
Abstract
Purpose:
The premature closure of the epiphysis of the distal radius is an infrequent condition in pediatric patients, often resulting in distal radius deformity. Currently, there is limited literature on its treatment, and controversy exists. This study aimed to evaluate the clinical efficacy of all-inside physeal bar resection with the aid of an arthroscope and patient-specific instrument.
Methods:
We retrospectively reviewed the patients who sustained distal radius physeal bar resection under all-inside visualization of the arthroscope with the aid of a patient-specific instrument during 2016–2022. Follow-up was performed for a minimum of 2 years, during which pre-operative and post-operative clinical and radiological parameters were compared.
Results:
There were six boys and two girls enrolled in this study. Six patients got satisfied results, while two patients didn’t benefit from the surgery. The mean pre-operative RAA of the affected side was −11.4° ± 13°, while the post-operative radial articular angle was 3.4° ± 11°. There was a significant difference between them. The mean pre-operative ulnar variance was 7.6 mm ± 6 mm, while the post-operative UV was 3.3 cm ± 8 mm. There was no significant difference between them. The pre-operative modified Mayo Wrist Score was 92 ± 5, while that for post-operative was 96 ± 7.
Conclusion:
All-inside physeal bar resection for partial physeal arrest of the distal radius with the aid of an arthroscopy and patient-specific instrument is minimally invasive, accurate, and safe. It should be the one option treatment for the premature closure of the distal radius epiphysis.
Introduction
Partial physeal arrest of the distal radius is often attributed to trauma, infection, neoplasms, and other factors, characterized by incomplete ossification of the epiphyseal plate.1,2 This can lead to the formation of a bone bridge, which adversely affects bone growth and development. The impact of the distal radius bone bridge on pediatric patients varies depending on its area, location, and the patient’s age, necessitating diverse treatment modalities. 3 The consequences of partial growth arrest include radial shortening, alterations in radial inclination and tilt, ulnocarpal impaction, injury to the triangular fibrocartilage complex, and incongruity of the distal radioulnar joint, which significantly impair the function and appearance of the wrist. 4
The resection of a physeal bar is currently a prevalently adopted therapeutic modality for the management of partial premature closure of epiphysis, which was initially documented by Langenskiöld in 1981. 5 The indications for bone bridge resection remain controversial, while the contemporary consensus among scholars is that patients with at least 2 years or 2 cm of growth remaining and less than 50% physeal area may benefit from physeal bar resection, which is responsible for the arrest. 6 Meantime, due to the significant individual variations in the area and location of the bone bridge, how to precisely resect the bone bridge while minimizing the potential of residual epiphysis injury remains a challenge for surgeons. Alongside the progression of medical technology, a multiplicity of forms of bone bridge excision has been evolved.7 –9 Satoshi Miyamura et al. conducted a physeal bar resection using a patient-specific guide with intramedullary endoscopic assistance for partial physeal arrest of the distal radius. 10 Takemura et al. employed computer navigation technology for physeal bar resection, achieving favorable clinical outcomes. 11 However, none of these approaches is capable of achieving a fully monitored physeal bar resection, while there remain few reports concerning the resection of the distal radius bridge.
In this study, we fabricated a sealed bone tunnel, augmented the water pressure, mitigated the volume of hemorrhage in the surgical field, clarified the surgical field, and accomplished the resection of the bone bridge under comprehensive endoscopic surveillance. We aim to evaluate the outcomes of all-inside distal radius physeal bar resection with the aid of patient-specific instrument and arthroscope, and provide a better understanding of the application of arthroscopically assisted physeal bar resection in the treatment of distal radius physeal bar growth arrest.
Methods
Patients
After obtaining approval from the institutional review board, we conducted a retrospective review of patients who experienced distal radius partial growth arrest and underwent physeal bar resection by Langenskiöld’s procedure using patient-specific instrument with arthroscope during 2016–2022. 12 Physeal growth arrest was determined through clinical examination and computed tomography findings. Patients who did not follow-up for a minimum of 2 years were excluded from this study. In total, eight patients who underwent surgery performed by the same surgeon were included in the final analysis. Patients were assessed regarding their pain levels and activity status, and underwent examination of wrist motion in both flexion-extension and pronation-supination before and after the surgical intervention. Computed tomography (CT) was used to evaluate the type of the physeal bar according to Peterson’s classification. 13 When a patient presents with two types of bone bridges, we classify it as the mixed type. 14 Wrist function was graded according to a modification of the Mayo Wrist Score (Table 1). 15
The modified Mayo Wrist Score.
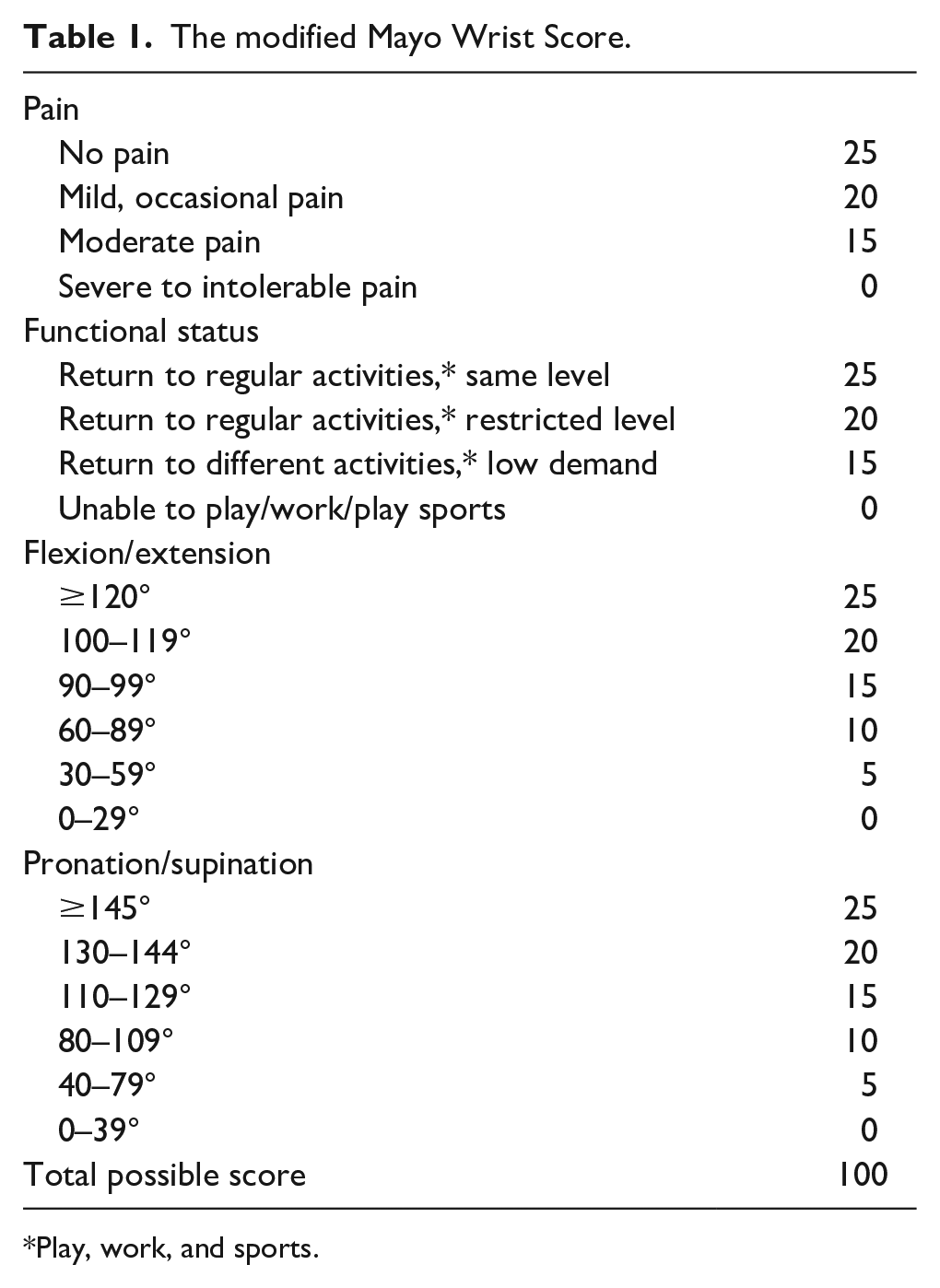
Play, work, and sports.
The standard forearm and wrist radiographs were taken in the anteroposterior and lateral views for the assessment of distal radius. The measurement of radial articular angle (RAA) and ulnar variance (UV) is shown in Figure 1 based on a previous report.16,17 The RAA and UV were measured by two pediatric surgeons at the last follow-up.
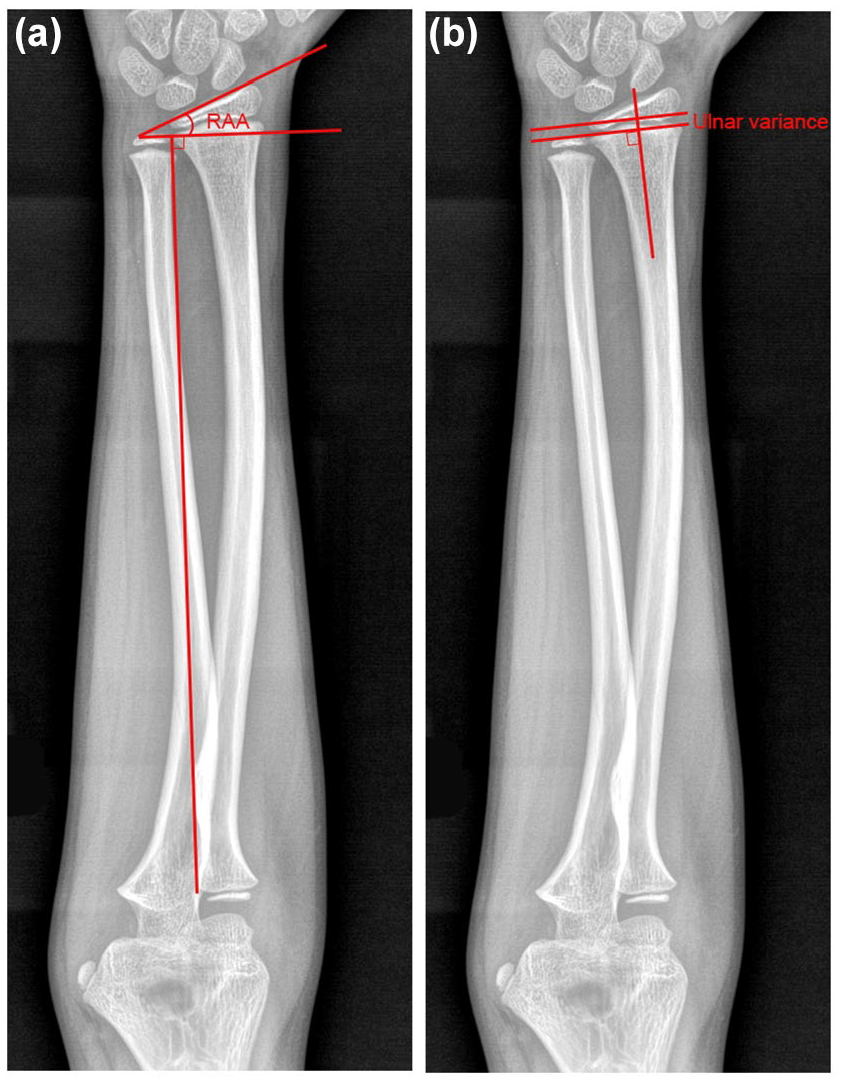
Diagrams showing the radiological measurements of RAA (a) and ulnar variance (b).
Patient‑specific guide
The bilateral digital CT image data was acquired for the generation of three-dimensional virtual surface models using the commercially available software package Mimics (Materialise, Leuven, Belgium). First, we performed simulated physeal bar resection on the virtual model. The radial cortex was selected as the entrance of the bone tunnel, and a multi-angle guide hole was made to accurately cover the epiphyseal plate in the region where the bone bridge was located, so as to facilitate the access of the lens or the drill. Based on this simulation surgery, the surgeon can generate patient-specific instrument (PSI) to facilitate the surgeon for establishing an appropriate bone tunnel and accurately replicate the pre-operative plan (Figure 2). Then, a full-size model and PSI were fabricated using ultraviolet curable resin.
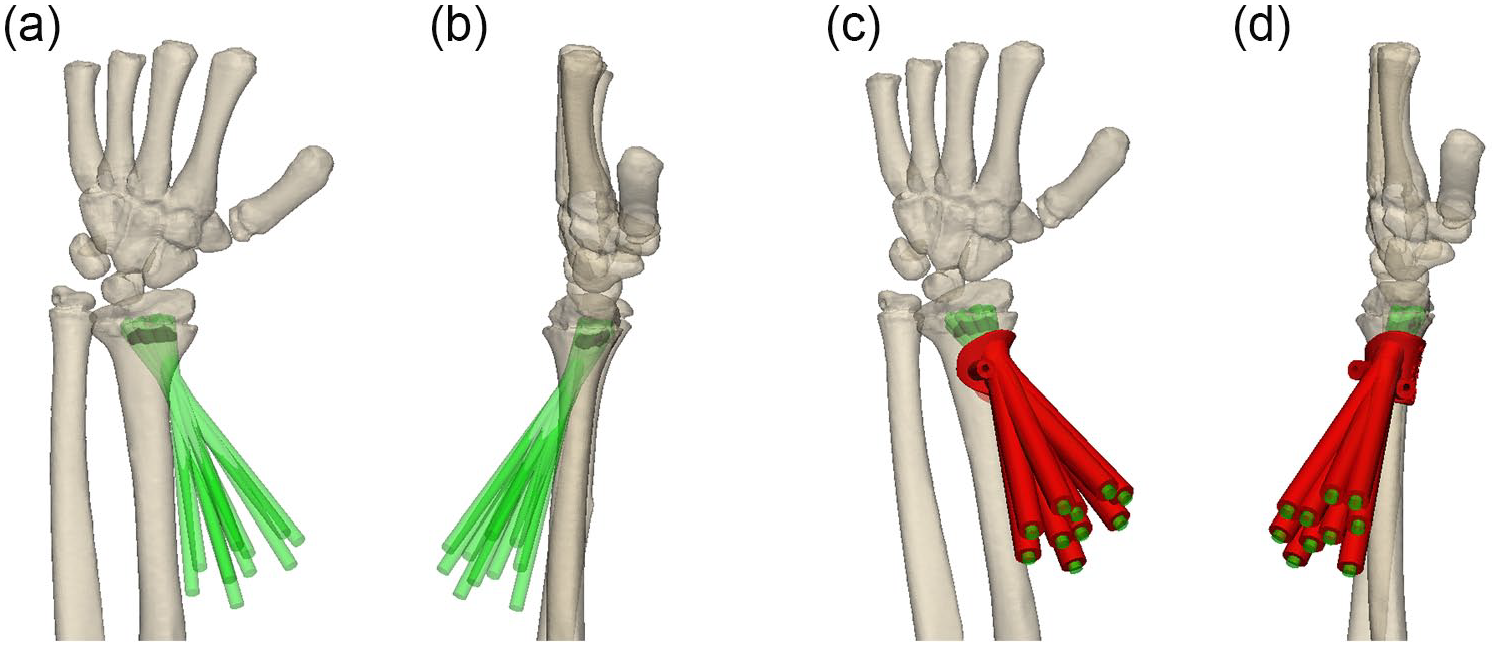
The procedure of PSI designing. (a) The anterior view of simulating surgery; (b) The lateral view of simulating surgery; The PSI (Red) guide for the direction of physeal bar resection at anterior view (c) and lateral view (d).
Surgical technique
The physeal bar resection was performed based on a previous report. 18 After administering general anesthesia, the patient was supine on the operating table with the affected limb extended and the tourniquet applied to the proximal end of the upper extremity. Prior to the surgery, once the epiphysis was located through fluoroscopy, a 5-cm surgical incision was made on the lateral end of the distal forearm and beneath the epiphysis of the radius. The surgeon dissected layer upon layer until reaching the radial surface and installed the PSI with two Kirschner wires fixing it.
There were 8 to 10 guide channels on each PSI, and drilling was carried out through the guide channel of the PSI. The guide was removed after drilling each channel. After conducting a preliminary cleaning of the artificial bone tunnel once again, a closed cavity of the bone tunnel was established by suturing the soft tissue of the wound. A 2.7 mm arthroscope lens was inserted through the wound gap to maintain the water pressure of the water entry channel, enabling the surgery field to have a certain degree of hemostatic effect under the action of water pressure and keeping the surgery field relatively clear. The bony bar was removed under an all-inside endoscope by inserting a drill through the wound gap until normal epiphysis was encountered at the last surgical step. After flushing with saline, the defect was filled with bone wax. Care was taken to avoid damage to the periosteum and the articular surface of the distal radius (Figure 3).
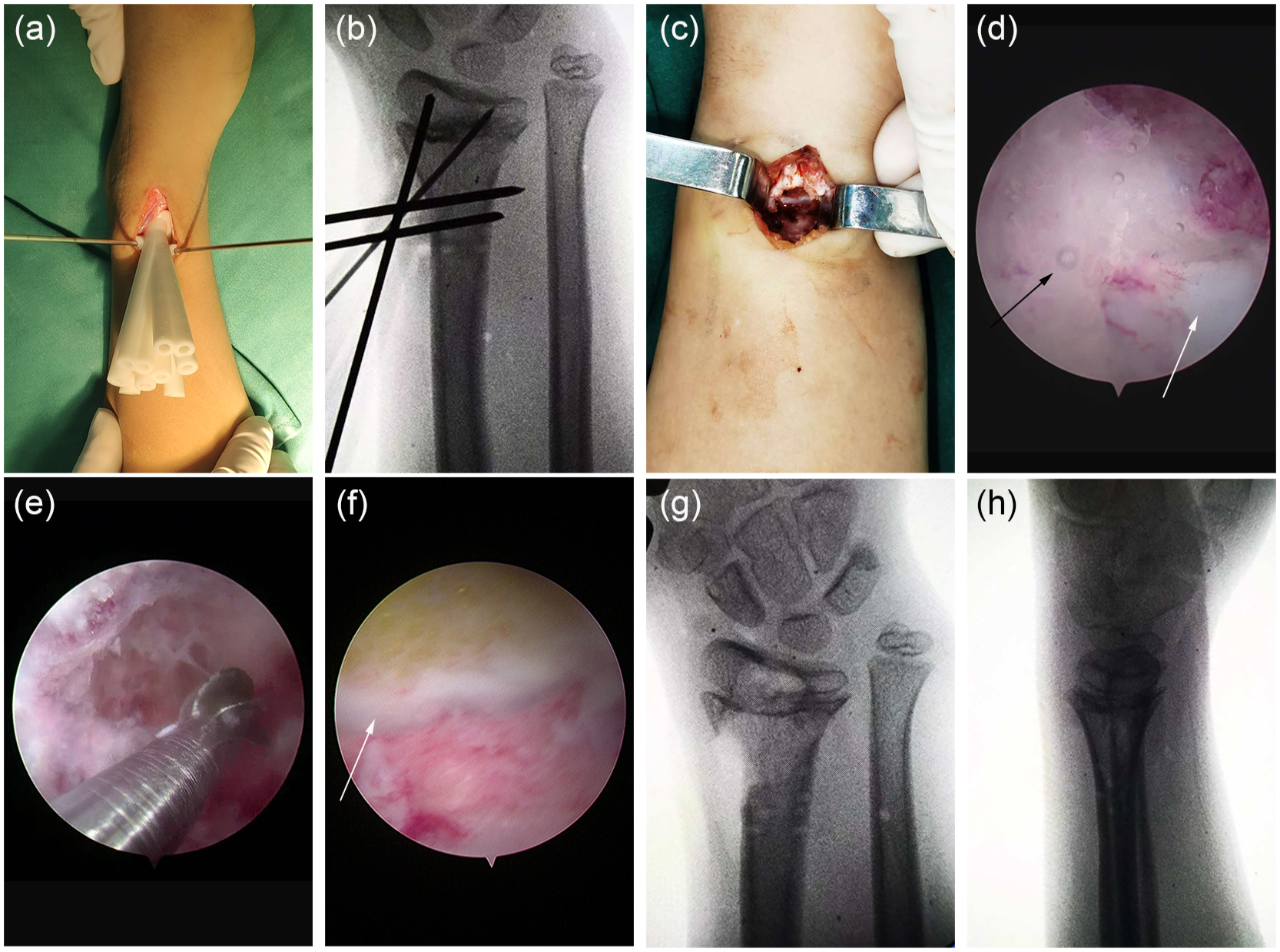
The surgical procedure under the aid of PSI and arthroscope. (a) Install the PSI; (b) Establish the bone tunnel with the aid of PSI; (c) General view of the bone tunnel entrance; (d) The view of the epiphysis after the bone tunnel was established. The epiphysis was not continuous. The white arrow showed epiphysis, while the black arrow showed the physeal bar; (e) The view of physeal bar removed by dental drill; (f) The view of epiphysis after the physeal bar was removed. The white arrow showed that the epiphysis was continuous; (g) Anteroposterior view and (h) lateral view of the wrist after physeal bar resection.
After surgery, a wrist brace was applied for 4 weeks to avoid a secondary fracture. Then, wrist movement was permitted as tolerated by the patient. Radiograph data were obtained to evaluate the effect of the operation during follow-up.
Data were presented as mean with min-max ranges for continuous variables, and percentages for categorical variables. We used the paired t-test to compare two dependent means of variables in patients. Statistically significant differences were considered when p < 0.05.
Results
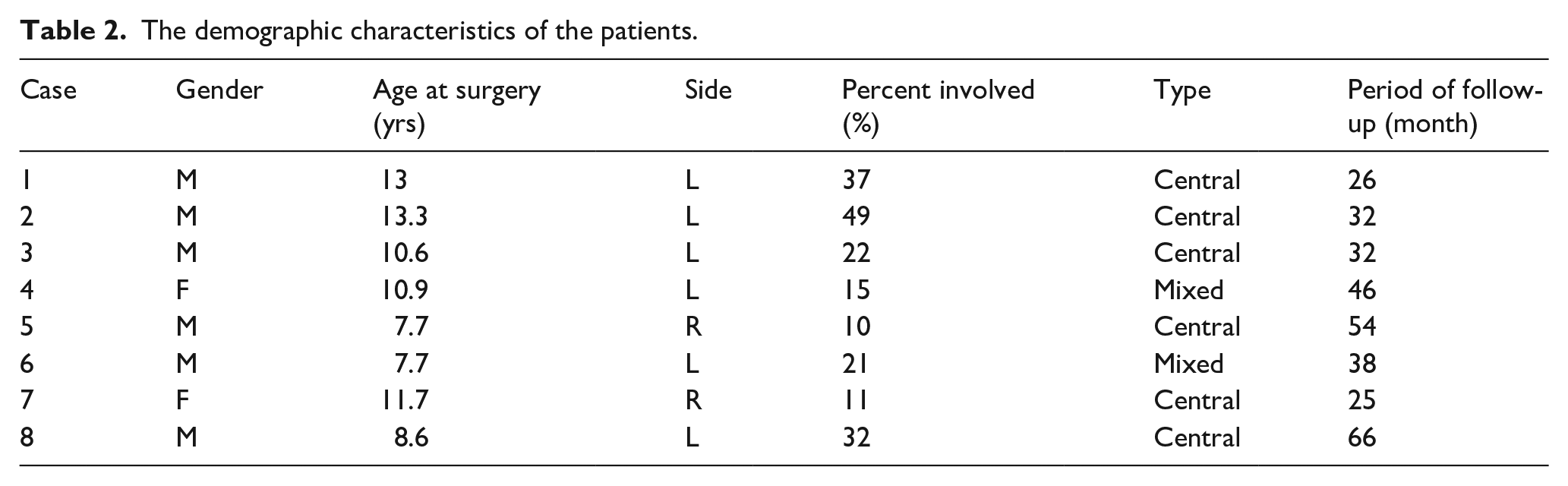
There were six boys and two girls enrolled in this study. All patients presented with a history of distal radius fracture and were identified with manifestation of wrist malformation. The average age at surgery was 10.4 ± 2 years (range 7.7–13.3). The percent of the bar area was 24.6 ± 13.7% (range, 10–49). The average follow-up time was 39.9 ± 15 months (range 25–66). The demographic characteristics of the eight patients are shown in Table 2.
The demographic characteristics of the patients.
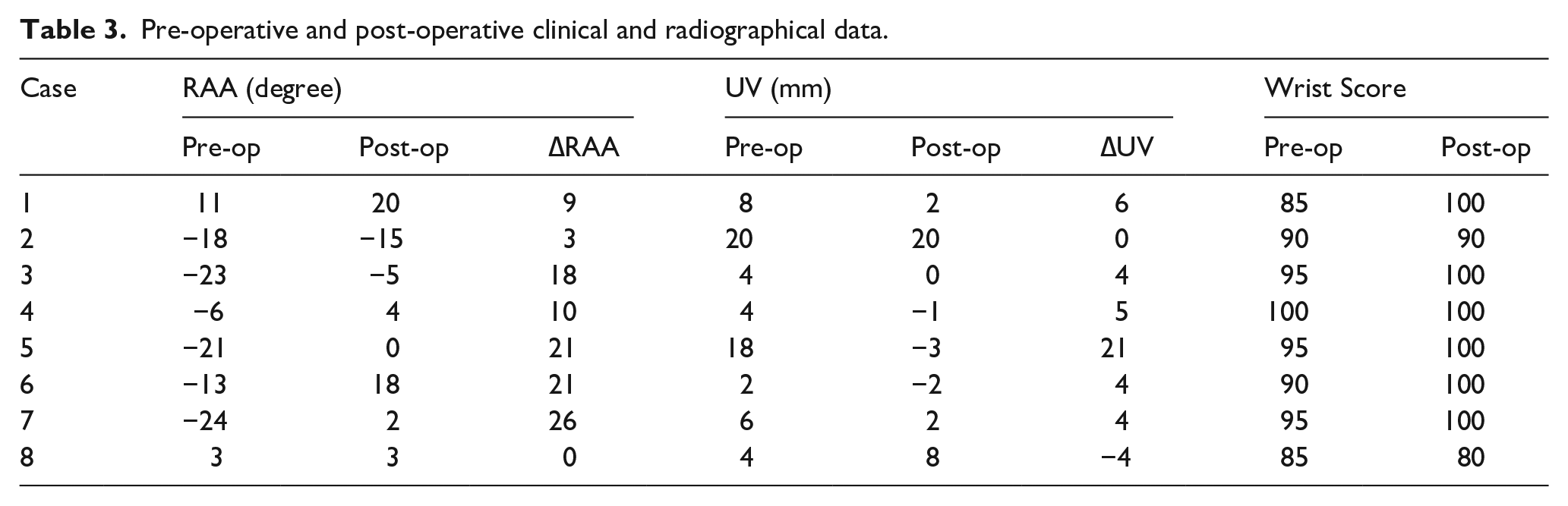
There were six patients who got satisfied results, while two patients didn’t benefit from the surgery. The mean pre-operative RAA of the affected side was −11.4° ± 13° (ranging from −24° to 11°), while that for the normal side was 21.6° ± 2° (ranging from 19° to 25°). The post-operative RAA of the affected side was 3.4° ± 11° (ranging from −15° to 20°). There was a significant difference between the pre-operative and post-operative RAA (p = 0.007). The ΔRAA was 14.8 ± 11° (ranging from 0° to 31°). The mean pre-operative UV was 7.6 mm ± 6 mm (ranging from 2 mm to 18 mm), while the post-operative UV was 3.3 cm ± 8 mm (ranging from −3 mm to 20 mm). There was no significant difference between the pre-operative and post-operative UV (p = 0.16). The ΔUV was 4.4 mm ± 8 mm (ranging from −5 mm to 21 mm). Our macroscopic evaluations confirmed significant improvement in wrist radial deviation deformities among six pediatric cases. The pre-operative modified Mayo Wrist Score was 92 ± 5, while the post-operative one was 96 ± 7. The pre-operative and post-operative parameters are outlined in Table 3.
Pre-operative and post-operative clinical and radiographical data.
In Case 1, it can be observed that the epiphysis of the distal radius is partially closed. The angle of the articular surface of the distal radius has decreased significantly and was radial inclination. The radius has shortened, and the distal epiphysis of the radius is significantly lower than that of the ulna. After surgery, the retarding effect of the bony bar vanished, and the growth of the distal epiphysis of the radius resumed. At the post-operative 2 years, the distal articular surface angle of the radius was significantly enhanced, the growth rate of the radius recovered, and the disparity in the length of the radius was ameliorated (Figure 4).
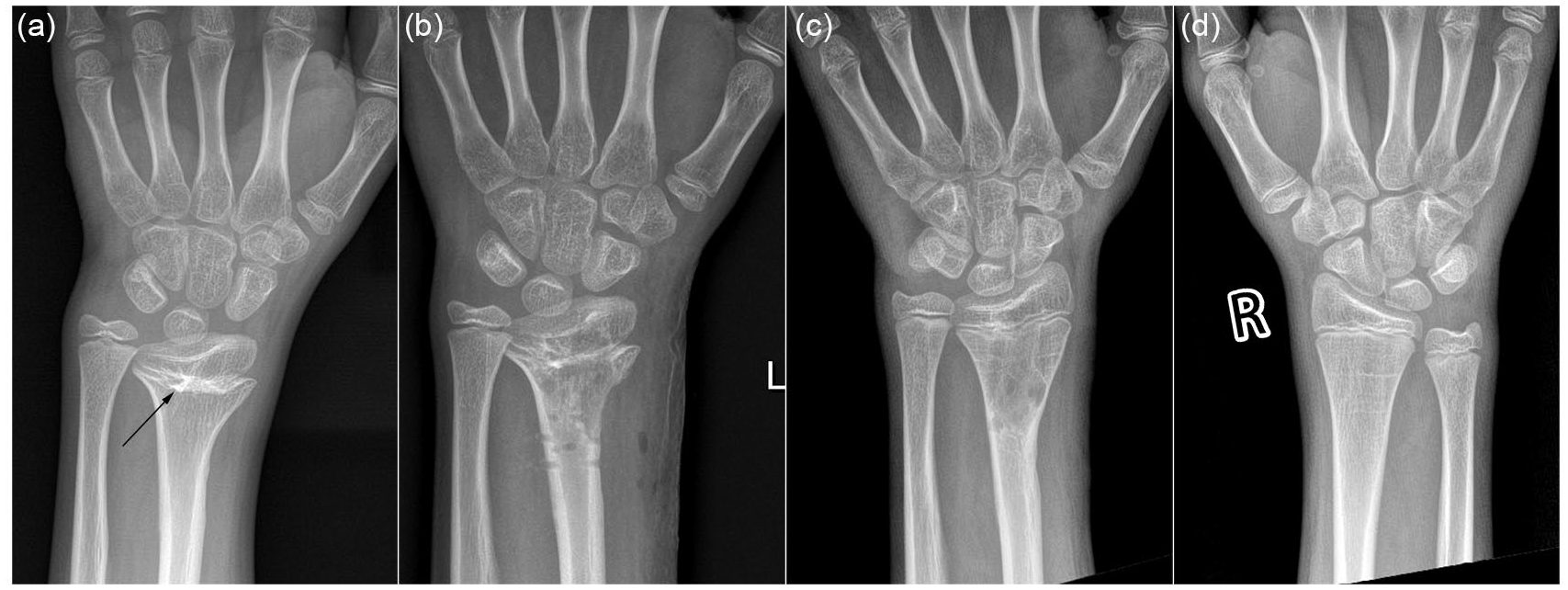
The radiographs of the affected wrist at different follow-up times: pre-operative (a), post-operative Day 1 (b), and post-operative 2 years (c). The radiography of the normal wrist (d). The arrow in (a) shows the location of the physeal bar.
At the post-operative 2 years, there was no obvious deformity in the wrist of the child, and no obvious limitation in flexion, extension, and rotation of the wrist in Case 6 (Figure 5). There were no post-operative fractures, infections, or intraoperative complications such as neurovascular injury among these patients.

The photographs of movement in Case 6 at post-operative 2 years. Extension (a), flexion (b), pronation (c) and supination (d).
For Cases 2 and 8, the patients showed no significant improvement in RAA, UV, or modified Mayo Wrist Score during post-operative follow-up. Case 2 underwent radial deformity correction osteotomy and ulnar lengthening due to insufficient growth potential (<2 years remaining growth) at 6 months follow-up, while Case 8 underwent ulnar lengthening surgery at 2 years follow-up.
Discussion
The incidence of premature closure of the epiphysis of the distal radius is between 1% and 7%. 15 As the distal radius physis is responsible for 75% of the longitudinal growth of the radius and the injured epiphysis is incapable of regeneration, the physeal bar frequently leads to serious deformation and is difficult to manage. 19 So far, it still presents a significant challenge to orthopedic surgeons. In this study, we precisely located the position of the physeal bar at the distal radius through pre-operative CT. Then, we made a suitable tunnel by the PSI. With the modified arthroscopically assisted procedure, the physeal bar was removed precisely and completely. Excellent outcomes were achieved in most of these patients.
The management of premature closure of the distal radius epiphysis remains controversial. Categories of treatment options include observation, physeal bar resection, epiphysiodesis, ulnar shortening, radial osteotomy, and distraction osteogenesis.1,15,20 Decision-making should base on patient age, remaining growth potential, location of injury within the physis, size of physeal bar, angular deformity, and individual patient and family desires.6,9 Given the significant trauma associated with ulnar shortening, radial osteotomy, and distraction osteogenesis, especially in younger children (< 10 years old), where multiple and staged operations might be necessary to rectify the deformity, we contend that physeal bar resection is the preferred treatment for children with a bone bridge area < 50% and a high growth potential for the following reasons. First, once the coalescent effect of the physeal bar is eliminated, most of the deformities of the distal radius will be rectified. Second, some deformities are not rectified. However, physeal bar resection can delay the progression of the deformity, thereby reducing the difficulty of subsequent surgery. Third, even if physeal bar recurs, physeal bar resection does not augment the difficulty of subsequent surgeries. The surgeon still possesses other alternatives to continue rectifying the deformity of the distal radius.
Despite the fact that physeal bar resection can conspicuously ameliorate the degree of deformity in certain children, we need to closely monitor the recovery of the epiphysis growth after physeal bar resection to prevent any further aggravation of the radial deformity in cases of surgical failure. In our research, six patients exhibited marked improvement in radial inclination deformity, and two patients with exacerbated deformity underwent radial distraction osteogenesis surgery. We attribute the unsatisfactory outcome in Case 2 primarily to the extensive physeal bar involvement coupled with limited residual growth potential at the distal radius. For Case 8, we speculate that incomplete resection of the physeal bar likely contributed to its recurrence. In our opinion, at least six months following surgery, the further exacerbation of the deformity serves as our indicator for conducting osteotomy or traction surgery. Due to the insignificant correction of radius length, we are inclined to conduct ulnar shortening, radial lengthening, or epiphysiodesis surgery concurrently with physeal bar resection in children with severe shortening.
The difficulty of the operation varies in accordance with the location of the physeal bar.21,22 In numerous instances, the surgeon is overly concerned about epiphysis injury, and the physeal bar resection is incomplete, leading to suboptimal clinical outcomes after the surgery. Generally, peripheral bone bridges and linear bone bridges are relatively easy to locate and considerably straightforward to resect. 3 However, for the central bone bridge, it is difficult to expose, thereby making it challenging to resect. The most significant challenge of the physeal bar resection lies in minimizing the damage to the normal epiphysis while achieving complete removal of the physeal bar. Currently, there are scarce literature reports on the physeal bar resection of the distal radius. Nevertheless, numerous scholars have investigated the surgical methods for the bone bridge of the distal femur, proximal tibia, and distal tibia. Jackson modified the Langenskiöld procedure and made the physeal bar resection more directly by cutting a pre-drilled and tapped wedge of metaphysis as a window. 23 Stricker utilized an arthroscope to optimize the visualization for the resection of central physeal bridges via small metaphyseal windows. 24 Still, the surgical field of vision is highly indistinct as it fails to completely cease the bleeding. Xiao modified it to make physeal bar resection under all-inside arthroscopic visualization feasible in distal femur and proximal tibia, using clamps to form a closed osteocavity. 18 Due to the small size of the distal radius, it poses a difficulty for the surgeon to operate within a confined space without causing harm to the normal epiphysis by these methods. In this study, by designing a suitable bone tunnel with a PSI and combining it with a 2.7 mm arthroscopic lens, the surgeon is capable of obtaining a favorable surgical field of view and achieving physeal bar resection under all-inside arthroscopic monitoring.
Nevertheless, there were certain limitations in this study. Firstly, due to the small sample size and the limited follow-up period, we have no evidence that its surgical effect will eventually outperform the traditional methods. Up to now, this method still requires further improvement for application in radial physeal bar resection because of the limited space. Nonetheless, further confirmatory studies involving a larger number of patients are necessary to validate the reliability of this modified technique.
Conclusion
All-inside physeal bar resection for partial physeal arrest of the distal radius with the aid of arthroscopy and patient-specific instrument is minimally invasive, accurate, and safe. It should be the one option treatment for the premature closure of the distal radius epiphysis.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251358639 – Supplemental material for All-inside physeal bar resection for partial physeal arrest of the distal radius with the aid of an arthroscope and patient-specific instrument
Supplemental material, sj-pdf-1-cho-10.1177_18632521251358639 for All-inside physeal bar resection for partial physeal arrest of the distal radius with the aid of an arthroscope and patient-specific instrument by Han Xiao, Baohui Xiao, Xiaoqian Tan, Qian Tan, Weihua Ye, Jiangyan Wu, Renfei Li, Haibo Mei, Guanghui Zhu and An Yan in Journal of Children’s Orthopaedics
Footnotes
Authors’ Note
Han Xiao is also affiliated to Hunan Provincial Key Laboratory of the Research and Development of Novel Pharmaceutical Preparations, “The 14th Five-Year Plan” Application Characteristic Discipline of Hunan Province, College of Pharmacy, Changsha Medical University, Changsha, P. R. China.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Hunan Provincial Health Commission scientific research project (B202304078478), Natural Science Foundation of Hunan Province, China (Grant No. 2023JJ40350), Natural Science Foundation of Hunan Province, China (Grant No. 2023JJ60450), and The Young Talents of 1233 program of Hunan Children hospital.
Contributors’ statement
A. Y. and H. X. designed experiments. H. X., G. Z., B. X., X. T., Q. T., J. W., W. Y., R. L., and H. M. measured and collected the data. A. Y. and H. X. analyzed the data. H. X. and A. Y. wrote the article. H. X., G. Z., B. X., X. T., Q. T., J. W., W. Y., R. L., and H. M. revised the article.
Ethical approval
This is a retrospective observational study involving human participants, and it was approved by Ethics Committee of Hunan Children’s Hospital (KSYQ2025-16).
Consent to participate
All participants gave informed consents.
Consent to publish
This work is approved by all authors for publication in Journal of Children’s Orthopaedics.
Availability of data and materials
My article has the data included as electronic supplementary materials.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.