
Abstract
Purpose:
Congenital radioulnar synostosis is a congenital disorder affecting the elbow. We aimed to investigate the baseline characteristics and the clinical and functional outcome of a cohort of children with congenital radioulnar synostosis undergoing operative and non-operative treatment.
Methods:
This multicenter retrospective study evaluated children with congenital radioulnar synostosis admitted to three European pediatric orthopedic centers from January 1998 to April 2021. Baseline characteristics were extracted from medical records. Operative cases treated with rotational osteotomy were further analyzed. Outcomes were assessed using the Mayo Elbow Performance Score and the Quick-DASH questionnaire.
Results:
Ninety-seven patients (122 forearms) were included. Forearm positions were predominantly neutral or excessively pronated. Type 3 Congenital radioulnar synostosis was the most common radiographic finding. A total of 52 patients (66 forearms) underwent proximal derotational osteotomy, achieving a neutral forearm position in 61.9% of cases. Six complications were reported. The mean follow-up was 4.5 ± 3.4 years. MEPS averaged 90.6 points and Quick-DASH 18.5 points. No significant differences were found between operated and non-operated cases. MEPS results were good or excellent in 77.9% of patients, while only 31% reported a Quick-DASH ≤ 7points.
Conclusion:
We present the largest case series of pediatric congenital radioulnar synostosis to date. Mild deformities caused minimal disability and required no surgery. For severe malrotation, proximal derotational osteotomy was safe, with low complication rates, restoring a neutral forearm position and yielding outcomes comparable to non-surgical management of mild cases.
Introduction
Congenital radioulnar synostosis (CRUS) is a rare congenital disorder affecting the elbow and forearm, characterized by a fibrous or bony bridge between the proximal ends of the radius and ulna. 1 The prevalence ranges from 1/5000 to 1/1,000,000 live births, being more frequent in the Chinese population.2,3 The affected forearm is placed in a fixed position, usually in a range varying from neutral to severe pronation.1,4,5 According to the Cleary and Omer classification, the deformity is classified into four categories, based on the kind of synostosis, the location, and the characteristics of the radial head. 6 Frequently, CRUS is noticed by parents around the age of 3 to 4 years, depending on the position of the forearm and loss of motion.7,8 The limitation is often compensated by the ipsilateral shoulder and wrist, especially in mild deformity with the forearm fixed in neutral rotation (20° supination to 20° pronation). However, CRUS can be extremely disabling, severely restricting basic daily activities, particularly when bilateral or in case of severe pronation or supination exceeding 20° of forearm rotation. 9
Surgical treatment is generally recommended in case of disabling CRUS, in which many daily life activities are limited. The main surgical procedures can be summarized in mobilization surgery (consisting of the excision of the bar and the eventual interposition of tissue) or reposition surgery (which places the forearm in a more functional position by rotation osteotomies). Theoretically, surgical mobilization is considered the ideal treatment, allowing complete restoration of the forearm range of motion (ROM). However, some authors reported unsatisfactory outcomes and a high rate of recurrences.10,11 Therefore, rotation osteotomy is currently the most practiced technique for severe CRUS.1,5
Although several studies reported satisfactory surgical results of rotation osteotomy, there is insufficient information concerning the effectiveness of surgical correction over nonoperative treatment. Specifically, only a few studies have reported information on non-operated patients, and just as few have provided objective clinical-functional outcomes using clinical-functional clinician-reported scores. Only one study has utilized patient-reported outcomes.1,5,12 Therefore, we aimed to investigate the baseline characteristics, and the clinical and functional outcome of a cohort of children with CRUS, undergoing operative or non-operative treatment.
Materials and methods
Study design and baseline patient characteristics
The present study is a multicenter retrospective investigation of a cohort of children with CRUS admitted at three European tertiary referral centers for pediatric orthopedics. The study was approved by the Institutional Review Board of the coordinator hospital. All children (aged < 18 years) with a diagnosis of CRUS assessed between January 1998 and April 2021 were included. The informed consent was obtained from all parents. Secondary proximal radio-ulnar synostosis (i.e., post-traumatic or iatrogenic) was excluded. Patient’s characteristics at baseline (age at presentation; sex; forearm rotation and position, elbow, and wrist ROM; and radiographic features) were extracted from medical records and plain radiographs. The position of the forearm was measured by a standard goniometer, considering positive values for pronation and negative values for supination. Based on the degree of forearm rotation, the position was classified as neutral if between −20° and +20°, as moderate pronation (20° to 45°) or supination (−20° to −45°), and as severe pronation or supination if exceeding 45° in either direction.
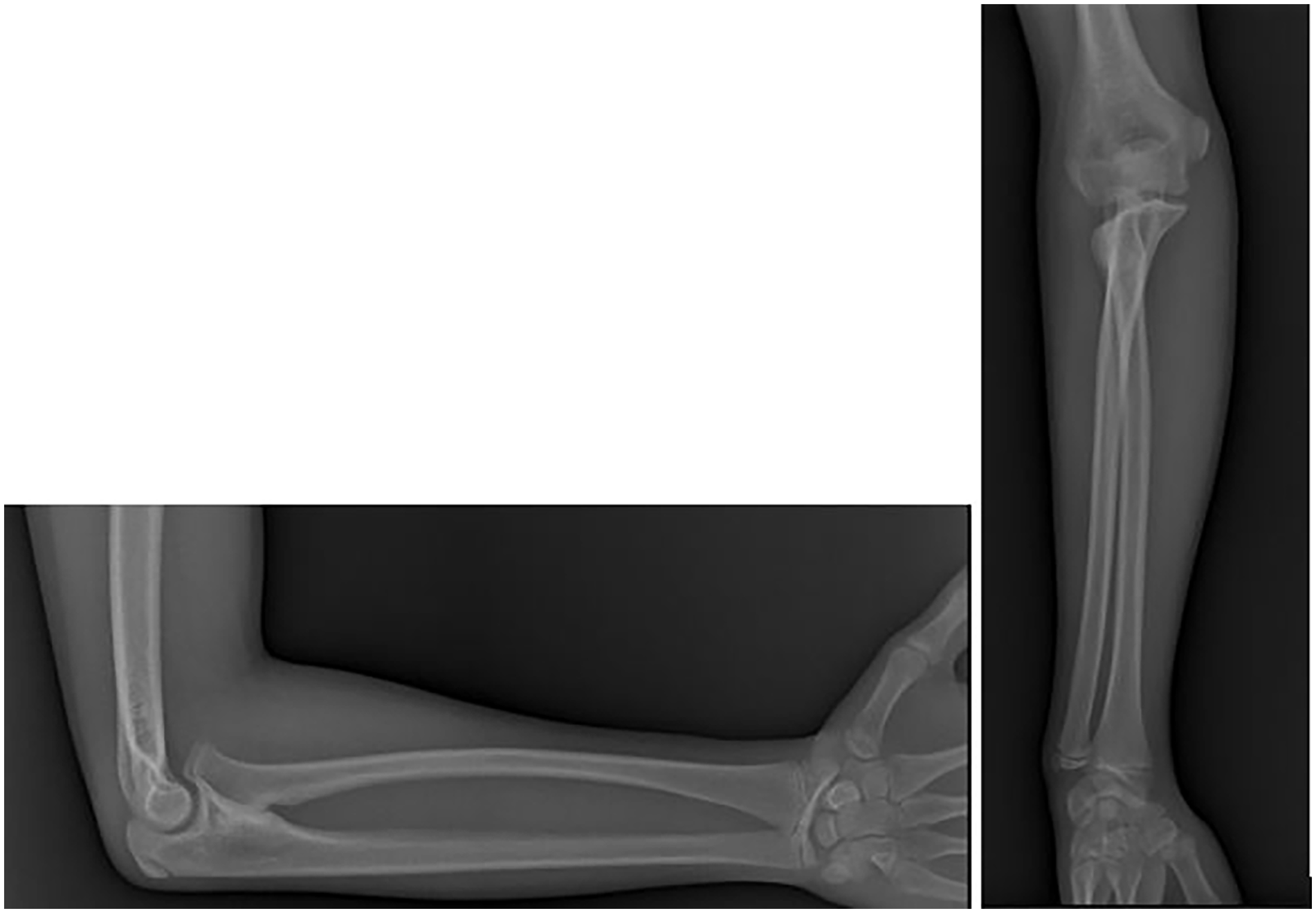
Elbow and wrist ROM were assessed at baseline, considering the normal values reported by the American Association for Orthopedic Surgery (AAOS).13 –15 According to the AAOS, normal elbow flexion-extension ranges from 150° to 0°, and normal wrist flexion-extension ranges from 80° of flexion to 70° of extension. On standard anteroposterior and lateral elbow radiographs, synostosis was classified according to the Cleary-Omer classification. 6 In this system, Type 1 is a fibrous synostosis with a normal radial head (Figure 1); Type 2 is an osseous synostosis without radial head dislocation (Figure 2); Type 3 is an osseous synostosis with the radial head dislocated posteriorly (Figure 3); Type 4 is a pseudo-synostosis with an anteriorly dislocated, mushroom-shaped radial head (Figure 4).

3D-CT images of a fibrous synostosis.

Antero-posterior and lateral X-rays of an osseous bridge with a correctly positioned radial head.

Type 3 synostosis shows a bony bridge and a posterior dislocated radial head in the X-ray images.
Antero-posterior and lateral X-ray images in a synostosis with an anteriorly dislocated deformed radial head.
Patients undergoing surgery were further investigated, for age at treatment, type of operation, hardware, and immobilization time. The surgery was indicated according to the surgeon’s expertise and in agreement with the parents. The decision considered the child’s difficulties with basic daily activities like eating, washing, personal hygiene, holding objects, dressing, writing, and drawing. Patients without significant disability in daily life activities generally did not require surgery. Surgery was recommended for those with a locked elbow in a non-functional position and evident disability. For clarity, we excluded the few mobilization surgery cases (two cases) and focused on rotational osteotomies, as they are the most common procedures in all three hospitals.
Surgical technique
The patient was placed in a supine position with a tourniquet at the arm. A longitudinal incision was made at the corresponding level of the synostosis along the subcutaneous border of the ulna. Subperiosteal elevation was performed around the synostosis, protecting the posterior and anterior interosseous nerves. In some cases, anterior transposition of the ulnar nerve was performed, according to the surgeon’s preference. After the exposition of the synostosis, an appropriately sized K-wire (typically 1.6–1.8 mm in diameter) was introduced percutaneously under fluoroscopy into the olecranon apophysis beyond the synostosis. The level of the osteotomy was chosen according to the surgeon’s preference and experience (generally at the level of the synostosis), and the forearm was gradually rotated until the neutral position was achieved. According to the literature, the ideal position would be in pronation of 0°–20° on the dominant side and in supination of 0°–20° on the non-dominant hand, although the optimal position in which the forearm should be fixed can be influenced by culture and custom. 1 Then, the osteotomy was stabilized by one or two K-wires, or by combining plate and wire fixation. In a few cases, no internal fixation was used, and the osteotomy was stabilized by cast only. The elbow’s motion was clinically checked to avoid impingement. Standard lay closure was performed, and the forearm was immobilized in a long-arm cast. The cast and the percutaneous K-wires, when present, were removed at the first postoperative visit, about 1 month after surgery.
Outcomes
Information about the clinical and functional results was abstracted from the latest follow-up visit reports in all patients (operative and non-operative). The entity of rotation and the final position of the affected forearm were recorded, and patients were scored according to the Mayo Elbow Performance Score (MEPS). 16 The MEPS is a clinician-reported functional score investigating four parameters (pain, elbow’s range of motion, joint stability, and ability to perform basic daily activities) with a maximum score of 100 points. A higher score demonstrates a better condition (91–100 points: excellent, 90–81 points: good, 80–71 points: fair, <70 points: poor condition).
Complications of operative cases were classified based on the modified Clavien-Dindo-Sink (CDS) classification for quantifying patient outcomes based on the treatment that the complication required and its long-term morbidity.12,17
All patients were contacted by mail and/or phone to complete the shortened version of the Disabilities of the Arm, Shoulder and Hand Outcome Measure (Quick-DASH), a patient-reported 11-item questionnaire with an additional 4-question sports/performance module for assessing upper limb function in musculoskeletal disorders. The Quick-DASH is validated for children over 8 years old with upper extremity pathology.18,19 Scores range from 0 (no disability) to 100 points (maximum disability), with higher scores indicating greater disability. 18 In our study, we excluded the work module due to patient age and used normative data for young adults since baseline Quick-DASH scores were not collected. A score of ≤7 points was considered within the first quartile of healthy individuals, while sports module scores of 6 points for males and 13 points for females were also within this range. 20 Scores below these thresholds suggest no perceived clinical or functional issues with the affected elbow. All questionnaires were administered in the languages of the participating hospitals.21,22
Statistical analyses
Continuous data were expressed as means ± standard deviation (SD) and range, whereas categorical and ordinal data were expressed as absolute values and percentages. Normality was tested using the chi-square test for categorical variables and the Kolmogorov–Smirnov test for continuous variables.
Differences between groups were analyzed using the Student’s t-test or ANOVA with post hoc Bonferroni or Tamhane correction for normally distributed variables. For non-normally distributed variables, the Mann–Whitney test or Kruskal–Wallis test was employed. Bivariate analyses were conducted using Pearson or Spearman correlation coefficients, selected based on the distribution of the variables. The strength of correlation was classified based on the correlation coefficient as negligible or none (<0.10), weak (0.10–0.39), moderate (0.40–0.69), strong (0.70–0.89), and very strong or perfect (0.90–1.00). Exploratory univariable and multivariable analyses were conducted using linear or logistic regression, as appropriate, to identify possible associations between baseline variables and outcomes. Linear mixed-effect models with patients as random effects were used, to avoid violation of the principle of independence in bilateral cases. Results were presented as crude and adjusted means with 95% confidence intervals. A p-value of <0.05 was statistically significant, and all reported p-values are two-sided. We used Excel (Microsoft, Redmond, WA, USA) and SPSS (version 25.0; IBM Corp, Armonk, NY, USA) for analysis.
Results
Patient demographics and baseline characteristics
Ninety-seven patients were included (32 females and 65 males). Patients’ demographics and characteristics at baseline are reported in Table 1. Thirty patients (7 females and 23 males, 32,6%) presented a bilateral deformity, thus leaving 122 forearms for the final analysis. A notable predominance of bilateral presentation was observed in males (p-value = 0.053), with a preference for the left side (p-value = 0.027). Twelve patients (13.0%) reported associated conditions (mainly cognitive impairment). The average age at the first clinical evaluation was 6.9 ± 3.3 years (range 0–20.5 years). The elbow was fixed in neutral position in 33/122 cases (27%), in supination in 2/122 cases (1.6%), and in excessive pronation in 72/122 cases (59%), while the initial forearm position was not reported in 15/122 cases (12.3%). As expected, non-operated cases predominantly exhibited neutral or moderate pronation, whereas operated cases showed a higher prevalence of excessive pronation or supination.
Patients’ characteristics at initial evaluation, differentiating between those managed non-operatively and those who required surgery.
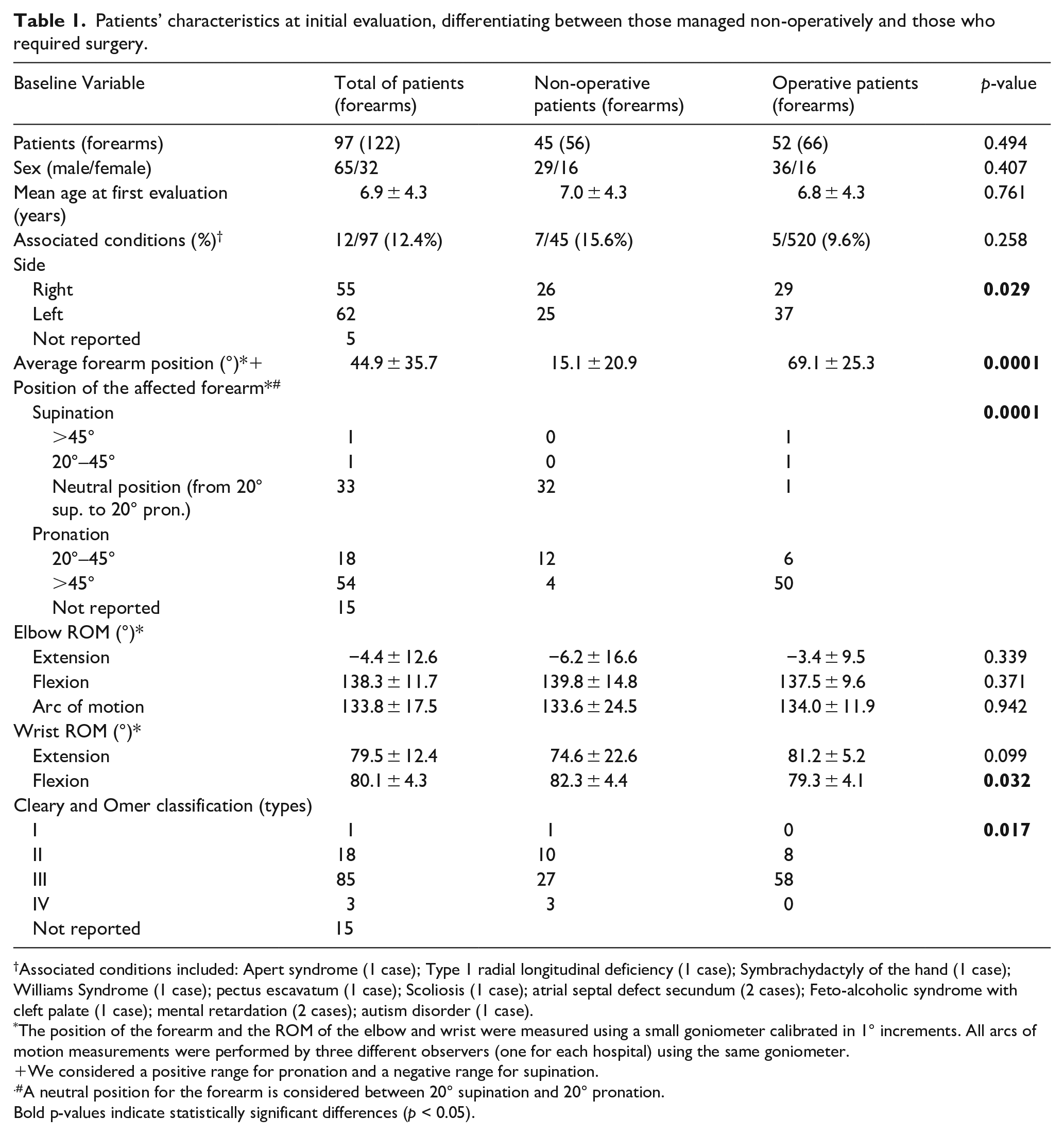
Associated conditions included: Apert syndrome (1 case); Type 1 radial longitudinal deficiency (1 case); Symbrachydactyly of the hand (1 case); Williams Syndrome (1 case); pectus escavatum (1 case); Scoliosis (1 case); atrial septal defect secundum (2 cases); Feto-alcoholic syndrome with cleft palate (1 case); mental retardation (2 cases); autism disorder (1 case).
The position of the forearm and the ROM of the elbow and wrist were measured using a small goniometer calibrated in 1° increments. All arcs of motion measurements were performed by three different observers (one for each hospital) using the same goniometer.
We considered a positive range for pronation and a negative range for supination.
A neutral position for the forearm is considered between 20° supination and 20° pronation.
Bold p-values indicate statistically significant differences (p < 0.05).
The elbow and wrist arc of motion were in the range of normality in 81% and 98% of forearms, respectively. We observed a statistically significant, but clinically negligible reduction in wrist flexion in the operated cases (see Table 1). Preoperative radiographs were obtained and evaluated in 106 cases (86.9%). Among these, types I and IV were much less frequent and did not require surgery; Type II was nearly equally distributed between operative and non-operative cases; Type III CRUS was the most common and required surgery in more than two-thirds of cases; this asymmetry in the distribution of operated and non-operated cases was statistically significant (see Table 1).
Operative cases
We reported the characteristics of the operative group in Table 2.
Characteristics of the operative group undergoing proximal rotational osteotomy at the level of synostosis.
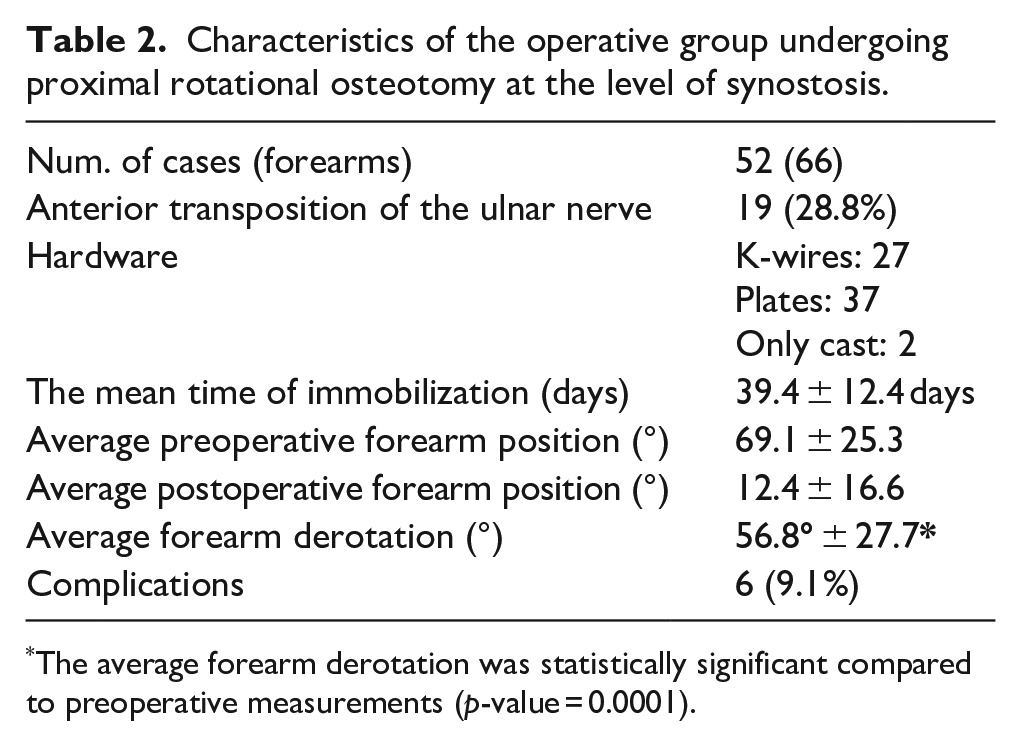
The average forearm derotation was statistically significant compared to preoperative measurements (p-value = 0.0001).
The mean age at surgery was 6.8 ± 4.3 years. All patients underwent proximal rotational osteotomy at the level of synostosis. and in 15 patients (19 elbows) an associated anterior transposition of the ulnar nerve was performed. To stabilize the osteotomy, K-wires were used in 24 patients (27 forearms) and plates in 29 patients (37 forearms). An immobilization cast was applied in every case. In two cases (2 forearms), only a cast was used without any hardware. The mean time of immobilization was 39.4 ± 12.4 days. In operated patients, we achieved an average forearm derotation of 66.5° ± 15.1° (p = 0.0001). Thirty-nine forearms (61.9%) reached a neutral position, 16 showed partial correction with residual moderate pronation (25.4%), and 7 (11.1%) exhibited no significant change in final forearm position. One forearm (1.6%) was overcorrected to moderate supination, while in three cases, the degree of correction could not be assessed due to lacking preoperative data.
We reported six complications in six patients (6.5%). Five were classified as minor (CDS types 1–2): two patients experienced transient radial paresthesia post-treatment, and two had weakness and slight limitation in thumb and index finger ROM post-surgery. All minor symptoms resolved spontaneously within a few months. One patient developed a mild compartment syndrome that resolved without additional surgery. The only major complication (CDS type 3B) was a compartment syndrome that required surgical fasciotomy. This patient was subsequently lost to follow-up.
Follow-up and outcomes
Overall, 16 patients (17.3%; 1 bilateral case) were lost to follow-up. We reported in Table 2 the characteristics of operative and non-operative groups. No significant differences in follow-up period or age at the latest visit were observed. MEPS was available for 59 patients (64%, including 13 bilateral), while 58 (63%, including 12 bilateral) completed the Quick-DASH questionnaire. A correlation was found between MEPS and Quick-DASH (Spearman’s r = −0.76; p = 0.0001), Quick-DASH and its sports module (Spearman’s r = 0.53; p = 0.0001), and Quick-DASH sports module and MEPS (Spearman’s r = −0.37; p = 0.0001). Age at presentation showed a weak correlation with both Quick-DASH (Spearman’s r = −0.27; p = 0.021) and MEPS (Spearman’s r = 0.33; p = 0.005). No significant differences were observed between operative and non-operative groups (see Table 3).
Clinical and functional scores of non-operated and operated patients at the most recent follow-up.
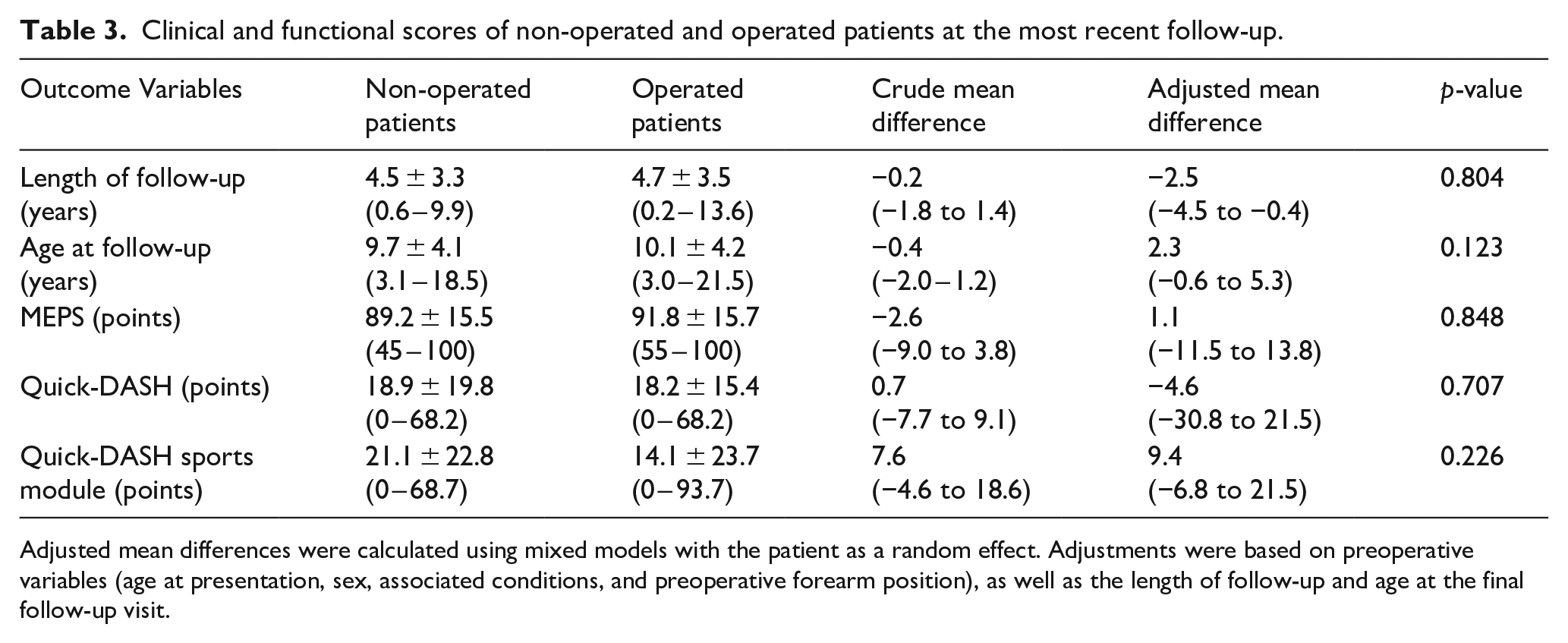
Adjusted mean differences were calculated using mixed models with the patient as a random effect. Adjustments were based on preoperative variables (age at presentation, sex, associated conditions, and preoperative forearm position), as well as the length of follow-up and age at the final follow-up visit.
Based on MEPS, results were typically positive (excellent in 37 patients (62.7%), good in 9 (15.2%)). Only 18 patients (31%) reported a quick-DASH ≤ 7 points. Based on Quick-DASH (item 9), 70% of cases had no pain, 15.7% had mild pain, 12.9% had moderate pain, and only one patient (1.4%) reported severe pain. The pain reported on Quick-DASH strongly correlated with pain reported on MEPS (Spearman’s r = −0.875, p = 0.0001). No further correlations were found between the presence of pain and any baseline or follow-up variables, except for a weak correlation with elbow flexion (Spearman’s r = 0.4 with Quick-DASH and −0.3 with MEPS). Four females (20% of respondents) scored below the normative value of 13 points on the Quick-DASH sports module, compared to 30 males (76.9%). The mean difference of 15.3 ± 5.8 points between males and females was statistically significant (p = 0.011). This difference was not observed in other scores.
Discussion
Although considered the most frequent congenital anomaly of the elbow, CRUS is a very rare condition.1,2,23 To date, we reported the largest cohort of pediatric patients with CRUS, detailing the clinical and functional outcomes of both operative and non-operative cases.
Originally described as an isolated and sporadic congenital deformity,3,4,24 CRUS is increasingly reported in syndromic associations and familiar presentations with identified genetic mutations. Our study also documented cases of CRUS in association with syndromic conditions, highlighting the need for further genetic research.3,25,26 We confirmed the male predominance and found bilaterality in one-third of cases, slightly less than in previous studies.1,12,16,17 The forearm is usually fixed in pronation, whereas supination is uncommon occurring in less than 2% of our cohort, but it is more disabling and almost always requires surgical correction.6,16 As expected, patients with severely pronated forearms presented earlier and were significantly more frequent in the operative cohort. On radiographs, we applied the Cleary and Omer classification, finding that type 2 and type 3 accounted for more than 95% of cases. Moreover, we observed that Type 3 CRUS was more severe and frequently required surgery. This observation aligns with a recent literature review, which found that 59.1% of all diagnosed CRUS cases were Type 3, particularly those requiring surgical intervention. 1 The rarity of Types 1 and 4, which did not typically require surgery in our experience, suggests a severity gradient, giving the radiological classification potential prognostic value rather than being purely descriptive. Recently, a new MRI-based classification has been proposed, focusing on the presence and size of forearm muscles, particularly the supinator. However, this classification has not yet been formally validated for its prognostic value.27,28 In our cohort, 42 patients (45%) were treated only by observation and showed substantial good clinical function at almost 5 years, confirming an adequate compensation by the ipsilateral shoulder and wrist if the forearm is neutral or in slightly pronation.4,29,30
However, 52 patients were indicated for surgical management undergoing rotational osteotomy at the level of the synostosis. We reported complications (generally transient nerve palsies that involved the radial or the interosseous nerve) in 6.5% of cases. Only one case (1.1%) showed a severe compartment syndrome that required surgical fasciotomy. At the most recent follow-up, patients achieved a stable neutral position of the forearm in 62% of cases, partial correction in 24% of cases, and loss of correction or recurrence in 14% of cases. These findings appeared independent of the type of fixation, although slightly better clinical outcomes were associated with the use of plates. As already reported by Shingade et al., 31 the achievement of a neutral or slightly pronated final position is associated with satisfactory clinical and functional outcome.
The best position in which the forearm should be derotated remains debated. It mainly depends on the laterality of the defect and the customs of the patient, although also the initial position of the forearm should be considered. In fact, a wide rotation angle could be associated with higher neurovascular risks.1,4,9,12,16,17,32 –42 In our cohort, we found a significant difference in forearm side between operative and non-operative cases, being the left forearm being more represented among the operative patients (38 left sides and 30 right sides), although no statistically significant differences were found. Despite we lack of information about the dominant hand, we can argue that the left hand requires more supination since it is generally the non-dominant hand.1,23,43
In literature, although isolated bar resection (with or without soft tissue interposition) has been proposed for restoring prono-supination, it did not gain popularity because of the reported high rate of failure. 39 We compared operative and non-operative patients, and, with the available data, we found no significant differences in clinician-reported and patient-reported outcomes between them even after adjustment for preoperative variables and length of follow-up. Our study demonstrated that a fixed forearm in a neutral position (eventually surgically achieved) might not necessarily hinder high-performance activities, 44 even if only about 30% of patients achieve Quick-DASH scores comparable to the general population. The true extent to which surgery contributes to clinical improvement compared to non-operative management remains unclear. To answer this, precise and long-term patient-reported data on cases with severe deformities who did not undergo surgery are needed. In our cohort, among the 32 conservatively treated patients who completed the Quick-DASH, 11 had moderate to severe fixed pronation deformity (>20°). This subgroup had an average Quick-DASH score of 24.2 points, compared to 16.1 points in patients with mild deformity and neutral forearm position. Although the difference between the two subgroups was not statistically significant (p-value = 0.414), an average Quick-DASH score of 24.2 points suggests a potentially significant residual disability that may justify surgical intervention.
Our study has inherent limitations. Although it represents the largest cohort of patients with CRUS, the retrospective nature, the limited number of available data, the high rate of missing data, the loss of follow-up limit, and weaken the quality of our analysis. We lack baseline patient-reported information to understand if and what conditions (pain, disability, aesthetic, and psychosocial concerns) perceived by patients and parents lead to the choice of operative or non-operative treatment, and how much rotational osteotomy can modify these conditions. We did not report the side dominance that is important for deciding the final position of the forearm.1,4,12,16,17,34 –37,39 We used a clinician-based score and a patient-based score that was already used in children with CRUS, although their use is debatable. In particular, the Quick-DASH was designed for adults and, despite adaptations for children,18,19 has never been used in children younger than eight. This limitation restricts its preoperative use in our cohort, which had an average age of fewer than 8 years at presentation, making it impossible to compare pre- and post-surgery clinical outcomes. Lacking a control group of matched healthy individuals, we used normative values for young adults to gauge function at the final follow-up. 20 However, despite similar values being reported in a population of children with an average age of 10 years, at least 2 years post-upper limb fracture, this approximation introduces potential bias. Our cohort had an average age of 9–10 years at the last follow-up, with less than 10% reaching adulthood by that time. A longer follow-up might reveal symptoms or degenerative changes in adulthood, regardless of treatment type.
In conclusion, CRUS is a rare malformation, typically diagnosed at school age, often causing parental concern. Our data show that prono-supination restriction is generally well tolerated with minimal or occasional mild pain, especially in patients with forearm rotation within a favorable range (20° supination to 20° pronation). Thus, non-operative treatment should be the first choice. In severe deformities, derotational osteotomy is a safe, low-risk procedure that restores a neutral forearm position with outcomes comparable to non-surgical management of mild cases. Comparative studies on alternative techniques, such as mobilization surgery, are needed to identify the most effective approach for optimal clinical and functional outcomes.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251322677 – Supplemental material for Operative and non-operative treatment of congenital radio-ulnar synostosis in children: Results from a multicenter study
Supplemental material, sj-pdf-1-cho-10.1177_18632521251322677 for Operative and non-operative treatment of congenital radio-ulnar synostosis in children: Results from a multicenter study by Paola Zarantonello, Giovanni Trisolino, Filippo Maria Senes, Giovanni Luigi Di Gennaro, Diego Antonioli, Nunzio Catena, Annalisa Culmone, Alexandra Stauffer, Laetitia Sophie Chiarella and Sebastian Farr in Journal of Children’s Orthopaedics
Footnotes
Authors contributions
Paola Zarantonello (PZ) conceived the study, developed the methodology, contributed to the analysis of the results, and wrote the manuscript in consultation with GT, GLDG, NC, and SF. Giovanni Trisolino (GT) directed the project, contributed to the study conceptualization, analyzed and interpreted the results, wrote the manuscript in consultation with PZ, GLDG, NC, and SF, and acquired financial support for the project leading to this study. Filippo Maria Senes (FMS) provided data from patients, performed measurements and calculations, aided in interpreting the results, provided technical details concerning the surgical techniques, and reviewed and edited the initial draft of the manuscript. Giovanni Luigi Di Gennaro (GLDG) contributed to study conceptualization, provided data from patients, contributed to the analysis of the results wrote the manuscript in consultation with PZ, GT, NC, and SF. Diego Antonioli (DA) provided data from patients, performed measurements and calculations; and provided technical details concerning the surgical techniques. Annalisa Culmone (AC) provided data from patients and performed measurements and calculations. Nunzio Catena (NC) provided data from patients, performed measurements and calculations, aided in interpreting the results, and wrote the manuscript in consultation with PZ, GT, GLDG, and SF. Alexandra Stauffer (AS) performed measurements and calculations and reviewed and edited the initial draft of the manuscript. Laetitia Sophie Chiarella (LSC) performed measurements and calculations, performed measurements and calculations, and reviewed and edited the initial draft of the manuscript. Sebastian Farr (SF) supervised the present study, contributed to study conceptualization, provided data from patients, contributed to the analysis of the results, and wrote the manuscript in consultation with PZ, GT, GLDG, and NC. All authors provided critical feedback on the study, discussed the results, and helped shape the research, analysis, and manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research (and APC) were funded by the Italian Ministry of Health — 5 × 1000 Anno 2022, Redditi 2021 “ Modellazione3D, Progettazione e Correzione di Deformità Muscolo-scheletriche Sostituzioni Protesiche
Ethical statement
The study was approved by the Institutional Review Board of the coordinator hospital (IRCCS Rizzoli Orthopaedic Institute); ethical board committee approval code: CE-AVEC 803/2020/Oss/IOR, date: 12/10/2020.
Informed consent
All participants to the study gave informed consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.