
Abstract
Purpose:
It was aimed to determine whether there is a statistically significant difference between various types of displaced supracondylar fractures of the humerus in children with movement impairment according to Flynn’s classification.
Methods:
Clinical results of 263 patients who were operated on with closed reduction and percutaneous pinning for displaced supracondylar fracture of the humerus were evaluated. Flynn’s classification was used to compare movement impairment.
Results:
One year after the procedure, only one patient in the category of extension fractures of type II displacement, and only in elbow flexion, had an unsatisfactory treatment outcome according to Flynn. All other patients achieved a satisfactory treatment outcome, with the vast majority, 252 patients (96%), in the excellent category. Four patients were in the good category, one patient in the fair category, and the aforementioned one patient in the poor category.
Conclusion:
In 1 year after the surgery, the limitation of elbow mobility is usually insignificant regardless of the grade of displacement or type of supracondylar fracture of the humerus.
Level of Evidence:
Level III—retrospective comparative study.
Keywords
Introduction
Supracondylar fractures of the distal humerus are one of the most common fractures in childhood. They account for ~3%–18% of all fractures in pediatric patients and about 50%–80% of fractures in the elbow region.1 –18 This fracture is most commonly encountered in children in the age range of 2–10 years.2,3,5,6,11 The mechanism of occurrence of this injury is most commonly a fall on an outstretched upper extremity or directly on the flexed elbow.3 –5,7 There are several classifications of this injury: (1) according to the type of fracture, most authors divide the fracture into extension and flexion; (2) according to the degree of displacement, the Gartland classification is used.3 –5,7,9,12,13 This second classification divides the fracture into three grades. The first grade indicates a non-displaced fracture. The second grade indicates a fracture with displacement, where the fragments are still in contact. The third grade classifies a fracture with significant displacement when the fragments are not in contact.2,19 X-ray examination is usually sufficient to diagnose and determine the type of fracture (Figure 1).1 –3,8,20
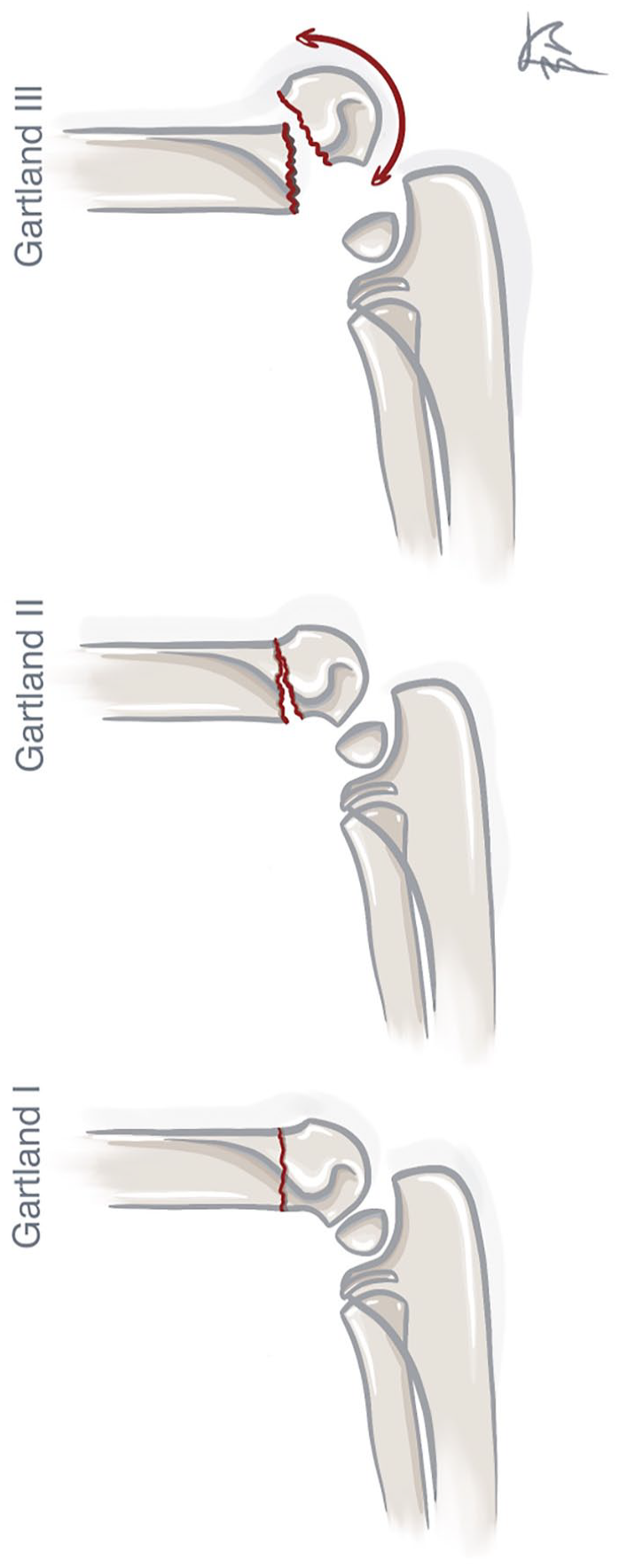
Gartland classification. Type of displacement according to Gartland.
The mainstay of therapy for non-displaced fractures is the immobilization of the fracture with plaster fixation, whereas closed reduction and transfixation with Kirschner wires (K-wires) is the method of choice for displaced fractures.1 –5,7 –11 This fracture is burdened with a relatively high incidence of complications, whether it is a neural or vascular lesion, limitation of mobility, bone deformity, growth disturbances, or compartment syndrome.1 –4,20
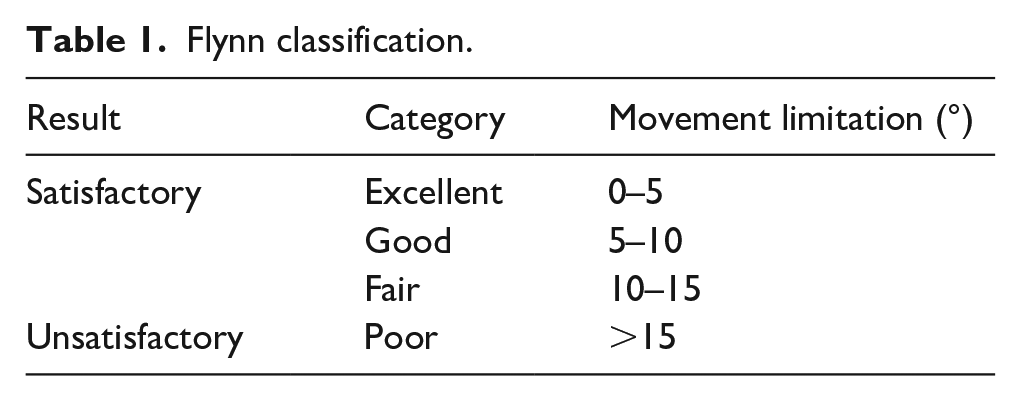
One of the criteria for evaluating the outcome of the treatment of a supracondylar fracture is the mobility in the elbow joint. This is most commonly defined by Flynn into four grades. 21 It can be assessed based on the limitation of mobility in flexion or extension, where we assess the worst of the parameters. The second parameter assessing the results of treatment and sequelae of the injury is the weight-bearing angle, which may differ from the other limb after healing. 12 The weight-bearing angle is the angle formed by the lines in the long axis of the humerus and ulna. Physiologically, there is a slight cubitus valgus.
This study aims to compare the severity of the complications of limitation of mobility depending on the type of fracture and the degree of displacement. We also aim to assess this limitation continuously up to 1 year after surgery and compare the results of the different fracture types and displacement with each other.
Methods
A single-center retrospective clinical study of patients with displaced supracondylar fracture of the humerus at the Department of Paediatric Surgery and Traumatology of the University Hospital between the years 2017 and 2021 was conducted.
The inclusion criteria for this study were:
a. displaced supracondylar fracture of the humerus according to the Gartland classification grades II–III.
b. standard surgical procedure, that is, closed reduction followed by crossed percutaneous pinning with Kirschner wires (K-wires) according to Swenson. 22
Patients for whom we did not have complete postoperative documentation were excluded from the study. In addition, patients with open fractures or pathological fractures, patients who required re-reduction, or patients who required open reduction or other non-standard osteosynthesis were excluded. The standard surgical procedure consisted of closed reduction under general anesthesia and crossed percutaneous pinning using 1.6–1.8 mm wide steel K-wires supplied by B Braun. Subsequently, the position of the fragments was checked by fluoroscopy. Anterior humeral line was evaluated, and the Baumann angle was compared with the other limb. The patient was then given a dorsal high plaster splint in the operating room. Follow-up was performed at an interval of 10–14 days after the procedure to check the K-wire entry points for infection without taking an X-ray. A follow-up X-ray was taken 3–4 weeks after the procedure, and according to the findings, K-wires were extracted in the outpatient clinic without the need for general anesthesia, and the plaster splint was removed. Three weeks of self-performed rehabilitation followed. After these 3 weeks, patients were prescribed physiotherapy unless they had good or excellent results in mobility according to Flynn. Control of elbow mobility was performed at intervals of 6 weeks, 3, 6, 9 months, and 1 year after surgery. Mobility in both flexion and extension was also monitored in respective time intervals. These values were then converted into categories according to the Flynn classification (Table 1).
Flynn classification.
The fractures were divided according to type into extension and other fracture groups. The other fracture group was every type of fracture, that is not the extension type. The values between types II and III displacement (according to Gartland classification for extension fractures) were compared. Also, the values between extension and other fracture types for type II displacement, and the values between extension and other fracture types for type III displacement were compared. Restriction of mobility was always compared separately in flexion and extension.
A line graph was created showing the evolution of the patient’s mobility limitation at each time interval. For this reason, each group of mobility limitation according to Flynn was assigned a score as follows: excellent—4 points, good—3 points, fair—2 points, poor—1 point. The number of individuals in a given Flynn group was then multiplied by the score for that group. The scores from all four groups were summed, and the resulting number was divided by the patient’s count. Thus, the result ranged from a value of 1 (all patients achieved the poor group result) to a value of 4 (all patients achieved the excellent group result during the period).
Statistical analysis
A demographic analysis of the data within each group (age, sex) was created. The group comparison was done between the groups as described above. The level of statistical significance was set at α = 0.05. Statistical processing was performed using GraphPad Prism software (GraphPad Software, San Diego, CA, USA). The chi-square test was primarily used. If the number of patients in any of the groups according to the Flynn classification was insufficient, Fisher’s exact test was used.
Results
In the observed period, a total of 319 patients had surgery for the diagnosis of displaced supracondylar fracture of the humerus. Inclusion criteria were met in 263 patients. The age range of patients was 1–14 years. A total of 85% of patients were in the age category of 3–9 years. The mean age was 6.4 years. The median age was 6 years. Male sex accounted for 55% of the patients and female sex for 45%.
The majority of the patients had surgery for the extension type of fracture with type II displacement—148 patients (56%). Furthermore, 78 patients (30%) had type III displaced extension type of fracture, 29 patients (11%) were included in the group of other fractures with type II displacement, and the least number of patients were in the group of other fractures with type III displacement, that is, eight patients (3%).
After 3 weeks of self-performed rehabilitation, 139 (53%) of patients had satisfactory results of mobility according to Flynn. Physiotherapy was prescribed to 124 (47%) patients. Out of these patients, 63 (51%) had extension-type grade II fracture, 42 (34%) patients had extension-type grade III fracture, 14 (11%) patients had another type grade II fracture, and 5 (4%) patients had another type grade III fracture.
A statistically significant difference was found comparing patients with extension-type fractures with grade II displacement to the other fractures with grade II displacement group at 3 months after elbow flexion injury. Furthermore, patients with extension-type fractures with grade II displacement and extension-type fractures with grade III displacement at 6 months after injury in extension. Then, in patients with extension-type fracture with grade II displacement and the group of other fractures with grade II displacement from baseline to 3 months after the injury in extension (Tables 2 and 3).
Statistical analysis - movement impairment in flexion.
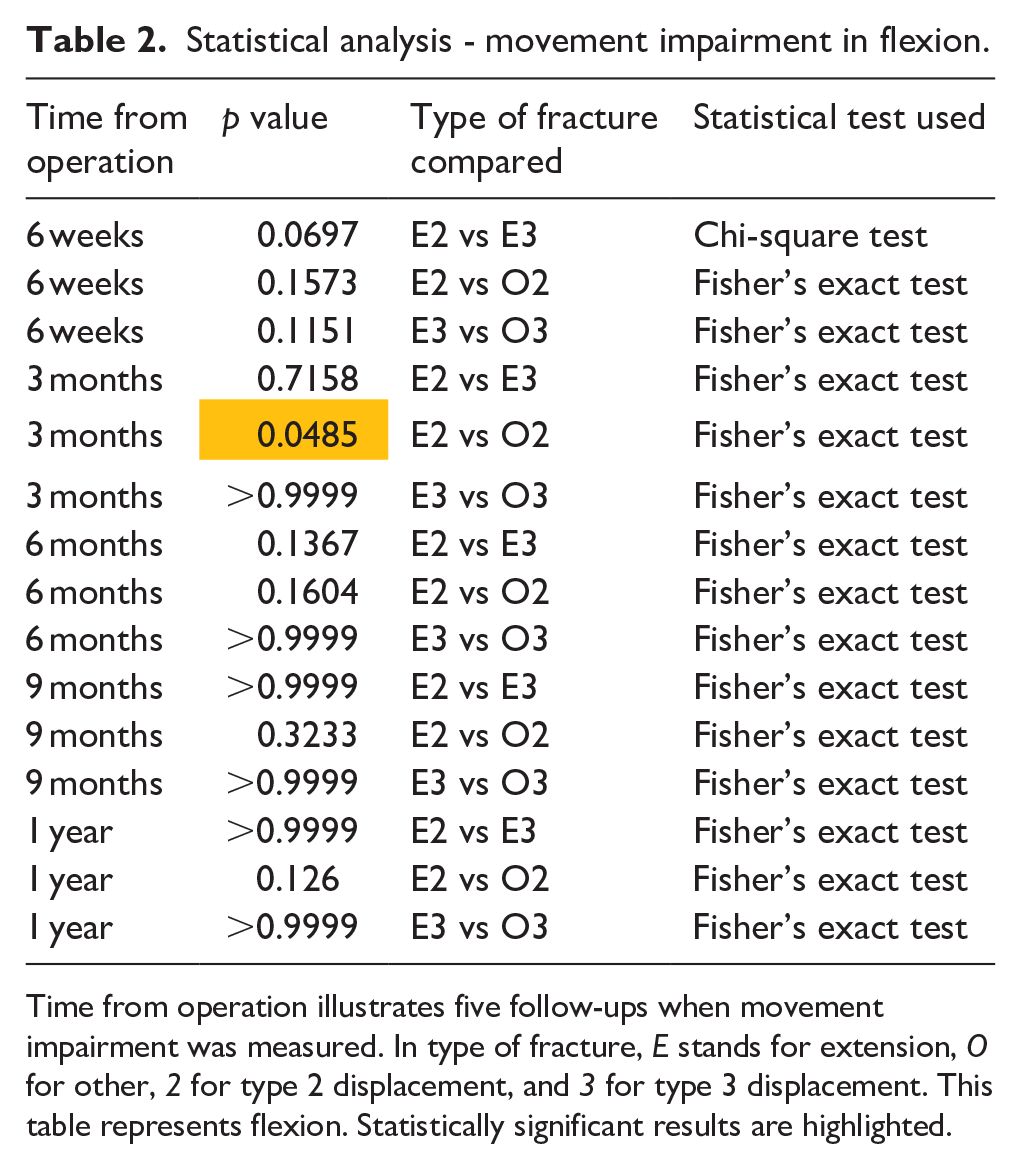
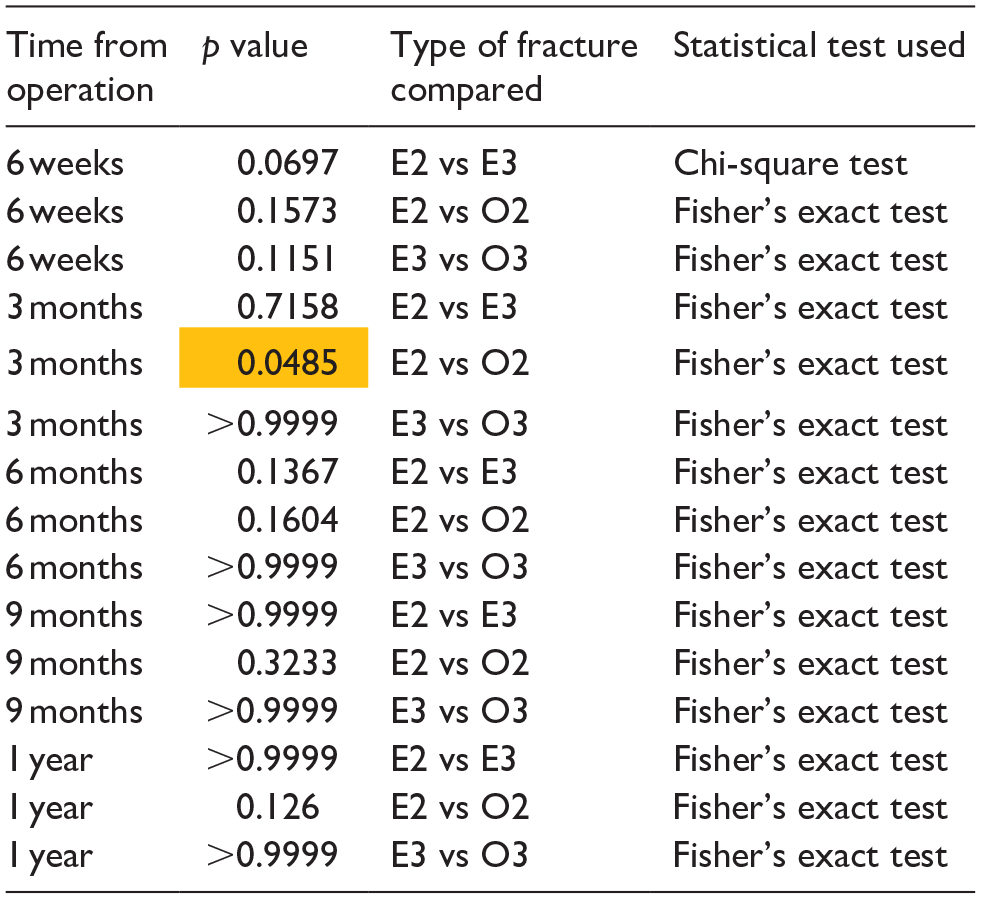
Time from operation illustrates five follow-ups when movement impairment was measured. In type of fracture, E stands for extension, O for other, 2 for type 2 displacement, and 3 for type 3 displacement. This table represents flexion. Statistically significant results are highlighted.
Statistical analysis - movement impairment in extension.
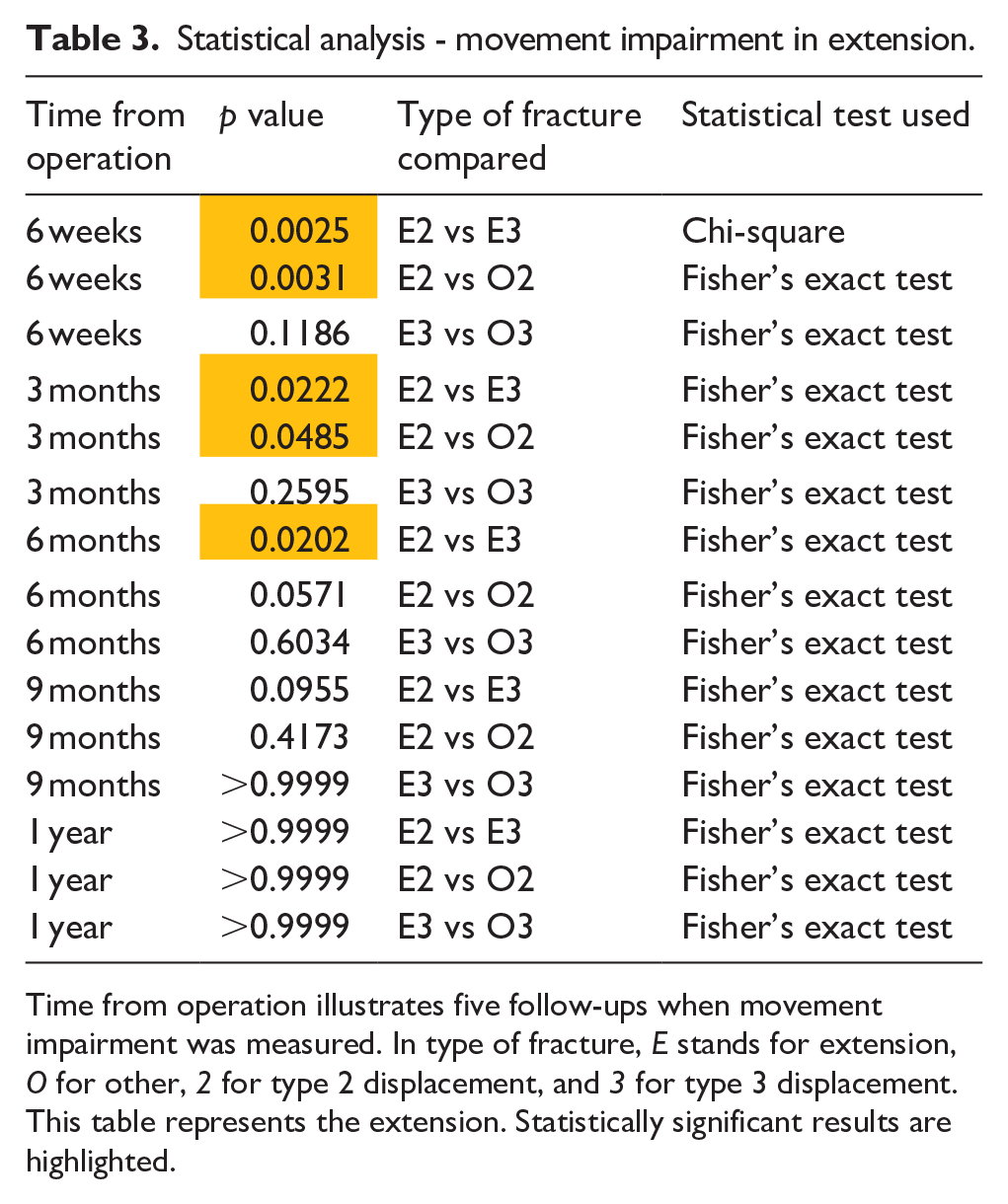
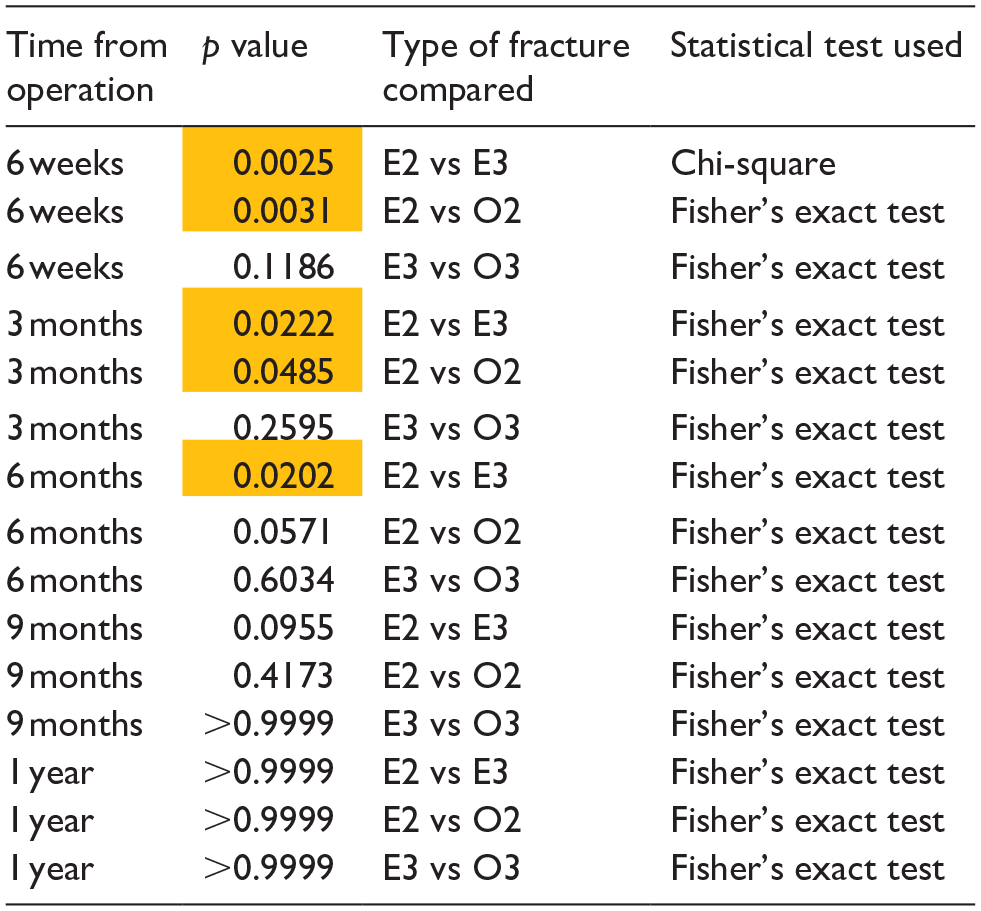
Time from operation illustrates five follow-ups when movement impairment was measured. In type of fracture, E stands for extension, O for other, 2 for type 2 displacement, and 3 for type 3 displacement. This table represents the extension. Statistically significant results are highlighted.
One year after the procedure, only one patient in the category of extension fractures of type II displacement, and only in elbow flexion, had an unsatisfactory treatment outcome. All other patients achieved a satisfactory treatment outcome, with the vast majority in the excellent category 252 patients (96%), four patients in the good category, one patient in the fair category, and the aforementioned one patient in the poor category (Figures 2 and 3).
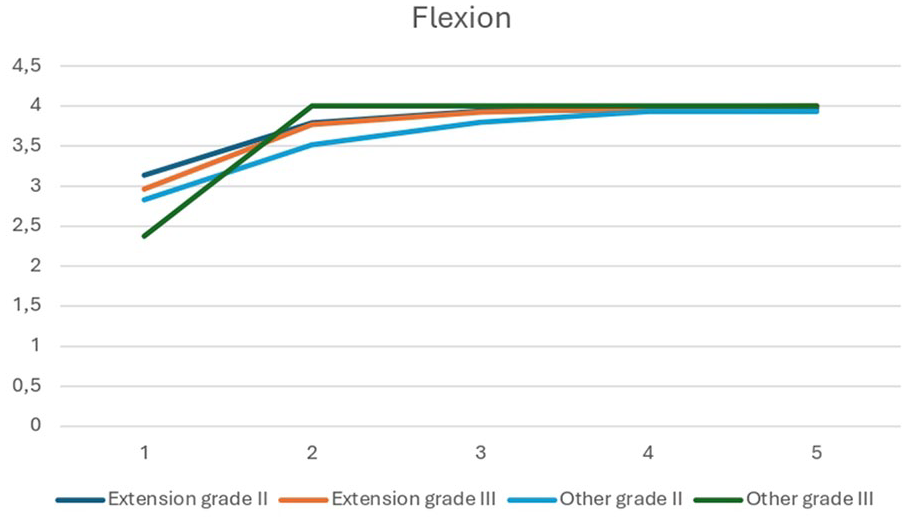
The value shown on the y-axis of the graph represents the value determining the relevance of movement impairment, calculated as mentioned above in the methods. The x-axis of the graph is then represented by the timeline axis, where the five intervals correspond to the five controls over time as defined above. The graph shows four lines, each corresponding to a single treatment group: extension fracture with grade II displacement, extension fracture with grade III displacement, other fractures with grade II displacement, and other fractures with grade III displacement.
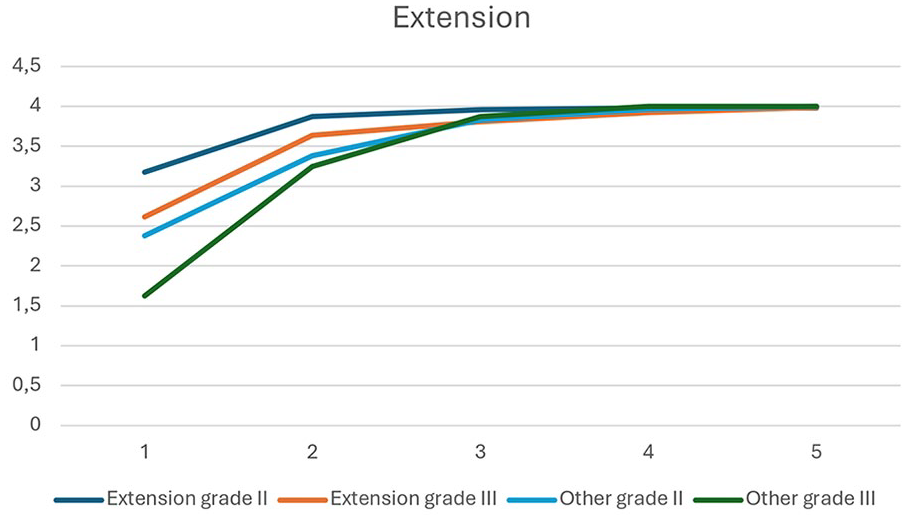
The value shown on the y-axis of the graph represents the value determining the relevance of movement impairment, calculated as mentioned above in the methods. The x-axis of the graph is then represented by the timeline axis, where the five intervals correspond to the five controls over time as defined above. The graph shows four lines, each corresponding to a single treatment group: extension fracture with grade II displacement, extension fracture with grade III displacement, other fractures with grade II displacement, and other fractures with grade III displacement.
Discussion
This study aimed to evaluate the severity of elbow mobility limitation in pediatric patients with a displaced supracondylar humerus fracture requiring surgical treatment. This complication was evaluated over time for 1 year after surgery at five time intervals. Groups with different types of fractures with different displacements were compared with each other. Supracondylar humerus fractures are one of the most common fractures in childhood.1 –13 Patients in the age range of 2–10 years are most commonly affected by this injury, which is consistent with our study, where most patients were in the age range of 3–9 years.2,3,5,6,11,20
At the first follow-up, where mobility limitation was monitored, 6 weeks after surgery, mobility limitation was highly variable. Some patients at this follow-up had no or minimal mobility limitation, belonging to the excellent category. In contrast, in some patients, mobility limitation was measured in tens of degrees. In general, patients with greater displacement, that is, Gartland grade III, had greater mobility limitation within a given fracture type at the first follow-up. Greater limitation compared to the other side was usually measured in extension. However, with time, this trend essentially disappeared, and at the fourth follow-up, 9 months after the injury, the difference was negligible. At the last follow-up 1 year after the surgery, all but one patient had a satisfactory treatment outcome according to Flynn, with 96% of patients having an excellent treatment outcome.
Statistical analysis of the data indicates a statistically significant difference in mobility when comparing patients with an extension-type fracture with grade II displacement to the group of other fractures with grade II displacement at 3 months after flexion injury. In addition, patients with extension-type fractures with grade II displacement and extension-type fractures with grade III displacement from the start of follow-up to and including follow-up at 6 months in extension. Furthermore, in patients with an extension-type fracture with grade II displacement and another fracture group with grade II displacement from baseline to 3 months after injury in extension. However, this does not support the idea that a certain type of fracture or displacement is associated with a greater limitation of mobility in the elbow in the long term.
Patient’s age at the first follow-up 6 weeks after the surgery, also had an effect on elbow mobility. Patients who were 9 years old or younger had an unsatisfactory Flynn mobility result in 70 cases (30%). Patients in the age group of 10–14 years had an unsatisfactory result in 15 cases (50%). However, this difference was already insignificant at the second follow-up 3 months after the surgery, when 20 patients (9%) in the age group 9 years and younger and three patients (10%) in the age group 10–14 years had an unsatisfactory result. Thus, it can be said that age played a role only in the initial stages of rehabilitation and had no long-term effect on the outcome of treatment.
One of the main components of postoperative care is rehabilitation. In our experience, if there is a fair or worse outcome of the elbow mobility according to Flynn after 3 weeks of self-conducted rehabilitation, professional physiotherapy is indicated. This procedure has certainly contributed to the excellent elbow mobility results that our patients achieve.
The statistically significant results in our cohort are rather random in nature and do not show any trend that clearly identifies the grade of displacement or type of fracture as being riskier than others. Thus, it can be said that with properly performed surgery and appropriately managed postoperative care, similar outcomes can be expected for both less and grossly displaced fractures across the different supracondylar fracture types.
Muslu et al. had very similar results to those in our study. All patients had satisfactory results of treatment. Most patients (92%) had excellent results, 7% of patients had good results and only 1% had fair results of movement in the elbow according to Flynn. 23
Mehlman et al. also had great results when 97% had satisfactory results and only 3% had unsatisfactory results, which is a slightly higher percentage than in our study. This can also be caused by that Mehlman et al. included also bearing angle of the extremity in Flynn’s classification. 24 Overall, it can be said that we achieved similar results as other studies on this topic.
The limitation of this study is that it is a retrospective study. Some factors that could affect the result of the treatment are not considered. For example, the timing of the surgery. In our department, third-degree displaced fractures are indicated for immediate surgery, that is, within 6 h from the time of injury. We also try to treat second-degree displacement fractures in this manner; however, it is not uncommon for a patient to be operated on in more than 6 h. This could be prevented by creating a prospective study. Another limitation is the evaluation of only the limitation of mobility in the elbow. However, the weight-bearing angle of the limb, which is part of the Flynn classification, was not considered. This is due to the absence of these values in the patient’s records. On the other hand, the strength of this study is the relatively large number of patients included in the study. All patients were operated on by an experienced pediatric trauma surgeon at our institution (at least 6 years of experience in pediatric trauma in a university hospital), which excludes potential complications due to the inexperienced surgeon.
Most of the studies published on this topic are retrospective studies. Although a prospective study would be more valuable, according to our results, there is no need for a prospective study. The surgery technique used in our department seems to be suitable for the treatment of this type of trauma. However, it is necessary, that an experienced surgeon operates to ensure satisfactory results.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251341140 – Supplemental material for Severity of elbow mobility limitation in pediatric patients with a displaced supracondylar humerus fracture requiring surgical treatment: A monocentric retrospective clinical study
Supplemental material, sj-pdf-1-cho-10.1177_18632521251341140 for Severity of elbow mobility limitation in pediatric patients with a displaced supracondylar humerus fracture requiring surgical treatment: A monocentric retrospective clinical study by Tomáš Merkl, David Astapenko, Radek Štichhauer, Pavel Navrátil, Antonín Šafus, Zuzana Burešová and Petr Lochman in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Tomáš Merkl—designed the methods, performed the literature search, collected the data, analyzed the data, and wrote the article; David Astapenko—analyzed the data, wrote, and edited the article; Radek Štichhauer—analyzed the data and edited the article; Antonín Šafus—collected the data; Pavel Navrátil—collected the data; Petr Lochman—analyzed the data and edited the article, Zuzana Burešová—created the picture number 1.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by Ministry of Education, Youth and Sports of the Czech Republic, Grant/Award, Number: SV/FVZ202305, The work was supported by the Ministry of Defence of the Czech Republic, DRO of the University of Defence, Faculty of Military Health Sciences Hradec Kralove, Czech Republic, Clinical Disciplines II (DZRO-FVZ22-KLINIKA II).
Ethical considerations
Ethical statement is not applicable because of retrospective study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.