
Abstract
Aim of the Study:
Aim is to define whether the type of anesthesia during the reduction and fixation of a pediatric forearm fracture, can influence the fracture reduction technique.
Materials and Methods:
All surgically treated forearm fractures were enrolled: patients underwent a different anesthesiology protocol depending on the on-call anesthesiologist: deep sedation in which the patient is still able to breathe with limited external support and nerve block (group A) and general anesthesia with curare (group B). Demographic data, type of fracture, surgical timing and technique, anesthesia type and timing, and clinical outcomes were recorded.
Outcomes:
Of the total 326 patients considered, 228 children were treated by closed reduction (70%), and 98 children were treated by open reduction (30%). Of the latter, 75% of the fractures reduced open were of group A and 25% were of group B. In more detail, in group A, of the 162 patients, 73 (45%) required an open reduction, while 89 (55%) did not. In group B, of the 164 patients, 25 (15%) required an open reduction, while 139 (85%) did not. This resulted in being statistically significant (p = 0.001). No statistically significant results emerged from the data related to complication and range of motion apart from the pronation movement (p = 0.153).
Conclusion:
According to our data, the use of curare, in a pediatric forearm fracture reduction and stabilization surgery, leads to a reduction in the number of open treatments. If deep sedation and nerve block are preferred to improve postoperative pain control, the technique and timing should be improved to facilitate reduction.
Keywords
Introduction
Forearm fractures 1 constitute the most common type of fracture in the pediatric population, accounting for 17.8% according to Naranje et al. 2 Joeris et al. 3 found that this type of fracture is typical of school-age and adolescent children; in 50.1% 4 of cases, the fracture involves both the radius and ulna and males are significantly more affected than females (63.3% versus 36.4%).
Forearm both bone fractures, 5 typical of children under 16 years of age, account for 5.4% of all pediatric fractures.
The gold standard1,6,7 for the treatment of forearm fractures, according to the available literature, is conservative treatment by cast immobilization due to the excellent remodeling 6 ability observed in the pediatric age group. Although this treatment is preferred to avoid surgical complications,6 –8 several studies have shown an increase in the number of forearm fractures surgically treated.
This phenomenon is mainly caused by the failure of the conservative method 8 because of the latter’s increased risk of causing secondary fracture displacement and reduced mobility of the elbow and wrist. In addition, unstable and irreducible fractures, exposed fractures, and fractures with neuro-vascular deficits must be treated surgically.1,7
The purpose of this study is to define whether deep sedation in which the patient is still able to breathe with limited external support and nerve block (group A) and general anesthesia with curare (group B), in a pediatric forearm fracture reduction and fixation, can influence the fracture reduction technique.
The proposed study is innovative because there are no studies in the literature analyzing the relationship between the use of paralyzing drugs, administered during anesthesia, and the reduction technique (closed or open) of pediatric forearm fractures.
The only existing studies concerning anesthesia and pediatric forearm fractures are related to the comparison of infraclavicular locoregional anesthesia 9 and conscious sedation, used during the procedure of closed fracture reduction in the emergency department before the cast, or the use of Bier’s block (intravenous block). 10
Material and methods
The study recruited a cohort of patients with metaphyseal and diaphyseal forearm fractures of both sexes, aged between 2 and 14 years, from the computerized database of a level 2 pediatric university center over a period of 3 years.
We excluded patients older than 14 years of age, patients who suffered other types of fracture apart forearm fractures (i.e., Monteggia fractures, greenwood fractures, Galezzi fractures, radial capitellum fractures, olecranon fractures, and Goyrand-Smith fractures), patients with fractures treated with plate and screws or external fixators and patients in whom the clinical and/or radiological iconographic documentation was incomplete.
Through the analyses of medical records and computer databases, the following patient data were collected: gender, age, weight, days between the date of fracture and the date of admission, days between the date of admission and the date of surgery, and whether a recent fracture was found in the same anatomical segment. In addition, the type of fracture was classified, and the surgical indication was given according to Noonan and Price’s 1998 recommendations, 11 so we excluded simple fracture with a satisfying reduction and stabilization with the cast.
Preoperative, immediate postoperative, and last follow-up radiographs were collected.
Using an online program (Online Protractor Angle Measuring Tool), the degree of displacement of the fractures for each bone in both anteroposterior and lateral views was measured on the preoperative radiograph and on the last available radiograph taken during follow-up.
The surgical reports were analyzed to collect data on the method of fracture reduction, the type of fixation device used, and the surgical and anesthesiologic time.
Regarding anesthesiologic-specific data, the two groups underwent different protocols according to the on-call anesthesiologist. Group A underwent a deep sedation protocol while maintaining airway control via face mask or laryngeal mask plus locoregional axillary or supraclavicular anesthesia with ropivacaine or Levobupivacaine. No children in group A were curarized.
Group B, on the other hand, was subjected to general anesthesia while maintaining control of the airway via an endotracheal tube. No children in this group underwent locoregional anesthesia. All children in group B were curarized.
The surgeon and anesthesiologist were the ones on call, all the surgeons have minimum 4 years of experience in pediatrics orthopedics. The anesthesiologists have minimum 5 years of experience in pediatric anesthesiology. The type of anesthesia was always decided by the on-call anesthesiologist without being influenced by the type of fractures or by the surgeon.
Data on the follow-up period result from the reports of follow-up visits at the outpatient clinic.
The first follow-up was around 35 days after the discharge, and the second follow-up was approximately 60–80 days after discharge.
Subsequent follow-ups are scheduled based on the clinical and radiological healing of the fracture.
Regarding range of motion, flexion-extension of the elbow and prono-supination movements were chosen to be included in the database but confrontation was made only at the last follow-up, because the children were considered healed if both clinically and radiographically were clear and patients were able to resume normal daily life, including sports activities.
Complications such as peripheral vascular and nervous deficits, infections, presence of hypertrophic and keloid scars, pseudoarthrosis or delayed consolidation of the bones, and presence of bone deformity or stiffness, were collected.
The Excel® program (Microsoft) was used for data collection and database creation; all analyses were performed using Stata version 12 (Stata Corporation, College Station, TX).
Descriptive analysis was done using, in the case of a single variable, the mean, standard error, and 95% confidence interval (95% CI). Absolute frequency, percentage frequency, and cumulative percentage frequency were used in the case of dual variables.
To analyze any existing differences between two percentages and demonstrate the significance of the data, the chi-square test was used. To analyze any existing differences between the means of different variables and demonstrate the significance of the data, the Student’s t-test was used. A significance level of 5% (0.05) was adopted.
Results
A total of 730 patients have access to the Emergency Department with a forearm fracture.
A total of 417 children with forearm fractures that could not be reduced with an acceptable result in the plaster room with the support of nitrous oxide were included in the study. Among them, 215 belonged to group A and 202 belonged to group B.
Based on the exclusion criteria, it was decided to exclude 18 patients from group A and 10 patients from group B for ages older than 14 years.
Furthermore, for group A, 35 patients were excluded: 8 patients suffered from a Monteggia-type fracture, 15 patients from an isolated radial capitellum fracture, 2 from radial capitellum and olecranon fractures, 4 patients from an isolated olecranon fracture, 2 patients from a Goyrand-Smith fracture, 3 patients from other types of fracture (1 coronoid fracture, 1 monostotic ulna fracture, and 1 radial neck fracture). One patient was excluded because his forearm fracture was treated with plates.
For group B, 28 patients were excluded: 9 patients suffered from Monteggia-type fracture, 11 patients from an isolated radial capitellum fracture, 5 patients from an isolated olecranon fracture, and 2 patients from a Goyrand-Smith fracture. One patient was excluded because his forearm fracture was treated with plates.
Therefore, the patient cohort examined consists of 326 total cases, of which 162 children were treated by deep sedation and locoregional anesthesia (group A, 49.69%) and 164 children were treated with general anesthesia combined with curare (group B, 50.31%).
Seventeen patients in group A and 20 patients in group A experienced a previous forearm fracture treated with a cast at minimum 6 months before the new fracture. The observation that it was a refracture did not affect the type of indication, based only on the impossibility of obtaining an acceptable reduction in the plaster room. Baseline and preoperative data are shown in Table 1. The mean weight was 27.27 kg (Std.Err. = 1.1088; 95% CI 25.094–29.456). In Table 2 we present patients in three groups of ages (2–5, 6–10, 11–14 years) and according to the type of anesthesiology protocol and reduction (open/close). In Table 3 preoperative fracture displacements are shown while in Table 4 bone angulations at the last follow-up are shown.
Baseline and preoperative data.
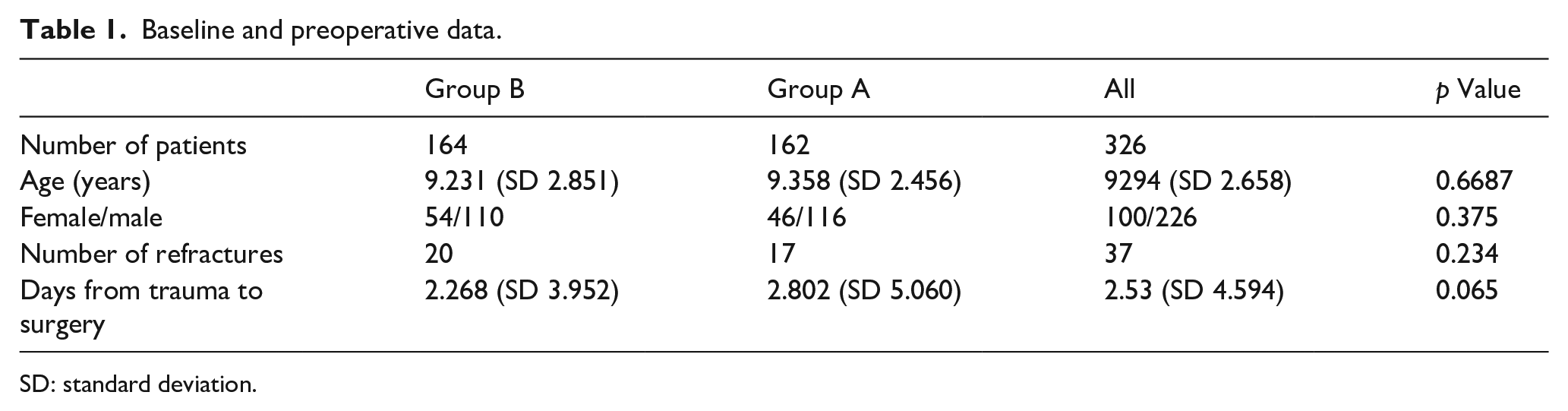
SD: standard deviation.
Details of ages and subdivision according to the type of anesthesiology protocol and reduction (open/close).
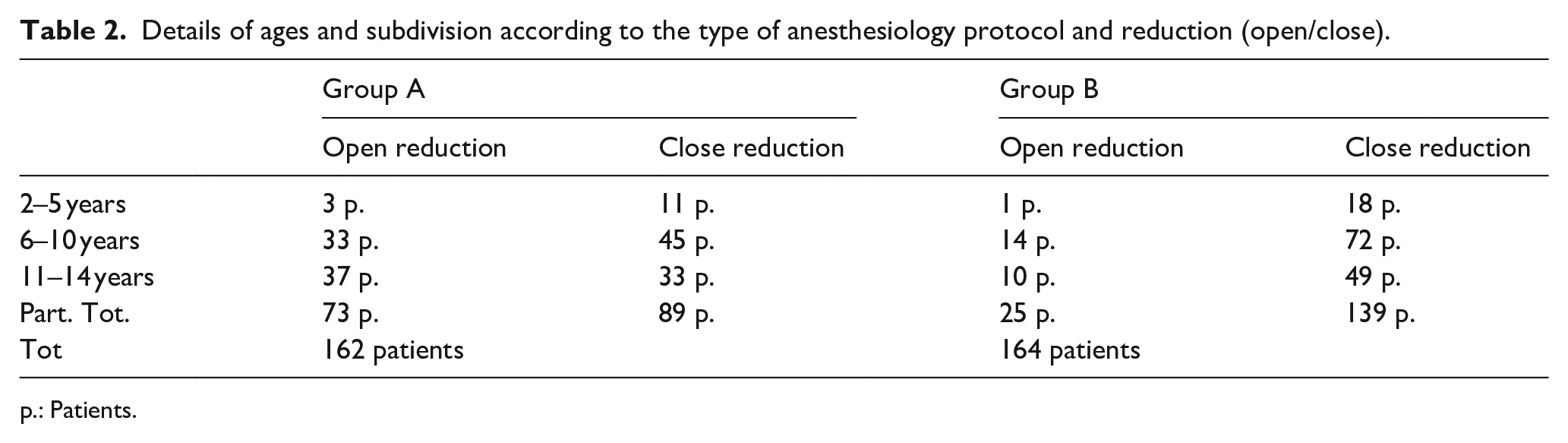
p.: Patients.
Preoperative fracture displacements are shown (in degrees).
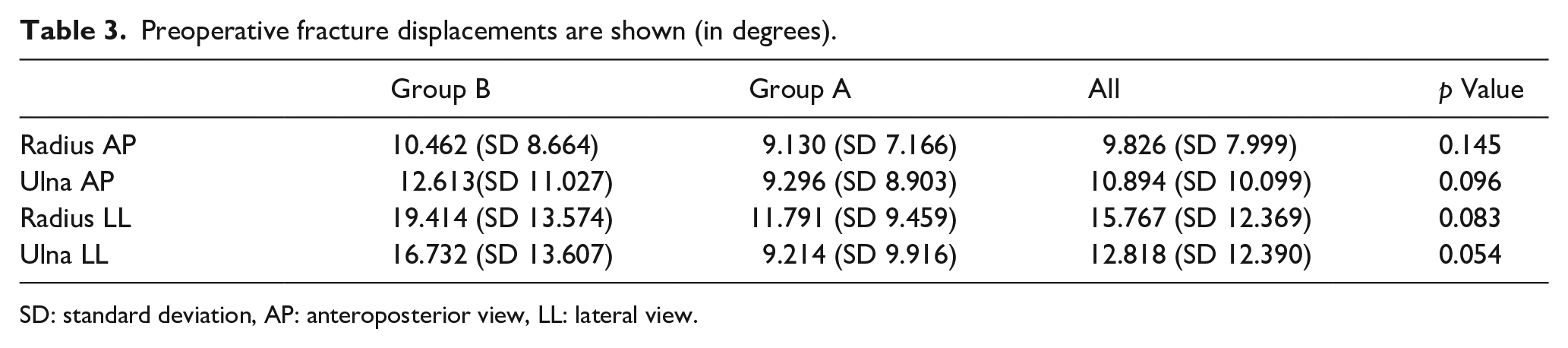
SD: standard deviation, AP: anteroposterior view, LL: lateral view.
Bone angulations at the last follow-up are shown (in degrees).
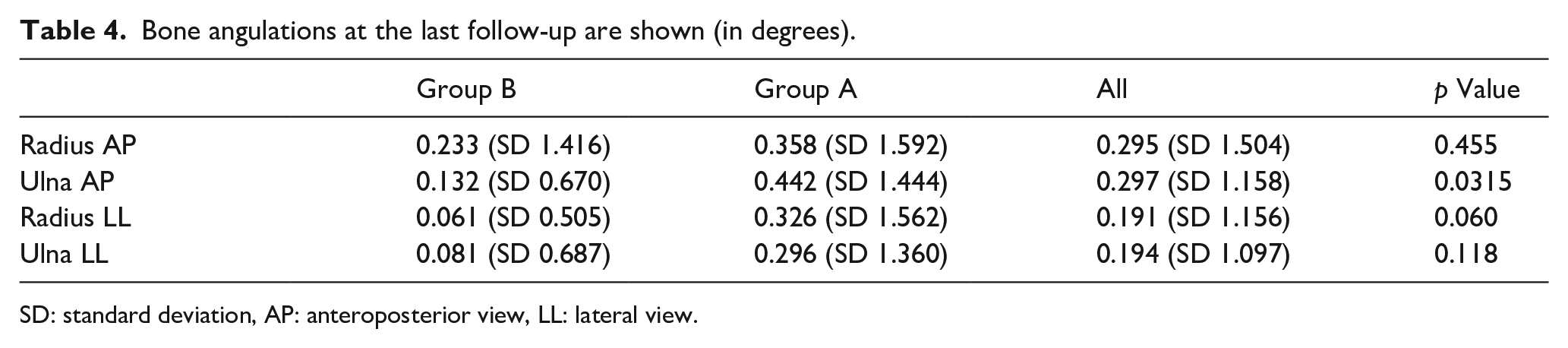
SD: standard deviation, AP: anteroposterior view, LL: lateral view.
Of the total 326 patients considered, 228 children were treated by closed reduction (70%), and 98 children were treated by open reduction (30%). Of the latter, 75% of the fractures reduced open were of group A and 25% were of group B.
In more detail, in group A, of the 162 patients, 73 (45%) required an open reduction, while 89 (55%) did not. In group B, of the 164 patients, 25 (15%) required an open reduction, while 139 (85%) did not. The chi-square test for the reduction method (χ2 = 34.4641) showed a statistically significant difference between the two groups (p = 0.000 < 0.05). Of the total number of children considered, 275 children were treated with Kirschner wires (84.3%), and 47 children were treated with elastic nails (15.63%), in 4 cases no-fixation devices were used. In group A 122 (75%) children were treated with Kirschner wires and 40 (25%) children were treated with elastic nails. In group B 153 (93%) children were treated with Kirschner wires, 7 (7%) children with elastic nails, and 4 children were treated without fixation devices.
The anesthesiology time was 20.03 min for group A and 13.37 min for group B. Student’s t-test revealed a statistically significant difference between the two groups.
The surgical time, that is, the time from the beginning to the end of the surgery, was recorded as 49.16 min for group A (Std.Err. = 2.158, standard deviation (SD) = 27.4745 95% CI 44.897–53.423) and 42.3 for group B (Std.Err. = 1.828, SD = 23.418 95% CI 38.73–45.95). Student’s t-test (T-test = −2.4127) revealed a statistically significant difference between the two groups (p = 0.0082 < 0.05).
All 326 patients, after surgery, wore a cast for 35 days for immobilization of the limb and were discharged the day after the surgery. The average follow-up was 76.01 days, specifically 75.48 for group A and 76.54 for group B.
Out of the total 326 patients examined, 11 children (3.4%) reported complications at the first follow-up: in group A 1 case of minor radial nerve palsy, in group B 1 case of minor ulnar nerve palsy. The other nine patients (seven in group A and two in group B) showed mild edematous fingers with a limited range of motion in extension. The chi-square test (χ2 = 2.2891) showed no statistically significant difference between the two groups (p = 0.130 > 0.05). At the last follow-up, the palsies were solved.
At the last follow-up, two children (0.62%) reported elbow flexion impairment of 15°, no children reported elbow extension impairment, five children (1.56%) reported pronation impairment (between 10° and 20°), and two children (0.62%) reported supination impairment (15°). The distribution in the two groups and the comparison between their functional limitations are shown in Table 5.
Functional limitations distribution and the comparison between the two groups for are shown (in degrees).

Discussion
The purpose of the study is to determine if the type of paralytic drugs in a fracture reduction and stabilization surgery, influence the technique of fracture reduction. The data collected showed that children who underwent general anesthesia with curare administration had less chance to be treated by open reduction (15% versus 45%, p = 0.001).
A recent review by Poutoglidou et al., 7 stated based on other studies12,13 that the open reduction rate of fractures during intramedullary fixation is between 9% and 33%. The authors claim that failure of multiple closed reductions, associated with longer-than-expected operative times, can cause the onset of compartment syndrome. Furthermore, open reduction results in disruption of blood circulation around the fracture and therefore may cause problems like malconsolidation 14 or pseudoarthrosis. 7 Of the total 326 patients considered, 228 children were treated by closed reduction (70%), and 98 children were treated by open reduction (30%). Of the latter, 75% of the fractures reduced open were of group A and 25% were of group B. In more detail, in group A, of the 162 patients, 73 (45%) required an open reduction, while 89 (55%) did not. In group B, of the 164 patients, 25 (15%) required an open reduction, while 139 (85%) did not.
Comparing the data collected with the literature, it appears that in group A there is a higher rate of open reduction than the percentages given (45% versus 9%–33%), while in group B the data collected are in line with the percentages given in the literature (15% versus 9%–33%).
The average surgical time (46 min), defined as the time between surgical incision and wound suturing, is in line with most of the data in the literature. The average surgical time, taken for intramedullary fixation, is 50.28 ± 4.82 min according to Zeybek and Akti, 5 48 ± 13 min according to Yaradılmış and Tecirli, 15 and 54 ± 7 min according to Zheng et al. 16 In our case series, the surgical time was recorded as 49.16 min for group A (Std.Err. = 2.158, SD = 27.4745 95% CI 44.897–53.423) and 42.3 for group B (Std.Err. = 1.828, SD = 23.418 95% CI 38.73–45.95). Student’s t-test (T-test = −2.4127) revealed a statistically significant difference between the two groups (p = 0.0082 < 0.05). The average surgical time in group A is longer than in group B, we think this is due to the greater number of open reductions.
In literature, the average final range of motion of pronation and supination is 82.03° ± 12.36°(P) and 83.72° ± 14.95°(S) according to Mahecha-Toroa, 13 on the other hand, according to Yaradılmış 14 it is 85.1° ± 6.6°(P) and 82.3° ± 7.8°(S). In 2016, Lu et al. 17 published a study showing that normal forearm rotation was recorded in 80% of patients undergoing intramedullary nailing. In 2017, Kruppa et al. 18 published an observational study in which they found that out of 202 children undergoing intramedullary nailing, 2 children (1%) experienced limited range of motion. Our data are in line with those papers although we found that in group A, no pronation deficit was found, whereas in group B, 5 children (3.14%) were found to have a slight pronation deficit but we are not able to correlate this finding with the type of anesthesia.
Along with clinical outcomes related to movement, complications amounting to 3.43% were also evaluated during the follow-up period, taking both groups into consideration. This percentage is significantly lower than the data that can be found in the latest studies published in the literature but this figure could be related to the complexity of the definition of complication. The complication rate is namely 27% according to Fujihara et al., 19 29% according to Freese et al. 20 and 9% according to Kruppa et al. 18 Notably, only 2 out of 326 patients experienced peripheral vasculo-nervous deficits or 0.62%, which is lower than the 2.5% indicated by the study of Fujihara et al. 19 and the 10% indicated by the study of Freese et al. 20
In addition, no patients experienced infections, as opposed to what is claimed in Fujihara’s study (5%) and Freese’s study (2.5%).
The data collected are again in line with those indicated in the review by Poutoglidou et al., 7 in which it is stated, based on Price’s criteria, 11 that reduction is defined acceptable when the fracture has less than 10° of angulation and 45° of malrotation.
The main limitations of our study are related to retrospective nature and the un-randomized allocation to a group. Nevertheless, this study may have laid a good foundation for conducting further prospective, randomized, double-blind studies through which an effective relationship between the use of paralytic drugs and the type of reduction could be identified.
Conclusion
According to our data, the use of curare, in a pediatric forearm fracture reduction and stabilization surgery, leads to a reduction in the number of open treatments. Anesthesiology techniques should be optimized in patients with forearm fractures to reduce the number of open treatments as much as possible. If deep sedation and nerve block are preferred to improve postoperative pain control, the technique and timing should be improved to facilitate reduction.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251325066 – Supplemental material for General anesthesia versus locoregional anesthesia in pediatric forearm fractures
Supplemental material, sj-pdf-1-cho-10.1177_18632521251325066 for General anesthesia versus locoregional anesthesia in pediatric forearm fractures by Alessandro Aprato, Alessia Fierro, Chiara Arrigoni, Mattia Cravino, Nathalie Bini and Carlo Origo in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Aprato A study conception and design, bibliography analysis, manuscript writing and revision, supervision. Fierro A and Arrigoni C collected and analyzed the data; Cravino M, Bini N, and Origo C were involved in manuscript conception, writing the manuscript, and contribute with important scientific knowledge giving the final approval.
Data availability
All data have been store in the dedicated repository of University of Turin and are available on request to the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This retrospective study received a waiver from the local committee (Comitato etico Citt. della Salute e della Scienza di Torino 2018/20121), trial number 287.718 (14/04/2020).
Consent to participate
Each patient gave written consent to participate.
Consent to publish
Each patient gave written consent to publish the results.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.