
Abstract
Purpose:
Compare functional, oncologic, and complication outcomes of distal femoral reconstruction after malignant tumor resection in children <12 years, in whom adult implants are unsuitable.
Methods:
Preferred Reporting Items for Systematic Reviews and Meta-Analyses-guided systematic review and meta-analysis of PubMed, Embase, Scopus, Web of Science, and Cochrane (inception–January 1, 2025). Eligible studies reported outcomes for expandable or non-expandable prostheses, osteoarticular allograft, allograft–prosthetic composite, epiphyseal-preserving reconstruction, rotationplasty, arthrodesis, spacers, or amputation. Random-effects models pooled means/proportions; risk of bias was assessed using the Newcastle–Ottawa Scale; and certainty was assessed using GRADE.
Results:
Forty-one studies (n = 1186) met criteria. Pooled mean Musculoskeletal Tumor Society was 24.9/30 (95% confidence interval, 23.9–25.9; I2 = 97%). Biological joint-preserving methods and rotationplasty tended to yield the highest function; arthrodesis and amputation were lower. Local recurrence was 5.2% (95% confidence interval, 3.3–7.1) without differences between techniques. Five-year overall survival was 81.6% (76.6–86.6); epiphyseal-preserving reached 93.3%, expandable prostheses 79.0% (contextual, not causal). Complications differed: expandable prostheses had reoperation rates of 57.2% and mechanical failure of 42.3%; osteoarticular allograft had a fracture rate of 27.4% and failure rate of 37.5%; allograft–prosthetic composite had a failure rate of 24.4% and nonunion rate of 13.5%; and arthrodesis had the fewest complications. Deep infection was 6.7%. GRADE certainty was as follows: high for local recurrence; moderate for 5-year survival and infection; and low for function and reoperation/failure (heterogeneity, retrospective design).
Conclusions:
Reconstruction should be individualized, prioritizing function and complication risk; oncologic outcomes appear driven by tumor biology/systemic therapy. Heterogeneity and inconsistent failure definitions limited cross-technique comparisons and precluded pooled implant survival.
Significance of study:
Our pooled estimates offer practical reference points for counseling families about function and complications across reconstruction options in children aged <12 years while highlighting priorities for standardized reporting and coordinated prospective research.
Keywords
Introduction
Malignant bone tumors of the distal femur in children present significant surgical and reconstructive challenges. In children under 12 years, adult-type endoprosthetic replacements are typically inappropriate because of small bone size, open growth plates with risk of iatrogenic closure, and considerable remaining longitudinal growth. 1 In addition, the likelihood of requiring multiple revision surgeries as the child grows increases, adding further complexity. 2 These factors necessitate alternative reconstructive approaches tailored to the unique anatomical and developmental needs of skeletally immature patients. 3
Various reconstruction methods have been developed for skeletally immature patients following distal femoral tumor resection. Options include expandable endoprostheses, which can be lengthened to accommodate growth 4 ; biological reconstructions using osteoarticular allografts (OAA) or allograft–prosthetic composites (APCs) 5 ; joint-sacrificing procedures such as rotationplasty (Van Nes procedure), where the limb is turned to use the ankle as a knee 6 ; arthrodesis 7 ; temporary spacer implants (often as an interim measure in infection or staged surgery) 8 ; and above-knee amputation. 9 Each technique has distinct trade-offs in terms of functional outcomes, complication risks, and impacts on a child’s development and quality of life (QoL). 10 However, current comparative evidence remains fragmented, with most studies being small, retrospective case series. Consequently, no clear consensus exists on the optimal reconstructive strategy, and decision-making often relies on the surgeon’s experience and individual case considerations. 11
To address this gap, we performed a systematic review and meta-analysis comparing the outcomes of various distal femoral reconstruction techniques in children ineligible for adult tumor prostheses. Specifically, we evaluated the functional outcomes, oncologic control, and complication rates of expandable prostheses, biological reconstructions, rotationplasty, arthrodesis, spacers, and amputation. By applying rigorous meta-analytic methods and adhering to open science principles, we aimed to inform clinical decision-making and improve long-term outcomes in this vulnerable pediatric population.
Materials and methods
Protocol and registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 12 The review protocol, outlining the study objectives, eligibility criteria, and planned analyses, was prospectively registered with the PROSPERO database (ID—CRD420251020941). The review team comprised orthopedic oncology specialists and methodologists.
Literature search strategy
We conducted a comprehensive search of PubMed, Embase, Scopus, Web of Science, and the Cochrane Library from database inception to January 1, 2025. The strategy combined free-text keywords with controlled vocabulary (Medical Subject Headings) using Boolean operators. Core terms included the distal femur, bone sarcoma (e.g., osteosarcoma, Ewing sarcoma), children/pediatrics, limb salvage, reconstruction, expandable prosthesis, rotationplasty, allograft, composite, and amputation. To maximize the yield, we hand-searched the reference lists of all included studies and relevant reviews. We limited inclusion to English-language publications and applied no study design restrictions at the search stage, and design- and data-based criteria were enforced during screening and eligibility assessment.
Eligibility criteria
Eligible studies enrolled children younger than 12 years who underwent distal femoral resection for primary malignant bone tumors (e.g., osteosarcoma, Ewing sarcoma); mixed-age cohorts were included only when data for the <12-year subgroup were extractable. We considered any index reconstruction after distal femoral resection, including expandable and non-expandable modular tumor prostheses, OAA, APCs, epiphyseal-preserving intercalary techniques that do not cross the knee joint, arthrodesis, rotationplasty, and temporary or permanent spacers. Amputation was also recorded for comparison. A comparator was not required for inclusion; when present, comparators were extracted as reported, and in multi-arm studies, we abstracted data by reconstruction type. Studies had to report at least one prespecified endpoint: functional outcomes (Musculoskeletal Tumor Society (MSTS), 0–30), 13 oncologic control (local recurrence (LR); overall or disease-specific survival, typically at 3–5 years), or surgical outcomes (complications and durability, including implant/reconstruction failure, infection, nonunion, mechanical/aseptic failure, reoperation, and limb/reconstruction survival). Eligible designs were original clinical investigations, retrospective or prospective cohorts, case–control studies, or trials published in peer-reviewed English-language journals; case series were included if they met the minimum size threshold. We excluded reports limited to patients ≥12 years without an extractable <12 subgroup, studies of non-malignant conditions, wrong site/intervention, or imaging-only endpoints, non-primary publications (abstracts, letters, reviews, technical notes), series with fewer than five patients, and studies lacking quantitative outcome data relevant to our endpoints. For consistency across screening and synthesis, reconstructions were categorized a priori as joint-preserving (intercalary/epiphysis-sparing procedures that do not cross the knee joint), joint-replacing (procedures that cross the joint, including OAA, APC, and endoprosthetic replacement; expandable or non-expandable), arthrodesis (knee fusion), and rotationplasty. Where expandable systems were mixed, we recorded noninvasive versus invasive lengthening when separable, and otherwise analyzed combined expandable cohorts with appropriate caution.
Study selection process
Two reviewers independently screened all titles and abstracts identified through a database search based on predefined inclusion and exclusion criteria. Studies deemed potentially eligible by either reviewer were advanced to full-text evaluation, which was conducted independently and in duplicate. Discrepancies at any stage of the screening process were resolved through discussion with a third reviewer who arbitrated unresolved disagreements. Reasons for exclusion during the full-text review, such as patient age >12 years, incorrect tumor location, ineligible intervention, or absence of relevant outcome data, were recorded. The overall study selection process is described in detail in the PRISMA flow diagram.
Data extraction and management
Two reviewers independently extracted the data using a standardized form. We recorded the study characteristics (first author, publication year, country, design), sample size, patient demographics (age, sex), tumor type, reconstruction method(s), and follow-up duration. Outcomes included MSTS scores (reported as means with ranges or standard deviations), LR counts, overall and/or disease-specific survival (typically at 5 years), and detailed surgical complications (limb/reconstruction survival, infection, nonunion, mechanical failure, and revision). When outcomes were reported by reconstruction method, we abstracted arm-specific data to enable subgroup analysis. Discrepancies were resolved by consensus after re-examination of the source material, with input from a senior reviewer when needed. This review focused on reconstruction-related endpoints (function, complications, limb/reconstruction survival); metastatic status at presentation (M0/M1) was not a predefined outcome and, given inconsistent reporting, was not analyzed.
Quality assessment
The methodological quality of the included studies was assessed using the Newcastle–Ottawa Scale (NOS) for non-randomized studies, 14 which evaluates three domains: selection of study groups, comparability between cohorts, and outcome assessment. Each study was assigned a score ranging from 0 to 9, with higher scores indicating a lower risk of bias. The studies were categorized as high quality (8–9 stars), moderate quality (6–7 stars), or low quality (≤5 stars). Two reviewers independently performed the NOS assessments, and discrepancies were resolved through consensus. To evaluate the overall certainty of evidence for each major outcome, we applied the GRADE framework during the analysis phase, considering five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. 15
Data analysis
Meta-analyses were performed in Review Manager (RevMan 5.4, Version 5.4. Copenhagen: TheNordic Cochrane Centre, The Cochrane Collaboration, 2020) using random-effects (DerSimonian–Laird) models to account for anticipated heterogeneity across studies. Continuous outcomes (e.g., MSTS) were pooled as weighted mean differences when comparative data were available or as pooled means with 95% confidence intervals (CIs) in single-arm series. Dichotomous outcomes, including LR, 5-year survival, 3-year limb survival, and complication rates, were synthesized via proportion meta-analysis using the Freeman–Tukey double-arcsine transformation to stabilize variance, particularly for proportions near 0% or 100%, and the resulting proportions were aggregated under a random-effects model. For interpretability, upper CIs exceeding 100% because of statistical estimation were truncated to 100%. Because Wald (normal) approximations can yield implausible negative lower bounds in sparse strata, 95% CIs were constrained to 0%–100%; where truncation occurred, the original subzero value is documented in Table 1.
Pooled local recurrence rates by reconstruction method.
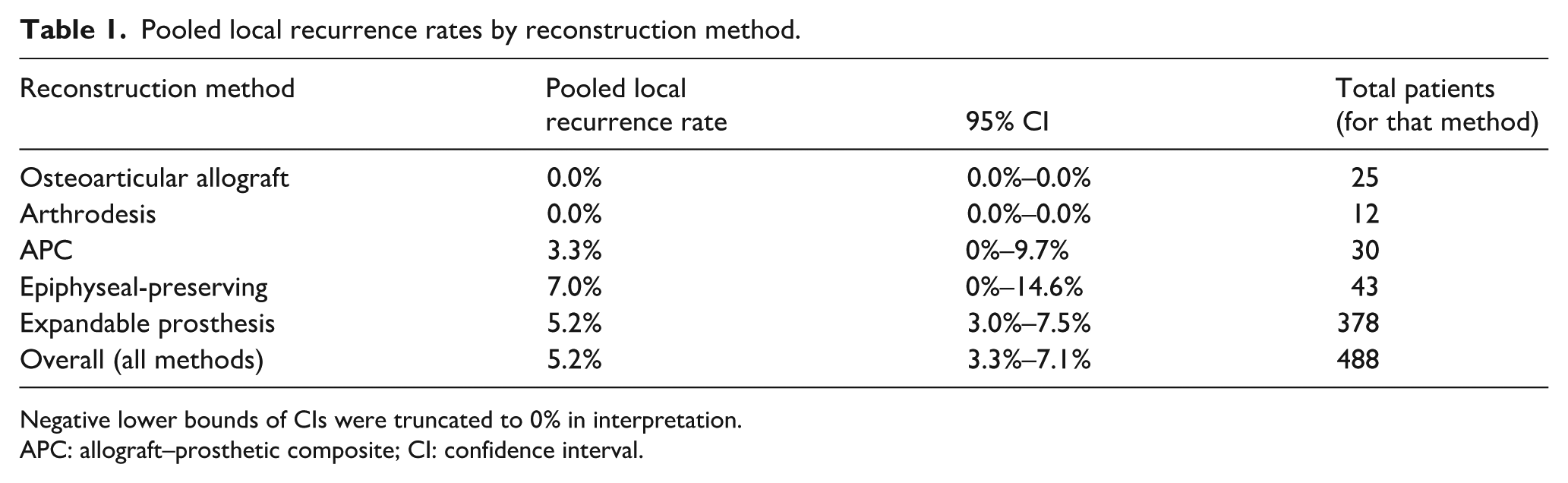
Negative lower bounds of CIs were truncated to 0% in interpretation.
APC: allograft–prosthetic composite; CI: confidence interval.
Statistical heterogeneity was assessed using I2 and the chi-square (Q) test, with I2 > 75% or p < 0.10 indicating substantial heterogeneity. To explore variability, we conducted pre-specified subgroup analyses by reconstruction method (e.g., expandable prosthesis, OAA, and rotationplasty). Because substantial heterogeneity was anticipated for MSTS, we used random-effects pooling and reported prediction-oriented summaries; the interpretation was descriptive rather than comparative when I2 was very high. Meta-regression was not performed owing to an insufficient number of studies per covariate. Sensitivity analyses assessed robustness by excluding low-quality studies (NOS score ≤5) and small-sample reports (n < 10).
The certainty of the evidence for each outcome was graded using the GRADE framework, which evaluates the risk of bias, inconsistency, indirectness, imprecision, and publication bias. Studies with serious methodological flaws, substantial heterogeneity, wide CIs, or indirect populations/interventions were downgraded. Publication bias was assessed by funnel-plot inspection and small-study effect testing; primarily Egger’s test for outcomes with ≥10 studies, with Begg’s test as a comparator; and, when applicable, Duval and Tweedie’s trim-and-fill method was used to estimate the impact of potentially missing studies. All statistical tests were two-tailed, with α = 0.05, unless otherwise specified.
Results
The search yielded 1061 records in total. After removing 742 duplicates, 319 titles/abstracts were screened, leading to 104 full-text articles being assessed for eligibility. Finally, 41 studies met the inclusion criteria, comprising 1186 pediatric patients who underwent distal femoral reconstruction after tumor resection (Figure 1). The total number of patients contributing to each meta-analytic endpoint varied by outcome because of differences in study reporting and the availability of outcome-specific data; some studies reported comprehensive outcomes, whereas others provided selective measures or had limited follow-up, resulting in different denominators across analyses.
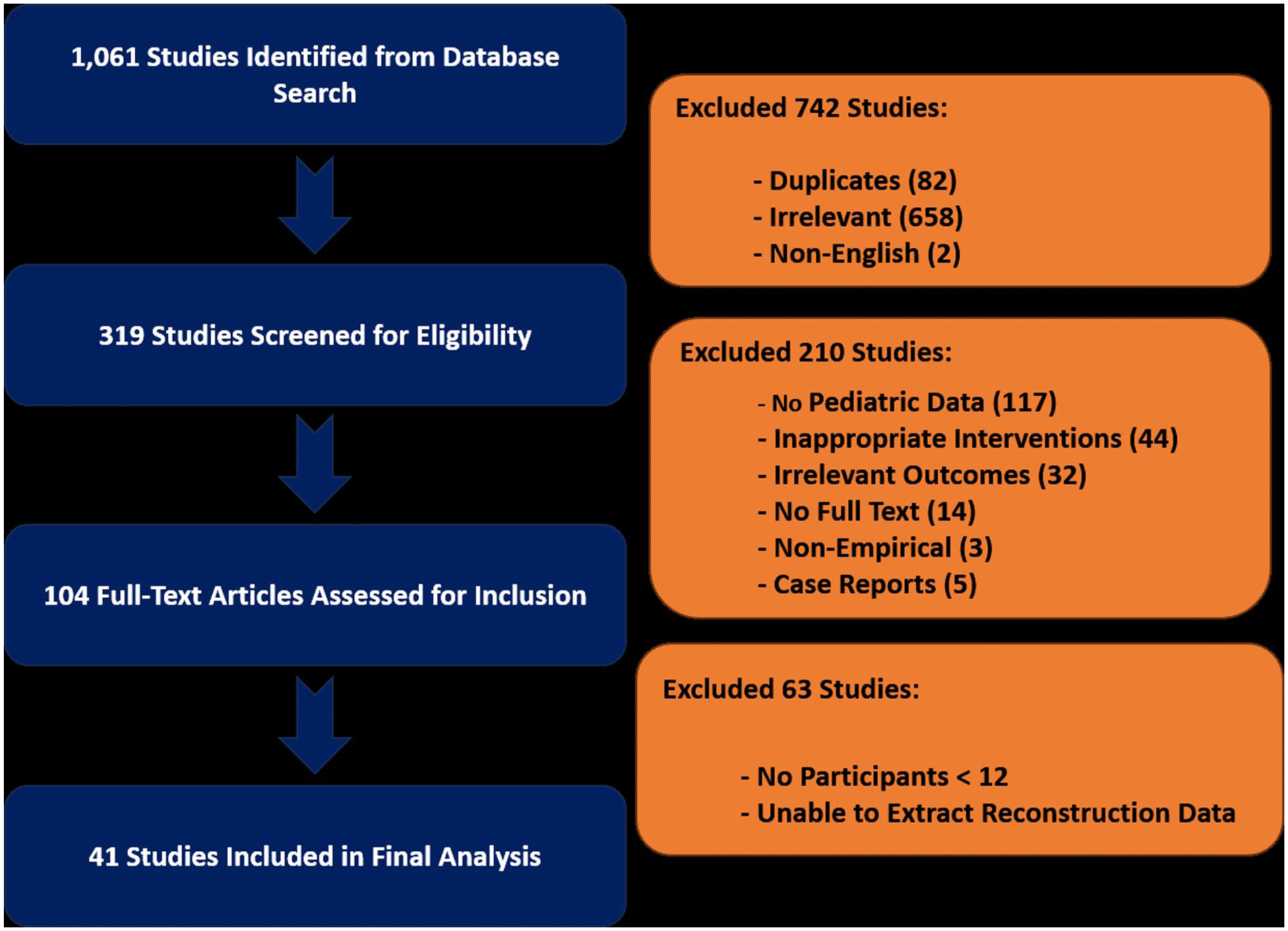
PRISMA flow diagram. Detailed overview of the systematic literature search, screening, inclusion, and exclusion processes used to select eligible studies for this systematic review and meta-analysis.
The patients were 2–12 years old and were predominantly diagnosed with osteosarcoma or Ewing sarcoma. The median follow-up was ~6 years (range, 21–180 months). The reported reconstruction methods included expandable endoprostheses (n = 627), OAA (n = 102), APCs (n = 78), epiphyseal-preserving techniques (n = 170), rotationplasty (n = 25), arthrodesis (n = 12), temporary spacer placement (n = 3), and amputation (n = 29). The detailed patient characteristics and study-level data are presented in Table 2.
Characteristics of included studies. Overview of study-level details for all 41 included articles, listing study authors, year, design, reconstruction methods, patient demographics, mean follow-up duration, and NOS quality rating.
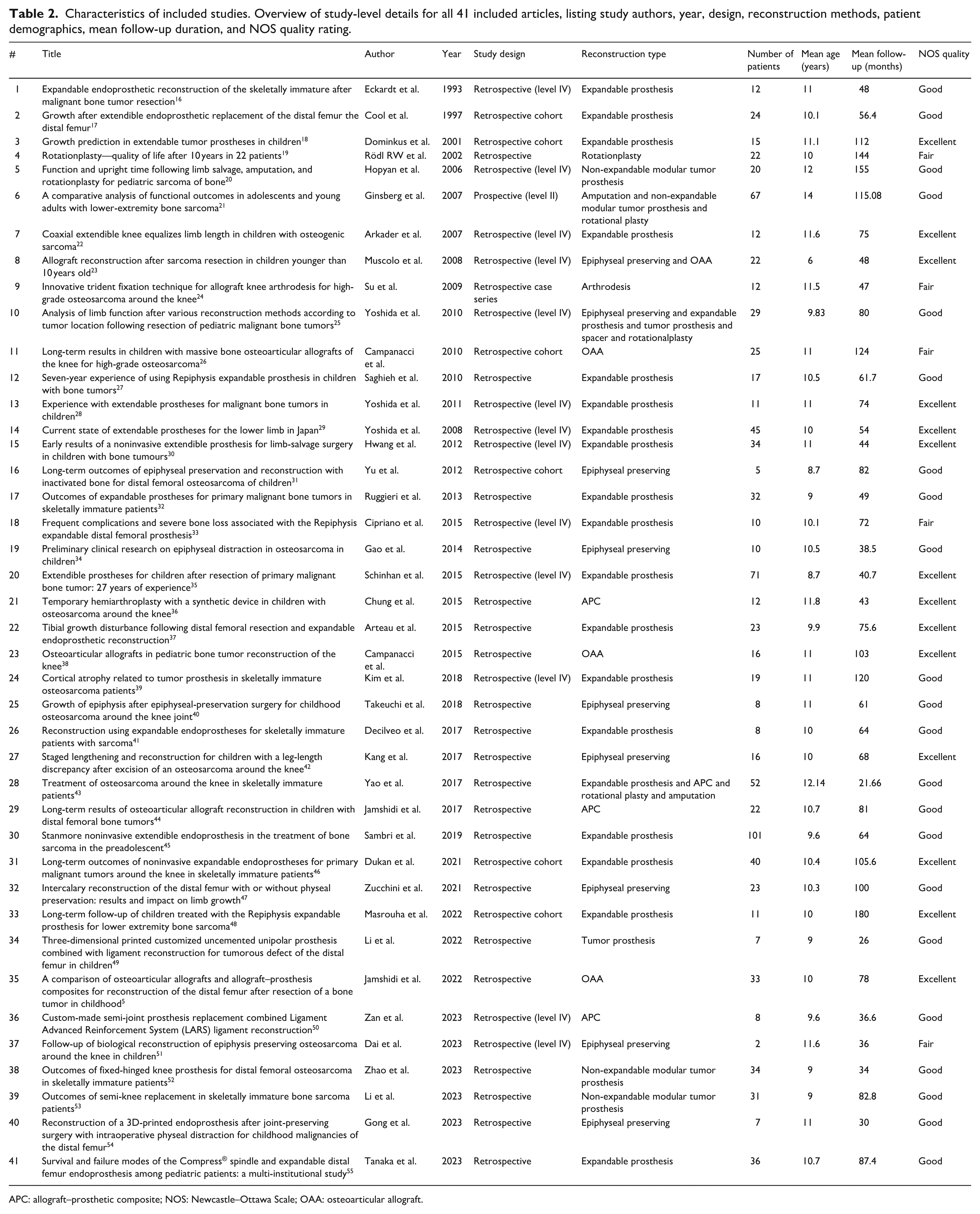
APC: allograft–prosthetic composite; NOS: Newcastle–Ottawa Scale; OAA: osteoarticular allograft.
Quality of studies
The methodological quality of the included studies, assessed using the NOS, had a median score of 7, indicating overall moderate quality. In total, 25% were of high quality (NOS ≥8), ~70% were of moderate quality (NOS 6–7), and <5% were of low quality (NOS ≤5). Common limitations include selection bias, absence of comparative groups, incomplete follow-up, and inconsistent reporting of complications. Sensitivity analyses excluding low-quality studies did not materially change the pooled estimates (Figure 2).
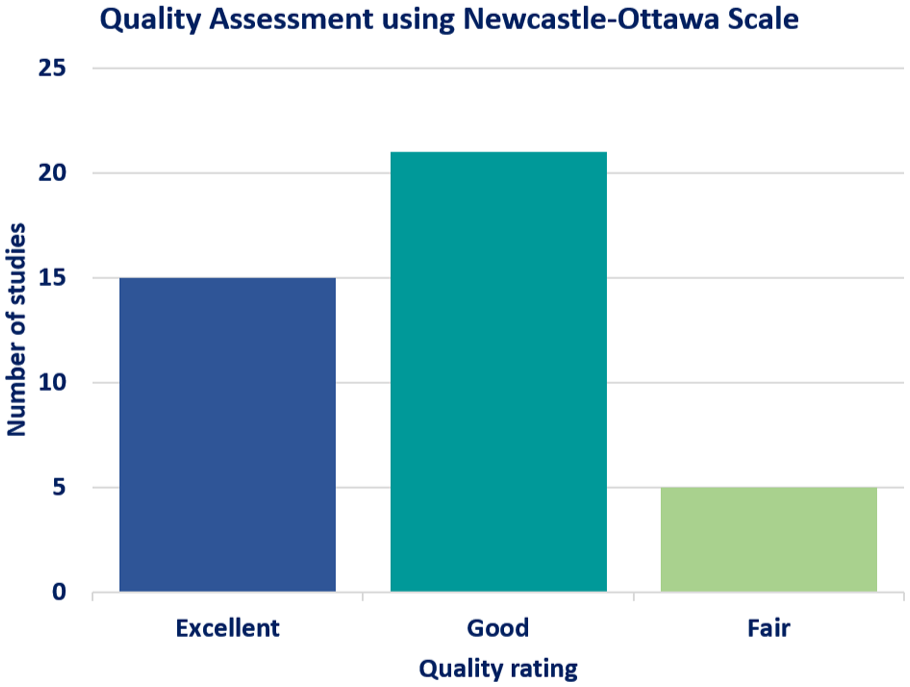
NOS quality assessment. Methodological quality assessment summary for the included studies, categorized by selection, comparability, and outcome reporting criteria. Higher scores indicated a lower risk of bias.
Functional outcomes (MSTS scores)
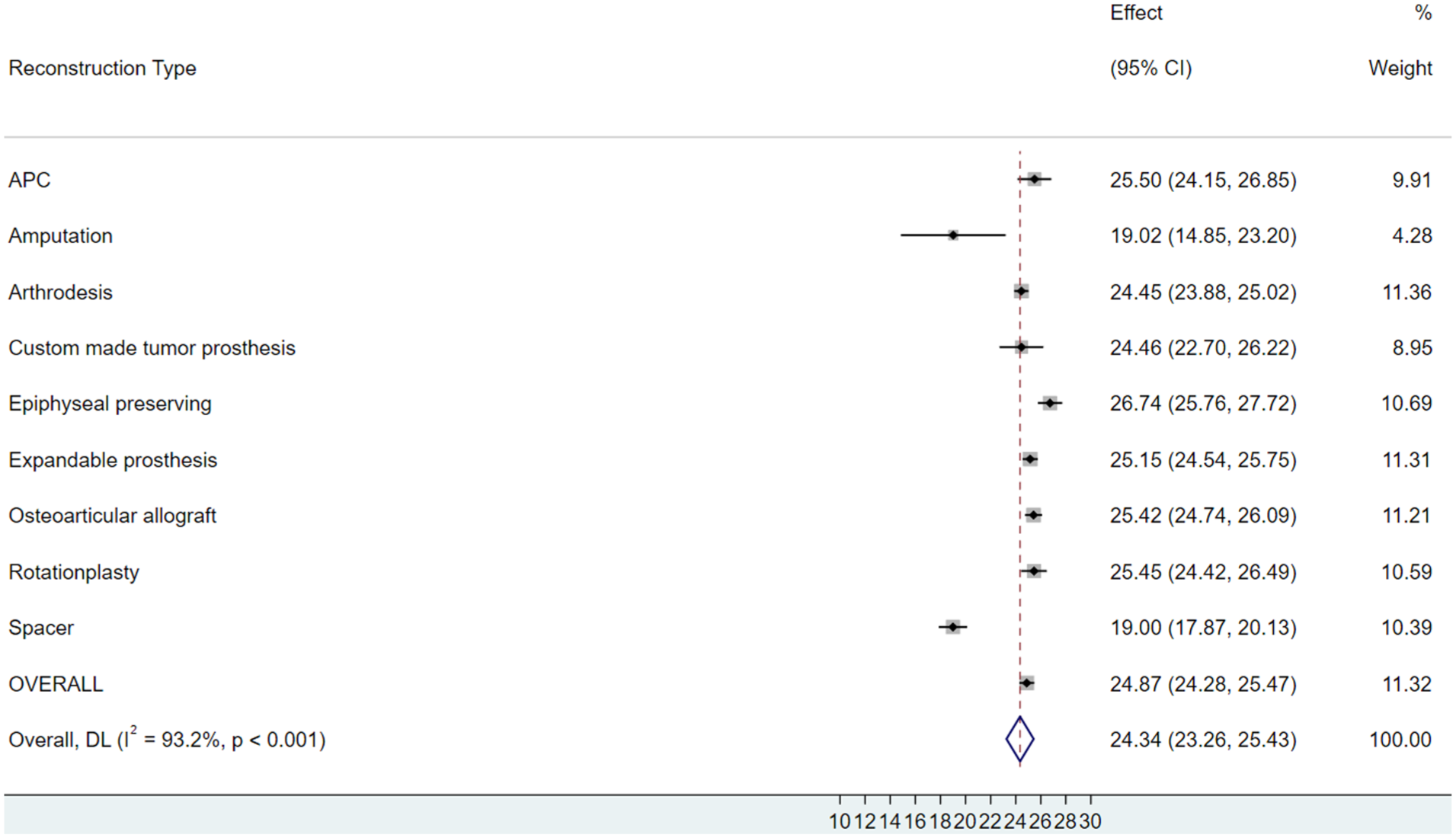
Functional outcomes were assessed using the MSTS scale (0–30 points). All 41 included studies reported MSTS scores or equivalent functional measures. The pooled mean MSTS across the reconstruction methods was 24.9 (95% CI, 23.9–25.9), indicating generally favorable postoperative function. However, heterogeneity was substantial (I2 = 97%, p < 0.001). Accordingly, MSTS findings are presented descriptively with random-effects intervals, and strict cross-technique comparisons were avoided.
Subgroup summaries suggest variation across reconstruction categories. For example, pooled mean MSTS values were as follows: OAA 25.42 (95% CI, 24.74–26.09), APC 25.49 (95% CI, 24.15–26.88), rotationplasty 25.45, expandable prosthesis 25.14; amputation was ~19. Strata sizes and precision differed (e.g., arthrodesis and amputation were small with wide CIs). Given I2 ≈ 97%, these estimates are descriptive and should not be used for cross-technique ranking. Estimates for arthrodesis and amputation were derived from very small strata and carried wide 95% CIs; these values are presented descriptively and should not be over-interpreted. A forest plot of the pooled MSTS scores by reconstruction method is shown in Figures 3 and 4.
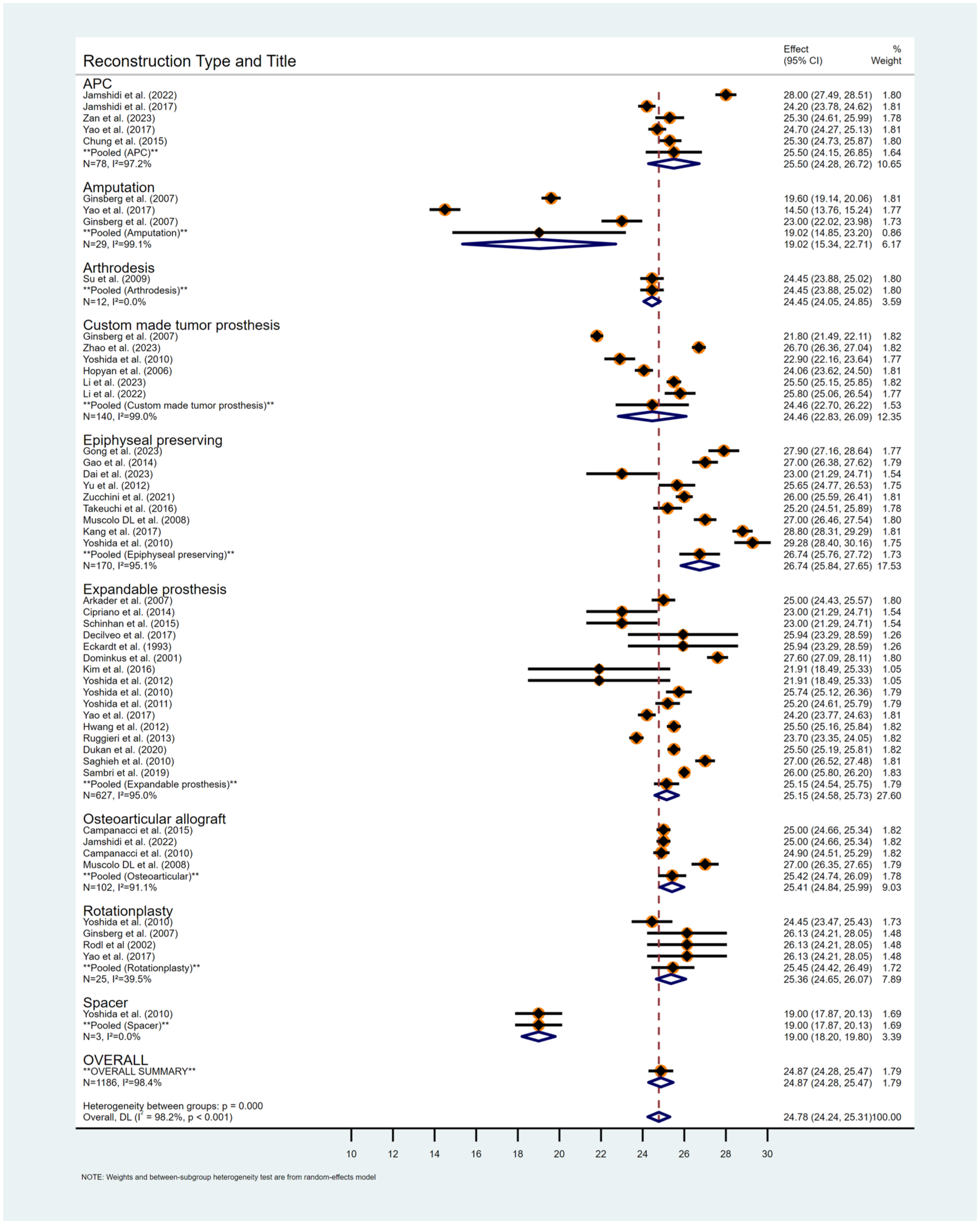
Forest plot of functional outcomes (MSTS scores) by reconstruction method. Meta-analysis comparing postoperative functional outcomes across different distal femoral reconstruction techniques, showing pooled mean MSTS scores with 95% confidence intervals.
Forest plot of MSTS scores (detailed by reconstruction type). Comparative functional outcomes expressed as mean MSTS scores and standard deviations, grouped clearly by each reconstruction type, emphasizing differences in functional performance.
Oncological outcomes
Local control
The pooled LR rate across all reconstruction methods was 5.2% (95% CI, 3.3–7.1). No LR events were reported after OAA or arthrodesis surgery. The LR with expandable prostheses and epiphyseal-preserving reconstructions were 5.2% and 7.0%, respectively, and these differences were not statistically significant. Patient overall survival is presented descriptively for context only; between-reconstruction comparisons were not performed because of confounding by baseline oncologic status and treatment factors (e.g., metastasis at presentation, surgical margins, and histologic response). The LR rates by reconstruction method are summarized in Table 1.
Survival outcomes
Overall survival and limb-specific durability are distinct yet complementary endpoints for evaluating distal femoral reconstruction in skeletally immature patients. Across all included studies, the pooled 5-year overall survival was 81.6% (95% CI, 76.6%–86.6%). By reconstruction category, epiphyseal-preserving procedures demonstrated the highest 5-year survival (93.3%), followed by non-expandable modular tumor prostheses (89.9%), whereas expandable prostheses showed a lower rate (79.0%), which likely reflects baseline differences in patient selection, tumor burden, and treatment responses. Because long-term follow-up (10–20 years) was limited across studies, survival estimates beyond 5 years were not reported.
Three-year limb survival, used to assess reconstructive integrity and early failure risk, was highest with arthrodesis (96.2%; 95% CI, 79.1%–99.4%), followed closely by APCs (91.4%) and expandable prostheses (92.3%). Epiphyseal-preserving reconstructions also performed well (87.9%), while non-expandable modular tumor prostheses were 82.6%. By contrast, OAA had the lowest 3-year limb survival (66.5%), with substantial variability across the individual studies.
Taken together, these findings suggest that patient survival is largely driven by tumor biology and systemic therapy, whereas limb survival is more closely related to the reconstructive strategy and its mechanical durability. The high limb-preservation rates observed with expandable and epiphyseal-preserving methods underscore the evolving success of modern pediatric limb-salvage approaches, whereas the lower limb survival associated with biological reconstruction highlights the technical challenges and structural vulnerabilities in the early postoperative period. A detailed breakdown of survival outcomes by reconstruction method is provided in Table 3.
3-Year limb and 5-year patient survival by reconstruction type. Summary of pooled 3-year limb survival and 5-year overall patient survival across the reconstruction strategies. Limb survival results were derived from a random-effects meta-analysis using the Freeman–Tukey transformation, and the between-study variance (τ2) was reported to reflect heterogeneity.
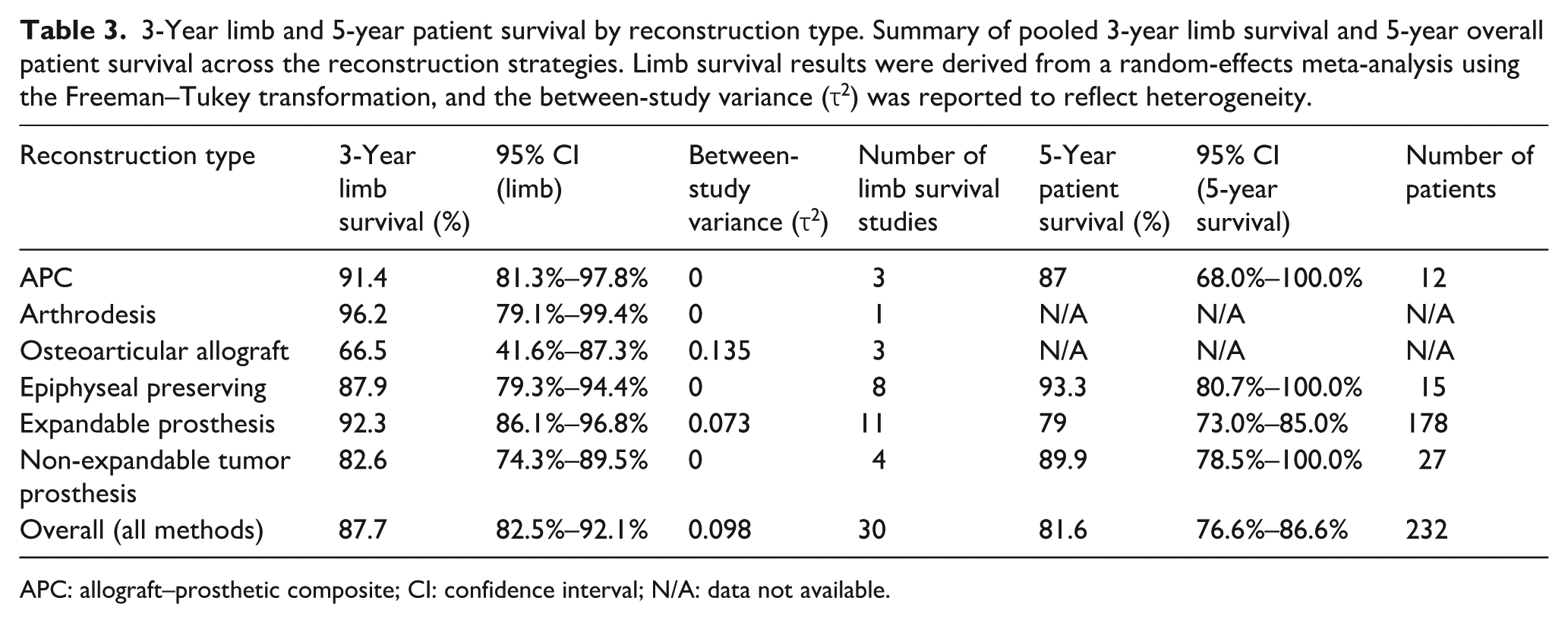
APC: allograft–prosthetic composite; CI: confidence interval; N/A: data not available.
Surgical outcomes and complications
The complication profiles varied substantially according to the reconstruction method. In studies reporting endpoint-specific complications, epiphysis-preserving (joint-preserving) intercalary reconstructions more often had union-related events (delayed/nonunion, graft/construct fracture, hardware failure) than joint-replacing constructs, whereas endoprosthetic reconstructions more commonly demonstrated mechanical/aseptic loosening and component failure.
Infection estimates vary by definition and denominator. Deep infection per patient (Table 4) was 6.7% overall; for expandable systems, it was 4.6% (n = 73). By contrast, the any-infection metric (superficial or deep) reported per construct (Table 5) for expandables was 13.9%. Because these metrics differ, they should not be compared directly. Within the any-infection (per construct) framework of Table 5, pooled estimates were as follows: expandables 13.9%, OAA 11.7%, and APCs 9.0%; these values are descriptive. Lower rates were observed with epiphyseal-preserving reconstruction (7.1%) and non-expandable modular tumor prostheses (6.0%). No infections were reported after arthrodesis, rotationplasty, temporary spacer implantation, or amputation.
Pooled infection rates by reconstruction method. Comparative summary of deep infection rates following distal femoral reconstruction, including pooled percentages, CIs, and sample sizes for each reconstruction method.
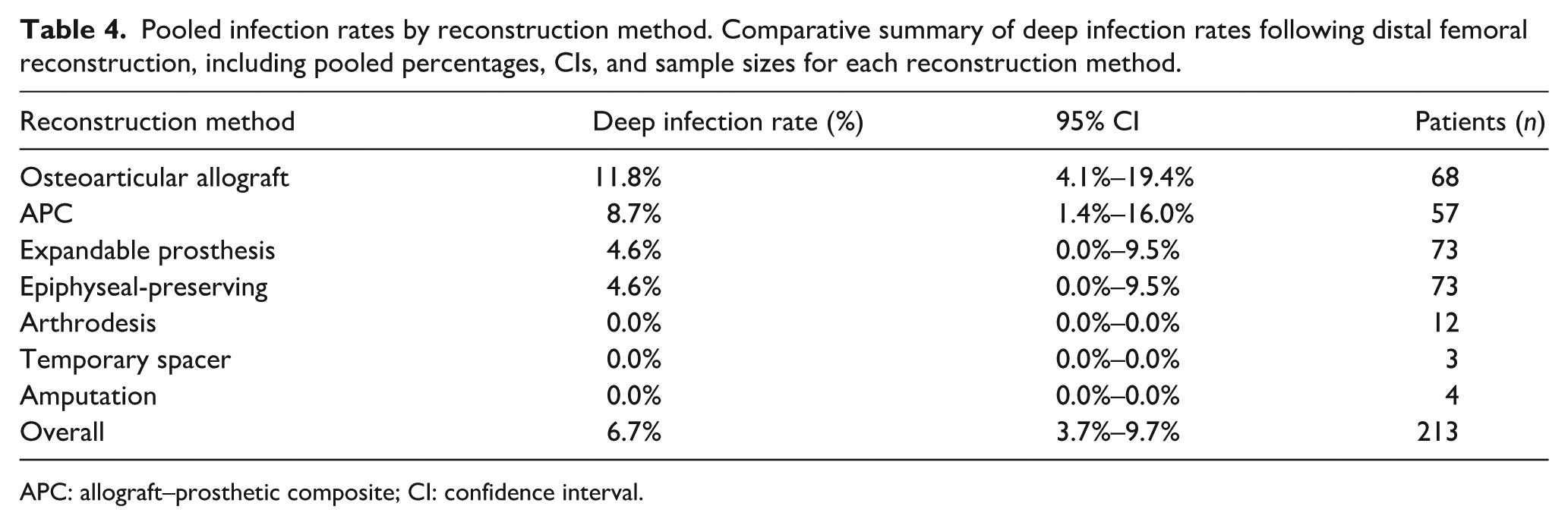
APC: allograft–prosthetic composite; CI: confidence interval.
Detailed surgical complication rates by reconstruction method. Comprehensive summary detailing pooled rates (%) of any-infections (superficial or deep), fractures, reoperations, nonunion, and prosthesis failures across different reconstruction types, highlighting significant differences in complication profiles among methods.
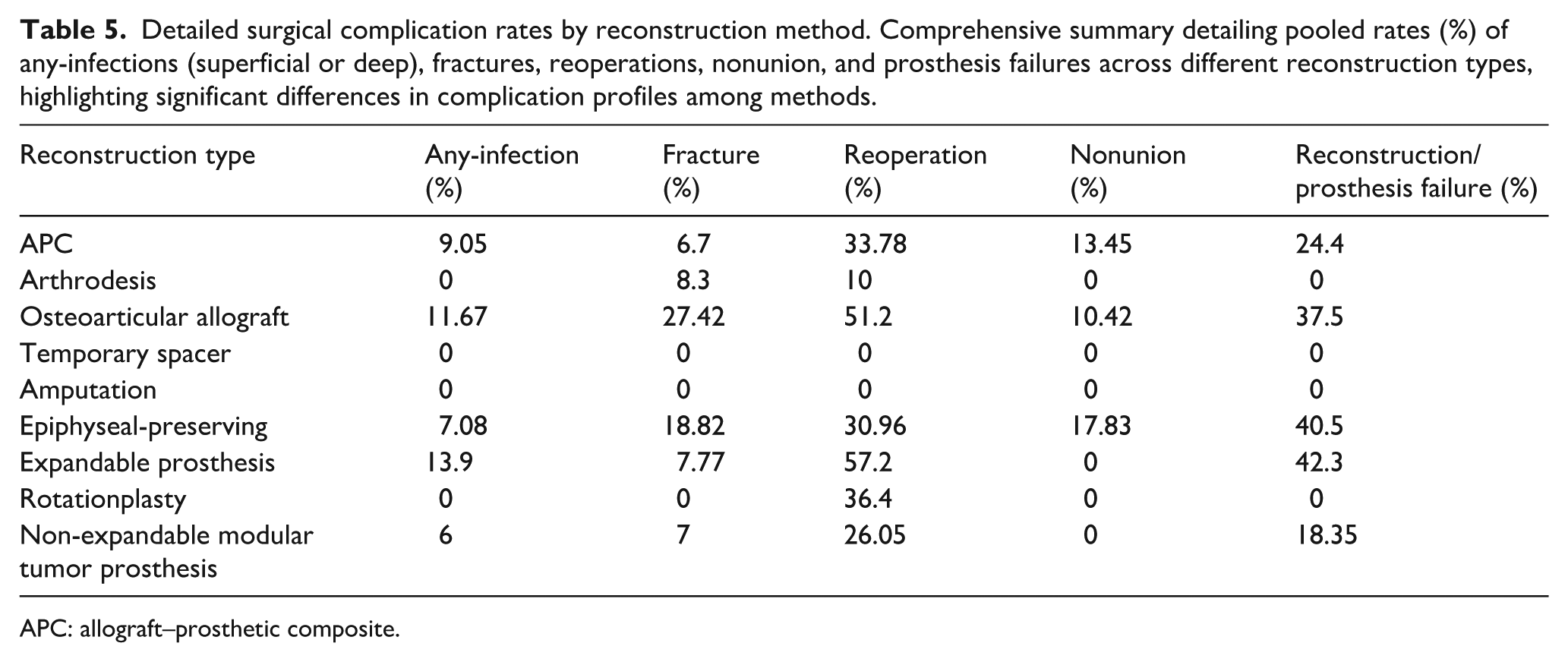
APC: allograft–prosthetic composite.
Mechanical complications were frequent in OAA, including fractures (27.4%), prosthesis failure (37.5%), and nonunion (10.4%). Epiphyseal-preserving reconstructions also showed substantial mechanical issues, including prosthesis failure (40.5%), fracture (18.8%), and nonunion (17.8%). Expandable prostheses had notably high prosthesis failure (42.3%) but comparatively lower fracture rates (7.8%). APC reconstructions demonstrated prosthesis failure (24.4%), nonunion (13.5%), and fewer fractures (6.7%). Arthrodesis exhibited minimal mechanical complications (fractures, 8.3%; prosthesis failure, 0%; nonunion, 0%).
Patterns of reoperation reflected these construct-specific profiles: in biological reconstructions, reoperations predominantly addressed union-related complications (nonunion, graft/construct fracture, hardware failure), whereas in endoprosthetic reconstructions, they more often addressed mechanical or aseptic loosening and component failure (Table 5). Reoperation rates were highest with expandable prostheses (57.2%), followed by OAA (51.2%) and rotationplasty (36.4%). APCs (33.8%) and epiphyseal-preserving reconstructions (31.0%) also required frequent revisions. Non-expandable modular tumor prostheses (26.1%) showed moderate reoperation rates, whereas arthrodesis (10%) showed notably fewer reoperations. No specific complications have been reported in studies on temporary spacers and amputations. A comprehensive summary of infection, mechanical failure, and reoperation rates by reconstruction type is provided in Tables 4 and 5.
Assessment of publication bias
Formal tests were discordant: Egger’s regression did not indicate small-study effects (p = 0.939), whereas Begg’s rank test suggested asymmetry (p < 0.001). These tests rely on different assumptions and have limited power in the presence of heterogeneity, so results should be interpreted cautiously. Duval and Tweedie’s trim-and-fill procedure did not impute additional studies; this finding is supportive but not definitive. Overall, evidence of publication bias is inconclusive. Funnel plots of the main outcomes are shown in Figures 5 and 6.
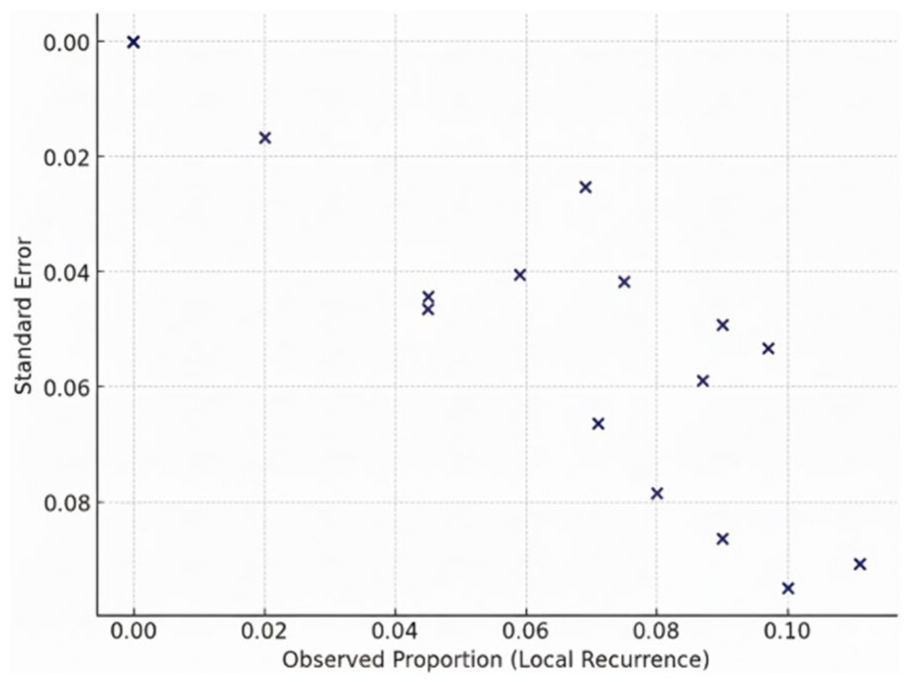
Funnel plot for local recurrence rates. Effect size versus standard error with pseudo-95% confidence limits. The scatter was approximately symmetric around the pooled estimate, suggesting no strong small-study effects. Interpretation remains qualitative and is limited by small k and heterogeneity; the absence of asymmetry does not exclude publication bias.
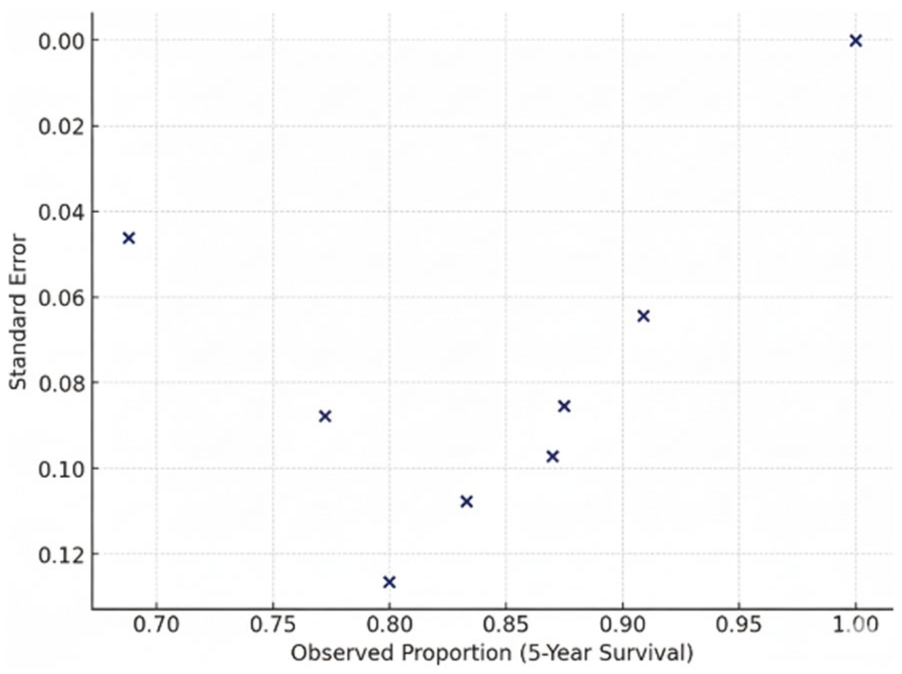
Funnel plot of 5-year overall survival rates. Effect size versus standard error with pseudo-95% confidence limits. The distribution appears to be broadly symmetric, consistent with limited small study effects. Inference is qualitative and underpowered when few studies contribute, and heterogeneity or size-related confounding factors may obscure bias.
GRADE evidence summary
The certainty of evidence assessed using GRADE varied by outcome. LR was rated with high certainty, reflecting consistent findings with narrow CIs. Five-year survival and infection were rated as having moderate certainty due to methodological concerns and imprecision. By contrast, functional outcomes, reoperation rates, and prosthesis (endoprosthetic) failures were supported by low-certainty evidence, driven by substantial heterogeneity, predominantly retrospective designs, and variability in the outcome definitions. A detailed outcome-level GRADE summary is provided in Table 6.
GRADE summary of evidence for major outcomes. Assessment of evidence quality across functional outcomes (MSTS scores), 5-year survival rates, local recurrence, and infection rates using the GRADE approach, clearly indicating the reasons for evidence rating downgrades (risk of bias, inconsistency, indirectness, imprecision, publication bias).


CI: confidence interval; MSTS: Musculoskeletal Tumor Society.
Discussion
This systematic review and meta-analysis provides a comprehensive appraisal of distal femoral reconstruction in children aged <12 years, emphasizing functional outcomes, oncologic safety, and complication profiles. The pooled MSTS score was 24.9 (95% CI, 23.9–25.9), indicating generally favorable postoperative function across reconstruction types, albeit with very high heterogeneity (I2 = 97%). This dispersion likely reflects differences in the surgical era and implant generation, rehabilitation strategies, access to pediatric prosthetics, center- or country-specific practices, and measurement variability (raw 0–30 vs percentage MSTS, assessor, and timing). Accordingly, the pooled values should be read as summaries across diverse settings, not as a single performance benchmark; therefore, the interpretation is descriptive, not comparative.
Within this context, techniques that preserve the native joint and limb length, particularly OAA and APCs, showed mean MSTS scores (≈27/30), consistent with prior reports describing biological joint preservation for optimizing function.56,57 Rotationplasty also yielded consistently high function (24–28/30), with amputation generally reporting lower central estimates, reinforcing its biomechanical advantages despite unique psychosocial considerations.19,21,25,43 Expandable prostheses demonstrated results around (25/30), plausibly influenced by serial lengthening and complication burdens, such as joint stiffness, in line with earlier findings.58–61 Arthrodesis produced scores in the mid-range, reflecting the trade-off between durable structural stability and loss of knee motion, as previously described.24,42,62,63 Given very high heterogeneity (I2 ≈ 97%), these values are descriptive rather than comparative.
LR was consistently low across the reconstruction methods, with a pooled estimate of 5.2% (95% CI, 3.3–7.1). No LRs were reported after OAA or arthrodesis, although these strata were small, and the findings should be interpreted cautiously. Recurrence rates with expandable prostheses (5.2%) and epiphyseal-preserving reconstructions (7.0%) were slightly higher but not statistically significant. These results align with prior evidence that limb-salvage procedures, when performed with appropriate oncologic margins, do not compromise local control compared to amputation.64–66 The pooled 5-year overall survival was 81.6% (95% CI, 76.6%–86.6%), and no significant differences were observed between the reconstruction methods, consistent with the literature indicating that long-term survival in pediatric bone sarcoma is driven primarily by tumor biology and systemic therapy and is largely independent of reconstruction choice.66,67 Accordingly, surgical decision-making in this population should place greater emphasis on functional outcomes, complication risk, and patient-centered priorities rather than oncologic concerns alone.
Three-year limb survival varied across techniques, reflecting the distinct mechanical, biological, and procedural attributes of each technique. The higher survival rate seen with arthrodesis, expandable prostheses, and epiphyseal-preserving reconstructions likely stems from mechanical stability and more standardized operative protocols. Arthrodesis offers structural simplicity, reducing early mechanical failure, whereas the performance of expandable systems reflects advances in implant design and surgical integration. Nevertheless, expendables frequently encounter mechanical and soft-tissue issues and often require reoperations, raising concerns regarding their long-term durability. By contrast, lower limb survival observed with OAA is driven by biological constraints, notably graft resorption, nonunion, and fracture risk, especially in younger children with limited host bone. Considerable heterogeneity across studies suggests variability in surgical expertise and postoperative management. Because reporting limitations necessitated a 3-year endpoint, the pooled analysis may have underestimated the later failure burden. Future studies should consistently report 3-year limb survival as a pragmatic early- to mid-term metric, enabling clearer comparisons and a more complete understanding of durability challenges across reconstruction strategies.
Substantial variability in the complication profiles was observed across the reconstruction methods. OAA had the highest overall burden, with fracture 27.4%, nonunion 10.4%, prosthesis/construct failure 37.5%, and reoperation 51.2%. APCs likewise showed considerable complication rates; prosthesis failure 24.4% and reoperation 33.8%, reflecting the technical complexity and biological demands of these procedures.38,44,68–70 Expandable prostheses also demonstrated notable complication rates, consistent with concerns about mechanical durability and the need for multiple interventions over time.58,71,72 Complications are particularly evident in expandable designs, which are either invasive (requiring surgery for lengthening) or noninvasive (electromagnetically actuated). In a systematic review of noninvasive expandable endoprostheses (NIEPRs), the revision rate was 46.2% for implant failures, including maximal lengthening with persistent limb-length discrepancy (10.4%), failed extension mechanisms (6.1%), prosthesis fractures (7.7%), hinge fractures (1.4%), and bushing wear (0.9%); additionally, 19.2% of patients had >20 mm limb-length discrepancy at final follow-up. In our meta-analysis of expandable prostheses (mainly invasive or mixed), reoperation (57.2%) and mechanical failure (42.3%) were observed, indicating shared durability issues, although NIEPRs may mitigate soft-tissue and infection morbidity. Despite favorable functional outcomes (mean MSTS 85.1% (≈25.5/30) in NIEPRs vs 25.14/30 in our cohort), both systems face mechanical challenges that warrant ongoing refinement to reduce revisions and improve limb-length equality in pediatric patients.4,73 By contrast, arthrodesis and amputation were associated with minimal complication rates, underscoring their potential utility in selected scenarios, particularly when minimizing reoperation risk is paramount or resource constraints limit access to complex reconstructions. 74 The reoperation pattern across methods followed construct logic: biological reconstructions were predominantly revised for union-related complications (nonunion, graft/construct fracture, hardware failure), whereas endoprosthetic reconstructions more commonly required revision for mechanical or aseptic loosening and component failure (Table 5). Finally, because small studies and selective reporting can preferentially capture positive or incomplete results, especially for complication subtypes, these subtype rates should be considered lower-bound estimates and interpreted with appropriate caution.
Our findings underscore a practical trade-off: techniques that maximize function, particularly joint-preserving biological reconstructions and rotationplasty, carry a higher risk of union-related or reconstructive complications, whereas options with fewer complications, such as arthrodesis, restrict motion and alter gait. Procedure selection should be personalized through a multidisciplinary discussion (orthopedic oncology, oncology, rehabilitation/prosthetics, nursing, psychology) that integrates (i) tumor factors (margin requirements, defect size, physeal involvement, soft-tissue status), (ii) patient factors (age and remaining growth, activity goals, rehabilitation capacity, psychosocial readiness), and (iii) system factors (infection risk, access to prosthetic services, feasibility of reoperations, and follow-up). In general, biological reconstructions are preferred when joint preservation and long-term function are priorities and reliable union/rehabilitation is feasible. Rotationplasty offers durable, high function for very young patients with large resections or when prosthetic longevity is a concern, but it requires careful counseling. Arthrodesis provides stability with a lower complication risk when soft tissue compromise, infection risk, or limited resources preclude more complex options. Non-expandable modular tumor prostheses are suitable for patients nearing skeletal maturity who have access to revision care, whereas expandable prostheses address anticipated limb-length discrepancies at the cost of higher reoperation rates. Given these trade-offs and the heterogeneous evidence base, our pooled estimates are offered as decision support to facilitate shared, individualized choices, rather than prescriptive comparisons.
Rotationplasty can deliver excellent function, but its visible limb differences may affect body image and social adaptation, particularly in children. Long-term QoL is generally favorable once rehabilitation is established, although early adjustment varies with psychological readiness, family support, and access to experienced pediatric prosthetic teams. 75 We recommend structured preoperative counseling, including images/videos and peer-mentor contact, along with the involvement of psychology/child-life and social work teams, coordinated school re-entry planning, and staged exposure to mitigate appearance-related concerns. 76 When cosmetic acceptability is low or durability with fewer reoperations is prioritized, arthrodesis may be preferred. Because QoL instruments were heterogeneous across studies, psychosocial outcomes were synthesized narratively to support shared, age-sensitive decision-making. 75
Several methodological limitations should be considered when interpreting the findings. First, the available data were markedly heterogeneous, which made it difficult to extract clean and consistent information specific to distal femoral reconstruction in children aged <12 years. A major source of variability was the inconsistent definition and reporting of key outcomes, particularly that of treatment failure. Across studies, the term “failure” has variously encompassed prosthetic loosening, mechanical complications, bone fractures, or nonunion, limiting uniform analyses and precluding direct comparisons.
To address this, we used implant/reconstruction failure as an umbrella descriptor and reserved endoprosthetic failure for joint replacement constructs. In endoprostheses, failure typically includes aseptic loosening, instability/dislocation, component breakage, and periprosthetic fracture, whereas in biological reconstructions (e.g., allograft/APC), it encompasses nonunion, graft/construct fracture, collapse, or resorption. Because primary reports were inconsistent in defining composite failure, we prioritized component complications and presented 3-year limb survival as a reconstruction-level durability anchor. Consequently, the comparisons should be interpreted with caution. In particular, strata with small samples (e.g., joint fusion/arthrodesis and amputation) are underpowered and imprecise, yielding wide intervals and low certainty; any apparent differences are exploratory rather than confirmatory findings.
All included studies were retrospective, introducing the risk of selection bias and reducing the overall level of evidence. The substantial heterogeneity observed in functional outcomes likely reflects differences in patient characteristics, reconstruction techniques, follow-up duration, rehabilitation protocols, and outcome assessment tools. Although statistical testing suggested minimal publication bias in the primary outcomes, under-reporting, especially of minor complications and reoperations, remains plausible.
Improving the evidence base will require prospective designs, standardized definitions (particularly for complications and failure), and uniform reporting of functional, oncologic, and surgical outcomes. Such consistency is essential for strengthening data integrity and supporting evidence-based decision-making in pediatric musculoskeletal oncology.
This review provides important insights into the comparative effectiveness and complication profiles of available distal femoral reconstruction strategies in skeletally immature children. No single method is universally optimal; reconstruction decisions should be individualized based on clinical and anatomic factors, psychosocial context, and resource considerations of the patient. A nuanced understanding of these variables allows clinicians to tailor strategies to each child’s functional goals, growth, and QoL.
Future research should close key gaps through well-designed comparative studies that track long-term functional and psychosocial outcomes, particularly rotationplasty versus contemporary expandable prosthesis. Head-to-head evaluations of noninvasive and invasive expandable implants are needed to clarify their relative benefits and trade-offs. Finally, the systematic use of validated patient-reported outcome measures (PROMs) is crucial for capturing QoL and psychosocial domains, thereby strengthening the foundation for patient-centered decision-making in pediatric orthopedic oncology.
Conclusion
This systematic review and meta-analysis highlights the complexity and individualized nature of reconstruction after distal femoral tumor resection in young children. Limb-salvage options, including OAA, APCs, rotationplasty, and expandable prostheses, achieve functional outcomes that are comparable to, and in some cases exceed, those after amputation. Because each technique carries a distinct profile of risks, benefits, and long-term considerations, decisions should be made through a multidisciplinary process that integrates functional potential, patient and family preferences, psychosocial context, and clinical scenarios.
All included studies were retrospective cohorts with susceptibility to selection, confounding, and reporting biases; accordingly, the GRADE certainty was predominantly low to moderate. Therefore, pooled estimates should be interpreted cautiously and used to support shared decision-making, not to assert comparative superiority. To strengthen the evidence base, prospective multicenter studies with standardized outcomes and reporting, consistent outcome definitions, and greater inclusion of PROMs are needed. Emphasizing long-term function, QoL, and patient-centered goals is essential to advance evidence-based, individualized care for this vulnerable population.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251398665 – Supplemental material for Functional and oncological outcomes of distal femoral reconstruction in young children: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-cho-10.1177_18632521251398665 for Functional and oncological outcomes of distal femoral reconstruction in young children: A systematic review and meta-analysis by Khodamorad Jamshidi, Bushra Zareie, Mehrdad Mokhtari and Seyyed Saeed Khabiri in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
The authors gratefully acknowledge the support and resources provided by the Joint Reconstruction Research Center, Tehran University of Medical Sciences, and the Bone and Joint Reconstruction Research Center, Iran University of Medical Sciences. Their technical and administrative assistance was invaluable to the completion of this work.
Author contributions
Conceived and designed the analysis: Khodamorad Jamshidi, Mehrdad Mokhtari, and Seyyed Saeed Khabiri. Collected the data: Bushra Zareie, Mehrdad Mokhtari, and Seyyed Saeed Khabiri. Contributed data or analysis tools: Bushra Zareie, Mehrdad Mokhtari, and Seyyed Saeed Khabiri. Performed the analysis: Bushra Zareie and Seyyed Saeed Khabiri. Wrote the article: Khodamorad Jamshidi, Mehrdad Mokhtari, and Seyyed Saeed Khabiri.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study did not involve human participants or animals; therefore, ethical approval was not required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Writing assistance and third-party submissions
No external writing or editing assistance was received, and this article was prepared and submitted solely by the listed authors.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.