
Abstract
Objectives:
To identify lifestyle-related risk factors for growing pains to advance the clinical prevention and management strategies.
Methods:
A case–control study was conducted from September 2023 to December 2024, enrolling 290 children clinically diagnosed with growing pains (case group) and 467 age-matched healthy controls. All participants underwent detailed medical history reviews, physical examinations, imaging examination, and laboratory tests. The main data were collected through structured questionnaires administered to both groups.
Results:
The results of univariate analysis showed that factors related to growing pains included maternal exposure to smoking environments, child exposure to smoking environments, preference for vegetables, grains, tubers, legumes, and fruits, sports preference, extreme fatigue after exercise, sleeping with parents at night, fear of sleeping alone, sleep latency between 15 and 30 min, sleep latency between 30 and 60 min, and average waking up twice per night (p < 0.050). Multivariate analysis indicated that maternal near-daily exposure to smoking during pregnancy (p = 0.042, odds ratio = 1.926), sleep latency between 30 and 60 min (p < 0.001, odds ratio = 3.696), and extreme fatigue after exercise (p = 0.015, odds ratio = 15.554) were independent risk factors for the occurrence of growth pain. On the other hand, legume preference (p = 0.001, odds ratio = 0.442) and sports preference (p = 0.009, odds ratio = 0.486) were protective factors against the occurrence of growth pains.
Conclusions:
Frequent maternal smoking exposure during pregnancy, prolonged sleep latency (30–60 min), and post-exercise exhaustion are independently associated with a higher prevalence of growing pains. And the preference for legumes and participation in sports were associated with a lower prevalence of growing pains.
Significance of Study:
The preference for legumes and participation in sports were associated with a lower prevalence of growing pains.
Introduction
Growing pains, a non-inflammatory childhood pain syndrome, commonly affect children aged 4–6 years, with prevalence rates ranging from 2.6% to 36.9%.1,2 Growing pains frequently cause distress for both children and parents and may result in affected children being overlooked or misdiagnosed in orthopedic clinics. 3 In recent years, lower limb growing pains have become a common reason for pediatric orthopedic outpatient visits, accounting for up to 30% of cases. 4 The lack of a clear cause or solution leads many children and parents to repeatedly seek medical care, resulting in a strain on medical resources and an increased burden on families. Therefore, growing pains represent an important issue in the field of pediatric orthopedics, and finding a solution to this problem holds significant clinical importance for alleviating the suffering of affected children.
Etiological research plays a crucial role in the prevention, diagnosis, and treatment of diseases. Currently, many studies have delved into the potential causes of growing pains, but different researchers hold varying perspectives on its etiology, including the theory of perinatal risk factors, 5 low pain threshold, 6 blood flow perfusion, 7 joint hypermobility, 8 reduced bone strength, 9 vitamin D deficiency, 10 hereditary factors, 11 among others. However, there has been less attention paid to the relationship between the characteristics of growing pains and potential lifestyle-related influencing factors. Therefore, this study aims to investigate lifestyle-related risk factors for growing pains through a questionnaire survey. The goal of this study is to identify environmental factors found to be associated with the occurrence of growing pains.
Methods
The study was conducted following the Declaration of Helsinki and approved by the Institutional Review Board of our institution. All participants and their parents gave their informed consent for inclusion before filling out the questionnaire.
Participants
Children diagnosed with growing pains in the orthopedic clinic of our hospital from September 2023 to June 2024 were selected as the case group. At the same time, children with normal school physical examination results within the same age range were collected as a control group.
Diagnostic protocol for growing pains
The diagnosis of growing pains is made based on the diagnostic criteria of Peterson 12 or Walters et al. 13 combined with clinical manifestations, medical history, and physical examination. Patients with suspected growing pains underwent a standardized evaluation: (1) clinical history and physical examination to exclude conditions such as swelling, infection, range of motion deficits, gait abnormalities, and musculoskeletal impairments; (2) laboratory tests to exclude conditions such as inflammation, rheumatologic disorders; (3) imaging (X-ray, ultrasound, magnetic resonance imaging) to exclude conditions such as tumor, fracture, etc.
Inclusion and exclusion criteria
Patients must satisfy at least four out of the seven items listed in criterion a. Furthermore, they must fulfill all of the following criteria: b, c, d, and e. (a): (1) pain typically occurs late in the day or during the night and disappears in the morning; (2) pain is intermittent with some pain-free days and nights; (3) typical distribution of pain in the anterior part of the thigh, calf, and posterior part of the knees, and (4) usually in both legs; (5) pain localized in the areas outside the region of joints; (6) there is no limitation of mobility and no limping; (7) pain is not associated with local trauma, infection, tenderness, erythema, and swelling; and (b) the results of physical examination, laboratory tests (see Supplemental Material), and imaging examination are normal. (c) Children aged between 3 and 18 years. (d) Both children and caregivers were able to speak and understand. (e) Caregivers can fill out the questionnaire through mobile phones. The exclusion criteria were as follows: (a) children with serious diseases (e.g., cancer); (b) children or caregivers with impaired cognitive capability and judgment; and (c) caregivers unable to fill out the questionnaire through mobile phones. 2 The diagnostic protocol for growing pains is shown in Figure 1.
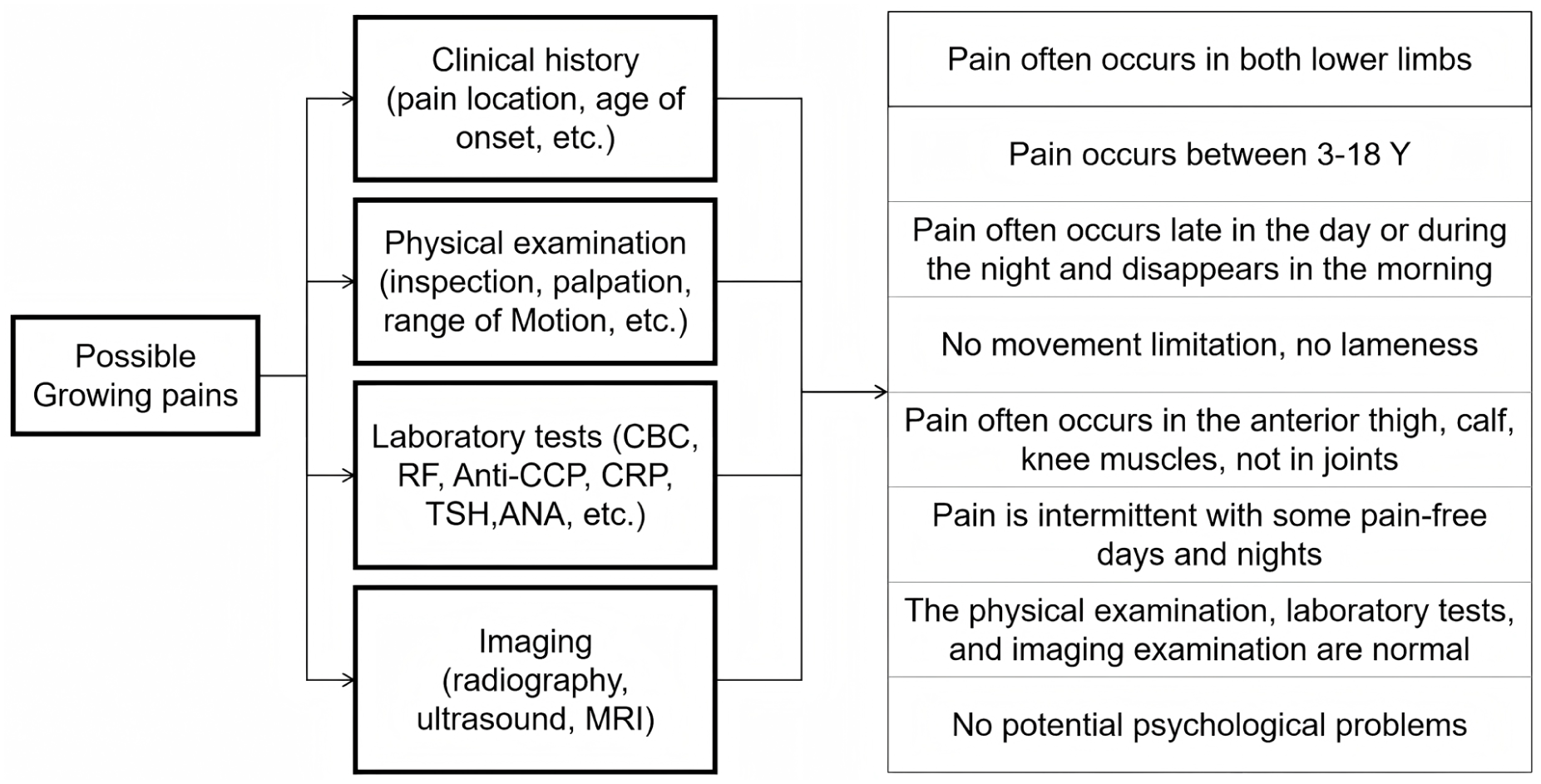
The protocol for evaluating children with possible growing pains.
Questionnaire design and content validity
According to the previous study questionnaire 14 and the characteristics of Chinese children, the questionnaire on growing pains was formulated. Since this questionnaire is non-scales-based, content validity indices (CVI) were used to assess its effectiveness. 15 After the initial draft of the questionnaire was designed, three pediatric orthopedic experts, two child health care experts, and one statistics expert were invited to score the relevance of each item to the corresponding content dimensions, screening out items with CVI <0.78. Subsequently, overall content validity was evaluated, and the internal validity assessed by experts was 0.90, meeting the required conditions for the survey.
Questionnaire survey process
Questionnaires were completed by the primary caregiver most familiar with the child’s condition, typically either parent (mother or father). And then we collected the following information through the online questionnaire platform:
General information and perinatal factors
Age, sex, weight, height, delivery method, prematurity, frequency of maternal exposure to smoking environment during pregnancy, frequency of maternal alcohol consumption during pregnancy, frequency of child’s current exposure to smoking, history of lower limb trauma or surgery, and history of underlying diseases.
Lower-extremity pain-related conditions
Pain location, pain intensity, pain type, time since initial onset, pain side, frequency of pain onset, pain onset regularity, pain onset time, the average duration of each pain session, child sensitivity to pain, abnormal lower limbs alignment, whether children have abnormal gait, how to handle the leg pain, the influence of pain on daily life, and the influence of pain on movement function.
Lifestyle-related factors
The lifestyle pattern-related data of children, including dietary habits, sports habits, and sleep habits.
Statistical analysis
Data were processed using R version 4.4.0 (The R Foundation, April 24, 2024). Measurement data with normal distribution were expressed as mean ± standard deviation, and the independent sample t-test was used for comparison between two groups, ANOVA for comparison between multiple groups, and the nonparametric test when variance was not uniform. Measurement data with a non-normal distribution are expressed as median, using the U or H test. The kappa coefficient was calculated by the chi-square test for count data, and the Spearman coefficient was calculated by correlation analysis for rank. The chi-square test was used for the data of the component ratio, and Fisher’s exact probability test was used for the data that did not meet the chi-square test condition. The propensity score matching was employed to mitigate selection bias and potential confounding effects by adjusting for differences in baseline characteristics between the two groups. The propensity score matching was conducted using a 1:1 ratio and the caliper matching method, with logistic regression used to calculate the propensity scores. Covariates such as gender and age were included in the propensity score calculation. Multiple sample non-parametric tests were used for rank variable data in counting data, and the t-test was used for two-sample mean data. A multivariable ordinal logistic regression model was used to explore the association between growing pains and its related variables. The stepwise method was adopted for variable screening. Results were expressed as odds ratios (ORs) and 95% confidence intervals (CIs), with statistical significance defined as a p value of <0.05.
Results
From September 2023 to December 2024, 312 questionnaires were gathered from the children’s legal guardians. After excluding 22 invalid questionnaires due to issues such as brief completion time, excessive answer repetition, incomplete responses, and clear logical errors, 290 questionnaires remained, resulting in a response rate of 92.9%. In the control group, a total of 518 questionnaires were collected, and after excluding 51 invalid questionnaires for similar reasons, 467 questionnaires were retained, yielding a response rate of 90.2%.
Statistics of demographic and clinical characteristics
In this study, the clinical characteristics of 290 growing pains, including 156 boys (53.7%) and 134 girls (46.3%), had a mean age of 7.31 years (7.31 ± 1.92, range = 3–12 years). The 6-year-old group had the highest proportion of 20.3%. Pain distribution analysis revealed that the anterior left knee was the most frequently reported site (45.9%), closely followed by the anterior right knee (44.1%). The majority of children reported pain primarily localized in the anterior knee region, with secondary involvement of the anterior leg. The statistics of the pain sites are shown in Figure 2.
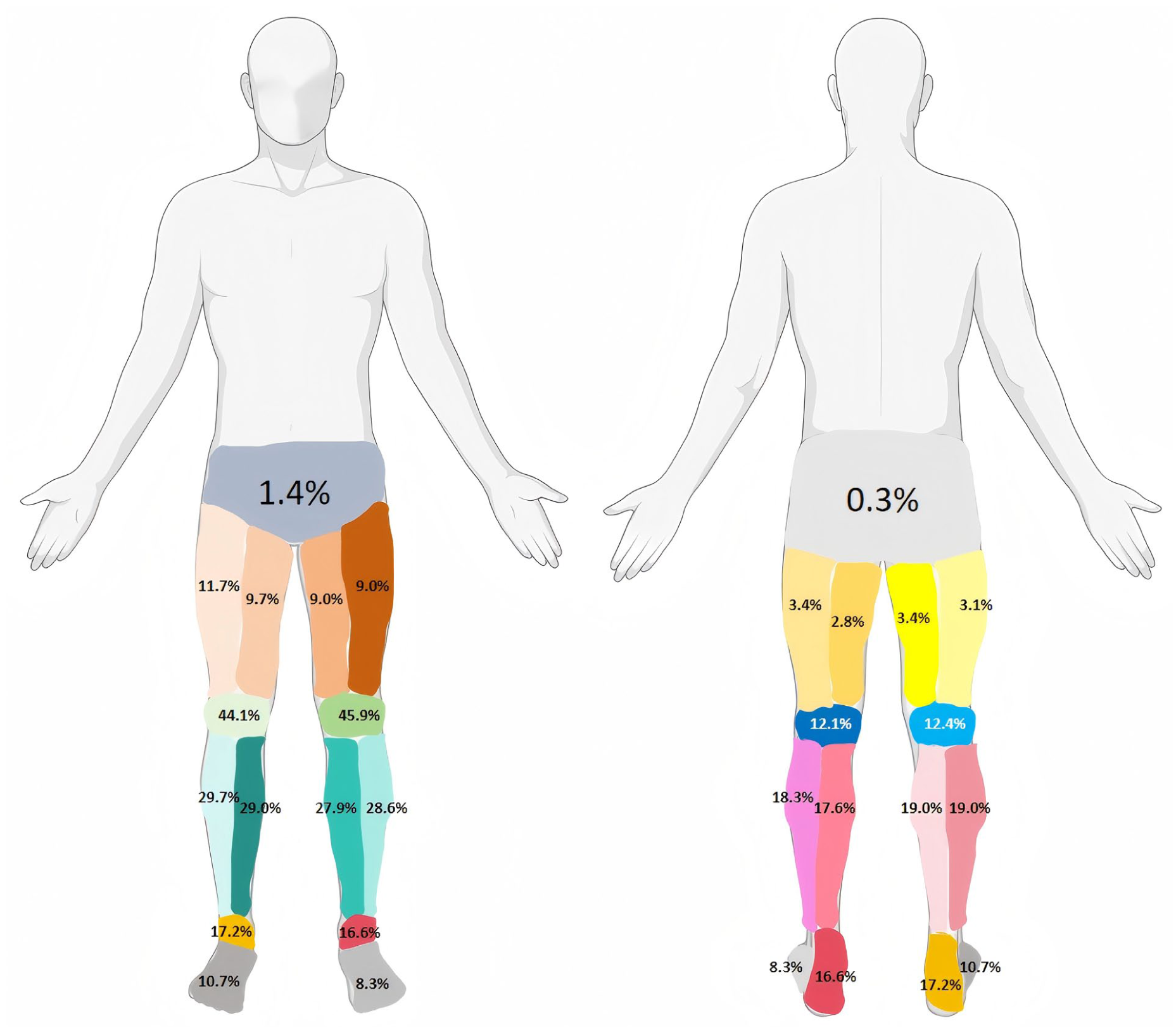
Distribution of the lower-extremity pain sites. The image uses different colors and percentages to indicate the areas where pain occurs.
The study findings on pain characteristics in children revealed that 32.0% experienced lower limb pain persisting for over 1 year. Temporal patterns showed that 41.0% reported worsening of pain at night, while 25.0% described their pain as irregular. Pain distribution analysis indicated bilateral involvement in 49.0% of cases, with right-sided predominance in 25.9% and left-sided predominance in 25.1%. Regarding pain duration, 54.0% of children reported episodes lasting less than 15 min, while 11.7% experienced prolonged episodes lasting over an hour. The frequency of pain episodes varied, with 27.6% of children reporting one to two episodes per month and 26.6% experiencing one to two episodes every 6 months.
Pain characterization analysis indicated that 42.8% of children described their symptoms as dull ache, while 41.7% reported soreness accompanied by a distending sensation. A minority (5.2%) found their pain difficult to characterize. Evaluation of pain intensity using a visual analog scale (ranging from 1 to 10) revealed a predominant distribution of scores between 2 and 6, with the highest proportion at 4 points (17.9%). Notably, 41.7% of children engaged in vigorous physical activity before the onset of pain. Family-related data revealed that 61.7% of relatives expressed concern about the condition, and 16.6% reported familial occurrence among first-degree relatives (parents or siblings). Physical examination findings demonstrated that 11.7% of children presented with lower limb deformities, including the genu varum and genu valgum. In addition, 12.8% exhibited an in-toeing gait pattern, and 3.8% had flat feet.
Before visiting the hospital, 43.1% of children believed massage could alleviate pain, while 25.9% thought self-relief was possible without treatment. Among them, 46.6% did not have any examination, while 39.7% of children received imaging examination, and 36.6% underwent routine blood and biochemical tests. After seeking medical treatment, 66.2% of the children were treated by resting the affected limbs, while 36.9% of the children had calcium supplements and vitamin D supplements. No child was treated with analgesic medication.
Risk factor analysis of growing pains
Before the propensity score matching, the distribution of age and sex was significantly different between the growing pains group and the control group. After propensity score matching, each group contained 242 subjects, and there was no significant difference in the distribution composition of each variable between the two groups (Table 1).
Propensity score matching.
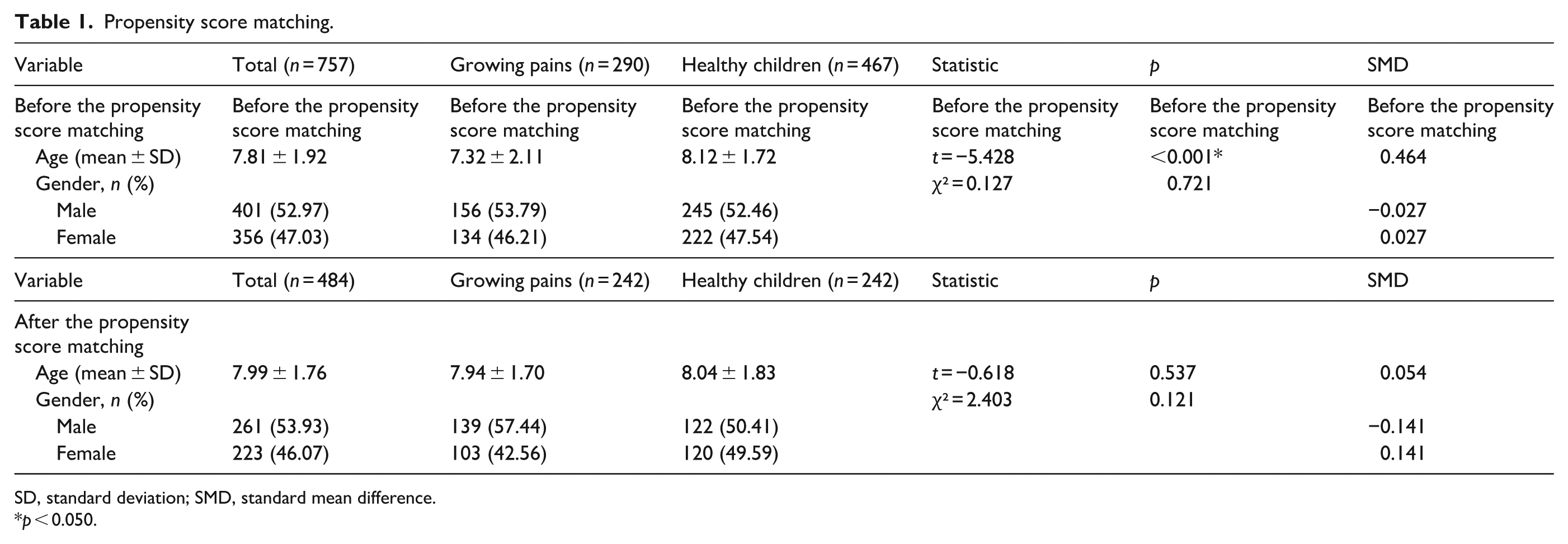
SD, standard deviation; SMD, standard mean difference.
p < 0.050.
Univariate analysis showed that the factors related to the occurrence of growing pains included maternal exposure to smoking at least once a week during pregnancy (p = 0.007), maternal exposure to smoking environments almost every day during pregnancy (p = 0.002), children exposure to smoking environments almost every day (p < 0.001), and none of the remaining items showed any statistical differences (p > 0.050). In terms of dietary habits, vegetable preference (p = 0.001), grain preference (p = 0.001), tuber preference (p = 0.002), legume preference (p < 0.001), and fruit preference (p = 0.009) were associated with growing pains, and there was no statistical difference in the other items (p > 0.050). In terms of sports performance, sports preference (p = 0.003) and extreme fatigue after exercise (p = 0.014) were associated with growing pains, and there was no statistical difference in the other items (p > 0.050). In terms of sleeping habits, sleep with parents at night (p <
Univariate analysis of the association of growing pains and lifestyle-related factors.
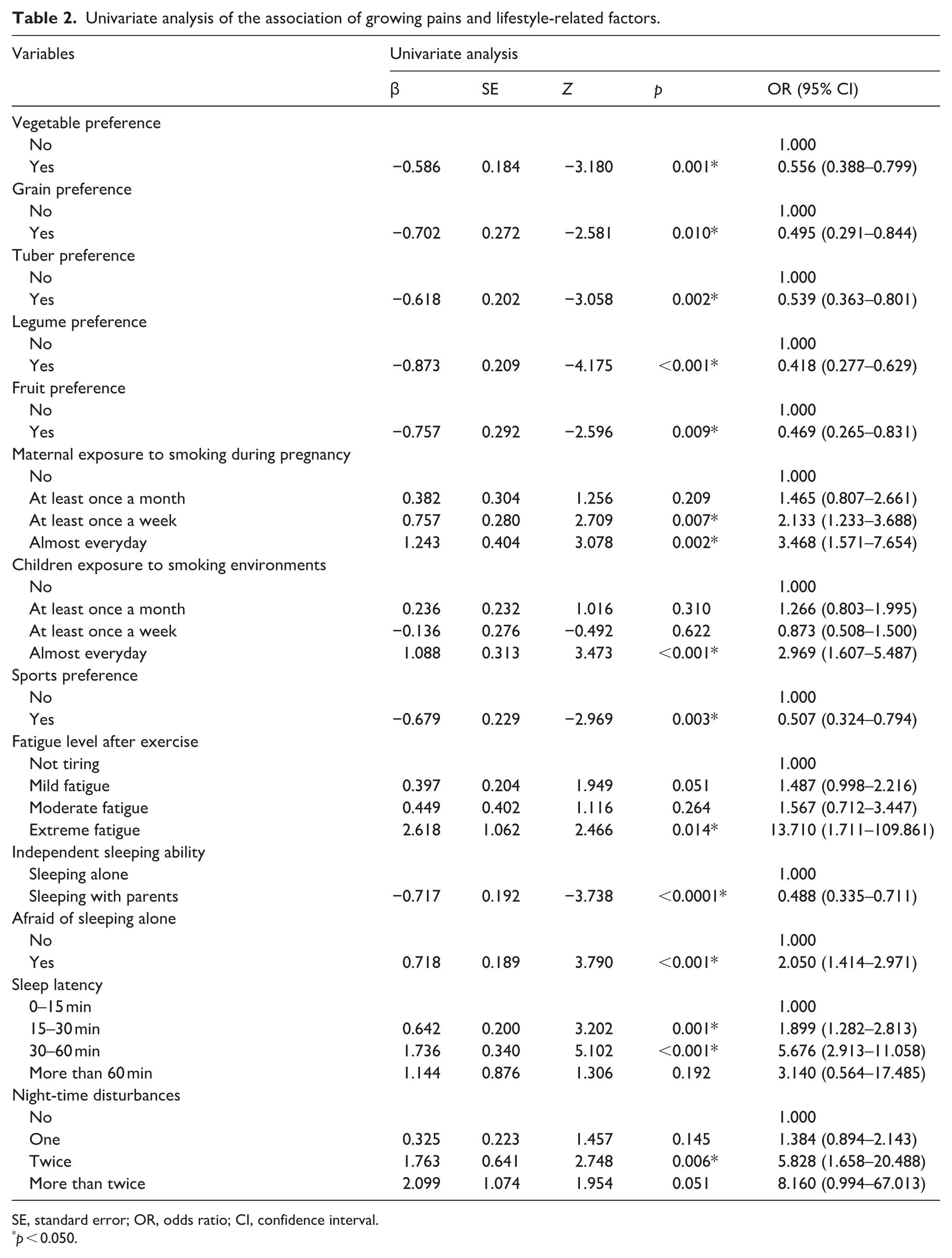
SE, standard error; OR, odds ratio; CI, confidence interval.
p < 0.050.
Multivariate analysis indicated that maternal near-daily exposure to smoking during pregnancy (p = 0.042, OR = 1.926), sleep latency between 30 and 60 min (p < 0.001, OR = 3.696), and extreme fatigue after exercise (p = 0.015, OR = 15.554) were independent risk factors for the occurrence of growth pain. On the other hand, legume preference (p = 0.001, OR = 0.442) and sports preference (p = 0.009, OR = 0.486) were protective factors against the occurrence of growth pains (Table 3).
Results of the multivariate analysis.
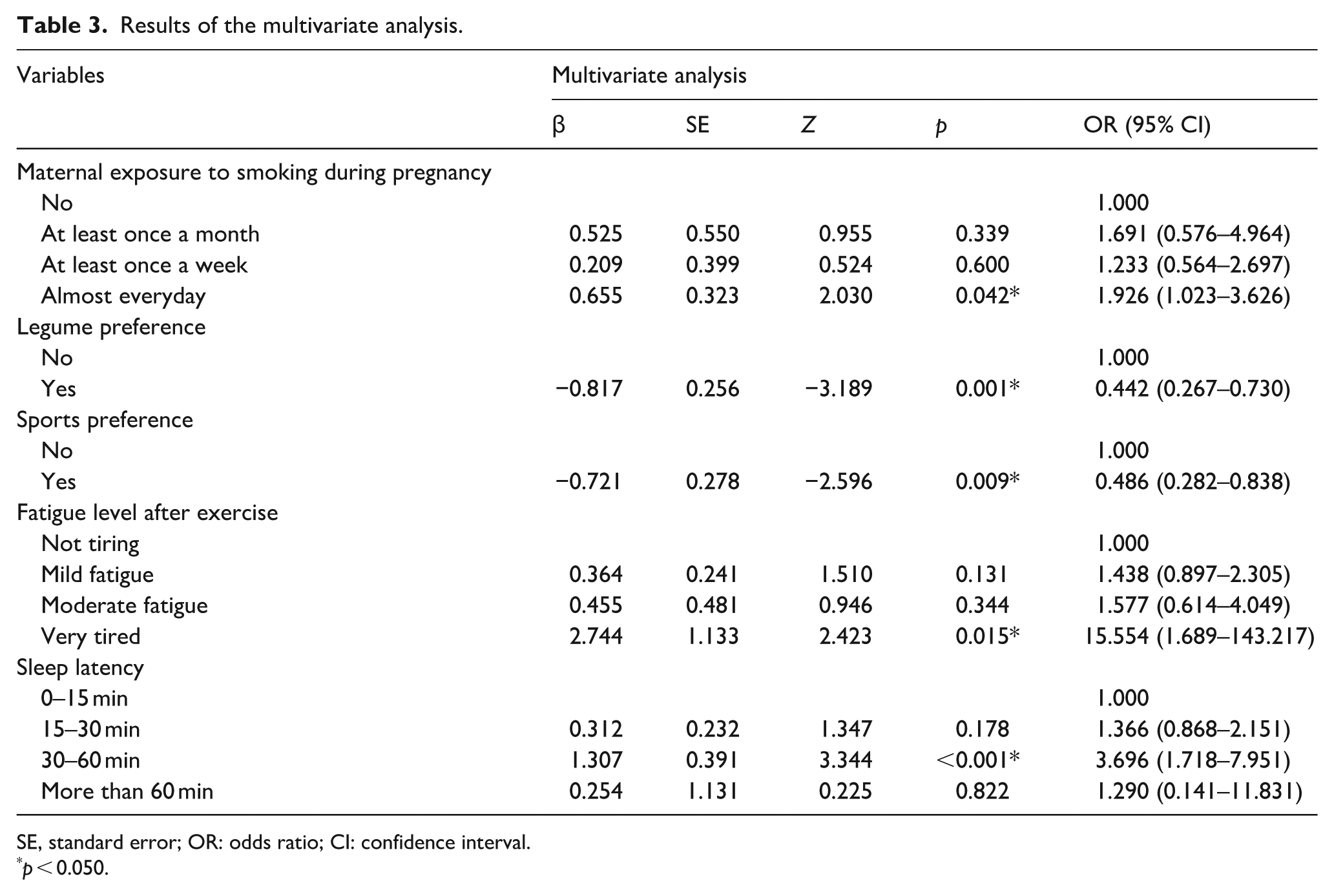
SE, standard error; OR: odds ratio; CI: confidence interval.
p < 0.050.
Discussion
Previous studies report that growing pains primarily affect the thighs and calves (75% of cases), with knee pain being most common (63.85%), followed by lower leg (54.11%) and ankle (25.84%). Hip involvement is rare (2.7%).2,16,17 Our study aligns with these observations. Growing pains predominantly occur at night (74%–81%).16,18 Our data similarly indicate that 47.1% of children experience pain predominantly during late-night hours. Although growing pains typically occur at night, daytime manifestations are possible. Therefore, daytime pain cannot be definitively excluded as growing pains. Bilateral pain was most common (49%), and most episodes (74.8%) lasted <15 min, aligning with previous reports. 2
Meanwhile, the etiology of growing pains remains unclear.19,20 Thus, this study aims to identify potential risk factors, thus allowing the generation and promotion of preventive measures. Among various risk factors, smoking is a key risk factor for chronic musculoskeletal pain, affecting areas like the neck, back, knees, and other joints. 21 Consequently, secondhand smoke exposure warrants consideration as a potential risk factor for growing pains. Both maternal smoking during pregnancy and childhood secondhand smoke exposure increase growing pains risk, 22 with a dose-dependent effect on musculoskeletal pain severity. 23 Our analysis showed maternal smoking during pregnancy significantly increased growing pains risk However, some studies have failed to establish a significant association between perinatal maternal smoking and growing pains. This discrepancy may be attributed to variations in the quantification of secondhand smoke exposure across different studies.
Research investigating the relationship between diet and growing pains remains limited. Our multivariate analysis identified legume consumption as an independent protective factor against growing pains. Legumes play a significant role in bone health maintenance. 24 Soy isoflavones exhibit protective effects against postmenopausal osteoporosis, 25 and soy protein can preserve mechanical bone strength. 26 Meanwhile, Various legumes significantly enhance osteocalcin levels in ovariectomized female mice. 27 These findings supported the bone strength theory of growing pains. 9 Kaspiris et al. 5 indicated that perinatal factors influencing bone strength are associated with growing pains, suggesting that legume consumption may exert protective effects through bone strength enhancement. The therapeutic potential of calcium supplementation in growing pains, as demonstrated by Simon et al., 28 and the observation by Li et al. 29 of significantly lower serum calcium and phosphorus levels in patients with growing pains provide additional mechanistic insights. Future research should differentiate between various legume types and their processed forms, such as fermented soybean products. Our clinical observations also suggest a potential role for dietary fiber in growing pains prevention. Previous literature demonstrates significant associations between higher dietary fiber intake and increased bone mineral density across all fiber subtypes. 30 And the women with high childhood consumption of fiber-rich vegetables and fruits exhibit greater bone mineral density. 31 While our univariate analysis revealed differences in the preference of vegetables, grains, fruits, and tubers between groups, these factors did not emerge as independent risk factors in multivariate analysis. Future investigations should consider stratifying dietary fiber intake levels to better elucidate the dose–response relationship between fiber consumption and growing pains incidence.
The relationship between physical activity and growing pains remains controversial partly. The fatigue theory suggests growing pains result from muscle overuse, 32 though this only partially explains the clinical manifestations of growing pains. Our findings indicate that exercise preference serves as a protective factor against growing pains, while excessive post-exercise fatigue emerges as a significant risk factor. Consistent with existing evidence, structured training improves muscular endurance and delays fatigue. 33 We hypothesize that children with regular sports habits develop greater muscular tolerance compared to sedentary children, potentially explaining their reduced susceptibility to nocturnal pain following daytime activity. These results align with prior findings that structured physical activity reduces pain incidence. 6 The association between excessive post-exercise fatigue and growing pains may reflect activity levels exceeding normal muscular capacity, potentially triggering nocturnal lower limb pain. However, this hypothesis requires further validation through objective measures such as electromyographic assessment.
In addition, growing pains have also been found to be associated with sleep disorders. Naish and Apley 34 found that children with growing pains showed irritability, nervousness, and fear of darkness. And our study found that the fear of sleeping alone is more likely to appear in the group of children with growing pains. Wong et al. 35 found that the periodic limb activity index of growing pains during sleep was significantly higher, which may influence their sleep quality. Lack of sleep can lead to increased sensitivity to pain, which, in turn, can increase pain perception the next day. 36 While univariate analysis identified co-sleeping with parents as significantly associated with growing pains, this association did not persist in multivariate modeling after adjusting for covariates. Co-sleeping with parents may indirectly influence growing pains by affecting sleep latency rather than being a direct cause, which may explain its exclusion in the multivariate analysis. However, further experiments are needed to verify this. Our study identified prolonged sleep latency (30–60 min) as a significant correlate of growing pains. Currently, pediatric sleep disorders lack standardized latency thresholds due to age-dependent variations in sleep patterns, 37 complicating the establishment of causal relationships with growing pains. Future research should prioritize investigating how sleep quality metrics influence pain susceptibility.
There are still some limitations in this study. While our sample size met basic requirements, broader regional representation would require larger multi-center studies. Future nationwide investigations could better characterize growing pains epidemiology and treatment outcomes across the country. Second, parent-reported data, despite quality controls (response time/consistency checks), may contain subjective biases affecting accuracy. Third, although we identified maternal secondhand smoke exposure as a risk factor, the influence of paternal smoking remains unexamined and warrants future investigation.
Conclusion
Frequent maternal smoking exposure during pregnancy, prolonged sleep latency (30–60 min), and post-exercise exhaustion are independently associated with a higher prevalence of growing pains. And the preference for legumes and participation in sports were associated with a lower prevalence of growing pains. Therefore, children with a maternal history of smoking exposure during pregnancy, sleep latency of 30–60 min, or extreme fatigue after exercise should be alerted to their increased risk of developing growing pains. It is also recommended that mothers avoid smoking exposure during pregnancy and that children maintain healthy sleep patterns, engage in regular but not excessive physical activity, and follow a balanced diet.
Supplemental Material
sj-docx-2-cho-10.1177_18632521251398410 – Supplemental material for Risk factor analysis for growing pains in children: Results of parental survey
Supplemental material, sj-docx-2-cho-10.1177_18632521251398410 for Risk factor analysis for growing pains in children: Results of parental survey by Ruoyi Guo, Weili Xiang, Hanjie Zhuang, Yiwei Wang and Pengfei Zheng in Journal of Children's Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251398410 – Supplemental material for Risk factor analysis for growing pains in children: Results of parental survey
Supplemental material, sj-pdf-1-cho-10.1177_18632521251398410 for Risk factor analysis for growing pains in children: Results of parental survey by Ruoyi Guo, Weili Xiang, Hanjie Zhuang, Yiwei Wang and Pengfei Zheng in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
None.
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was conducted following the Declaration of Helsinki and approved by the Institutional Review Board of our institution.
Consent to participate
All participants provided written informed consent before recruitment.
Consent for publication
Written informed consent for publication was obtained from all participants.
Data availability statement
The data are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.