
Abstract
Purpose:
The simultaneous and ipsilateral occurrence of medial epicondylar and radial neck fractures is rare. This study evaluated the clinical and radiological outcomes of medial to lateral diagonal injury of the elbow (MELAINE).
Methods:
Six males and 6 females were diagnosed with MELAINE (left: 10, 83.3%; right: 2, 16.7%). Medial epicondylar and radial neck fractures were classified according to Papavasiliou’s classification (seven type II, two type III, three type IV) and Judet’s classification (three type I, four type II and five type III), respectively. All patients underwent surgery. The carrying angle, range of motion, and Kim et al. Elbow Performance Score were used to evaluate clinical and functional outcomes; related complications were recorded.
Results:
Mean age at injury and mean follow-up were 11.1 ± 2.5 (range, 6–14) and 40 ± 25.6 months (range, 13–90), respectively. All fractures consolidated in 6.3 ± 1.2 weeks on average (4–9). Outcomes were good (n = 1; 8.3%) to excellent (n = 11; 91.7%). The carrying angle of the injured and uninjured side was 15.5°± 2.6° and 14.7°± 2°, respectively (p = 0.218). The range of motion of elbow flexion-extension and forearm pronation-supination of the injured side was 144.2°± 10.4°, 4.6°± 5.4°, 76.7°± 9.1°, 80.4°± 9.2°, respectively, with no significant differences from the healthy side (p > 0.05). The Elbow Performance Score of the injured and uninjured side was 96.3 ± 5.3 and 98.8 ± 2.3, respectively (p = 0.139). No cases of infection, cubitus valgus, stiffness, or instability were recorded.
Conclusion:
Although uncommon, MELAINE should not be neglected. Surgery aims to stabilize the elbow and avoid valgus deformity. If diagnosed and treated, clinical and radiological results are excellent in most cases.
Introduction
Fractures of the medial epicondyle (MEP) and radial neck (RN) are relatively frequent injuries in children, representing 11%–20% and 5%–10% of pediatric fractures, respectively.1,2
However, the simultaneous and ipsilateral occurrence of these two lesions is unknown, and very few cases are available in the literature. In particular, the rare publications reporting the association between MEP and RN fractures in children are mostly case reports in high-energy trauma.3 –5
Considering the fact that the MEP and radial head and neck are proximal and medial and distal and lateral to the elbow joint, respectively, it is possible that a forced valgus mechanism, with the elbow in hyperextension, may be responsible for this type of injury. Specifically, forced valgus would induce MEP detachment due to traction of the flexor-pronator muscles1,6,7 and injury to the RN by the capitellum compressing the radial head,2,8 leading to a medial to lateral diagonal injury of the elbow (MELAINE). A similar pathogenetic mechanism has been described by Li et al. 9 in the adult knee for the so-called “diagonal lesion” of the knee.
The purpose of this study was to evaluate the clinical and radiological outcomes of children with a MELAINE lesion and to explore the pathogenetic mechanism of such lesions in the pediatric population.
Materials and methods
This study was approved by the Institutional Review Board (IRB) of our institution (No. 2022213). Following IRB approval, we retrospectively reviewed medical records to identify children and adolescents who presented to the Emergency Department (ED) of our institution for MELAINE injury from February 2015 to August 2021.
The inclusion criteria were as follows: (1) age < 14 years; (2) acute injury of the elbow; (3) diagnosis of ipsilateral MEP and RN fractures (MELAINE lesion) diagnosed on plain radiographs, computed tomography (CT) scans, or magnetic resonance imaging (MRI); (4) follow-up > 1 year; and (5) complete clinical and radiographic data. Exclusion criteria were (1) pathological or open fractures; (2) follow-up < 1 year; and (3) incomplete clinical and radiographic data.
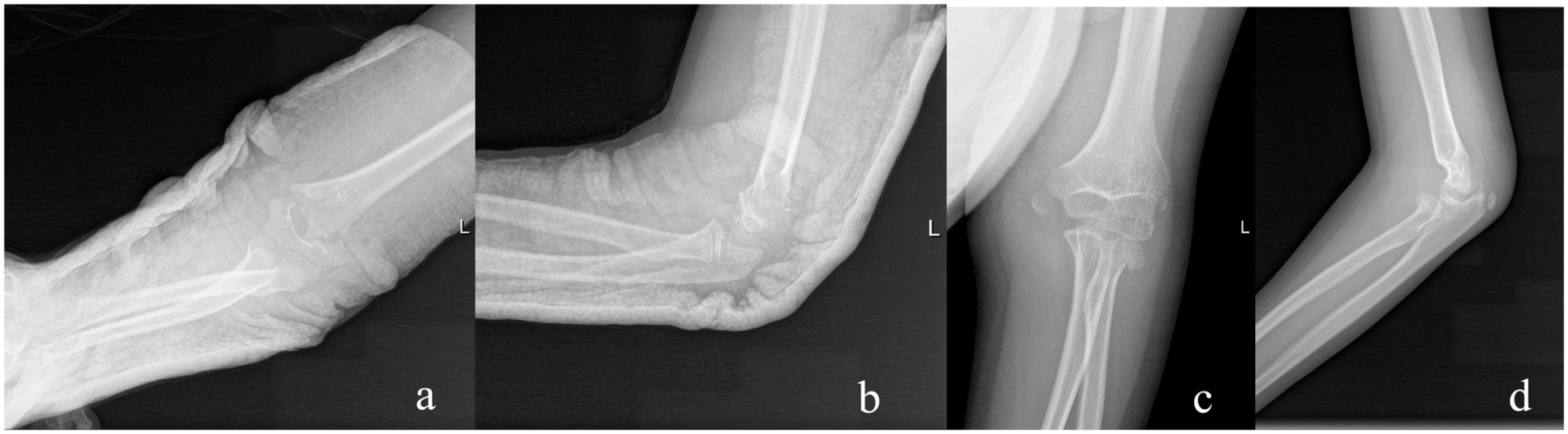
During the study period, we identified 173 cases with a MEP fracture and 258 cases with a RN fracture. In 6.9% of cases, MEP fracture was associated with RN fracture and in 4.7% of cases, RN fracture was associated with MEP fracture. Overall, ipsilateral MEP and RN fractures were identified in 12 of 419 patients (2.9%; 6 males and 6 females) and were considered as MELAINE-type injuries (Figure 1, Case 6). The patients were consecutive and all fractures were managed in one institution by the same surgical team.
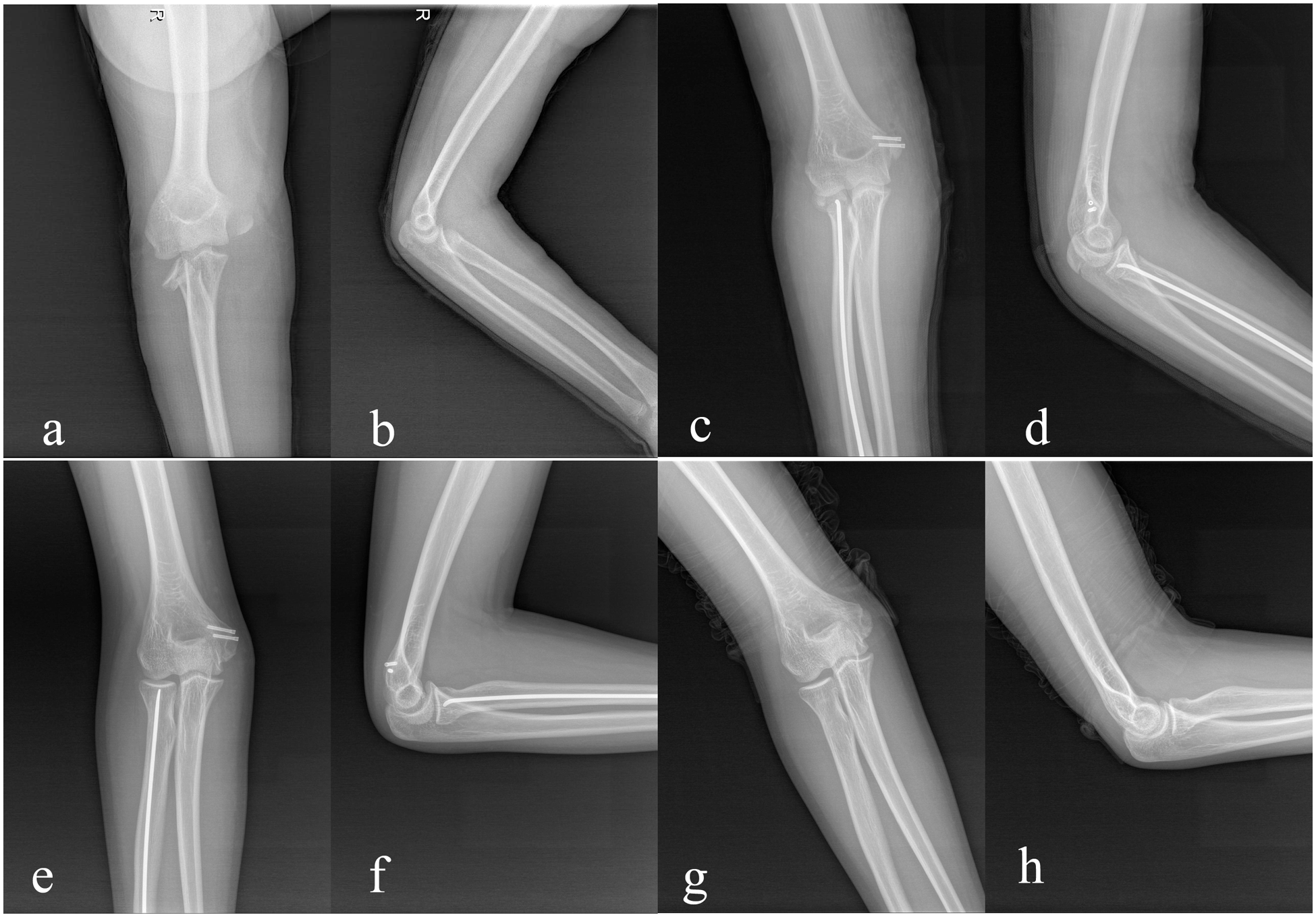
Case 6: A 13-year-old boy with a MELAINE lesion of the right elbow: (a, b) type II MEP fracture and type III RN fracture; (c, d) postoperative radiographs; (e, f) outcome; and (g, h) hardware removal.
The mean age at injury was 11.1 ± 2.5 years (range, 6–14); 10 fractures involved the left side (83.3%) and 2 (16.7%) involved the right side.
The traumatic mechanism was falling in six patients (50%), falling during sport in four patients (33.3%), and falling from a height in two patients (16.7%). The time from injury to surgical treatment was 3.8 ± 3.4 days (range, 1–12).
The MEP fractures were classified according to Papavasiliou’s classification 10 : type I, no or slight displacement; type II, avulsion fracture at the joint level but not trapped in the joint; type III, avulsion fracture trapped in the joint; and type IV, avulsion fracture associated with elbow dislocation. There were seven cases of type II (58.3%), two cases of type III (16.7%), and three cases of type IV MEP fractures (25%).
The RN fractures were classified according to the system described by Judet et al. 11 : type I, no displacement; type II, <30° angulation and <50% displacement; type III, 30°–60° angulation and <100% displacement; and type IV, 60°–90° angulation and >100% displacement. There were three cases of type I (25%), four cases of type II (33.3%), and five cases of type III RN fractures (41.7%). Two cases of type I RN fracture could not be diagnosed on plain radiographs but were later confirmed by CT scan (Figure 2, Case 4).
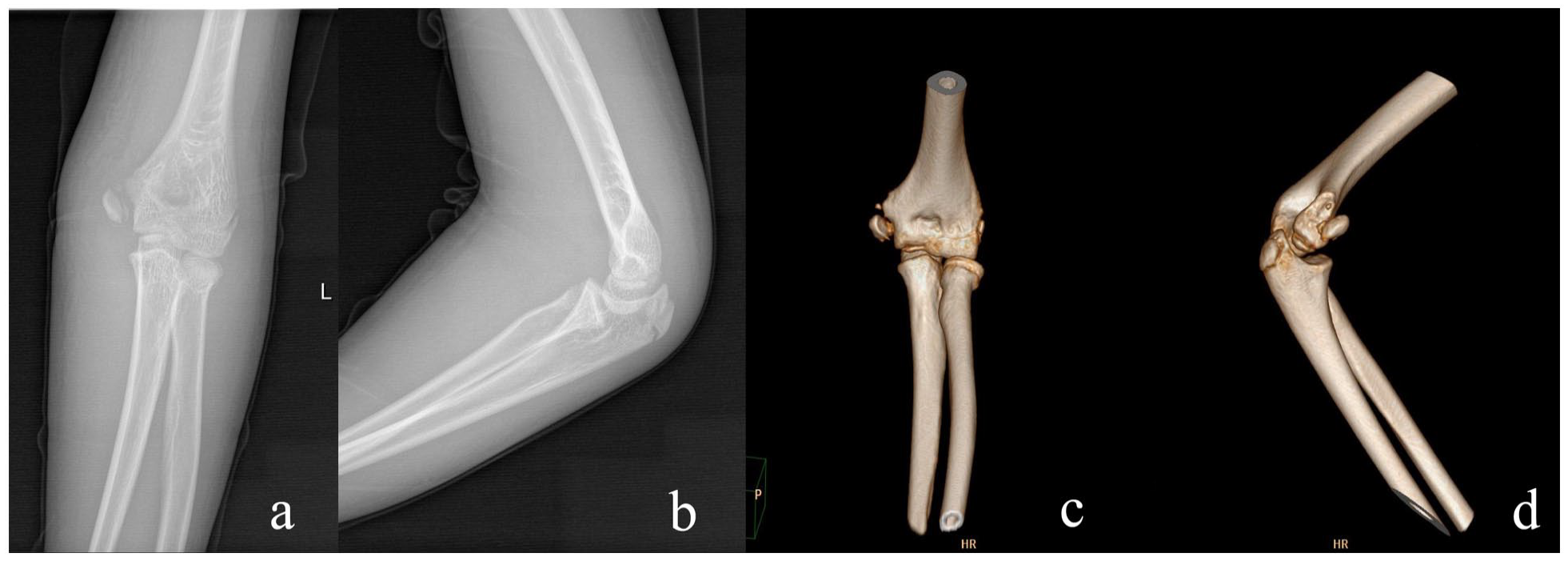
Case 4: A 13-year-old boy with a MELAINE lesion of the left elbow: (a, b) type II MEP fracture and type I RN fracture diagnosed on CT images (c, d).
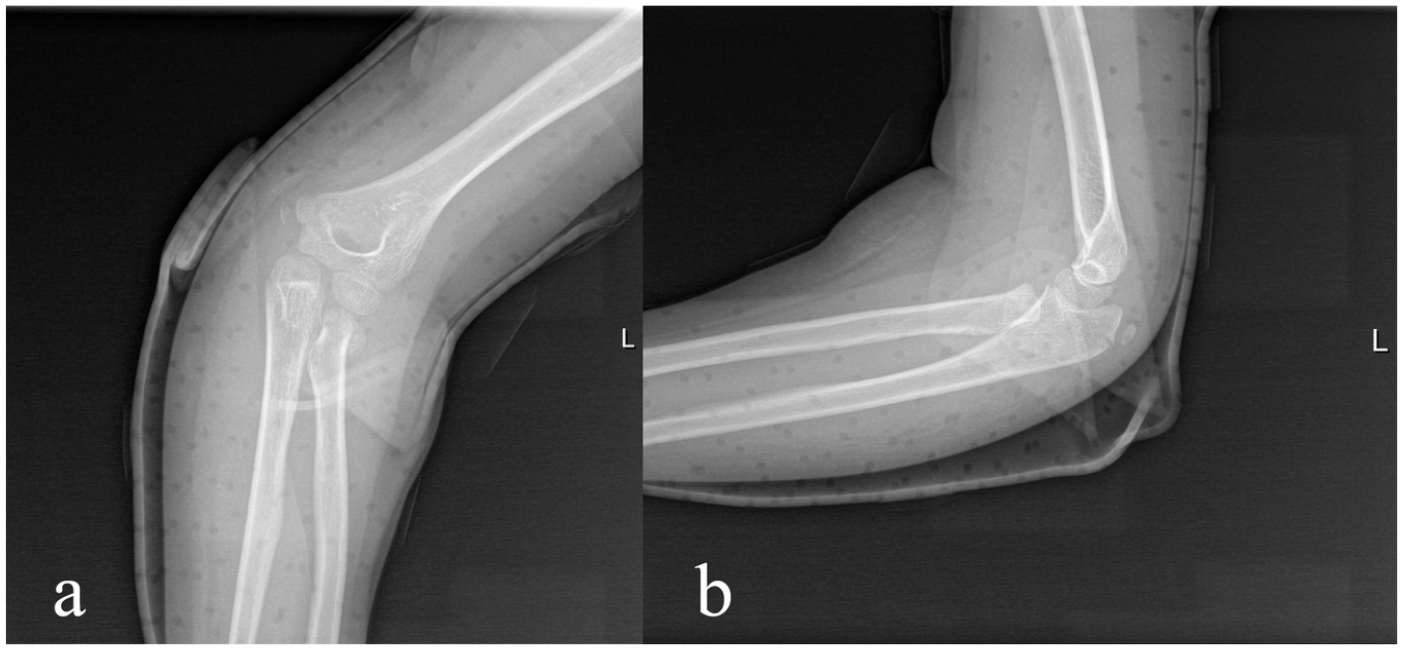
In addition, six patients had associated injuries: elbow dislocation (n = 3) (Figure 3, Case 8), olecranon fracture (n = 1) (Figure 4, Case 10), ulnar nerve injury (n = 1) and capitellum contusion (n = 1) (Figure 3, Case 8). One patient (Figure 5, Case 1) had been treated for a supracondylar fracture of the humerus 1 year before the MELAINE injury and had developed a residual cubitus valgus of 8°.
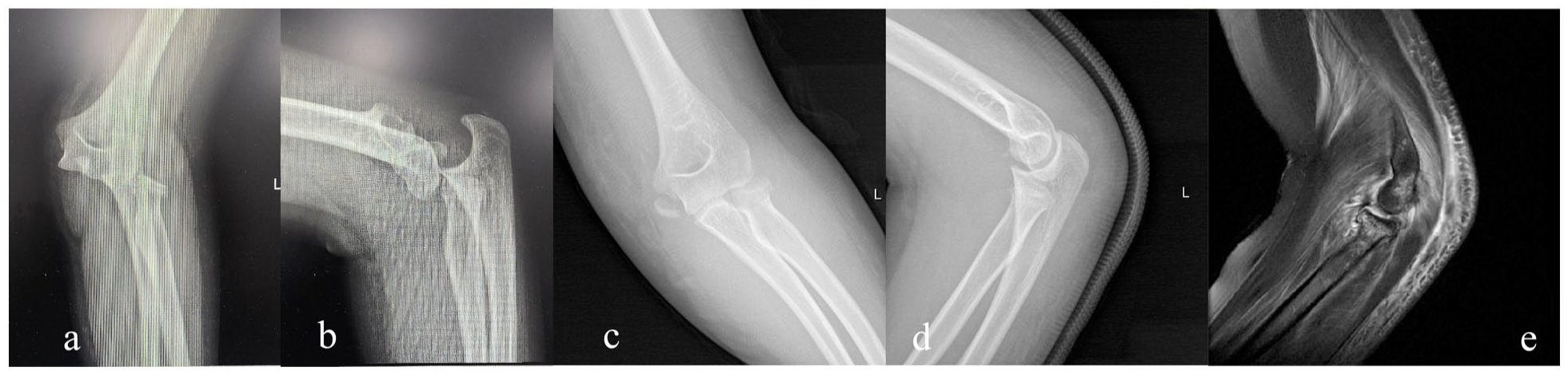
Case 8: A 12-year-old girl with a MELAINE lesion of the left elbow and associated elbow dislocation: (a, b) type IV MEP fracture, type II RN fracture and elbow dislocation; (c, d) reduction of elbow dislocation; (e) contusion of the capitellum diagnosed on MRI images.
Case 10: A 7-year-old girl with a MELAINE lesion of the left elbow with an associated olecranon fracture: (a, b) type II MEP fracture, type II RN fracture and olecranon fracture.
Case 1: An 11-year-old boy with a MELAINE lesion of the left elbow and previous supracondylar fracture of the humerus with 8° of residual valgus (a, b); 1 year later, with a MELAINE lesion: (c, d) type II MEP fracture and type III RN fracture.
Table 1 shows the patient demographics and fracture characteristics.
Patient demographics and fracture characteristics.
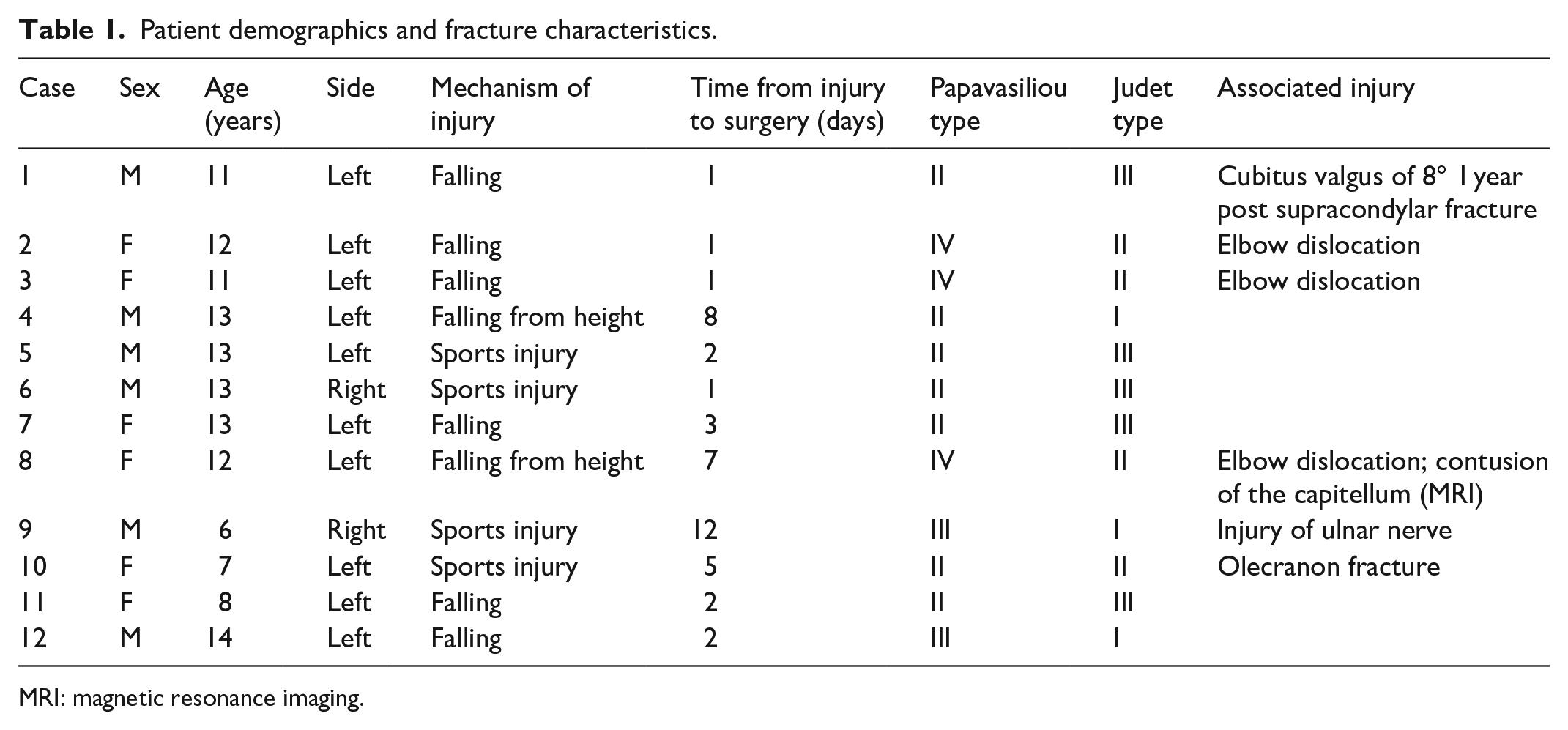
MRI: magnetic resonance imaging.
Treatment
Patients with type II, III, and IV MEP fractures underwent surgical treatment and were fixed with a cannulated screw. Overall, nine MEP fractures underwent screw fixation, and three underwent K-wire fixation.
Type II with >20° angulation and type III RN fractures were reduced and stabilized by the use of an elastic intramedullary nail (titanium elastic nail (TEN)), while those with fractures classified as type I or type II with <20° angulation underwent conservative treatment (long arm cast immobilization for 6 weeks). Overall, eight RN fractures underwent TEN fixation, and four underwent conservative treatment.
Among the patients with associated lesions, those with an olecranon fracture (n = 1) underwent closed reduction and K-wire fixation, ulnar nerve injury (n = 1) benefited from surgical exploration followed by anterior nerve transposition, and capitellum contusion (n = 1) underwent conservative treatment; elbow dislocations (n = 3) were reduced before fracture treatment.
All procedures were performed under general anesthesia with the patient lying in the supine decubitus position. Elbow stability (varus/valgus stress) was texted before and after surgical procedure.
Table 2 shows the treatment modality and outcomes.
Treatment and outcomes.
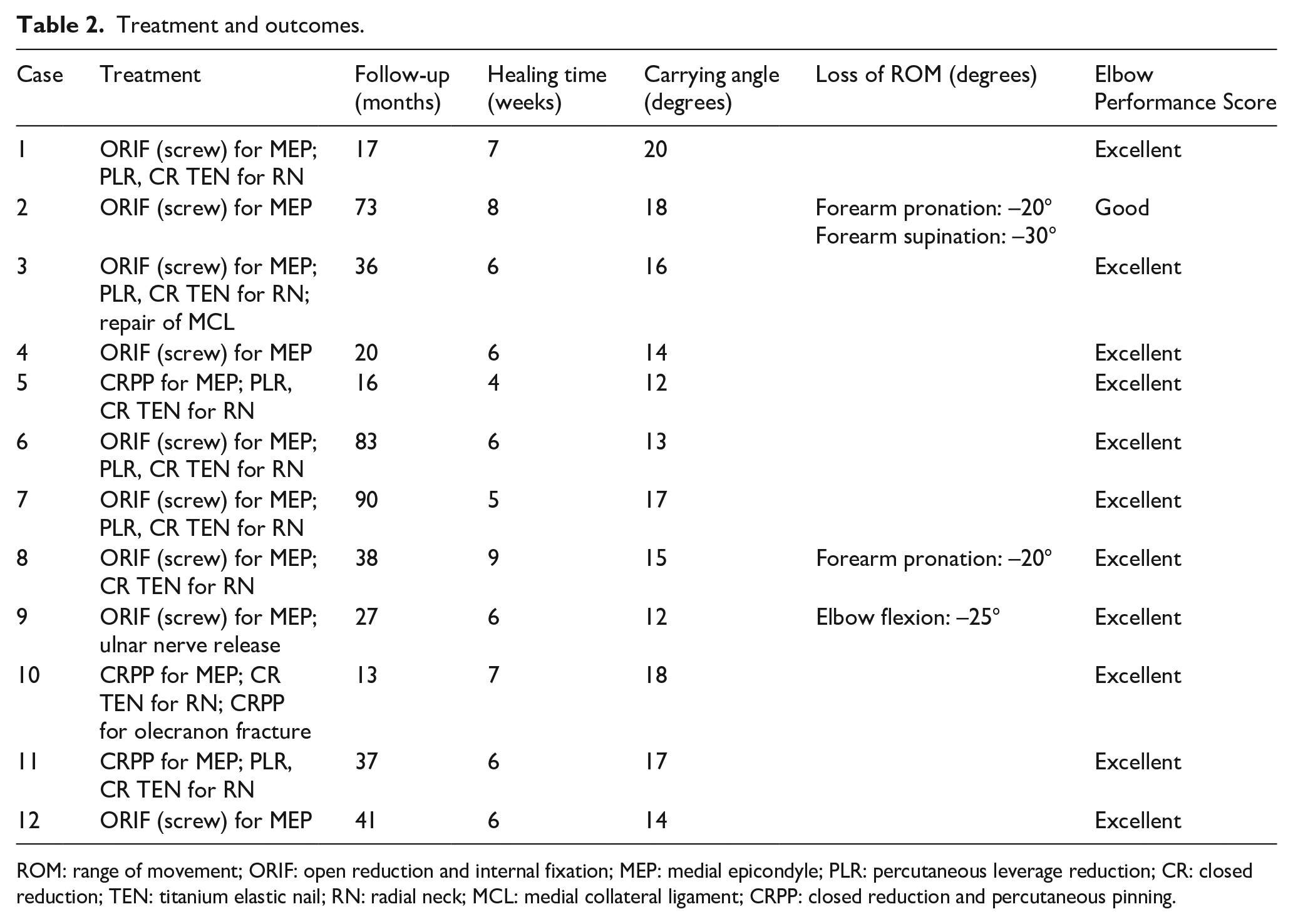
ROM: range of movement; ORIF: open reduction and internal fixation; MEP: medial epicondyle; PLR: percutaneous leverage reduction; CR: closed reduction; TEN: titanium elastic nail; RN: radial neck; MCL: medial collateral ligament; CRPP: closed reduction and percutaneous pinning.
Clinical and radiographic follow-up
All study patients had full-length AP and lateral radiographs of the injured upper extremity and underwent regular radiographic evaluation for at least 12 months after index surgery (range, 13–90) to assess fracture consolidation and detect complications such as secondary displacement, refracture, hardware migration, nonunion or malunion. In particular, radiographs were performed every month for the first 3 months posttreatment and every 3 months thereafter.
After surgery, the upper limb was immobilized with a cast for 3–4 weeks, after which progressive limb mobilization was allowed.
The carrying angle (CA) and function of both elbows were measured at the last clinical-radiographic follow-up visit performed no less than 12 months after index surgery.
The CA is the angle between the longitudinal axes of the arm and forearm with the elbow extended12,13 (Figure 6, Case 1). The axis of the arm is defined distally by the midpoint between the medial and lateral epicondyles of the humerus and proximally by the lateral edge of the cranial surface of the acromion. The axis of the forearm, on the contrary, is defined distally by the midpoint between the radial and ulnar styloid processes and proximally by the midpoint between the medial and lateral epicondyles of the humerus.
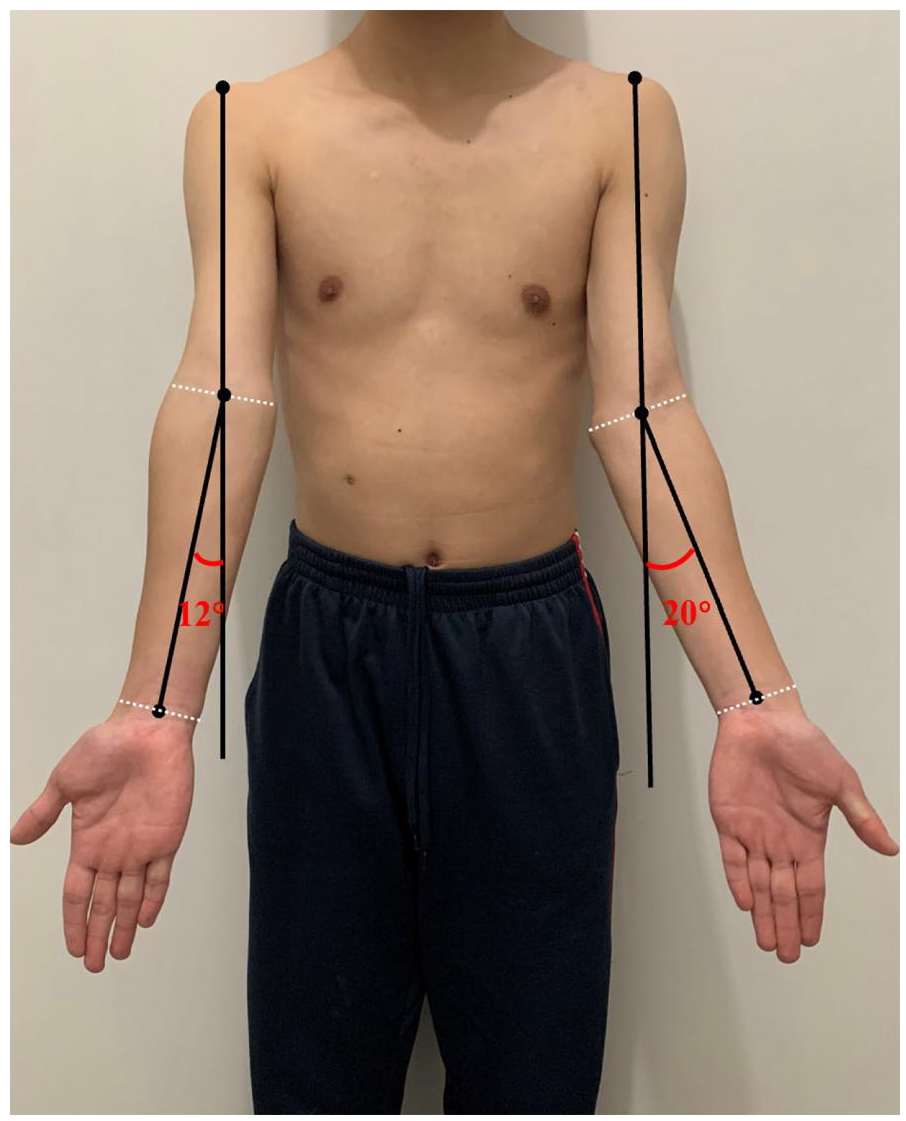
Patient with residual valgus of 8° (Case 1).
Functional assessment included the range of motion (ROM) of elbow flexion-extension and forearm pronation-supination on the injured side compared with the healthy side. Loss of ROM was defined as a reduction in ROM of more than 20° in each direction. The upper extremity function was evaluated using Elbow Performance Score (EPS) proposed by Kim et al., 14 which is a composite score out of 100 with higher scores reflecting better results 15 (deformity: 25; pain: 25; ROM: 25; function: 25). The functional outcome of the elbow is graded as excellent (score: ≥90), good (score: 75–89), satisfactory (score: 60–74), or poor (score: <60).
Statistical analysis
Data were analyzed using the IBM SPSS statistical package version 22.0 (IBM Corporation, Armonk, NY, USA). The Shapiro–Wilk test was first used to determine whether the data fit the normal distribution. Paired-sample t-tests or Wilcoxon rank sum tests were used to compare the differences in the CA, ROM, and EPS between the injured elbow and the uninjured elbow at the last follow-up. The threshold for statistical significance was set to a p value less than 0.05.
Results
Tables 1 and 2 show the patient demographics and treatment outcomes, respectively.
All patients were followed up for an average of 40 ± 25.6 months (range, 13–90). Radiographs showed that all fractures healed in 6.3 ± 1.2 weeks on average (range, 4–9). At the last follow-up visit, the CA of the injured side was 15.5° ± 2.6°, while it was 14.7° ± 2° on the uninjured side (p = 0.218) (Tables 2 and 3).
Comparison between injured and uninjured sides.
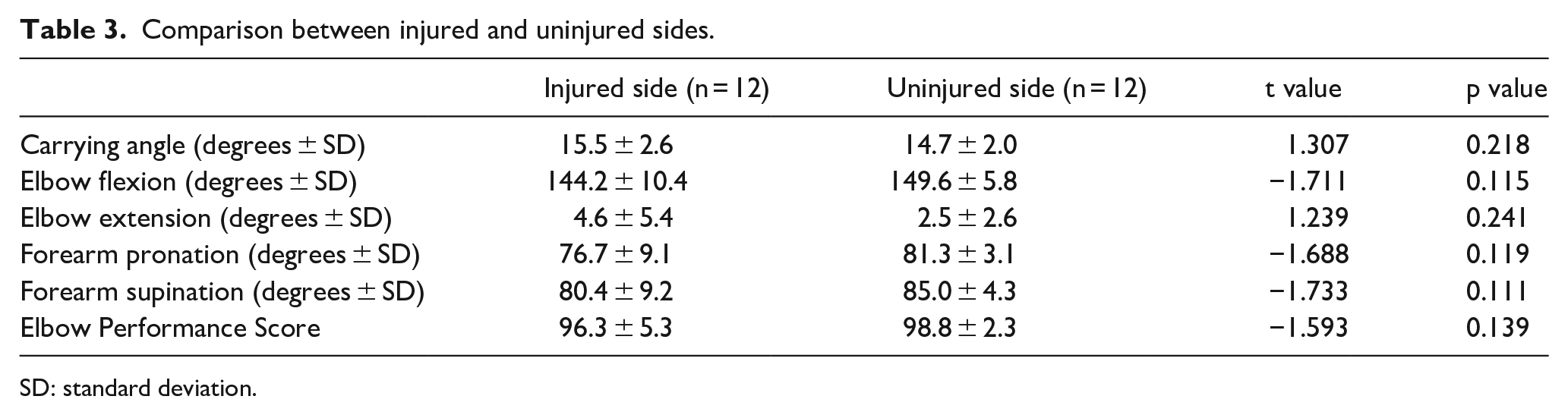
SD: standard deviation.
The EPS was 96.3 ± 5.3 on the injured side and 98.8 ± 2.3 on the uninjured side (p = 0.139). Outcomes were good to excellent in all patients: the EPS was excellent in 11 patients (91.7%) and good in 1 patient (8.3%) (Tables 2 and 3).
The ROM of elbow flexion-extension and forearm pronation-supination of the injured side was 144.2° ± 10.4°, 4.6° ± 5.4°, 76.7° ± 9.1°, 80.4° ± 9.2°, respectively, with no significant differences from the healthy side (p > 0.05). (Table 3); at the end of surgery, elbow was judged as stable in all operated cases.
The patient with a good outcome (score: 85) had a type II RN fracture, type IV MEP fracture and concomitant elbow dislocation; the patient underwent closed reduction of the elbow dislocation, screw fixation of the MEP fracture, and conservative management of the RN fracture. At the last follow-up visit, pronation-supination was limited to 60°-0-60° due to residual angulation of the RN (35°) (Table 2).
Radiographically, no secondary displacement, hardware migration, consolidation delays, nonunion, malunion, or refracture were noted.
None of the patients developed complications such as infection, cubitus valgus, stiffness, or instability.
Discussion
Our study showed that concomitant MEP and RN fractures are possible in pediatric patients and are suggestive of a “diagonal injury of the elbow.” MELAINE-type injuries, if recognized and treated appropriately, yield favorable clinical and radiological outcomes.
The concept of a “diagonal lesion” was introduced by Li et al. 9 to describe the association between a compression fracture of the anteromedial tibial plateau and a tensile disruption of the posterolateral complex (PLC) or the posterior cruciate ligament (PCL) when the overextended knee joint is impinged by varus stress; the lesion is also known as a “reverse Segond fracture.” 16 In the past, a lack of understanding of this injury has led to diagnostic errors and delays in treatment, resulting in varus deformity of the knee or joint instability.9,17
The elbow and the knee are both hinge joints, which are prone to compression on one side and avulsion on the other side when subjected to a force perpendicular to the plane of motion in the load-bearing position. 9 A forced valgus of the hyperextended elbow is responsible for MELAINE-type injuries. In such a situation, in fact, the MEP and the head and neck of the radius are proximal and medial and distal and lateral to the elbow joint, respectively. Consequently, forced valgus induces traction of the flexor-pronator muscles at the MEP, which causes a MEP fracture, especially when the forearm is supinated and the wrist extended.1,7 At the same time, compression exerted by the capitate on the head and neck of the radius (kissing injury) causes a RN fracture.4,8,18,19 The annular ligament may act as a stress riser, predisposing to RN fracture and lateral tilt.2,16 This type of injury can occur more easily when the CA increases, along with valgus stress in the elbow. In our study, one patient had a history of supracondylar fracture of the humerus (Figure 6, Case 1) with 8° of residual valgus. The patient sustained a MELAINE injury 1 year after the supracondylar fracture. Moreover, compared with other types of elbow fractures, patients with MEP fractures have a larger CA, as reported by Jeong et al. 20 Although isolated avulsion fractures of the MEP have been documented in adolescents who were arm wrestlers or overhead athletes, they are rarely concomitant with RN fractures.21,22 However, the association between MEP and RN fractures has rarely been documented in the pediatric population.1 –3
Figure 7 shows the pathogenetic mechanism of MELAINE lesions.
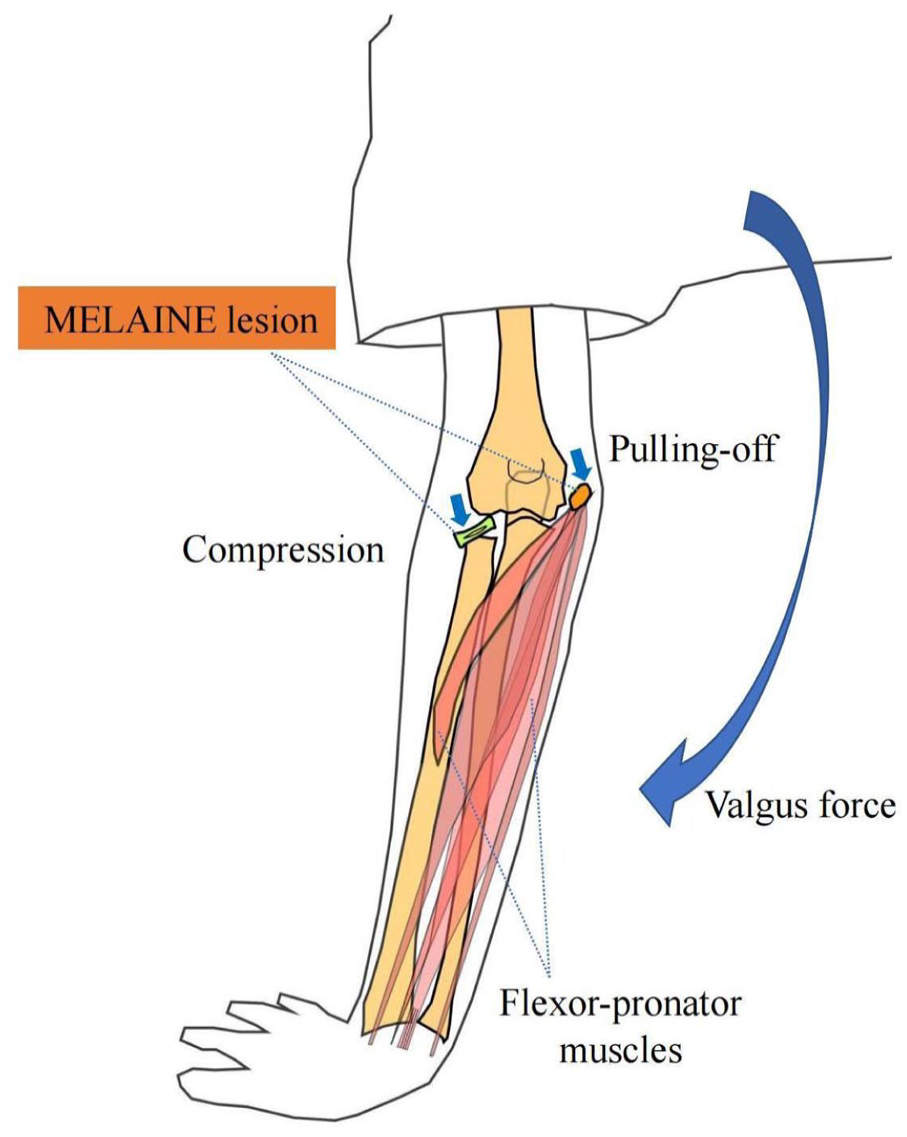
Schematic diagram of the pathogenetic mechanism.
Moreover, in addition to the classic lesion characterized by the association between MEP and RN fractures, other MELAINE-type lesions exist. In particular, there was a case of capitellum contusion associated with MEP fracture in our patient group; this case showed the characteristic impact of the capitellum with the radial head following valgus stress at the elbow; if the force is strong enough, the capitellum fracture can occur simultaneously with the proximal radius fracture, which is known as a “kissing injury.” 18 In addition, in another case, a concomitant olecranon fracture occurred secondary to the impact of the tip of the olecranon with the medial wall of the olecranon fossa, as reported by Carl and Ain 3 when valgus stress was applied to the hyperextended elbow.
In our study, most of the MEP fractures had significant displacement (7 type II, 2 type III, and 3 type IV), while the majority of RN fractures had mild displacement (3 type I, 4 type II, and 5 type III). Overall, avulsion fractures are more severe than compression fractures. This feature is similar to that reported by Li et al. 9 regarding “diagonal lesions” in the knee in which ligament tears or avulsion fractures are more severe than compression fractures of the tibial plateau. Therefore, it is important to avoid the missed diagnosis of a concomitant minimally or nondisplaced RN fracture. When the proximal radius is swollen and painful in patients with a MEP fracture, a CT scan or MRI should be performed to assess whether the RN is fractured. In our group, there were two cases of type I RN fracture detected by CT scan that had not been previously detected on radiographs.
In our opinion, MELAINE injuries should be managed surgically to avoid elbow valgus deformity and joint instability.
Minimally displaced MEP (types I and II) and RN fractures (types I and II) can be treated conservatively.23 –25 However, in MELAINE lesions, there is both medial and lateral instability, and more active intervention should be favored. Therefore, the surgical indication to stabilize the elbow is reserved for RN type II–IV fractures and MEP type II–IV fractures. On the contrary, minimally displaced MEP (type I) and RN (type I) fractures can be treated conservatively.
Outcomes were good to excellent in all patients: the EPS was excellent in 11 patients (91.7%) and good in 1 patient (8.3%) (Tables 2 and 3); moreover, the CA, ROM, and EPS of the injured and uninjured sides were comparable. One patient with a type II RN fracture, type IV MEP fracture, and concomitant elbow dislocation underwent closed reduction of the elbow dislocation, screw fixation of the MEP fracture, and conservative management of the RN fracture. At the last follow-up visit, pronation-supination was limited to 60°-0-60° due to residual angulation of the RN. Therefore, we recommend surgical reduction and fixation of MELAINE lesions, even those with minimal displacement, especially when associated with elbow dislocation.1,5,23
In addition, according to our experience, some important points should be kept in mind during surgery: (1) First, the MEP fracture should be reduced and fixed, particularly for type III and type IV lesions, to stabilize the elbow joint. 1 (2) The forearm should be placed in pronation and the wrist in flexion while applying some varus force at the elbow joint to ease MEP fracture and RN fracture reduction. 7 (3) Fixation should be minimally invasive to minimize the damage to the soft tissues and the growth cartilage. (4) The medial collateral ligament and the joint capsule should be repaired only when the elbow remains unstable after reduction and fixation of the MEP fracture.7,23 In our series, we found one case requiring medial collateral ligament repair. (5) Postoperative long arm cast immobilization of the upper extremity for 3–4 weeks is recommended before allowing progressive mobilization. 5
We encountered some limitations in the analysis of our results, including the retrospective design of the study and the relatively small number of patients included. Moreover, only surgically treated patients were assessed and lack of control group. In addition, the concept of MELAINE lesions was based on pathogenetic mechanisms and radiographic findings only, as no biomechanical studies were performed. Despite these limitations, this is the first study that evaluated a series of pediatric patients and documented the clinical and radiographic outcomes of MELAINE lesions. The study patients were consecutive and were all treated similarly according to the same principles. Future prospective controlled trials with a larger number of pediatric patients as well as biomechanical studies are needed to confirm the findings of our study.
Conclusion
In conclusion, although relatively rare, MELAINE lesions are possible and should not be neglected. Surgical treatment aims to stabilize the elbow and avoid valgus and deformity. If properly diagnosed and treated, clinical and radiological results are excellent in most cases.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231182422 – Supplemental material for Diagnosis and treatment of “medial to lateral diagonal injury of the elbow” in children: Concomitant medial epicondylar and radial neck fractures
Supplemental material, sj-pdf-1-cho-10.1177_18632521231182422 for Diagnosis and treatment of “medial to lateral diagonal injury of the elbow” in children: Concomitant medial epicondylar and radial neck fractures by Yunan Lu, Federico Canavese, Yongjie Xia, Ran Lin, Dianhua Huang, Tianlai Chen and Shunyou Chen in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Yunan Lu: Study design, drafting of the manuscript, manuscript preparation, data analysis, statistical analysis, and revision of the manuscript.
Ran Lin and Dianhua Huang: Drafting of the manuscript, statistical analysis.
Yongjie Xia and Tianlai Chen: Statistical analysis, revision of the manuscript.
Federico Canavese: Study design, drafting of the manuscript, manuscript preparation, data analysis, statistical analysis, revision of the manuscript.
Shunyou Chen: Design of the study, surgery and general supervision of the research group.
All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the financial support of the Fujian Provincial Clinical Medical Research Center for First Aid and Rehabilitation in Orthopedic Trauma (2020Y2014) and the Key Clinical Specialty of Fujian Province (20220104).
Compliance with ethical standards
All procedures in studies involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This was a retrospective study, and IRB approval was obtained (Approval No. 2022213).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.