
Abstract
Purpose:
Non-surgical treatment is indicated in children with severe developmental dysplasia of the hip. Immobilisation may affect motor development. This study assessed motor outcomes in children treated with closed reduction, cast and brace or closed reduction and brace.
Methods:
We conducted a retrospective study on 35 children (mean age 2.1 ± 1.4 months) and a prospective study on 17 children (mean age 1.4 ± 0.9 months), involving 68 hips (22 type D, 31 type III and 15 type IV). Treatment duration averaged 4.7 ± 2.2 months in retrospective study and 3.5 ± 1.9 months in prospective study. Multivariate regression analysed predictors of walking age, including treatment type, age at treatment start, developmental dysplasia of the hip severity, family history and breech presentation. A mixed-effects linear model compared treatment duration across studies. p values of z-score tests on regression coefficients are reported.
Results:
Mean walking age was 14.6 ± 2.6 months in retrospective study and 14.7 ± 2.4 months in prospective study. Dysplasia severity (p < 0.05) and later treatment start (p < 0.001) predicted delayed walking age. Treatment type showed no overall effect; however, in type III, casts significantly delayed walking (p < 0.05). Severity had no impact when treatment began before 2 months, whereas later treatment led to significant differences based on severity (p < 0.01). At the last follow-up of prospective study, at 16 months, no parents reported persistent motor impairments compared with peers.
Conclusion:
Treatment initiated within 2 months mitigates the effect of developmental dysplasia of the hip severity on motor development, resulting in similar walking outcomes across severities. These results underscore the importance of early treatment in severe developmental dysplasia of the hip.
Level of evidence:
II.
Introduction
Developmental dysplasia of the hip (DDH) is a condition that includes a wide spectrum of severity with ultrasound (US) as the preferred diagnostic approach for hip morphology evaluation. 1 There is disagreement regarding the aetiology and pathogenesis although recent genetic studies, including genome-wide association analyses, highlight the multifactorial nature of DDH. 2 A conservative approach in DDH is commonly considered the first choice of treatment in children aged up to 6 months. 3 Open reduction surgery is indicated in later diagnosed DDH or more often after failure of conservative treatment. 4 However, further complications such as avascular necrosis (AVN) of the femoral head and residual acetabulum dysplasia are reported after open reduction.2,5 Thus early diagnosis, which is correlated with early treatment, represents the most effective tool for achieving excellent results in DDH.1,6,7 In DDH, non-surgical treatment options include dynamic bracing using the Pavlik method and harness or static bracing using more stable devices.8–10 Casting after closed reduction, with or without a traction period beforehand, is indicated in severe DDH with hip dislocation. 11
Outcomes are mostly analysed radiologically. 12 Clinically, leg length discrepancy correlated to femoral head disorders such as AVN or coxa vara and limited range of motion are commonly evaluated at follow-up, whereas motor skills acquisition during DDH treatment in the first year of life and up to walking age (WA) are rarely described.13–15
Among the parameters for evaluation of motor development in children in their first year of life, such as gross motor skills, reflexes and stationary position, walking is considered a fundamental step in healthy children and also in children treated for DDH. Parents’ concerns are often related to walking acquisition and WA, which are considered the ‘global’ parameter for healthy motor development. According to the literature, walking onset is expected to occur physiologically between 9 and 18 months of life. 16
Immobilisation in a plaster cast (PC) or in a brace may influence the child’s motor development in their first year of life. Prolonged positioning of the hip in flexion and abduction to deal with DDH, and limited joint movement have a negative impact on muscle development and motor skill acquisition, typically leading to a delay in WA with respect to healthy peers. Indeed, the World Health Organization (WHO) advises against maintaining fixed positions for over 1 consecutive hour before the age of 12 months and recommends at least 30 min of tummy time daily.17,18 These guidelines, however, cannot be fully adhered to during treatment of severe DDH where the type and duration of treatment vary based on the severity of DDH and the age at diagnosis, which ranges from a few weeks to several months.3,19,20
The aim of this study was to evaluate WA after early conservative treatment in children with severe DDH. Additionally, the potential correlation among WA, DDH severity, treatment type and duration and age at treatment start were analysed.
Materials and methods
A retrospective study including 35 children (30 female, 5 male) treated between January 2015 and April 2020 with a mean age at treatment start of 2.1 ± 1.4 months, and a prospective study, conducted between May 2020 and March 2021, which involved 17 children (15 female, 2 male) with a mean age of 1.4 ± 0.9 months at treatment start, were performed. A total of 52 children with severe DDH affecting 68 hips (bilateral involvement in 16 cases) were evaluated across both studies.
US examinations were performed by the same certified operator (paediatric orthopaedic surgeon with expertise in US techniques and DDH), using a Siemens Acuson X300 apparatus (Siemens Aktiengesellschaft, Erlangen, Germany) with a multifrequency US transducer. The hips were classified according to the Graf classification 21 and included, across the two studies, 22 type D, 31 type III and 15 type IV. All patients were followed up by US until a type I hip (alpha angle >60°) was achieved.
DDH treatment included closed reduction and immobilisation in a PC followed by bracing, or closed reduction and bracing (Figure 1). Closed reduction was not preceded by a traction period.
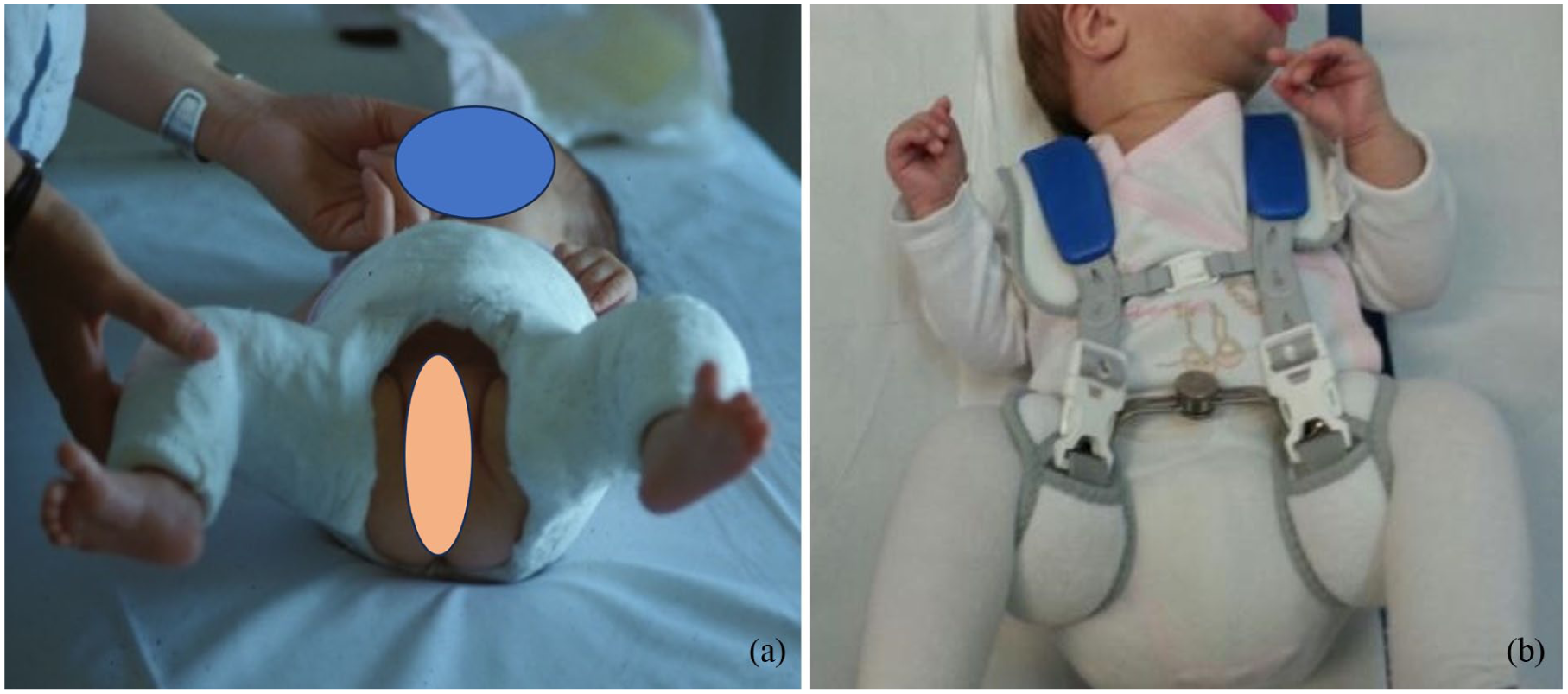
(a) Hip stabilisation after closed reduction with plaster cast in flexion and safe abduction. (b) Bracing* in flexion and abduction for further treatment after 4/6 weeks casting. (*Hip med® Brace).
Casting and bracing (Hip med® Brace; Thuasne Deutschland GmbH, Burgwedel, Germany; hip brace (HB)) were performed with positioning of the hip at ~100° flexion and abduction not exceeding 50°–60°.
The following inclusion and exclusion criteria were adopted:
● Inclusion criteria: ○ Diagnosis of DDH types D, III and IV according to the Graf classification. ○ US examination by the same certified operator. ○ Presence of complete clinical and imaging documentation. ○ Duration of orthopaedic treatment longer than 6 weeks. ○ Receipt of informed consent from both parents.
● Exclusion criteria: ○ Diagnosis of DDH types IIb and IIc according to the Graf classification. ○ Presence of neuromotor pathology, or genetic or congenital malformation. ○ Presence of other clinical problems during standardised paediatric examinations. ○ Prematurity with gestational age <32 weeks. ○ Prolonged postnatal hospitalisation in neonatal care (>2 weeks).
In the retrospective study, the children’s parents were contacted by telephone to collect a detailed history, including the following data: (1) date of birth, (2) sex, (3) position of the foetus in utero, (4) family history for DDH, (5) presence of other orthopaedic problems, or neurological and/or genetic disorders, (6) age at diagnosis and treatment start, (7) type of DDH according to the Graf classification, (8) type and duration of treatment, (9) WA (defined as the age when the child is able to walk at least 3 m independently) and (10) any physiotherapy or other rehabilitation treatments carried out.
In the prospective study, the children were assessed by a single physical therapist (MS) using the Peabody Developmental Motor Scale-2 (PDMS-2). 22 Among the many parameters evaluated (e.g. gross motor skills reflexes, stationary position, locomotion, object manipulation, grasping, eye-hand coordination), WA was extrapolated for this study, and walking onset was registered. Assessments were conducted at baseline (4–8 weeks) and at 3, 6, 9, 12 and 16 months of age.
At each follow-up visit, the paediatric orthopaedic surgeon conducted a clinical assessment for hip dysplasia and performed an US examination until normalisation of the hips was achieved (alpha angle >60°). Independently, the paediatric-trained physiotherapist assessed motor development using the PDMS-2. Items were administered according to the child’s age, as specified in the scale manual, and the scores obtained were compared with normative data using the corresponding tables provided in the manual.
The study was performed according to the ethical standards of the 1964 Declaration of Helsinki and was approved by the hospital’s ethics committee.
Statistical analysis
Multivariate regression was employed to study the relationship between WA and the following categorical predictive factors in the retrospective dataset: treatment type (−1: cast application; 1: no application of cast), age of treatment start (−1: before 2 months; 1: after 2 months), DDH Graf classification (−1: type D; 0: type III; 1: type IV), family history for DDH (−1: no family history; 1: family history) and breech position (−1: no breech; 1: breech). All categorical values were converted to zero-centred integer values to improve the quality of the linear regression fit. Ordinary least squares (OLS) regression was performed, followed by weighted least squares (WLS) regression using the reciprocals of OLS residuals as weights to account for heteroscedasticity. 23 The influence of a predictor was deemed significant if a z-score test on its regression coefficient produced a p < 0.05. Goodness-of-fit for the WLS model was evaluated using the F-statistic (indicating whether predictors explain variance in the outcome), the D’Agostino–Pearson omnibus test and the Jarque–Bera test (indicating normality of residuals) and the Durbin–Watson statistic (indicating absence of correlation between residuals and observations).
To evaluate the effectiveness of treatment, the children in the prospective study were compared to the retrospective cohort, investigating the relationship between treatment duration and WA. A mixed-effects linear model was applied to quantify the variation in treatment duration (in months) between the retrospective and prospective groups (−1: retrospective; 1: prospective), considering disease severity as a grouping variable. Only types D and III were included since type IV was not adequately represented in the prospective dataset. The variation in treatment duration was deemed significant if a z-score test on the regression coefficient between the study group and treatment duration produced a p < 0.05.
All results were computed using Python’s statsmodels library (Copyright 2009−2023, Josef Perktold, Skipper Seabold, Jonathan Taylor, statsmodels-developers).
Results
The demographic and clinical characteristics of the study population are summarised in Figure 2. The distribution of dysplasia severity highlights that type III dysplasia was the most frequent, representing 46.0% of cases, followed by type IV (34.0%) and type D (20.0%). Regarding treatment type, 60.0% of children were treated with both PC and HB, while the remaining 40.0% were treated exclusively with HB. The age at treatment end ranged from 2.5 to 12.5 months, with most cases clustering in the 5- to 7.5-month range. Treatment duration varied from 2 to 10 months, with the highest concentration observed between 3 and 5 months.
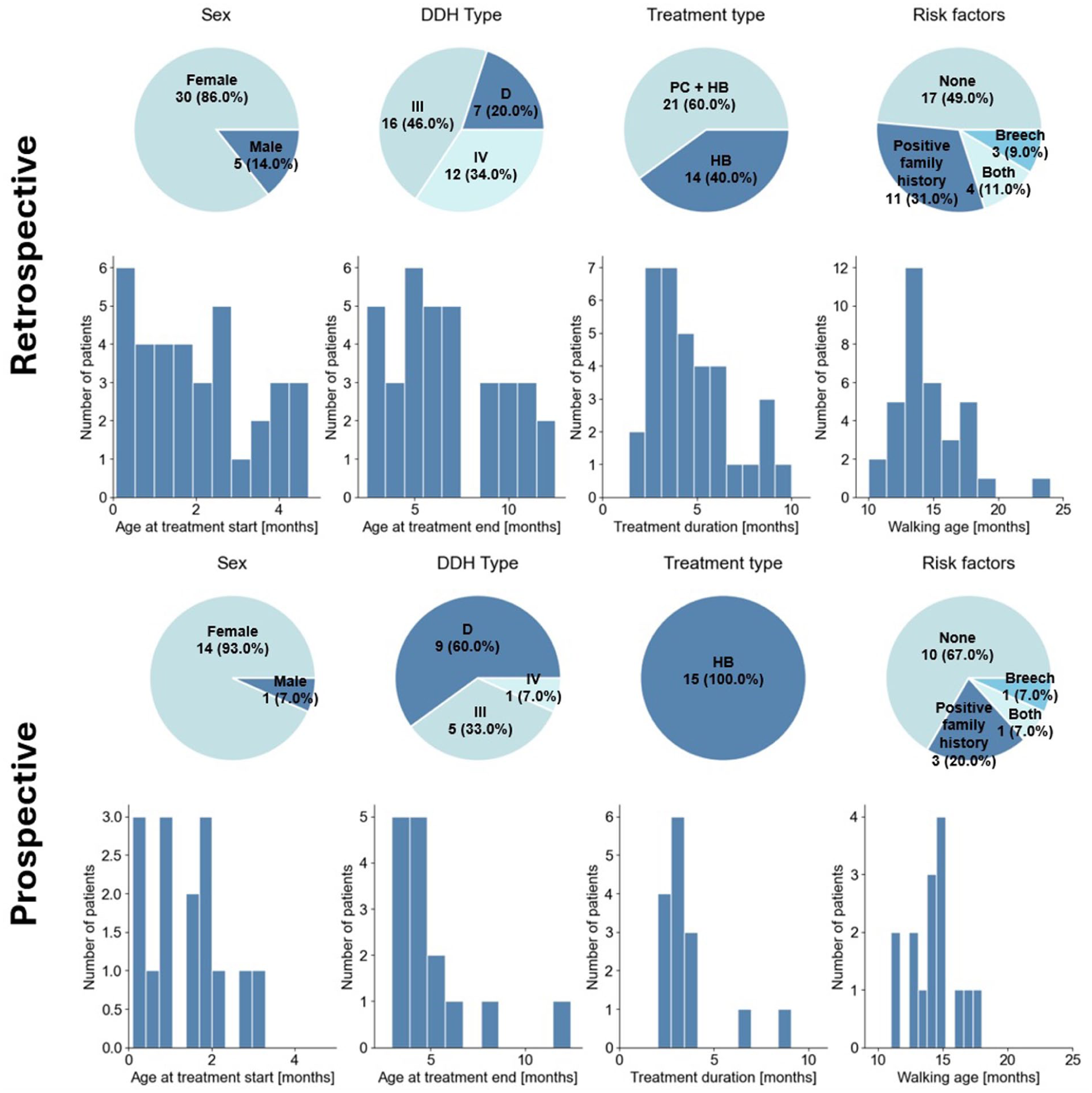
Demographic and treatment characteristics of study populations. Comparison of retrospective and prospective datasets. Pie charts display distributions of sex, DDH severity types (D, III and IV), treatment type and risk factors. Histograms illustrate the distributions of age at treatment start, age at treatment end, treatment duration and age at walking onset.
A multivariate regression analysis revealed that only the severity of dysplasia (p < 0.05) and the age of treatment start (p < 0.001) significantly influenced WA, with more severe dysplasia and later start of treatment being associated with delayed WA (Figure 3(a)). Although the use of PC was associated in general with a later WA, this was not of statistical significance. Similarly, family history for DDH and breech presentation did not show significant associations with WA. The presence of risk factors did not influence WA, which is likely to be due to the heightened clinical attention and prompt interventions in these cases. A strong imbalance in the distribution of treatment types across dysplasia severities was observed, with PC being predominantly used in more severe cases, as shown in Figure 3(b). To address this imbalance, a subgroup analysis was conducted on patients with type III hips, which were evenly distributed across the treatment groups. This analysis confirmed that both the age at treatment start (p < 0.001) and the type of treatment (p < 0.05) had a significant effect on WA, with PC leading to later WA (Figure 3(c)).
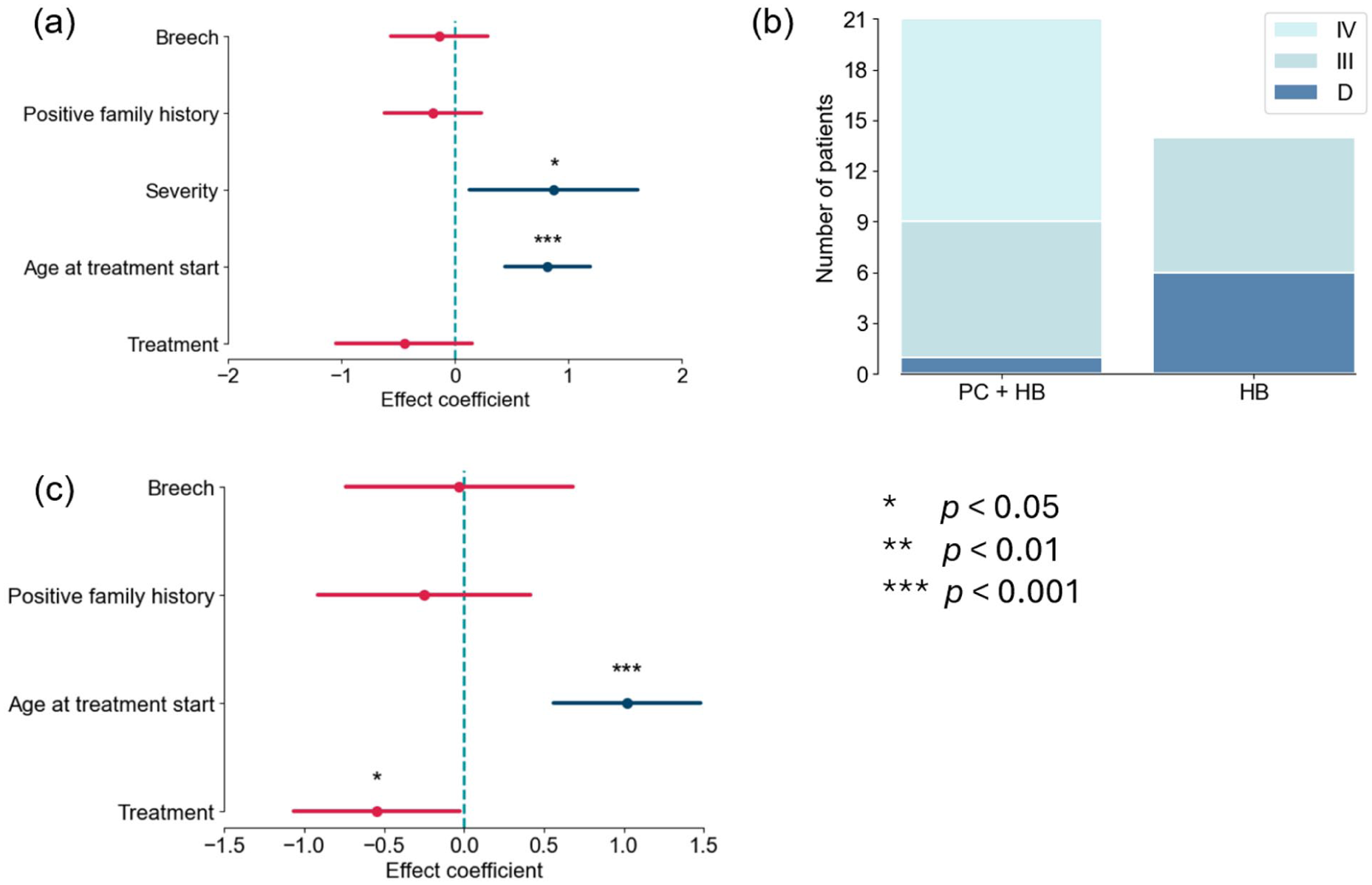
Predictive factors of age at walking onset. (a) Effect coefficients of predictive factors from the multivariate regression model explaining WA from the predictor breech presentation, positive family history, dysplasia severity, age at treatment start and treatment type. (b) Distribution of DDH severities (D, III and IV) for the PC + HB and HB populations. (c) Subgroup analysis of type III dysplasia patients showing effect coefficients of predictive factors: breech presentation, positive family history, age at treatment start and treatment type.
Further analyses explored the influence of treatment timing and severity. In Figure 4(a), we show the distribution of patients in the retrospective study across the different treatment types, different age at the start of treatment and DDH severity (Figure 4(a)). When treatment started before 2 months of age, the severity of dysplasia did not significantly impact WA, resulting in comparable outcomes across severities (Figure 4(b)). Conversely, when treatment began after 2 months, severity became a significant predictor, with more severe cases exhibiting later WA (p < 0.01, Figure 4(c)).
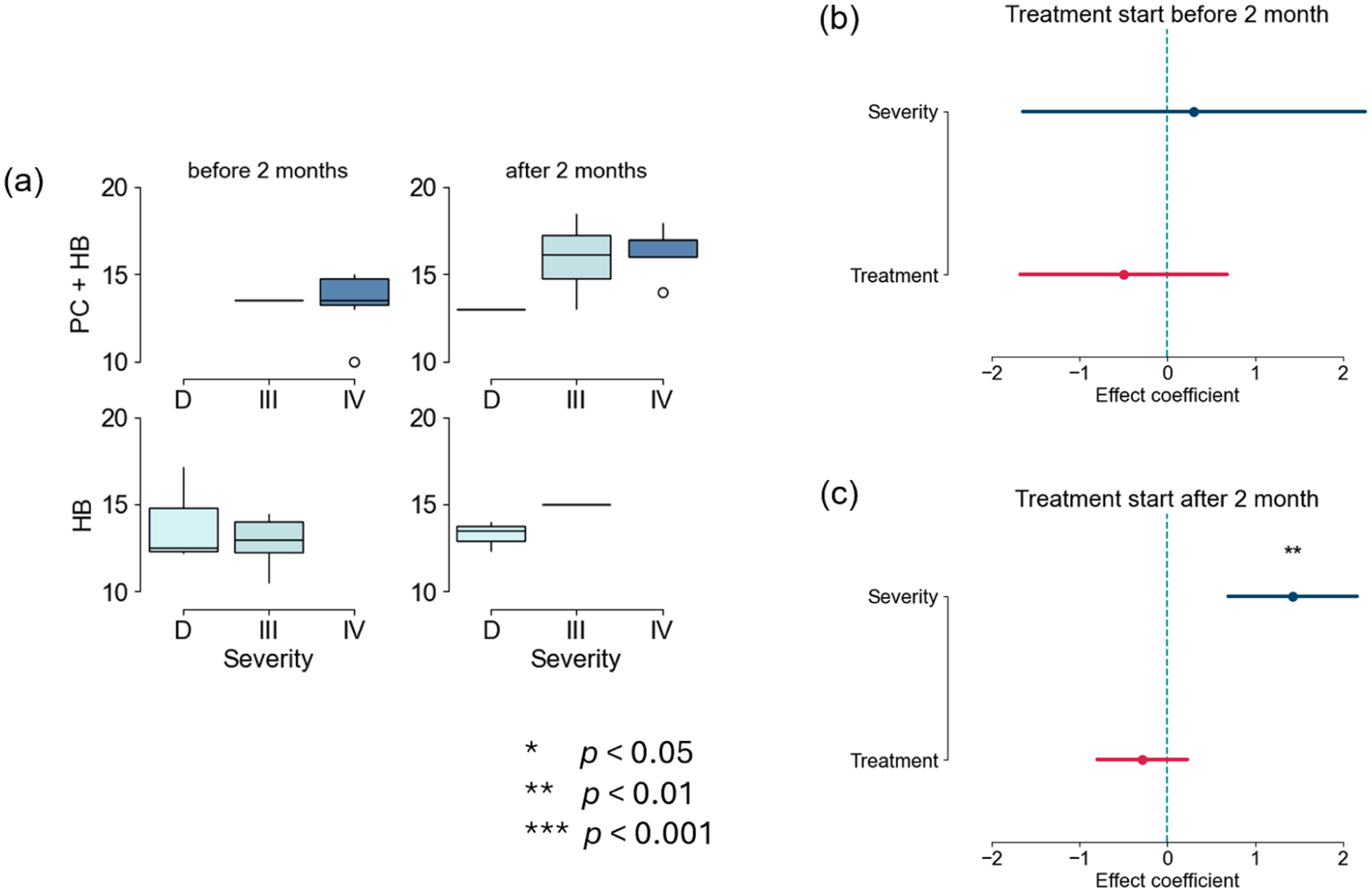
Predictive factors of age at walking onset, grouped by age at treatment start. (a) Box plots showing the distribution of WA across dysplasia severities (D, III and IV) and treatment types (PC + HB and HB) for treatment start before 2 months and after 2 months. (b) Effect coefficients of dysplasia severity and treatment type on WA when treatment started before 2 months. (c) Effect coefficients of dysplasia severity and treatment type on WA when treatment started after 2 months.
In the prospective study, in which treatment started earlier and casting was not performed, WA was comparable to the retrospective cohort but it was possible to reduce treatment duration. For children with type D hips, treatment duration was reduced by more than 1 month (Figure 5(a)–(c)), while for type III hips, it was reduced by almost 2 months (Figure 5(d)–(f)). The mixed-effects linear model confirmed this finding and showed a statistically significant reduction in treatment duration for the prospective cohort, with an average reduction exceeding 1 month across severities (p < 0.05). This indicates that the optimised treatment approach achieves equivalent motor outcomes in a shorter time, providing a more efficient therapeutic strategy for managing severe DDH.
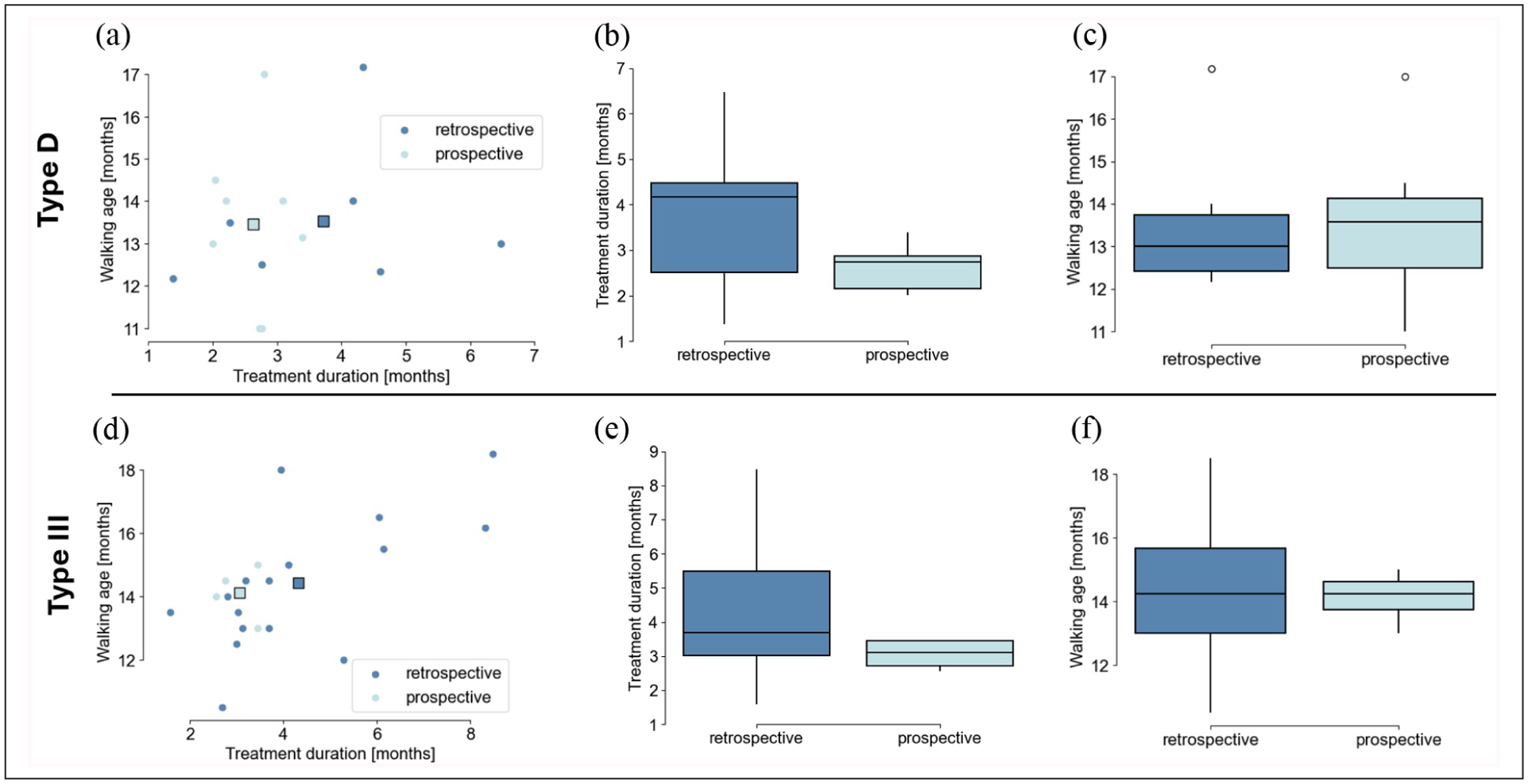
Comparison of walking onset age and treatment duration between retrospective and prospective cohorts. (a) Scatter plot of treatment duration versus walking onset age for type D hips for both retrospective and prospective cohorts. (b) Box plot comparing the treatment duration between retrospective and prospective cohorts for type D hips. (c) Box plot comparing the walking onset age between retrospective and prospective cohorts for type D hips. (d) Scatter plot of treatment duration versus walking onset age for type III hips in retrospective and prospective cohorts. (e) Box plot comparing treatment duration between retrospective and prospective cohorts for type III hips. (f) Box plot comparing walking onset age between retrospective and prospective cohorts for type III hips. In panels (a, c), the square markers indicate the centroid of the respective population.
Treatment duration was 4.7 ± 2.2 and 3.5 ± 1.9 months in the retrospective and prospective studies, respectively.
Discussion
Conservative treatment is the first treatment option in the majority of cases, also in severe DDH. In dislocated hips, closed reduction and stabilisation with immobilisation in a PC or brace are a common strategy reported in the literature.1,3,24–27
However, immobilisation may influence motor skills acquisition as reported by Zgoda et al. 14 Motor development and particularly walking onset are the parents’ main concern at treatment start regardless of the type of treatment.
Previous studies have highlighted a statistically significant delay in WA for children treated with abduction braces compared to healthy peers, reporting a mean WA of 12.5 and 13.1 months, respectively.13,14 Jesus et al. reported an average WA of 14.0 months for the 55 children treated exclusively with the Pavlik method. 15 Our findings in 52 children extend these observations and provide typical values for severe cases (types D, III and IV), revealing an even greater delay in WA, with a mean of 14.6 months for the retrospective group and 14.7 months for the prospective group in children treated with PC and HB after closed reduction, or only with HB.
Risk factors 24 such as breech presentation and a positive family history for DDH did not influence treatment outcomes, whereas severity of DDH and age at treatment start did.
The importance of early treatment was shown to be a critical factor in this study. Children who began treatment before 2 months of age demonstrated comparable WA across all severities of DDH, suggesting that early intervention may mitigate the impact of dysplasia severity on motor development. Conversely, delays in beginning treatment were associated with progressively later WA, particularly in more severe cases.6,7 These findings reinforce the value of early diagnosis regardless of the type of screening strategy (clinical, selective by US, universal by US).25,26
Universal ultrasound screening showed the best results in terms of early treatment.1,27,28
The analysis of treatment type further underscores the influence of therapeutic approaches on WA. Children treated exclusively with abduction braces showed earlier WA compared to those requiring both PCs and braces. This is in line with the hypothesis that less restrictive treatments better support musculoskeletal and motor development during the critical early stages of growth. However, the observed imbalance in the allocation of treatment types across severities, with more severe cases often receiving PCs, makes the interpretation of these results more complicated. A subgroup analysis of children with type III dysplasia—where treatment allocation was more balanced—confirmed that both the timing of treatment start and the use of PCs significantly affected WA. These results suggest that while conservative approaches are necessary in severe cases, motor outcomes may be improved if the use of PCs is minimised, whenever feasible.
Despite achieving an age of walking onset comparable to the retrospective cohort, the prospective study showed a significant reduction in the overall duration of treatment, particularly for type D and III hips. This reduction—over 1 month for type D and nearly 2 months for type III—demonstrates the efficiency of the optimised approach in achieving equivalent motor outcomes with a shorter treatment time. Minimising the use of restrictive casting may reduce the burden on both patients and caregivers, while still addressing the motor development needs of children with severe DDH.
Our findings also highlight the challenges of adhering to developmental guidelines, such as those recommended by the WHO. 16 The long-term fixed positioning required for DDH treatment contradicts recommendations for unrestricted movement and tummy time, which potentially influence early motor development. Despite these constraints, our data suggest that any initial delays in motor milestones do not lead to persistent developmental differences, as reported by the parents in the retrospective group.
This study highlights the critical role of early diagnosis and treatment in mitigating the impact of severe DDH on motor development. Starting treatment before the age of 2 months can effectively counteract the negative influence of DDH severity on WA, leading to comparable outcomes across different severities. Conversely, delayed intervention significantly correlates with a later age of walking onset, particularly in cases with more severe dysplasia. This study emphasises the importance of finding a balance between effective orthopaedic management and minimising the burden on patients and families.
Limitations and future directions
This study presents some limitations that should be considered when interpreting the results.
First, the sample size—particularly in the prospective cohort—was relatively small, which may have limited the statistical power of the subgroup analyses. For this reason, we only included types D and III since type IV was not adequately represented in the prospective dataset. Future studies involving larger, multicentre cohorts could strengthen the findings and help better define the correlations between treatment variables and motor development outcomes.
Second, we recognise that different methodologies were used to assess WA in the retrospective and prospective groups. However, efforts were made to ensure consistency and reliability of the data collected in both groups. While the initial mode of data collection differed, the use of a uniform definition and recall strategy in both groups was intended to reduce discrepancies and support comparability of the WA data.
In the retrospective group, WA was obtained via structured telephone interviews with parents. During these interviews, a clear and standardised definition of independent walking was provided (i.e. the ability to walk at least 10 consecutive steps without falling or support). Parents were also encouraged to review personal photos or video recordings to accurately recall the timing of walking onset. This approach aimed to minimise recall bias and improve the accuracy of retrospective reporting.
In the prospective group, although the children were monitored during scheduled follow-up visits, the exact acquisition of independent walking did not always coincide with these visits. For this reason, when walking onset occurred between follow-ups, the same structured questions and recall strategy used in the retrospective group were applied to parents of the prospective group, ensuring methodological consistency across both cohorts. This approach helped ensure data homogeneity and comparability, even in cases where the timing of walking onset was not directly observed.
Future directions include expanding the sample size and further investigating long-term functional outcomes. It would also be valuable to incorporate broader assessments of motor development, taking into account not only WA but also additional aspects such as balance, coordination and participation in physical activities, to provide a more comprehensive understanding of how conservative treatment for DDH impacts child development.
Conclusions
This study confirms that early conservative treatment in severe forms of DDH can lead to comparable WA outcomes, regardless of the severity of dysplasia, if started before 2 months of age. The severity of DDH and delayed treatment initiation are significant predictors of later walking acquisition, emphasising the critical importance of early diagnosis and intervention. The findings highlight that timely treatment initiation is a key factor in improving motor outcomes in children with severe DDH, contributing to an effective and sustainable therapeutic pathway for both patients and their families.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251390250 – Supplemental material for The influence of non-surgical treatment on walking age in children with severe developmental dysplasia of the hip
Supplemental material, sj-pdf-1-cho-10.1177_18632521251390250 for The influence of non-surgical treatment on walking age in children with severe developmental dysplasia of the hip by Maurizio De Pellegrin, Marina Sarzana, Daniele Emedoli, Simone Romeni, Lorenzo Marcucci and Nicola Guindani in Journal of Children's Orthopaedics
Footnotes
Author contributions
MDP and MS: main contributors in study design, performing measurements, article preparation. DE: performing measurements, physiotherapy assessments. SR: data analysis. LM and NG: article preparation. All the authors have read and agreed to the published version of the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical considerations
This study complies with ethical standards. The study has been performed in accordance with the ethical standards in the 1964 Declaration of Helsinki. The study was approved by the Ethic Committee of the San Raffaele Hospital in Milan (protocol no. 16/int/2020).
Consent to participate
Parental informed consent was obtained for all subjects involved in this study.
Consent for publication
All the authors read and approved the final article.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.