspected tumor. A key challenge in the clinical use of MCED testing is determining the best approach for diagnostic follow-up after a positive result. A clinical algorithm for diagnostic resolution through imaging following an MCED test is proposed for tests not returning information on the TOO from which the cancer signal originates has been proposed by Kiesel et al. 77 While these approaches need to be investigated and validated in future prospective studies, a recent modeling study characterized the diagnostic burden of both strategies. The model incorporated positive predictive value, molecular TOO localization accuracy, and numbers of procedures associated with each diagnostic outcome based on clinical guidelines. 78 Across all PPVs and localization performances, a molecular TOO prediction strategy resulted in a higher diagnostic burden compared to the imaging-based strategy (3.6 procedures vs 2.6 procedures, respectively). The estimated diagnostic burden was higher for a molecular-based TOO approach in 95.5% of all PPVs and TOO localization accuracy scenarios. The potential efficiency of an imaging-based diagnostic strategy is primarily driven by the diagnostic procedures needed to resolve a FP MCED result.
While MCED tests may offer long-term cost savings, initial investment costs for healthcare systems, including technology, training, and infrastructure, may be required. Introducing MCED testing as a routine part of cancer screening will require provider time to manage shared decision-making with patients. Providers and patients will require education to interpret MCED test results and manage diagnostic follow-up care. Physicians and practices may benefit from having access to shared decision-making tools and guidance for diagnostic workups of positive test results. Healthcare providers may be uncomfortable with FP results until additional data from larger cohorts, collected over longer intervals, becomes available. Measurement of burdens and benefits of clinical implementation on providers and systems will assist test developers in developing “best practices” for MCED dissemination.
Current and planned trials
Randomized controlled trials (RCTs) offer the highest quality of evidence of clinical utility. GRAIL's randomized controlled trial, NHS-Galleri (ISRCTN91431511),
33
is evaluating the impact of MCED testing on the incidence of late-stage cancer in asymptomatic individuals who are not currently under investigation for suspected cancer. Long-term follow-up utilizing interconnected databases may enable researchers to explore the test's impact on cancer-specific mortality rates. Exact Sciences plans to conduct a randomized controlled screening trial to evaluate the safety and effectiveness of its MCED test. The
Conclusion
Multi-cancer early detection tests have the potential to revolutionize cancer screening by offering a single blood test capable of detecting multiple types of cancer. By complementing existing single-cancer screening approaches, MCED tests have the potential to detect a wide range of cancers at earlier stages when patients are asymptomatic, enabling more effective treatment options and the potential for reduced morbidity and mortality. 2 MCED tests could serve as effective screening tools for the general population, broadening screening availability to more cancer types and facilitating access and adherence with screening recommendations. The development of MCED tests will require a wide variety of evidence, from randomized controlled trials and observational studies to real-world evidence, to establish clinical utility, and evaluate the implementation and economic impact of these tests. The Multicancer Early Detection Consortium Clinical Utility Working Group has developed a framework outlining strategies that should be adopted for successful MCED test evidence development. 79 Similar frameworks are being developed by the BLOODPAC Consortium's Early Cancer Detection and Screening Working Group with primary objectives which include the development of a common lexicon and the establishment of standardized frameworks for evidence development pertaining to innovative blood-based technologies, with the aim of fostering consensus within the field. 80
Footnotes
Abbreviations
Acknowledgements
The authors would like to thank Michelle Beidelschies, Xiting Cao, Stephen Eckert, Lindsay Houff, Angana Kharge, Nancy Nazmi, and Jessica Profato-Partlow (Exact Sciences Corporation, Madison, WI) for their contributions and review of this manuscript. Writing and editorial assistance was provided by Carolyn Hall and Feyza Sancar (Exact Sciences Corporation, Madison, WI). Exact Sciences provided support for this manuscript.
Author contributions
Conception: Seema P. Rego. Interpretation or analysis of data: Jon O. Ebbert, Ernest T. Hawk, Christopher V. Chambers, Margaret A. Tempero, Elliot K. Fishman, Jospeh E. Ravenell, Tomasz M. Beer, Seema P. Rego. Preparation of the manuscript: Jon O. Ebbert, Ernest T. Hawk, Christopher V. Chambers, Margaret A. Tempero, Elliot K. Fishman, Jospeh E. Ravenell, Tomasz M. Beer, Seema P. Rego. Revision for important intellectual content: Jon O. Ebbert, Ernest T. Hawk, Christopher V. Chambers, Margaret A. Tempero, Elliot K. Fishman, Jospeh E. Ravenell, Tomasz M. Beer, Seema P. Rego. Supervision: Tomasz M. Beer.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article from Exact Sciences Corporation.
Declaration of conflicting interests
![]()