
Abstract
Purpose:
Manual anthropometric evaluations of pediatric lower extremities are essential in orthopedic pediatric practice due to their noninvasive and time-feasible nature. Therefore, this study aims to assess the test–retest reliability of clinical measurements obtained on children to examine measurement stability over time.
Methods:
In a test–retest design, data were collected from 50 Danish school children with 5–to 6 weeks between sessions. Measurements encompassed the joint range of motion (ROM), rotational profile, and angular alignment of lower extremities for a representative sample of school children. Reliability was assessed using intraclass correlations (ICC), and agreement was assessed using limits of agreement (LoA) and precision.
Results:
Reliability analysis revealed excellent results for foot length (ICC > 0.9), good results for foot width (ICC < 0.9), and poor to moderate results for all other measurements (ICC < 0.5, ICC < 0.75). Agreement results for hallux valgus were acceptable (within established reference) and the remaining variables were not acceptable (outside established reference).
Conclusions:
The majority of the manual assessment procedures were found to have poor reliability. This study highlights the need for reliable and time-efficient tools to assist clinicians in assessing manual clinical measurements and future research should explore this.
Level of evidence:
Level III.
Reliability is a crucial element of trustworthiness in the field of research and measurement. Evaluating discrepancies in reliability between tests or equipment that are challenging to execute accurately necessitates intricate designs and corresponding analysis. 1 With the ever-increasing demand for research and thus reliable data, understanding the nuances of test–retest becomes crucial. Evaluation of the reliability of clinical measurements serves to obtain robust and dependable measurements and is essential to orthopedics due to its significance for standard clinical practice, diagnostics, and interventions. To have confidence in clinical decision-making, stability and reproducibility of clinical measurements between sessions must be ensured.
Overall, data reliability assessments are an important aspect of database applicability. It can be divided into three subcategories: test–retest reliability, internal consistency, and interrater reliability, in turn, to evaluate variability and measurement error over time, across items, and across researchers, respectively. Test–retest reliability plays a critical role, offering insights into the consistency and stability of measurements over time. In essence, it refers to the ability of a measurement to consistently yield similar results when administered under the same conditions and using the same methods. Reliability can be influenced by various sources such as participants, examiners, or environmental factors. It is important to consider these sources of influence when conducting studies to minimize their impact on the results.
Reliability for pediatric joint motion measurements has not yet been established. 2 Therefore, the main aim of this study is to estimate and evaluate the test–retest reliability of lower extremity joint range of motion, rotational profile, and angular alignment of the lower extremity in the pediatric population. This will elucidate how accurate and stable clinical manual measurements are over time.
Methods
Design and participants
This study is a part of the PA.NI.C Feet study (Pathologies and Interventions in Children’s Feet), a cross-sectional study that examines children in Danish primary schools’ feet and pathologies. The PA.NI.C-study aims to assess children’s lower extremity morphologies to quantify children’s feet status and abnormalities and to determine whether prevention and rehabilitation can be installed instead of surgical interventions. 3 The PA.NI.C Feet study examined the lower extremity morphology and pathology of 501 children in Danish primary schools in the first, fifth, and ninth grades. Overall, examinations were performed by specifically educated podiatrists and involved foot size, shape, foot health, rotational profile, angular alignment, and range of motion in lower extremity joints. Foot health includes conditions such as callosities, warts, ingrown nails, and other pathologies. These were documented in the evaluation forms during both tests and retests, following the same procedures as all other measurements. Since this article focuses on clinical manual measurements, the foot health data were excluded from the interpretation in this test–retest study. In this current study, a subset of 50 children that were included in the PA.NI.C-study were randomized to participate in retest examinations to evaluate the reliability and agreement of the data obtained in the PA.NI.C Feet study with intraclass correlation (ICC), limits of agreement (LoA), and precision as primary outcomes.
Retests took place 5–6 weeks after the primary tests, with the same podiatrist examining the same child as in the initial assessments. The clinicians involved deemed the children as stable study subjects, reasoning that time did not exert a significant influence on their development. In total, 50 children participated in the retest examinations. Of those 23 were girls and 27 were boys. 21 in first grade, 25 in fifth grade, and 4 in ninth grade. The mean age was 10.35 years, the mean height was 145 cm, and the mean weight was 38 kg (Table 1).
Descriptive statistics of the 50 children included in the analysis of test–retest reliability of clinical measurements in the lower extremity.
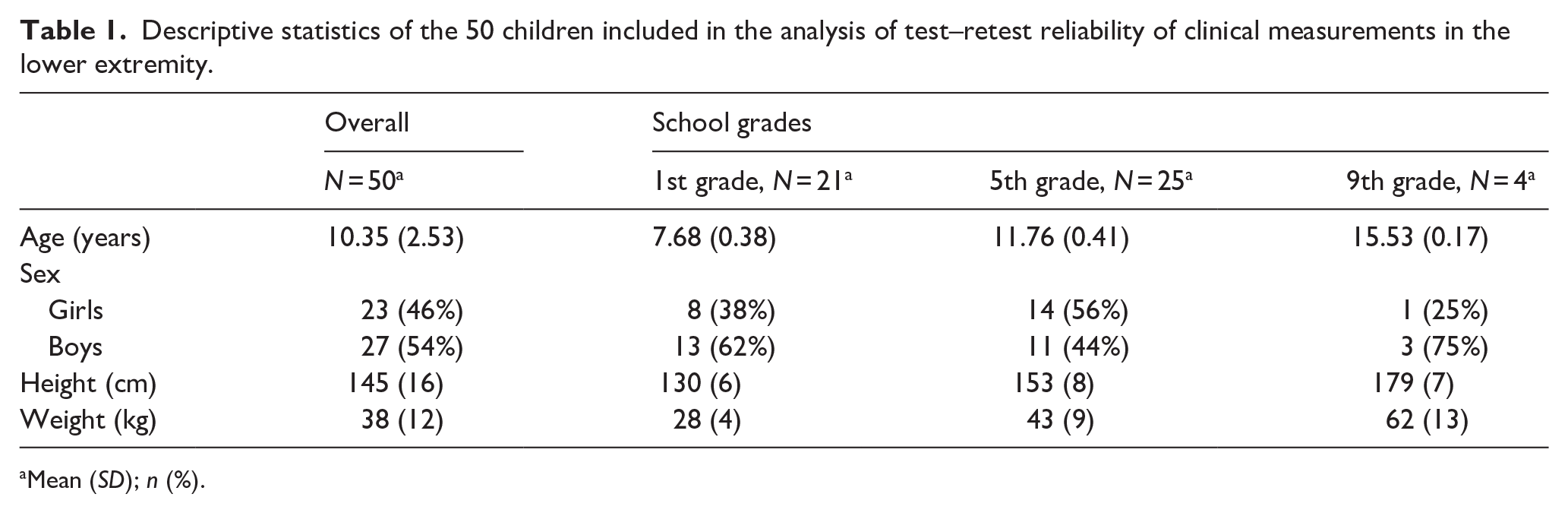
Mean (SD); n (%).
Ethics
This study was declared as a non-scientific study and thus not appropriate for evaluation for approval following the Danish Act on Research Studies (journal nr.: 21054014). Regional registration was obtained in accordance with the Danish Data Protection Agency as stipulated by Danish law J.nr. 2008-41-2240 and approved by the local review board (Privacy). The study adhered to relevant national guidelines and was carried out following the Declaration of Helsinki (JBJS 79A:1089-98,1997). Informed signed consents were obtained from all the participant’s legal guardians.
Measures
Podiatrists from the Association of Danish Podiatrists with clinical experience between 1.5 and 41 years performed the clinical assessments. The team comprised six podiatrists who worked collaboratively in pairs, with each podiatrist assigned to assess one participant at a time. They provided separate ratings and had the opportunity to consult with one another. They received complementing clinical education from pediatric orthopedic surgeons before the examinations for the PA.NI.C Feet study. As an initial preparation, the podiatrists conducted a full examination under the instruction of one pediatric orthopedic surgeon in three consecutive pilot retest sessions, where three children were evaluated independently three times at least 1 week apart to assess their ability to reproduce measurements. During the study, the podiatrists had ongoing opportunities to consult with the team of pediatric orthopedic surgeons regarding their procedures and findings. Each podiatrist conducted multiple trial runs of the tests on children of comparable ages to the participants, facilitating familiarization with the testing procedures and measurements.
Each child underwent a 30–40 min assessment, with the children being evaluated in pairs by their assigned podiatrist. This time frame allowed sufficient time to comfortably undergo examinations and was estimated based on a pilot study involving five children initiated before the study. Measurements were recorded on evaluation schemes and stored safely until subsequent manual data entry into the REDCap database.
The data collected in the study were assessed based on the neutral zero method: a principle of measuring joint function from a defined neutral 0-position. 4 A conventional goniometer was used to measure the function of the hip-, knee-, ankle-, and foot joints and for lengths, a Brannock device (The Brannock Device Company© (copyright logo) 2019, USA) was used.
Included parameters
Foot length
The distance between the most posterior contour of the foot and the longest toe. The participant stands up straight with equal weight on both feet. The foot length is assessed using a Brannock device.
Forefoot width
The distance between the medial and lateral forefoot edges. The participant stands up straight with equal weight on both feet. The foot width is assessed using a Brannock device on the widest part of the foot.
Arch height
The length from the floor to the navicular bone protrusion. The participant stands up straight with equal weight on both feet. The height is measured perpendicular to the floor and the navicular tuberosity.
Feiss line
Determination of the longitudinal arch of the foot. 5 The participant stands up straight with equal weight on both feet. The Feiss line is a clinical reference line for determining the navicular tubercle’s position and thereby the foot pronation and longitudinal arch of the foot. Feiss line extends from the apex of the medial malleolus to the first metatarsophalangeal joint. It is used as an imaginary line to assess whether the navicular tubercle is above, underneath, or intersects with the Feiss line and hereby the pronation and longitudinal arch of the foot. It is denoted whether the navicular tubercle is above, underneath, or intersects with the Feiss line.
Knee axis
The angle between the femur and the tibia in the frontal plane. The participant stands up straight with equal weight on both feet. The angle is measured with a goniometer. If the tibia deviates laterally, the angle is denoted as positive and is referred to as knee valgus. If the tibia deviates medially, the angle is denoted as negative and is referred to as knee varus.
Heel valgus and varus standing on flat foot
The angle between the calcaneus and tibia in the frontal plane. The participant stands up straight with equal weight on both feet separated one hip width. The angle is measured with a goniometer. If the calcaneus deviates laterally, the angle is denoted as positive and is referred to as heel valgus. If the calcaneus deviates medially, the angle is denoted as negative and is referred to as heel varus.
Heel valgus and varus standing on toes
The angle between the calcaneus and tibia. The participant stands on a maximal toe stance with equal weight on both feet. They are inspected from behind and it is denoted if the heel is in varus or valgus.
Hallux valgus
The angle in the first metatarsophalangeal joint. The participant stands up straight with equal weight on both feet. The angle between the longitudinal axis of the first metatarsal and the axis of the first toe is measured with a goniometer. If the first toe deviates laterally, the angle is denoted as positive and is referred to as hallux valgus. If the first toe deviates medially, the angle is denoted as negative.
Metatarsus varus
The severity of potential medial deviation of the forefoot. The heel is held in a neutral position and a line extending from the heel to the toes is drawn. The deviation of the forefoot is categorized as normal when the inner part of the foot is parallel with the line, and it intersects the second and third toes. When the metatarsals deviate medially, more of the toes appear on the medial side of the line and are categorized as mild, moderate, and severe using an evaluation scheme (Supplemental Figure 1).
Hip movement
The amount of movement in flexion, internal- and external rotation, abduction, adduction, and anteversion. The participant lies in a supine position and the passive movements of the joint are assessed using a goniometer. Flexion, abduction, and adduction are measured with the hip in extension and internal and external rotation with the hip and knee bent at 90° flexion. Anteversion is measured while the participant lies in a supine position with the hip and knee flexed 90°. The lower leg is then passively rotated outwards until trochanter major is palpable laterally. The angle between the axis of the tibia and the longitudinal axis is measured.
Knee movement
The amount of movement in flexion and extension between the femur and the tibia. The participant lies in a supine position and the passive movements of the joint are assessed using a goniometer. Knee flexion is measured with the hip flexed 90° and knee extension is measured with the hip in extension. Knee flexion is denoted as a positive angle and extension is denoted as a negative angle. When the lower leg cannot be extended to the neutral position, the extension is denoted as a positive angle.
Ankle movement
The amount of movement in plantarflexion and dorsiflexion. The participant lies in a supine position and the passive movements of the joint are assessed using a goniometer. The plantarflexion is assessed with the hip and knee in extension and dorsiflexion is measured with the hip and knee in extension and 90° flexion.
Tibial torsion angle
The angle between the intermalleolar line and the femur. The participant lies in a supine position with the hip and knee flexed 90°. The intermalleolar line is between the centers of the medial and lateral malleoli. The angle between the intermalleolar line and a line perpendicular to the long axis of the femur is then assessed using a goniometer.
Foot-thigh angle
The angle between the foot in a neutral position and the femur. The participant lies in a supine position with the hip and knee flexed 90°. The angle between the long axis of the femur and the long axis of the foot from the heel to the second toe is measured with a goniometer. If there is internal tibial torsion, the angle is denoted as negative and if there is external tibial torsion, the angle is denoted as positive.
Procedure
The reliability of the PA.NI.C Feet database and clinical applicability were evaluated based on the following outcome parameters: ICC, LoA, and precision.
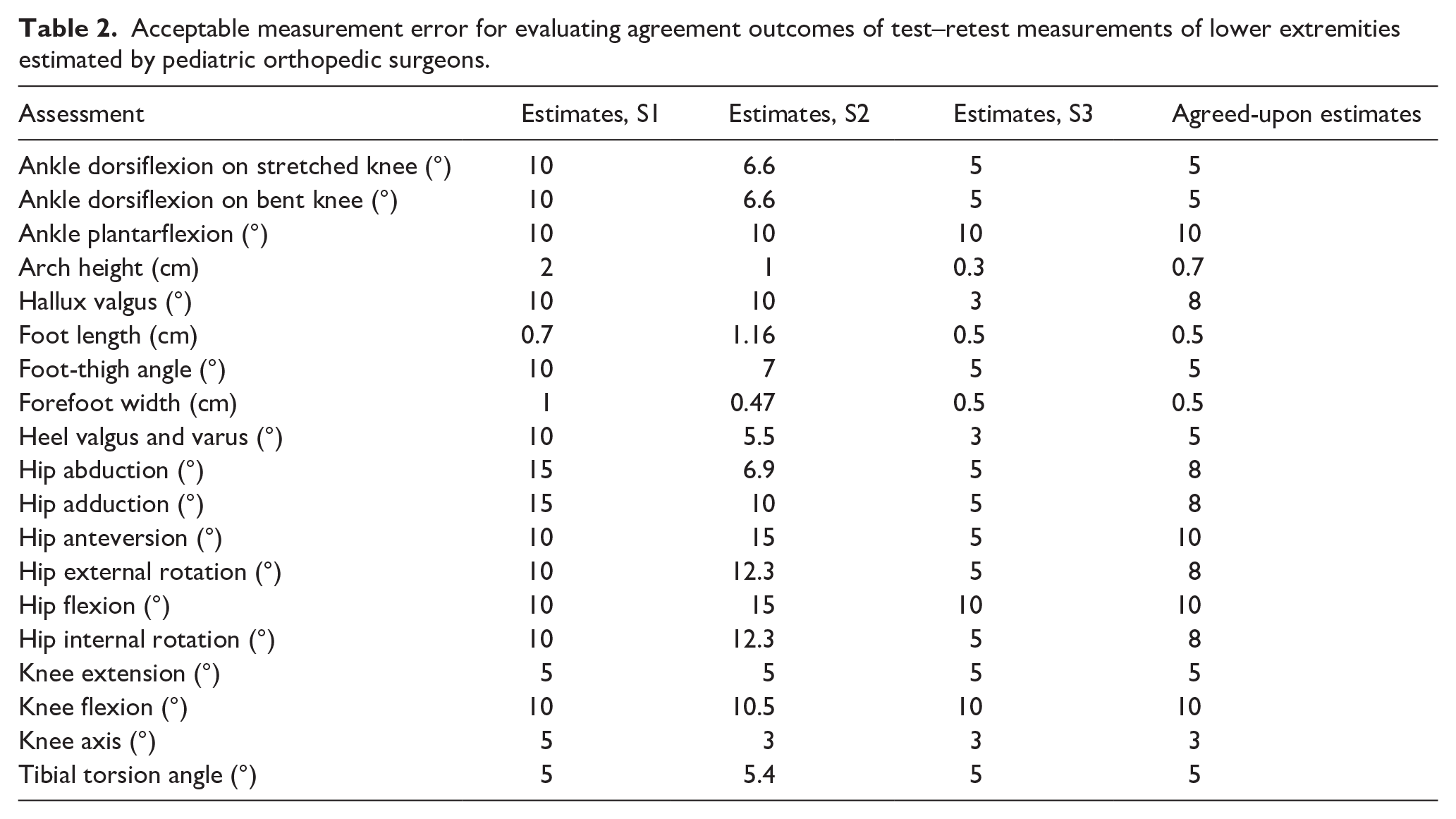
In general, when conducting reliability analysis, two parameters are considered: agreement and reliability. Agreement is the absolute error between two measurements and this article will express it as the LoA and precision. LoA is the 95% likely range of change of an individual’s measurement between two trials. 6 Precision is the degree to which an individual’s measurement between two trials shows the same result. 7 Whether an agreement measure is good and within the target ratio depends on the variation within the test population and the degree of measurement error allowed. 8 In this study, three consultant pediatric orthopedic surgeons (S1–S3) were asked to estimate acceptable measurement errors allowed for each of the assessments. These estimates are based on the maximal amount of measurement error allowed before requiring treatment or extrusive observation. The surgeons made their estimates independently and afterward the discrepancies were discussed to reach a consensus as a modified Delphi process (Table 2). In this article, agreement of the clinical measurements is interpreted using the agreed-upon estimates.
Acceptable measurement error for evaluating agreement outcomes of test–retest measurements of lower extremities estimated by pediatric orthopedic surgeons.
Reliability is determined by measuring errors concerning the heterogeneity of the sample participants. Accordingly, a greater spread within the population entails more accurate reliability measures. 9 The reliability of the assessments in this study will be expressed as the ICC. To assess the reliability of the manual clinical examination measurements, the test results will be compared to the retest results.
Data analysis
Measures were separated into continuous and categorical measures and analyzed accordingly. The analysis of the reliability for both continuous and categorical measures was performed using the ICC coefficient of consistency (ICC(2.1)C) and line of equivalence plots. ICC(2.1)C values were interpreted as follows: poor < 0.5, moderate < 0.75, good < 0.9, or excellent > 0.9. 10
The continuous measures were also analyzed by calculating 95% LoA and precision estimates. Precision was calculated as 1.96 × standard deviation of the difference and LoA was calculated as the mean difference ± 1.96 × standard deviation of the difference. Agreement was interpreted as either acceptable (within the agreed-upon estimates) or unacceptable (outside the agreed-upon estimates). Data are presented as mean and standard deviation unless otherwise stated. The absence of heteroscedasticity was ensured by evaluating mean difference plots. 6
Data were analyzed using the program “R” version 4.3.2. 11 and the packages tidyverse 12 and gtsummary. 13
Results
In the following section, the results are presented in continuous and categorical assessments respectively. Each measurement is presented with its corresponding outcome parameter: ICC, LoA, and precision if applicable (Tables 3 and 4).
Reliability results of continuous test–retest measurements of lower extremities for the 50 included children.
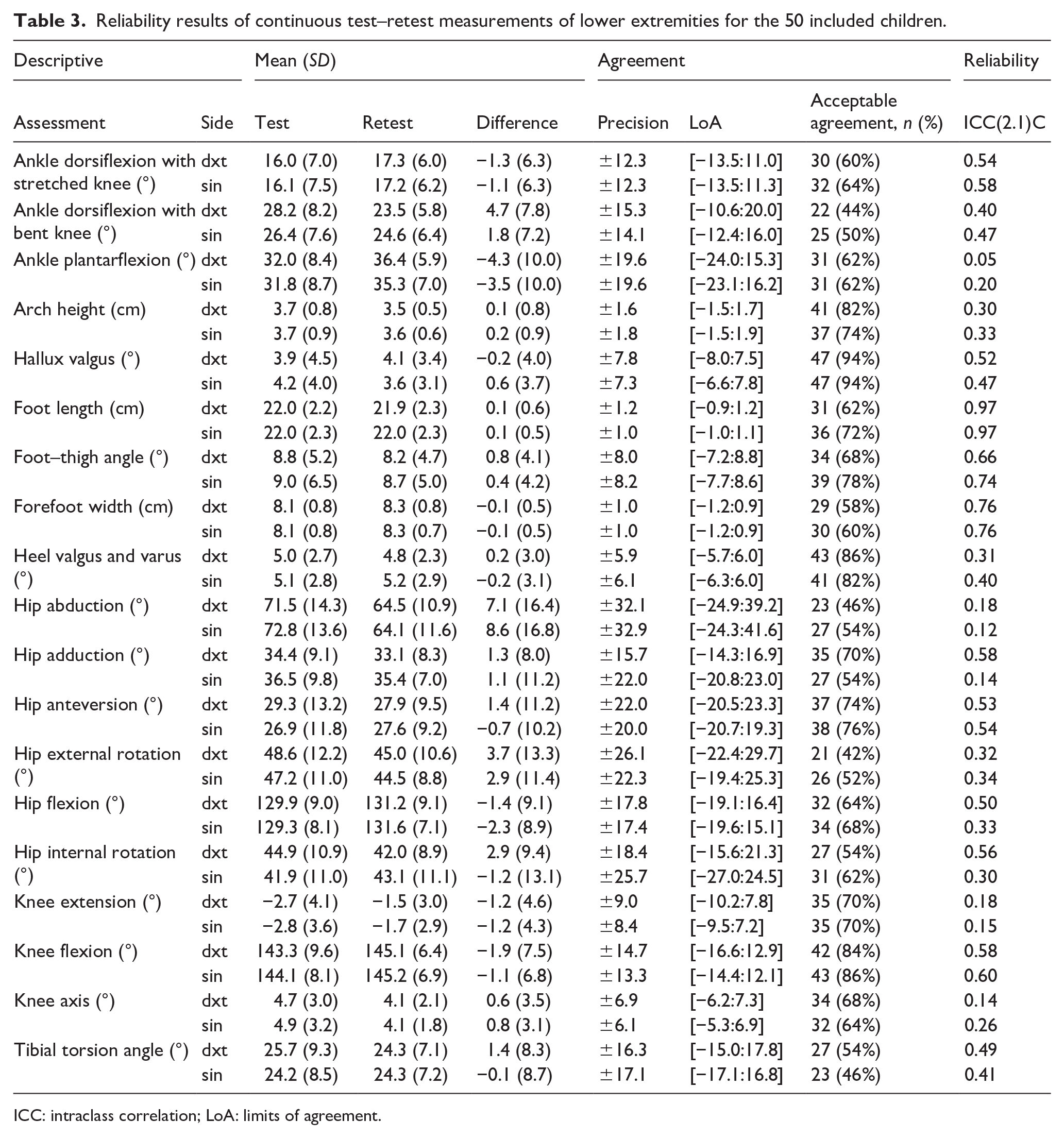
ICC: intraclass correlation; LoA: limits of agreement.
Reliability results of categorical test–retest measurements of lower extremities for the 50 included children.
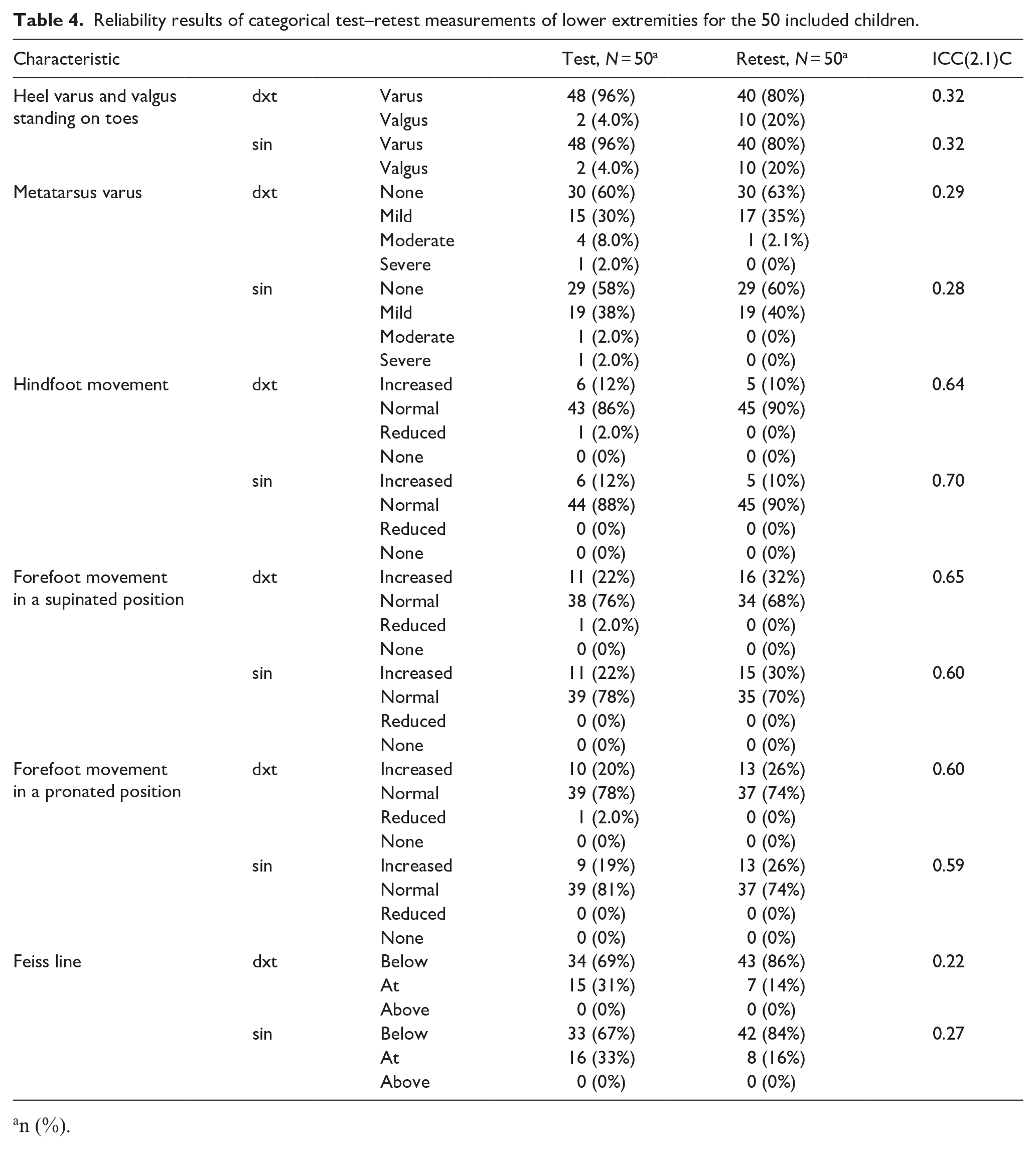
n (%).
Continuous assessments
In the examination of the clinically obtained continuous measurements, the estimated ICC across tests and retests was excellent for foot length (0.97 and 0.97). Measurements of forefoot width (0.76 and 0.76) reached good levels. Assessments of dorsal flexion of the ankle with stretched knee (0.54 and 0.58), right-sided hallux valgus (0.52), foot–thigh angle (0.66 and 0.74), right-sided hip adduction (0.58), hip anteversion (0.53 and 0.54), right-sided hip flexion (0.50), right-sided hip internal rotation (0.56), and flexion of the knee (0.58 and 0.60) only reached moderate levels. The estimated ICC for the remaining measurements was poor (Table 3).
The estimated agreement for hallux valgus (7.8° and 7.3°) was found to be acceptable with 94% of the assessments within the agreed-upon estimates. The remaining measurements were outside the agreed-upon estimates. However, 82% of right-sided arch height assessments, 86% and 82% of heel valgus and varus assessments, and 84% and 86% of knee flexion were within the agreed-upon estimates. Right-sided ankle dorsiflexion on the stretched knee (44%), right-sided hip abduction (46%), right-sided hip external rotation (42%), and left-sided tibial torsion angle (46%) had more than half of the assessments outside the agreed-upon estimates.
The following line of equivalence plots represents reliability estimates reaching excellent, moderate, and poor values. Furthermore, mean difference plots (Bland-Altman limits of agreement plots) are presented for each of the three measurements demonstrating unequal scatter of points (Figure 1).

Line of equivalence plots and mean difference plots for foot length, knee flexion, and knee extension. Foot length exhibits excellent reliability, knee flexion exhibits moderate reliability, and knee extension exhibits poor reliability.
Categorical assessments
In the examination of the clinically obtained categorical measurements, the estimated ICC across tests and retests reached moderate levels for hindfoot movement (0.64 and 0.70), forefoot movement in a supinated position (0.65 and 0.60), and forefoot movement in a pronated position (0.60 and 0.59). The estimates for heel varus and valgus, metatarsus varus, and Feiss lines were categorized as poor (Table 4).
Discussion
This study analyzed the test–retest reliability of manual clinical assessments of children’s lower extremities. The majority, 46 out of 50, of parameters measured reached poor to moderate levels of reliability and four parameters reached good to excellent levels. The majority of the agreement assessments were not acceptable according to the agreed-upon estimates proposed by the team of pediatric orthopedic surgeons.
Several estimates of hip range of motion including adduction, flexion, and internal rotation exhibited moderate levels of reliability on the right side but poor levels on the left side. The notable variation between the estimates may not stem solely from increased challenges in measuring the left side compared to the right. One potential explanation could be that podiatrists assessed hip joint range of motion predominantly from the right side of participants, potentially resulting in increased measurement error for left-sided measurements. Furthermore, all podiatrists performing retests were right-handed. Anteversion of the hip was the sole hip measurement achieving moderate levels of reliability for both sides. According to Choi and Kang, 14 anteversion poses a great challenge in measurement due to difficulties palpating and locating the trochanter major while maintaining the internal rotation of the hip and measuring the alignment with the goniometer. We encountered similar obstacles for alignment estimation by our podiatrists. However, this difficulty may have entailed greater attention to the specific measurement method, potentially resulting in improved reliability. Hip abduction reached the lowest value of reliability compared to the other hip range of motion measurements, which was also reported by Mutlu et al. 15 This is intriguing, as sagittal range of motion generally is expected to be more accurate than rotational range of motion measurements.
Surprisingly, the knee axis reliability estimates were poor despite exhibiting minimal absolute measurement error (6.1° and 6.9°) compared to the other measurements. This indicates significant challenges in determining the angle, which the pediatric orthopedic surgeons are aware of, as they presented a low-valued measurement error estimate (3°). Normally, the knee axis angle has a narrow range, meaning even slight measurement errors can have a great impact on the reliability results. 9 This observation could explain the poor reliability estimates uncovered in the study. Furthermore, measuring joint range of motion can be influenced by various factors including pain or muscle stiffness. 16 We speculate if the lack of significant reliability observed during the reassessment of knee joint motion could potentially stem from genuine discrepancies in the range of motion between tests, as the assessment is considered simple but, in this case, difficult to reproduce.
The reliability estimates of foot width and length reached good and excellent levels in contrast to range of motion estimates that only reached moderate levels indicating that using a goniometer for assessing joint movement can pose challenges. Visual estimation of the anatomical reference lines may not correspond to the true bone orientation and thus the alignment of the goniometer is likely to introduce measurement error. Youdas et al. 17 reported that lack of reliability when measuring joint range of motion is mostly based on an erroneous determination of reference points by the examiner.
The agreement estimates for hallux valgus were acceptable according to the agreed-upon estimates, but only reached moderate levels of reliability. On the other hand, foot length reached excellent levels of reliability, but not acceptable agreement estimates. This demonstrates that an evaluation may gather substantial reliability evidence while being unsuitable for use in clinical settings and vice versa.
Agreement estimates for arch height, heel valgus and varus, and knee flexion showed more than 80% of the assessments within the agreed-upon estimates. In total, 4 out of 38 measurements demonstrated less than 50% of the assessments within the agreed-upon estimates despite complementing training and application of standardized procedures. Significant errors can happen during clinical evaluations even when experienced physiotherapists apply standardized measurement techniques. 18
Martin and McPoil 19 reviewed the reliability of ankle range of motion measurements. All included studies reported greater ICC reliability for ankle dorsiflexion (0.64–0.99) and plantarflexion (0.47–0.99) than in our study. However, retest measurements were assessed on the same day or a maximum of 7 days from the initial test measurements. Reliability may be improved by shorter test intervals because they can lessen the impact of outside variables or participant changes. In addition, shorter intervals could induce a risk of examiner bias, as the examiner may recall values from the original test when noting values for the retest. Geere et al. 20 reported that reliability declines as the time interval between tests and retests increases. Longer intervals between tests and retests may be necessary to evaluate stability over time and prevent examiners from remembering previous values. In our study, longer intervals were implemented to assess the reliability of manual measurements over time. As previously stated, all clinicians involved deemed that 5–6 weeks did not exert significant influence on the children’s development reasoning them as stable study subjects. This assumption was agreed upon before retest sessions were commenced.
Furthermore, the evaluation score applied for ICC interpretation in our study is stringent, resulting in lower levels of test–retest reliability compared to other studies. Sankar et al. 21 reported excellent intra-rater reliability for all assessments with ICC > 0.81 indicating that results were interpreted using lower values. Stringent interpretation scores reduce the likelihood of misleading conclusions and improve the quality and impact of findings.
With only four ninth graders in the population, the retests have a low spread, which could affect the reliability estimates. Reliability results are less affected by measurement error in more varied samples. Despite the more homogeneous population, the sample size was appropriate for the retest analysis since a sample of approximately 50 participants, in general, is necessary, to achieve reasonable precision in estimating reliability, which is obtained in the study. 1
This study’s strength is that the values used to estimate agreement are predetermined and unaffected by the analysis. These values should be established beforehand to aid in interpreting the agreement. However, predefined values for estimating agreement are rarely used. 22
Study limitations
There are certain limitations in this study. First and foremost, the team of pediatric orthopedic surgeons who determined the acceptable measurement errors in the agreement assessments were co-authors of this study. Second, podiatrists conducted hip measurements despite not being part of their standard practice. In addition, due to the study setup and limited financial resources, multiple assessments were conducted in a short time frame potentially affecting the reliability of the results compared to reducing the number of assessments per test. Furthermore, the measurement tools utilized in this study can contribute to measurement errors. Lastly, many variables included in this study can exhibit daily variation such as foot size based on standing activity and joint stiffness due to strenuous activities. 23
Conclusions
To measure the stability of manual clinical measurements, we examined test–retest reliability and agreement among 50 children from the PA.NI.C Feet project. We found that reliability measurements for foot length and width were categorized as excellent and good, the remaining were moderate (N = 18) and poor (N = 28). In addition, agreement estimates for hallux valgus were categorized as acceptable, the remaining were not acceptable. This means that precautions must be taken when comparing clinical evaluations on children’s feet with the results of the PA.NI.C Feet study and when evaluating children’s lower extremities for clinical and research purposes. Accordingly, clinical decision-making must not be based only on these quantitative measurements of children’s feet but must incorporate individual clinical and qualitative evaluations of each patient. Decision-making in treatment is usually not based solely on range of motion testing and clinical evaluation but is assisted by X-rays, gait analysis, and other tests. In conclusion, the variable reproducibility of the assessments presented in this article and the clinical measurements of children’s lower extremities pose challenges, particularly for non-experienced personnel. It is unknown whether pediatric orthopedic surgeons due to their experience can perform the assessments resulting in greater test–retest reliability outcomes. Although this is a compelling subject, subsequent studies should investigate this. While this study contributes valuable insights into the stability and reproducibility of clinical manual measurements, it also highlights the need for reliable and time-efficient tools to assist clinicians in assessing manual clinical measurements in pediatric lower extremity research and practice, and future research should explore this.
Supplemental Material
sj-docx-2-cho-10.1177_18632521251322639 – Supplemental material for Test–retest reliability of clinical measurements of lower extremity joint motion and alignment in the pediatric population
Supplemental material, sj-docx-2-cho-10.1177_18632521251322639 for Test–retest reliability of clinical measurements of lower extremity joint motion and alignment in the pediatric population by Thea Saabye, Thomas Colding-Rasmussen, Andreas Balslev-Clausen, Søren Bødtker, Christian Wong and Steen Harsted in Journal of Children’s Orthopaedics
Supplemental Material
sj-docx-3-cho-10.1177_18632521251322639 – Supplemental material for Test–retest reliability of clinical measurements of lower extremity joint motion and alignment in the pediatric population
Supplemental material, sj-docx-3-cho-10.1177_18632521251322639 for Test–retest reliability of clinical measurements of lower extremity joint motion and alignment in the pediatric population by Thea Saabye, Thomas Colding-Rasmussen, Andreas Balslev-Clausen, Søren Bødtker, Christian Wong and Steen Harsted in Journal of Children’s Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251322639 – Supplemental material for Test–retest reliability of clinical measurements of lower extremity joint motion and alignment in the pediatric population
Supplemental material, sj-pdf-1-cho-10.1177_18632521251322639 for Test–retest reliability of clinical measurements of lower extremity joint motion and alignment in the pediatric population by Thea Saabye, Thomas Colding-Rasmussen, Andreas Balslev-Clausen, Søren Bødtker, Christian Wong and Steen Harsted in Journal of Children’s Orthopaedics
Footnotes
Author contribution
TS: Data curation, Formal analysis, Investigation, Validation, Writing – original draft; TCR: Data curation, Formal analysis, Writing – original draft; ABC: Conceptualization, Methodology, Writing – review and editing; SB: Conceptualization, Methodology, Writing – review and editing; CW: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – review and editing; SH: Formal analysis, Methodology, Software, Validation, Visualization, Writing – review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Association of Danish Podiatrists; and the Novo Nordic Foundation’s pregraduate scholarships.
Ethical statement
This study was declared as a non-scientific study and thus not appropriate for evaluation for approval following the Danish Act on Research Studies (journal nr.: 21054014). Regional registration was obtained in accordance with the Danish Data Protection Agency as stipulated by Danish law J.nr. 2008-41-2240 and approved by the local review board (Privacy). The study adhered to relevant national guidelines and was carried out following the Declaration of Helsinki (JBJS 79A:1089-98,1997). Informed signed consents were obtained from all the participant’s legal guardians.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.