
Abstract
People living with the rare, genetic condition Duchenne muscular dystrophy have particular orthopaedic care needs that are not universally understood or implemented at sites across the UK, putting them at risk of not receiving the correct treatment. They may require orthopaedic management and intervention for contractures caused by their muscle weakness. Importantly, they are also at a high risk of fractures due to increased bone fragility as part of the nature of Duchenne muscular dystrophy but also resulting from reduced weight-bearing and from the long-term use of corticosteroids as standard of care. In addition, progressive skeletal muscle weakness increases the risk of falls that may cause fractures. DMD Care UK’s orthopaedic working group has developed a guideline by consensus to inform all those involved in the orthopaedic management of people with Duchenne muscular dystrophy about the care needs and imperatives. This covers children and adults and focuses on fracture management and elective orthopaedic procedures. The guideline has been endorsed by the British Society for Children’s Orthopaedic Surgery.
Background: About Duchenne muscular dystrophy
Duchenne muscular dystrophy (DMD) is a rare, genetic muscle-wasting condition caused by mutations in the DMD gene which codes for the protein dystrophin.1,2 This is located on the X-chromosome and inherited via an X-linked recessive pattern, meaning that affected individuals are almost always male, although there are some, very rare, manifesting female carriers. In addition, a significant minority of carrier mothers develop dystrophinopathy-related cardiomyopathy and therefore need regular cardiac monitoring. 3 Around 60% of mutations are inherited from the mother and 40% are de novo mutations. 4 In all cases, the production of functional dystrophin is almost or completely absent. DMD affects around 1 in 5000 live male births. 5
Dystrophin is required for effective muscle function and repair. Without it, muscles are damaged over time and replaced with fatty and fibrous tissue, resulting in a progressive loss of function. All muscle tissue is affected, which means an inevitable impact on movement, heart, breathing and digestive systems. The brain is also affected, although this is currently less well understood. Learning difficulties, speech and language delay, autism spectrum disorder, attention deficit hyperactivity disorder and anxiety disorders are more common in people with DMD than in the general population. Brain involvement does not appear to be progressive. 2
Ambulation is lost on average at 11–13 years of age, with cardiac and respiratory involvement becoming significant in the later teens and representing the most frequent cause of death. In the UK, the median life expectancy is around 29 years. 6
The complex, multi-systemic nature of DMD brings with it complex, multi-disciplinary care needs. 7 Combined with the rarity of the condition and resource pressures in healthcare, this complexity means that care delivery may not be comprehensive and may not be optimised for the best possible health outcomes.
Early recognition and diagnosis are therefore important to meet these complex needs from the outset, and to provide adequate family-planning counselling and support for any behavioural or learning needs. Newborn screening programmes for DMD do not yet exist in the UK and if they are introduced, some children will still be missed. This is of particular relevance to orthopaedics because undiagnosed boys may first present to an orthopaedist with delayed ambulation, difficulty rising from the floor (using the Gower’s manoeuvre), large calves and other movement issues. A diagnosis of DMD should be considered and appropriate investigations should be undertaken, including blood creatine kinase levels, which are unequivocally elevated in DMD. 8
Scope and methodology
To address this, a collaborative programme was established to develop and agree on UK-relevant, practical standard of care guidelines based on evidence and expert clinical experience and opinion. DMD Care UK is a joint initiative between the John Walton Muscular Dystrophy Research Centre at Newcastle University and Duchenne UK, a leading patient charity. It is embedded in the UK’s North Star Network of Specialist Neuromuscular Centres and, to date, has established 13 working groups, each looking at a specific area of care for DMD.3,9,10
This article outlines a consensus recommendation on orthopaedic care and management for children and young people living with DMD in the UK. The authors represent DMD Care UK’s orthopaedic working group (WG), established in February 2023 with members recruited from UK orthopaedic surgeons with significant experience in DMD, representatives from the British Society for Children’s Orthopaedic Surgery (BSCOS), neuromuscular consultants, specialist physiotherapy, orthotics, endocrinology and patient representatives. Levels of clinical experience, agreement to proactive participation and geographical spread were the key factors in finalising membership. The group is supported by the project management team of DMD Care UK in Newcastle.
The international guidelines on orthopaedic treatment and management of people living with DMD were taken as the starting point for this group. 11 The limited additional evidence published since on orthopaedic care and management in DMD was reviewed by the lead author and other authors and shared with the wider WG. Key statements were proposed based on this, on the WG’s clinical experience and on the infrastructure of healthcare delivery within the UK. Three rounds of review and revision of the key statements with supporting discussion, evidence and references where available were conducted by the WG. This draft was presented to BSCOS at an internal meeting by the lead author, approved and then shared with the North Star network of neuromuscular centres (orthopaedic surgeons and neuromuscular consultants) for review. Resulting comments were addressed and a final version was signed off by the DMD Care UK orthopaedic WG and BSCOS.
We present here a summary of that final guideline.
Overview and key principles for orthopaedic care in DMD
Orthopaedic care is an area of particular priority for people with DMD for a number of reasons.
Widespread use of long-term corticosteroids along with reduced weight-bearing, has a negative impact on bone health. Meanwhile, the pathophysiology of DMD itself also impacts bone health from the beginning.12,13
Low-trauma long bone and vertebral fractures are extremely common.14–17 Fracture incidence is reported to be approximately four times higher in children and adolescents with DMD compared with healthy growing children. 17 Fracture incidence is reported to be approximately twice as high in adult men with DMD compared to healthy men. 18
Corticosteroid increases the risk of fracture. Whilst the use of daily corticosteroids has a greater impact on muscle function, the daily regimen has been shown to be associated with a higher risk of fracture compared with the intermittent regimen, with one study reporting the highest fracture incidence in boys treated with daily deflazacort.17,19–23 As skeletal muscles weaken, falls are a bigger risk, further increasing the chance of fractures.
When ambulant individuals have a fracture, being immobilised for any significant period of time can significantly impact their ability to regain ambulation and lead to a dramatic loss of bone density.24–26
The risks of fat embolism syndrome (FES) are higher than in people without DMD – even where there is no obvious fracture or significant trauma.27,28
The DMD Care UK orthopaedic guideline has a significant focus on the management of long bone fractures to make sure that decisions taken are based on evidence and expert opinion and result in the best outcome possible for patients. Important considerations for elective surgery are also presented. There are some key underlying principles that inform this guideline. These are highlighted in Box 1.
Preserving mobility and independence by maintaining weight-bearing status and/or wheelchair use is a priority in patients with Duchenne muscular dystrophy (DMD). 11
A patient with an acute injury is likely to present to their local trauma unit. Unnecessary patient transfers must be avoided, and appropriate fracture management may be delivered locally if the necessary medical and anaesthetic expertise is available and as long as there is a prior discussion with the regional specialist centre.
Direct communication between senior clinicians is key to safe management in this patient group.
Most patients with DMD take corticosteroid medication (prednisolone, deflazacort or vamorolone) which leads to bone fragility and increased fracture risk.11,16
Long-term treatment with corticosteroids means that patients are at risk of adrenal insufficiency due to adrenal suppression (see Endocrine Guidelines: https://dmdcareuk.org/clinical-recommendations). 8 Extra corticosteroids are needed when corticosteroid-treated patients with DMD present with a fracture. Extra corticosteroids, given intravenously, are also needed during any surgical procedure in these patients. Further information on the management of adrenal insufficiency (children, adolescents and adults) during the peri-operative period can be obtained via NICE. 35
Fat embolism syndrome (FES) is a particular risk for patients with DMD, with fatalities reported.28,36 It has been reported in DMD even after minor trauma 27 and should always be considered as a differential diagnosis. Warning: the symptoms and signs of fat embolism present within 72 h of fracture or injury, but may be subtle.
In the UK, North Star centres coordinate care for children with DMD and can advise specialist care (Appendix A). The adult North Star network can help guide care for adult patients. 37
All patients with DMD should be under the care of a specialist neuromuscular MDT with links to a specialist orthopaedic team when needed, but a regular review by an orthopaedic surgeon should not be necessary.
It is important to remember that DMD is a multi-systemic condition and patients’ needs are often complex. Cardiac and respiratory involvement, as well as chronic treatment with corticosteroids and risk of adrenal crisis, mean that DMD patients should always be considered at high surgical/anaesthetic risk. Therefore, management should be multi-disciplinary and performed in a centre with the appropriate expertise. Surgical management of fractures should only be conducted at DMD-experienced centres that can provide the necessary anaesthetic and/or critical care support. Complex surgical procedures should only be done in hospitals with critical care facilities.
Elective orthopaedic management
Fatty infiltration of muscle and the development of fibrotic tissue in DMD result in contractures, which may require orthopaedic management. 29 If a decision is made that elective surgery for contractures is appropriate, this should only be conducted at specified centres that can provide the necessary anaesthetic and/or critical care support and always in conjunction with the patient’s existing neuromuscular team. This is likely to be at one of the North Star Centres (Appendix A) – a well-established UK network of paediatric neuromuscular expertise. It is also important to include their specialist physiotherapy and orthotics teams. Box 2 outlines the key considerations for elective (non-emergency) orthopaedic management of people with DMD. A summary of these recommendations is given in Figure 1 alongside the same for acute management of fractures (also discussed below).
The aim of elective orthopaedic surgical intervention in ambulatory patients is to maintain motor function for as long as possible. The aim of surgery in non-ambulatory patients is to allow comfortable, balanced sitting and functional upper limb use.
Patients should have a home stretching programme and regular physiotherapy input to try to prevent joint contractures. Ankle-foot orthoses (AFOs) can be considered when there is reduced ankle dorsiflexion (consider night-time use in ambulatory and daytime use in non-ambulatory patients).
A decision to proceed with surgery should involve the patient, family and multi-disciplinary team (physiotherapist, occupational therapist, orthotist, neurologist, community paediatrician, cardiologist, respiratory specialist, anaesthetist and orthopaedic surgeon).
The patient should have a full respiratory and cardiac review before surgery.3,10 A critical care bed should be available following surgery.
In an ambulatory patient with equinovarus ankle contractures (together with good quadriceps and hip extensor strength), Achilles tendon lengthening can be considered. Regular post-operative physiotherapy input is needed. Surgery at the hip and knee level is generally not recommended.
In patients in the early non-ambulatory phase with equinovarus ankle contractures, Achilles tendon lengthening may be considered to allow the feet to sit comfortably on wheelchair footplates or if unable to find comfortable footwear.
Regular skin checks (with plaster removal) are required in the post-operative period to prevent pressure ulcers. Wound healing can be affected by long-term treatment with oral corticosteroids and should be carefully monitored. Following plaster removal, a post-operative AFO may help prevent contracture recurrence.
In the late non-ambulatory phase, the risks of surgery are higher. However, surgery should still be considered after careful discussion, particularly if the patient has significant pain or recurrent skin problems.
The patient and family must be aware of the significant risks associated with surgery. These include wound infection and wound breakdown, worsening cardiac function, respiratory problems, pressure ulcers from plasters, pain, fat embolism and a small risk of death. The patient may need admission to a critical care facility following surgery and may require ventilatory support for an unknown length of time.
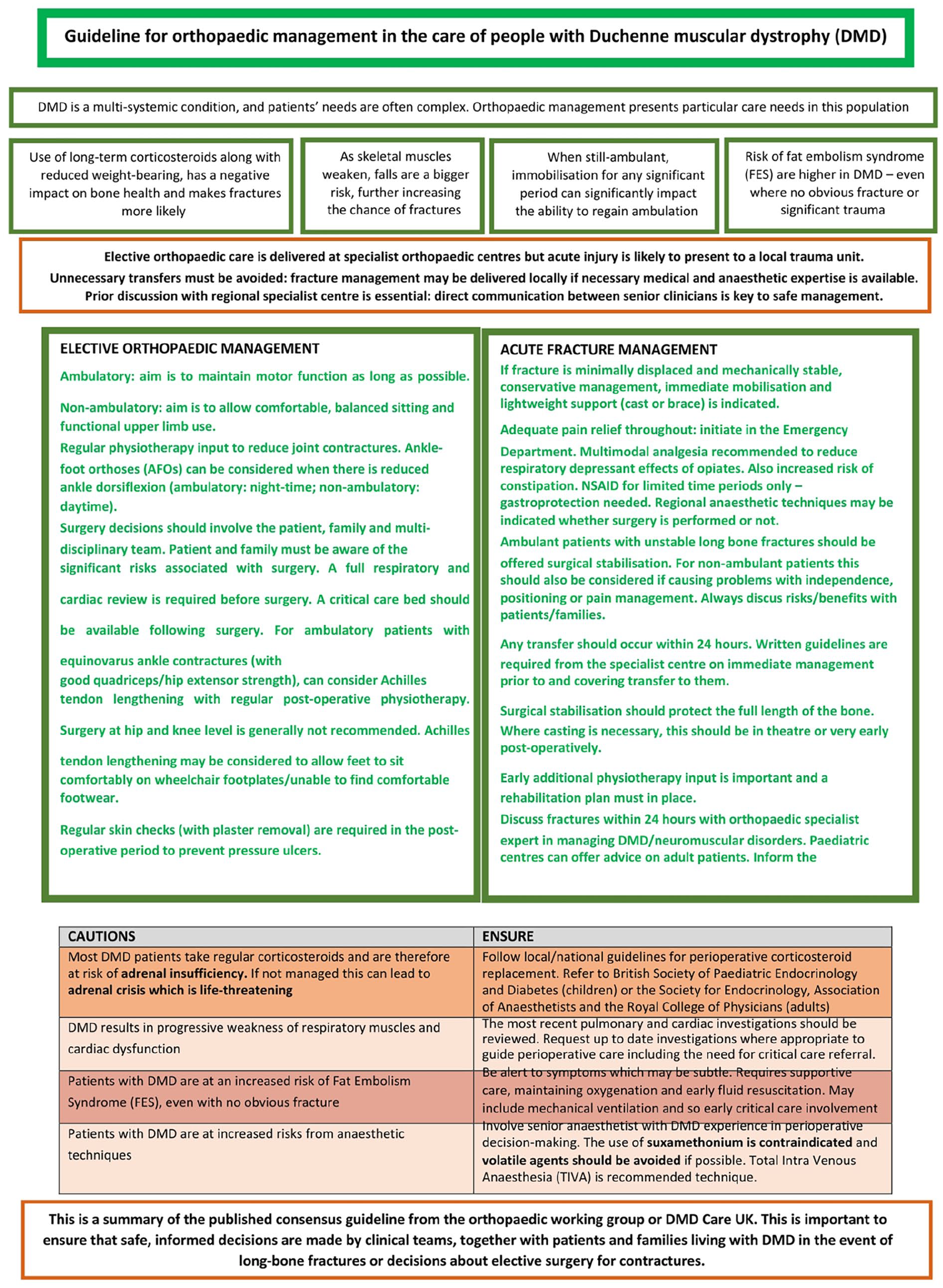
Summary for orthopaedic management in DMD. DMD: Duchenne muscular dystrophy.
Fracture management
Whilst elective orthopaedic care will be delivered at specialist orthopaedic centres, a patient with an acute injury is likely to present to their local trauma unit. However, unnecessary patient transfers must be avoided, and appropriate fracture management may be delivered locally if the necessary medical and anaesthetic expertise is available and as long as there is a prior discussion with the regional specialist centre. We consider that direct communication between senior clinicians is key to safe management in this patient group.
We list below some key considerations for fracture management in these patients, which are also summarised in Figure 1.
Many fractures in DMD patients are minimally displaced and mechanically stable. In these cases, conservative management with immediate mobilisation with lightweight support using a cast or brace is indicated. 30
Adequate pain relief must be given throughout and initiated in the Emergency Department. The use of multimodal analgesia is recommended to reduce the potential respiratory depressant effects of opiates in patients with reduced reserves. Use of nonsteroidal anti-inflammatory drugs should be for limited time periods only and gastroprotection should be provided. This is particularly important when combined with corticosteroids. Be aware that constipation is an increased risk in people with DMD and this can be exacerbated by opioid drugs. 31 Their use should be carefully considered.
Regional anaesthetic techniques may be indicated whether surgery is performed or not. Single nerve blocks or nerve infusion catheters should be considered. Ultrasound guidance is recommended where body habitus and/or joint contractures prove a challenge.
Ambulant patients with unstable long bone fractures should be offered surgical stabilisation. This is to enable immediate weight-bearing or upper limb use to optimise muscle function, joint position and maximise the chances of preserving independent mobility and function. A discussion about potential risks and benefits with the patient/family is required.
In non-ambulant patients with an unstable long bone fracture, surgical stabilisation should also be considered and discussed with patients/families if causing problems with independence, positioning or pain management.
Once transfer to a specialist centre for surgical fracture management is agreed upon, the transfer should occur within 24 h. The initial admitting centre should be provided with written guidelines from the specialist centre on immediate management prior to and covering transfer to the specialist centre.
Surgical stabilisation of long bone fractures should protect the full length of the bone. Combined intramedullary and plate fixation, or double plate fixation, should be considered in metaphyseal fractures where bone fragility compromises stable intramedullary fixation.
Where casting is necessary, the knee should be cast in maximal extension and the ankle at 90° (or maximum dorsiflexion if already restricted) to avoid flexion contractures. In this case (where the knee is in maximum extension), upright sitting will not be possible, so a reclining wheelchair should be provided. Casting should be done and applied in theatre or very early post-operatively.
Occupational therapy, physiotherapy and wheelchair services should be involved pre-operatively, where possible, to ensure appropriate seating and equipment for transfers are available post-operatively. Moving and handling assessments should be carried out as required.
Early additional physiotherapy input should be ensured to prevent contractures to injured and non-injured limbs during the recovery period. Intensive onward rehabilitation must be in place to regain independence. Fracture healing may be rapid, so joint motion may be able to be re-established early. A documented rehabilitation plan must be in the inpatient notes, shared with the patient/carers and passed on to community services.
All long bone or disabling fractures in children and young people (<19 years old) should be discussed for advice with a children’s orthopaedic surgeon at a local designated children’s trauma centre within 24 h of presentation (a list of children’s trauma centres with necessary expertise and facilities is given in Appendix B). The patient’s usual neuromuscular care team should be informed at the same time.
The management of fractures in adult patients (generally those who are 19 years and older) follows the same principles as in younger people and carries the same risks. We advise discussion with the regional specialist children’s orthopaedic team wherever possible in view of their greater experience of the condition and ask them to liaise with the admitting adult service as appropriate. In all cases, fractures in DMD should be discussed with an orthopaedic specialist with expertise in managing DMD and/or neuromuscular disorders. The patient’s neuromuscular care team must be informed at the same time.
Important considerations across orthopaedic care
Whether a person with DMD presents in an emergency following a fall or fracture, or whether the orthopaedic team is involved in elective surgical management or other intervention, there are several imperative factors to consider.
Use of corticosteroids – Most DMD patients take regular corticosteroids and are therefore at risk of adrenal insufficiency. For these patients, corticosteroid replacement is a vital part of perioperative management and local/national guidelines should be followed appropriately.
Detailed national guidance for the management of paediatric adrenal insufficiency (including during surgical procedures) has been developed by the British Society of Paediatric Endocrinology and Diabetes: https://www.bsped.org.uk/adrenal-insufficiency
For adults, the guidance of the Society for Endocrinology, the Associations of Anaesthetists and the Royal College of Physicians should be followed. 32
Cardiopulmonary assessment – DMD results in progressive weakness of respiratory muscles and cardiac dysfunction. The most recent pulmonary and cardiac investigations should be reviewed.3,10 Consider requesting up-to-date investigations where appropriate, as this will guide perioperative care, including the need for critical care referral.
FES – Patients with DMD are at an increased risk of FES. 28 Symptoms are generally present within 72 h of a fracture or injury. These include tachypnea and air hunger; reduced pO2; petechiae; confusion, agitation or drowsiness (altered sensorium). However, signs may be subtle and a low suspicion threshold should be employed.
Treatment of FES centres around supportive care by maintaining oxygenation and early fluid resuscitation, including the use of mechanical ventilation with positive end-expiratory pressure. Management may include the requirement for mechanical ventilation, and in such cases, involve critical care early.
Anaesthesia-induced rhabdomyolysis (AIR) – is a complication risk in people with DMD undergoing general anaesthesia, particularly associated with suxamethonium and volatile compounds (see below). This can manifest during anaesthesia with hyperthermia and tachycardia and can progress rapidly to cardiac arrest. AIR is an anaesthetic emergency that requires prompt recognition, immediate withdrawal of the inciting agent and efficient assessment and management of metabolic disturbances, particularly hyperkalaemia.
Many centres advocate the empirical use of dantrolene in the management of AIR due to similarities in presentation to malignant hyperpyrexia, where it is the principal treatment. It should be available in all centres where general anaesthesia is taking place.33,34
Anaesthetic technique – Perioperative decision making should involve a senior anaesthetist with experience in managing DMD patients. Total intra-venous anaesthesia is the recommended anaesthetic technique as the use of succinylcholine and volatile anaesthetics is associated with a risk of severe hyperkalaemia and AIR.
The use of suxamethonium is contraindicated in DMD, as there is a risk of hyperkalaemic cardiac arrest.
Volatile agents should be avoided if possible, as there is a risk of AIR, and anaesthetic machines should be flushed prior to use. In exceptional circumstances, volatile anaesthetics can be used, but the duration should be kept to a minimum and the anaesthetist should be prepared to manage life-threatening sequelae.
Regional techniques, including spinal and epidural anaesthesia, can be considered, but caution is needed where cardiac dysfunction/cardiomyopathy is present due to the effects of sympathetic blockade.
Concluding remarks
This consensus guideline is important to ensure that safe, informed decisions are made by clinical teams, together with patients and families living with DMD in the event of long bone fractures or decisions about elective surgery for contractures.
Where available, published evidence has been used to support recommendations. Where this is not yet possible, expert experience and opinion of the multi-disciplinary working group (including patient representatives) provide helpful information on best practices. Endorsement from BSCOS offers further validity.
Implementation of these recommendations into clinical practice will harmonise and improve care for all people living with DMD, no matter in which centre they are seen. The next steps for these authors will include collaboration to collect data – for example on long bone fracture outcomes after casting versus internal fixation – and so increase the evidence base to inform and support future updates to these guidelines.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251348972 – Supplemental material for Development of a guideline for orthopaedic management in the care of children and young people with Duchenne muscular dystrophy in the UK National Health Service
Supplemental material, sj-pdf-1-cho-10.1177_18632521251348972 for Development of a guideline for orthopaedic management in the care of children and young people with Duchenne muscular dystrophy in the UK National Health Service by Philip D Henman, Catherine Turner, James Aird, William Guy Atherton, Donald Campbell, Clare Carpenter, Maria Belen Carsi, Melville Dixon, Nikolaos Giannakakis, Thomas Girdler-Hardy, Alison Hulme, Meredith James, Shuko Joseph, Nigel T Kiely, Kirsty Ohly, Anna Porter, Darius Rad, Emily Reuben, Roger Walton, Sze Choong Wong and Michela Guglieri in Journal of Children’s Orthopaedics
Footnotes
Appendix A: Paediatric hospitals with specialist neuromuscular centres in the NorthStar Network
Appendix B: List of hospitals with specialist children’s trauma care suitable for management of fractures in Duchenne muscular dystrophy patients
Aberdeen Royal Infirmary
Addenbrooke’s Hospital, Cambridge
Alder Hey Children’s Hospital, Liverpool
Birmingham Children’s Hospital
Bristol Children’s Hospital
University Hospitals, Plymouth
Dundee Ninewells Hospital
Evelina London Children’s Hospital
Great Ormond Street Hospital
John Radcliffe Hospital, Oxford
Leeds General Infirmary
Leicester Royal Infirmary
Manchester Children’s Hospital
Norfolk and Norwich Hospital
Queen’s Medical Centre, Nottingham
Royal Belfast Hospital for Sick Children
Royal Hospital for Children and Young People, Edinburgh
Royal Hospital for Children in Glasgow
Royal Stoke Hospital
Royal Sussex County Hospital
Royal Victoria Infirmary, Newcastle Upon Tyne
Sheffield Children’s Hospital
Southampton Children’s Hospital
University Hospital of Wales, Cardiff
Acknowledgements
Funding for DMD Care UK is received from Duchenne UK, Duchenne Research Fund and Joining Jack. The authors thank Mr. Daniel Reed, Evelina London Children’s Hospital and Mr. Athanasios Tsirikos, Royal Hospital for Children and Young People, Edinburgh, for additional input during the revision process.
Disclaimer
The guidance herein is expert opinion drawn from national multi-disciplinary experience and published research, but the working group acknowledges that there are no randomised controlled trials to support it.
Author contributions
PDH: lead author of guidelines. Incorporation of feedback and chairing of discussions to reach consensus. Liaison with BSCOS. CT: editing author and coordination of feedback during reviewing process. Corresponding author. JA, WGA, DC, CC, MBC, MD, NG, AH, SJ, NTK, DR, RW: guideline reviewer/contributor. TG-H: anaesthetics-expertise input. Guideline reviewer/contributor. AP: literature review to inform working group. Guideline reviewer/contributor. MJ: liaison with physiotherapy specialist group. Guideline reviewer/contributor. KO, ER: patient perspective contributor and review of the guideline. SCW: Liaison with bone and endocrine specialist group. Guideline reviewer/contributor. MG: Clinical lead and Principal Investigator of DMD Care UK. Guideline reviewer/contributor.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: CT is funded by Duchenne UK, Duchenne Research Fund and Joining Jack. This article presents independent research supported by the NIHR Newcastle Biomedical Research Centre (BRC; CT, MJ, MG) which is a partnership between Newcastle Hospitals NHS Foundation Trust and Newcastle University, funded by the National Institute for Health and Care Research (NIHR). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Ethical considerations
This article does not contain any studies with human or animal participants. There are no human participants in this article and informed consent is not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.