
Abstract
Purpose:
Our purpose was to analyze the impact of Pavlik Harness treatment on children motor skills development, comparing to a control group.
Methods:
A total of 121 children were included: 55 cases (children with Developmental Dysplasia of the Hip) and 66 healthy controls. Cases were recruited from 2017 to 2021 and followed up to 2022. Controls (healthy children without orthopedic pathology) were recruited from 2020 to 2022. The primary endpoint was the time of achievement of three gross motor milestones (sitting without support, hands-and-knees crawling, and walking independently).
Results:
The groups had no differences regarding sex distribution, gestational age, birth weight, and rate of twin pregnancy. The prevalence of positive family history of Development Dysplasia of the Hip (20.0% vs 3.0%, p < 0.003), breech presentation (38.2% vs 1.5%, p < 0.001), and C-section delivery (60.0% vs 19.7%, p < 0.001) was significantly higher in Development Dysplasia of the Hip group. Children with Development Dysplasia of the Hip achieved the three gross milestones evaluated 1 month later than healthy controls, although this was not statistically significant (p = 0.133 for sitting, p = 0.670 for crawling, and p = 0.499 for walking).
Conclusion:
Children with Development Dysplasia of the Hip, treated by Pavlik harness, do not have significant delays in motor skills acquisition.
Introduction
Developmental Dysplasia of the Hip (DDH) is a complex musculoskeletal wide spectrum of conditions in which the hip joint bones and adjacent soft tissues are not properly developed. 1 This results in imperfect alignment and consequent instability of the joint, varying from change in bone’s shape to severe dislocation needing surgical treatment. 2 DDH is one of the most common orthopedic pediatric conditions, affecting 0.1–6.6 per 1000 children worldwide. 3 This condition may develop in the early stages of fetus formation all the way through early childhood. Although there are some theories regarding its exact cause and physiopathology, all remain unproven, and more research is needed to further understand and prevent this condition. 3 A multifactorial origin is generally accepted, and some risk factors have been identified, such as positive family history, breech position, oligohydramnios, first born, female sex, and the presence of other musculoskeletal conditions. 4 If not treated promptly, the child may present with difficulties walking, pain, osteoarthritis, and other potentially severe consequences, 3 making early diagnosis and prompt treatment of extreme importance. Clinical signs such as limitation of hip abduction or difference between length of both legs should arise suspicion of DDH. Physical examination maneuvers, like the Barlow and Ortolani maneuvers, should be performed by the pediatrician as part of a complete routine physical exam of all infants.5,6 If any sign of DDH is present, the infant must be observed by an orthopedic specialist to confirm the diagnosis and initiate treatment. 7
The Pavlik Harness is the most commonly used orthosis to treat DDH in children under 6 months of age. 5 It is usually worn for 1–3 months and has reported success rates of 73% in dislocated hips to 100% for mild dysplasia.8,9 Severe complications of treatment are rare, 10 but little is known about its impact on child motor development. In fact, most studies focus on the development repercussions of surgical treatment of DDH. Pavlik is thought to affect gross motor skill acquisition, 11 and parents of DDH patients often inquire about Pavlik treatment’s impact on gross motor skill acquisition, but this is mostly an unexplored field of investigation. In this study, we aimed to evaluate the impact of Pavlik Harness treatment of children with DDH on their gross motor skills development, in comparison with counterparts without an orthopedic condition (control group).
Methods
A prospective case–control study was designed. Cases were defined as children diagnosed with DDH by a Pediatric Orthopedic Surgeon in our tertiary Hospital. International clinical and ultrasonographic criteria were used for the diagnosis.12,13,14,15 Hips were classified according to Graf’s classification. Children with other orthopedic or neurological conditions or in the need for other treatment rather than the Pavlik Harness were excluded. All cases were recruited from February 2017 to April 2021. Explanation on the aim and methods of study were provided, and written informed consent was obtained. Parents were given a diary for registering time acquisition of all three development milestones considered in our study (sitting without support, hands-and-knees crawling, and walking alone). Data regarding sex, medical history (including obstetric and birth data), family history (first degree relative with DDH), clinical signs of DDH (asymmetric skin folds, positive Ortolani maneuver, positive Barlow maneuver, positive Galeazzi test, and limitation of the abduction of the hip), and duration of treatment were registered.
Controls were recruited from 2020 to 2022 from routine evaluation appointments by their family doctor at a local health center. All children in our country are included in a free national pediatric health program, as part of the National Health Service, having a Family Doctor assigned. Hence, all children go through the same examinations in a defined age schedule. Orthopedic maneuvers such as Ortolani and Barlow and motor skills evaluation are routinely performed since birth, with evaluation of motor skills acquisition at 6, 9, 12, 15, 18, and 24 months of age. Parents were given the same diary sheets as cases to fill in with time of motor skills acquisition. Whenever, for any reason, these diaries were incomplete, the needed information was gathered from medical records or phone interviews, to complete data collection. Again, children with orthopedic or neurological conditions were excluded.
Both groups reported information regarding time of achievement of three gross motor milestones. “Sitting without support” was defined as the ability to remain seated without support for a minimum of 30 s. “Crawling” was defined as the ability to move using their hands and feet for a minimum distance of 3 m. “Walking independently” was defined as the ability to walk without support for a minimum distance of 3 m. 16
Statistical analysis was performed using the software IBM SPSS Statistics 27. For continuous data, normality was assessed through histograms and the Shapiro–Wilk test. For normal data, we used the descriptive measures mean and standard deviation (SD). For non-normal distribution data, we used the median. For comparison of two binomial categories, Chi-square test or Fisher’s exact were used. When continuous variables were involved, unpaired t-tests were performed. Statistical significance level was established at 0.05.
This study was approved by the Ethics Committee of our hospital center and by the Regional Health Administration. All participants provided signed informed consent.
Results
A total of 55 DDH cases and 66 healthy controls were included in our study. Nine children with DDH were initially included in our study but excluded during follow-up due to failure of treatment. Cases were referred to a Pediatric Orthopedic Surgeon by their Family Doctor (40.0%), by a pediatrician at birth (25.5%), by a pediatrician at routine consultation (20.0%), by other hospitals (7.3%), or by an Orthopedic Surgeon that evaluated the child in the Emergency Department of our hospital (7.3%). Reasons for referral are listed in Table 1. Most children had clinical or imaging suspicion of DDH, with only 21.8% being referred for DDH screening.
Reasons for referral to a Pediatric Orthopedic Surgeon (n = 55).
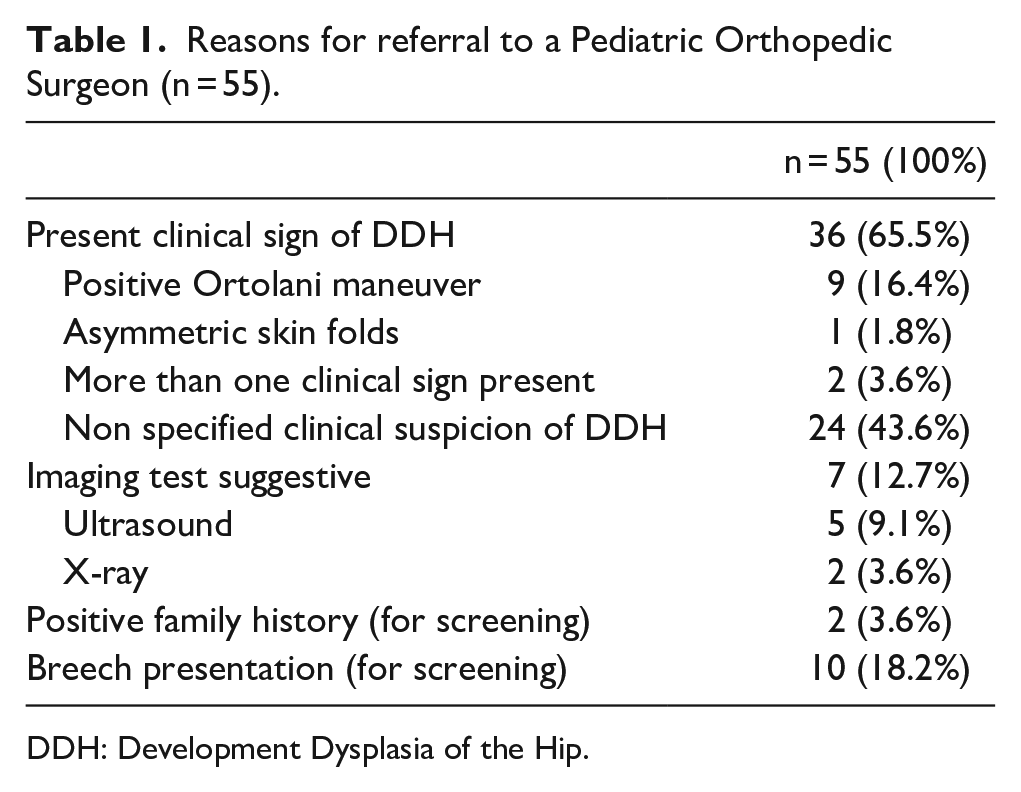
DDH: Development Dysplasia of the Hip.
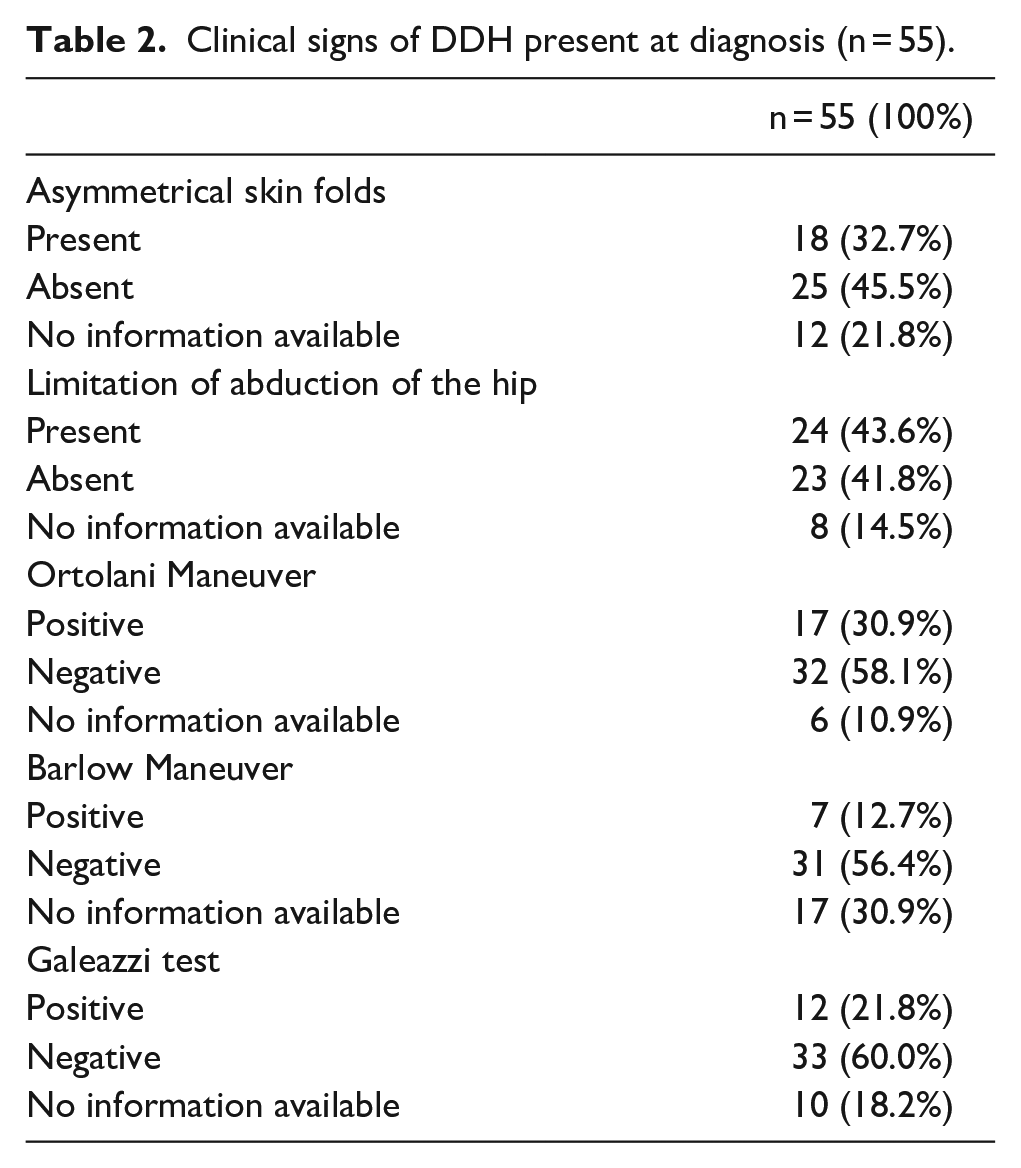
Cases included 10 children with only the right hip affected (18.2%), 27 with only the left hip affected (49.1%) and 18 children with both hips affected (32.7%). Information regarding the clinical signs of DDH present at time of diagnosis is listed in Table 2. Limitation of abduction of the hip was the most common sign of DDH present at diagnosis, affecting almost half of the population studied (43.6%).
Clinical signs of DDH present at diagnosis (n = 55).
Median age of first orthopedic evaluation was 3.3 months (youngest and oldest child having 1.4 and 9.1 months, respectively). Treatment with Pavlik Harness was initiated in the first appointment for almost all cases, or within a month of the first consult, with 4 (7.3%) children initiating treatment after 6 months of age. End of treatment was at a median age of 7.0 months (minimum age of 3.9 months, maximum of 12.6 months), with 29 (52.3%) finishing treatment after 6 months of age. The average duration of treatment was 91.2 days (shortest and longest duration of treatment of 19 and 195 days, respectively).
Most children had severe dysplasia, with 18 patients having at least one Graf IV hip and 14 patients having a Graf III hip (Table 3).
Graf’s classification in the DDH Group (n = 55).
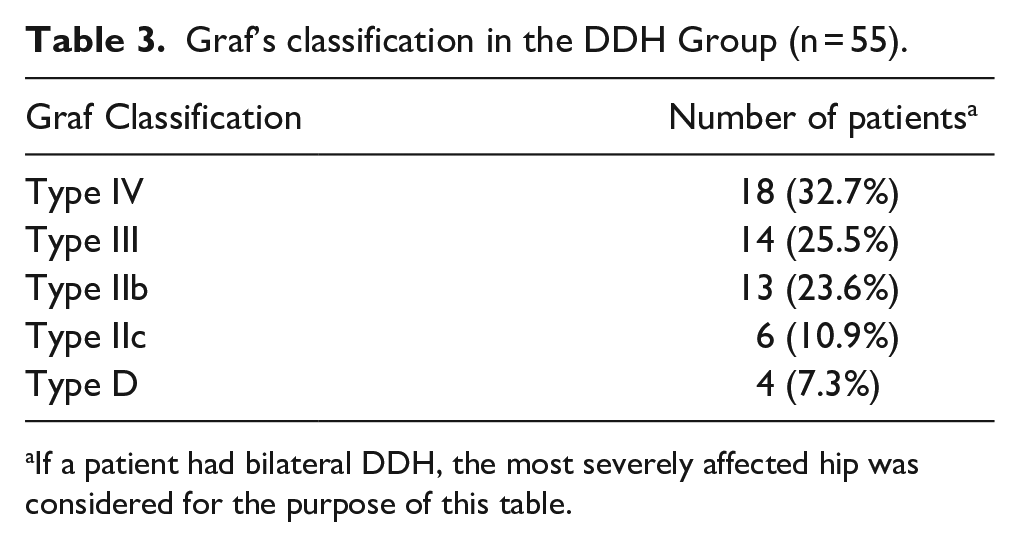
If a patient had bilateral DDH, the most severely affected hip was considered for the purpose of this table.
Table 4 shows the comparison between groups. No significant differences were found regarding sex, gestational age, birth weight, and twin pregnancy. Control group had significantly less cases of a positive family history of DDH (3.0% vs 20.0%, p < 0.003). Breech presentation was more common among cases (38.2% vs 1.5%, p < 0.001), as well as C-section birth (60.0% vs 19.7%, p < 0.001). The median age, in months, for achieving all three motor skills milestones considered in the study was higher by 1 month in children with DDH, but no statistically significant difference was found.
Comparison between groups.
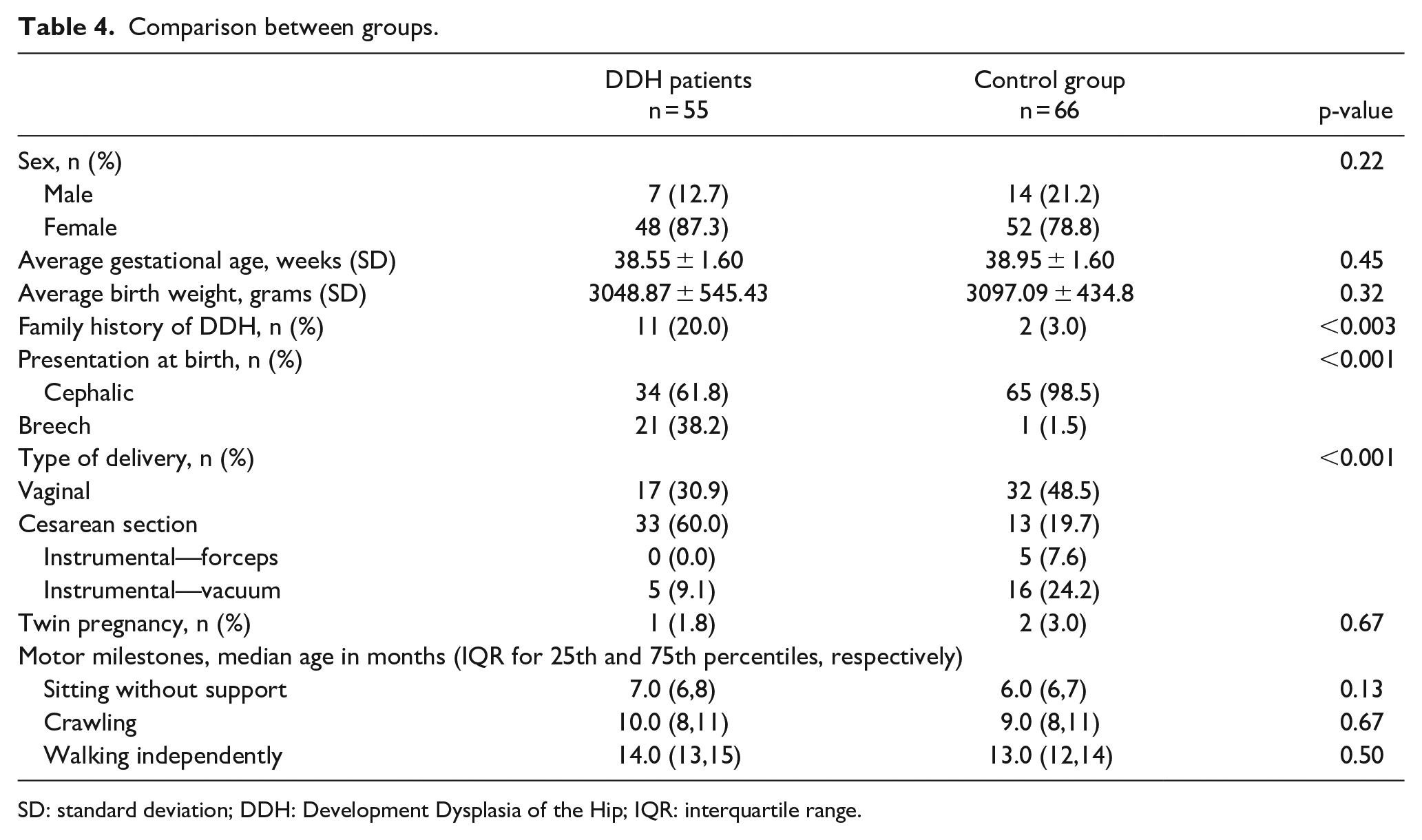
SD: standard deviation; DDH: Development Dysplasia of the Hip; IQR: interquartile range.
Discussion
DDH is one of the most common orthopedic pediatric conditions 3 and has potentially severe consequences for the child’s quality of life. 17 Prompt evaluation by a Pediatric Orthopedic Surgeon plays an important role in the diagnosis, whenever clinical suspicion or risk factors are present. 18 Routine screening, through complete physical examination of the hip of the newborn and infant, and targeted ultrasonographic evaluation are also essential for early detection of DDH,13,19,20,21 useful in preventing future severe problems or need for extensive surgery. 22 Universal clinical screening and selective ultrasound is standard practice in our country. Children with risk factors for DDH, such as positive family history and breech presentation are selected for ultrasound screening. It was therefore unsurprising that over 85% of children with DDH in our population were referred by their Family Doctor or Pediatrician.
The left hip was more frequently affected in our population, consistent with worldwide reports. 10 Clinical signs of DDH are well established in the literature.5,7 Limitation of hip abduction was the most common sign found in our patients. We found these data unsurprising as it correlates with the pathophysiology of DDH itself and has been reported as a specific and reasonably sensitive sign.23,24 Asymmetrical skin folds were the second most common clinical sign observed, which was, again, unsurprising as it can be present frequently even in up to 30% of children without DDH.5,25 Frequencies of the clinical signs found in our study appear to be higher than others found in similar articles.26,27 An explanation for this may be that all children included in our study had DDH that needed to be treated with Pavlik Harness, therefore having more “severe” disease than others that only had a “wait and see” approach. Furthermore, although our data were gathered from existing clinical records in which not all maneuvers and other clinical signs were registered for all children, all were evaluated by an experienced Orthopedic Pediatric Surgeon that could potentially be more sensitive to the detection of the clinical signs mentioned. Other reason for this is timing of evaluation, as the Barlow and Ortolani maneuvers positivity may change through time, as capsule laxity also changes. 23
The median age for first orthopedic evaluation in our population with DDH was 3.3 months. This accounts for the delay between referral and time of consult, but it is also a reflection that not all DDH can be diagnosed at birth and therefore may not show signs before a certain amount of time has passed. There were virtually no delays between diagnosis and start of treatment. Median age for starting the Pavlik Harness treatment was within recommended limits.26,28,29 Similarly, the average treatment duration was also consistent with worldwide practices.8,29
Most patients with DDH were female, as seen in previous studies.30,31 It has been hypothesized that female hormones may play a role in the etiopathogenesis of DDH, as in may increase joint laxity, making females more susceptible to development of this condition. 2 In our study, both groups had similar percentage of female individuals, gestational age, birth weight and twin pregnancies, making comparison possible. Higher birth weight (large for gestational age) has been associated with congenital anomalies, including DDH.30,32 The risk is weight-dependent, with heavier children having greater probability for hip dysplasia. 32 Higher birth weight also increases the risk of other orthopedic conditions that may affect motor skills acquisition. Although some authors have suggested that prematurity would be a risk factor for DDH, 30 as breech presentation is more common at younger gestation ages, a recent meta-analysis has shown that prematurity is not strongly associated with DDH. 33 Another recent study suggested it may in fact be protective for DDH. 34 Prematurity may, however, pose a higher risk for neurodevelopment impairment, including motor development issues. In our study, no differences were found between groups regarding birth weight nor gestational age. Our results are therefore unaffected by possible differences resulting from conditions caused by these factors.
It has been hypothesized that twin pregnancy may be a risk factor for DDH, as less space available for each fetus may lead to immobilization and the development of orthopedic conditions, DDH being one of them. 35 Some guidelines suggest the screening of twins, especially if any other risk factor mentioned is present. 36 However, other studies have found no increase in DDH risk in multiple births.35,37 Twin pregnancy as also been associated with a higher risk of complications, such as lower gestational age and low birth weight. 38 Again, these factors may delay neurodevelopment including motor skills acquisition. As no differences were found between groups in our study regarding twin pregnancy, our results are unaffected by this possible confounding factor.
Positive family history, a well-known risk factor of DDH,2,39 was unsurprisingly more commonly found in cases. Our numbers stress the importance of a good medical history including first degreed relative orthopedic history, as this may be an indication for screening.18,40 Breech presentation and cesarean section birth were also expectedly more common among cases. Breech presentation has long been identified as a risk factor for DDH.30,31 Cesarean delivery is the delivery method of choice whenever breech presentation is present. In these cases, it seems to have a significantly lower risk of DDH, when compared to vaginal delivery of breech presenting newborns. 30 As with positive family history, gestational history should also be considered when evaluating a newborn or infant, 40 as it may dictate the need for evaluation by a Pediatric Orthopedic Surgeon.
In our study, no differences between groups were found in median age for achieving the three motor skills milestones considered. Case–control studies analyzing motor skills milestones achievement are limited. A retrospective case–control study of 2004 41 studied 86 children with DDH and found the median age for independent walking 1 month less in normal controls when compared with children with late presentation of DDH but still within normal limits (and therefore clinically insignificant). However, children in that study were not treated with Pavlik Harness and therefore were not subjected to a period of immobilization. A 2007 Spanish case–control study 16 of 24 DDH patients treated with Pavlik Harness showed similar ages to our study for achievement of all three milestones (for controls and cases, respectively: 6.12 vs 6.42 months for sitting; 8.84 vs 9.38 months for crawling; 12.14 vs 13.21 months for walking). The differences found were significant for crawling and walking without support; however, they were still within normal limits. This is consistent with the results found in our study.
Our study had some limitations that must be mentioned. We used a small sample, with a short time of follow-up (2 years), and we only considered three motor skills milestones, disregarding other potential ones. The enrollment of controls was affected by several constraints. As they are healthy children, parents may be more prone to miss routine doctor appointments, therefore having longer periods of time between consultations. This may lead to more memory errors when recording timing of milestone achievement. In addition to this, controls were enrolled after the enrollment of cases, at the time when the SARS-CoV-2 pandemic quarantine started. These kids may have potentially been less stimulated as daycares were closed and therefore have a delay in motor skill acquisition. 42 However, studies point to language and communication as the areas more affected by isolation seen during COVID. 43 On the contrary, it has been hypothesized that during quarantine, parents may have spent more time with their child working on their skills and minimizing any possible pandemic negative effects. In fact, some studies show no association between pandemic exposure and development. 44 More studies, with a broader population and a longer follow-up period, are needed to further clarify this subject.
Conclusion
Our study suggests that Pavlik Harness treatment of children with DDH does not delay motor skills acquisition, when comparing to a control group. As some challenges for DDH treatment remain yet today, the Pavlik Harness seems to be an effective and safe alternative, when used by experienced orthopedic surgeons.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241240367 – Supplemental material for Impact of Pavlik Harness treatment on motor skills acquisition: A case–control study
Supplemental material, sj-pdf-1-cho-10.1177_18632521241240367 for Impact of Pavlik Harness treatment on motor skills acquisition: A case–control study by Ana Rita Jesus, Catarina Pinto Silva, Inês Romão Luz, José Eduardo Mendes, Inês Balacó and Cristina Alves in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
The authors are grateful to all members of the Department of Pediatric Orthopaedics of our hospital and all participants and their families.
Author contributions
A.R.J. contributed to acquisition of controls’ data, statistical analysis, interpretation of data, bibliographic research, and drafting the article. C.P.S. contributed to acquisition of controls’ data, interpretation of data, review, and approval of the final article. I.R.L. contributed to designing the study, bibliographic research, acquisition of cases and controls’ data, interpretation of data, review, and approval of the final article. J.E.M. contributed to acquisition of controls’ data, interpretation of data, review, and approval of the final article. I.B. contributed to designing the study, acquisition of cases’ data, review and approval of the final article. C.A. contributed to designing the study, acquisition of cases’ data, review, and approval of the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethics Committee of our hospital center (approval no. 091-15). All participants provided signed informed consent before enrolling in this study. This paper is original work, reflecting the author’s own research and analysis. All sources used are properly disclosed. This not been previously published or being considered for publication elsewhere. All authors have been personally and actively involved in the making of this article, and all meaningful contributions properly credited.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.