
Abstract
Objective:
This study examined test–retest relative (intraclass correlation coefficient) and absolute (minimum detectable change) reliabilities for heart rate, blood pressure, rate of perceived exertion, and the cerebral oxygen response during both forward and backward treadmill walking in clients with Parkinson disease. In addition, the intensity of exercise based on the individual’s heart rate response during forward and backward walking treadmill work was assessed.
Design:
Test–retest reliability study.
Subjects:
A total of 22 clients with Parkinson disease (Hoehn and Yahr stages 1–3).
Main measures:
Outcome measures of heart rate, blood pressure, and cerebral oxygen response were assessed during forward and backward walking on a treadmill for a total of 20 minutes up to an intensity based on the clients’ prior treadmill work and their rate of perceived exertion.
Results:
Good to excellent 6–8 day test–retest findings for both forward (intraclass correlation coefficient(2,1), 0.89–0.99) and backward (intraclass correlation coefficient(2,1), 0.82–0.99) treadmill walking were found for heart rate, blood pressure, cerebral oxygen response, and the participants’ rate of perceived exertion. Low minimum detectable change (MDC)95 values were found for heart rate (4.9 and 4.8), rate of perceived exertion (1.0 and 1.6), and cerebral oxygen response (1.2 and 0.92), during forward and backward walking, respectively. All treadmill exercise heart rates attained by participants were within an intensity of 54%–87% of the client’s predicted maximal heart rate.
Conclusion:
Treadmill exercise training can be included in Parkinson disease exercise programs with relative confidence in test–retest reliability of cardiovascular response. It was also demonstrated that individuals with Parkinson disease previously involved with exercise consistently self-select walking speeds which induce heart rates within recommended guidelines for positive cardiovascular adaptation.
Introduction
Parkinson disease (PD) is a progressive, multisystem neurodegenerative disorder that primarily affects dopaminergic neurons in the substantia nigra. Common clinical manifestations of PD are characterized by dysfunctional movements such as bradykinesia, gait hypokinesia, resting tremor, rigidity, muscle weakness, freezing of gait (FOG), postural instability, and increased risk of falls.1,2 One type of therapy that has been shown to be effective in improving movement-related disorders is exercise training often consisting of both forward walking (FW) and backward walking (BW). Prior research has shown increased gait impairment during BW compared to FW in individuals with PD. 3 Protas et al. 4 found that multidirectional gait and step training which included BW reduced falls and improved gait and balance. It has also been suggested that there are separate neural control mechanisms for FW compared to BW. 5 Based on the principle of specificity of training adaptations, BW treadmill training may better target the BW deficits and the specific neural control mechanisms. Additionally, increased endurance, improvement in independent ambulation, and reduction in the risk of falls have all been demonstrated following treadmill exercise training. 6 Several studies have shown that this type of exercise can also positively impact cognitive function through increases in brain-derived neurotropic factor (BDNF). 7 Moderate to vigorous intensity exercise has been reported to induce greater increases in BDNF than low intensity work. 8
The cardiovascular response to treadmill exercise in individuals with PD can be highly variable. 9 The variability appears to be most significant with higher intensity exercise and may be due to autonomic dysfunction, the effect of the client’s primary PD medication, or a combination of both.10,11 Because forward and backward treadmill training are used in exercise therapy for clients with PD, there is a need to establish the consistency of cardiovascular responses including heart rate (HR), blood pressure (BP), cerebral oxygen response (COR), and the rate of perceived exertion (RPE) for both efficacy and safety in these programs. The minimum detectable change (MDC)95 measures for these variables should be established to document true change versus measurement error related to therapeutic interventions. 12 Although the importance of monitoring HR and BP during exercise is understood by most clinicians, there is little information regarding COR during exercise in individuals with PD. Cerebral oxygenation typically demonstrates a slight increase during moderate to moderately vigorous exercise in healthy populations however; there is often a reduction in COR during very vigorous exercise. 13 There is little information on COR in individuals with PD during varying exercise intensities. If reductions in COR were to occur during exercise in the individual with PD, it could further impact balance, decision making, and overall cognitive function, posing a potential safety risk.14,15
The primary purpose of this study was to assess the test–retest reliability and MDC95 values for HR, BP, COR, and RPE in people with PD for both forward and backward treadmill exercise. Based on recent reports of the potential neuroprotective effects of higher intensity exercise, a secondary purpose was to determine whether these participants would self-select treadmill walking speeds that would increase their HR to a level that would be classified as moderate to vigorous intensity.
Method
Study design and study population
Seven females and 15 males (71.5 ± 8.5 years) with PD were recruited from local PD exercise groups. All participants were involved with both FW and BW treadmill training, one to two times per week for at least 6 months or longer prior to the study. Two separate 1hour sessions, 6–8 days apart at the same time of day, were conducted for both test–retest exercise trials with FW preceding BW both times. All testing was completed during the participant’s “on medication” period.
Co-existing medical conditions reported by the participants included cholesterol abnormalities 36% (8/22), elevated BP 32% (7/22), depression or anxiety 23% (5/22), a history of cardiac disease 18% (4/22), prostate problems 14% (3/22), and urinary incontinence 14% (3/22). On an individual basis, back pain, breast cancer, dizziness, gout, leg cramps, macular degeneration, osteoarthritis, pulmonary disease, shoulder pain, and stomach issues were also reported. Five of the participants were on medications that blunted their HR response to exercise. One participant had an implanted deep brain stimulator.
Inclusion criteria consisted of a medical diagnosis of PD and current involvement in an exercise program consisting of forward and backward treadmill walking. Exclusion criteria included any absolute contraindication for exercise testing according to guidelines from the American College of Cardiology (ACC) and the American Heart Association (AHA) or a non-ambulatory status. 16 Safety was maintained with the use of a gait belt during both treadmill conditions. Study procedures were approved by the University’s Institutional Review Board and all participants signed an informed consent prior to testing.
Arterial oxygen saturation (SpO2) was obtained using a finger pulse oximeter (Ohmeda Tuffsat, GE Healthcare, Finland), BP was assessed manually using a stethoscope and standard aneroid cuff, and RPE was obtained using a 1–10 scale from the Cleveland Clinic Heart and Vascular Health and Prevention Web site. 17
Testing procedures
Participant’s electrocardiograph (ECG) and HR were monitored by a computer-based stress testing system (Case, GE Medical, Milwaukee, WI). A continuous noninvasive arterial pressure (CNAP) monitor (CNAP monitor 500, CN Systems, Graz, Austria) was applied to the arm with the least amount of tremor to assess BP. A continuous wave near-infrared spectrometer (NIRS; Artinis Medical Systems BV, The Netherlands) was used to assess COR by measurement of oxygenated hemoglobin (HbO2) using two separate sensors secured to the forehead over the left and right prefrontal cortex.
Participants walked 10 minutes (min) both forward and backward at self-selected speeds determined from their previous treadmill exercise training. All participants had recent experience with this type of treadmill walking for approximately 10 min each direction twice per week either in a group exercise program or independently. An effort was made to allow the participants to work at their current level of exercise prescription while also trying to achieve a moderate to moderately hard intensity based on their RPE (4–6 on the 1–10 RPE scale). 17 Participants were allowed to hold onto the treadmill handrail with the arm not being used for BP assessment to help maintain balance. Heart rate, BP, SpO2, and RPE were recorded at rest and at 2 min intervals during both FW and BW. COR was recorded continuously during each 10 min walking trial. A 5 min rest occurred between the two walking trials to allow physiological responses to return to baseline. This protocol was repeated 6–8 days later for test–retest reliability.
Data analysis
The intraclass correlation coefficient ICC(2,1) was calculated for all treadmill exercise variables. 12 The MDC95 was calculated using the formula: [1.96 (SDbaseline) × √2(1 −ICC)]. 12
Test–retest reliability and MDC95 for HR, BP, and RPE were determined by comparing each 2 min interval measurement during the 10 min trials for both forward and backward treadmill walking. COR was determined by calculating the O2Hb change in micromoles per liter (µmol/L) from pre-exercise baseline to the last 5 min of steady-state exercise. Percent of HRmax was calculated using the steady-state HR from treadmill walking and then dividing that HR into the participant’s predicted maximal HR attained by subtracting 220 – their age. The exercise intensity was based on the classification scheme from guidelines recommended by the AHA and the American College of Sports Medicine (ACSM): light intensity 57%–63% HRmax, moderate intensity 64%–75% HRmax, and vigorous intensity 76%–95% HRmax. 18
Results
Hoehn and Yahr classificat ion ranged from 1 to 3 with primarily bilateral involvement. 19 There were no adverse events noted during either of the test–retest trials. The average levodopa dosage was 567 milligrams (mg) per day.
Hemodynamic response comparing the two treadmill sessions demonstrated good to excellent test–retest reliability ICC(2,1) for forward (HR = 0.99, systolic BP = 0.90, RPE = 0.89, COR = 0.92) and backward (HR = 0.99, systolic BP = 0.84, RPE = 0.82, COR = 0.92) walking (Table 1). Table 1 reports the mean and standard deviation as well as the MDC95 for the four treadmill test variables assessed during the two sessions. All steady-state HRs attained by participants during treadmill work were within 54%–87% HRmax. Four participants attained steady-state HR classified as vigorous during both FW and BW. An additional eight were classified as moderate intensity for FW while nine attained moderate intensity for BW (Table 2). All remaining individuals exercised at an intensity that would be classified as light intensity based on the AHA/ACSM %HRmax classification scheme. 18 Only 2 of the 22 participants self-selected walking speeds that were the same for both FW and BW exercise, and the remaining 20 participant’s BW was slower than for FW (FW 2.2 ± 0.9 vs BW 1.1 ± 0.5 mph).
Participant test–retest (6–8 days) and minimum detectable change (MDC)95 for forward walking (FW) and backward walking (BW) treadmill exercise variables (n = 22).

SD: standard deviation; ICC: intraclass correlation coefficient; HR: heart rate in beats per minute; SBP: systolic blood pressure in mmHg; RPE: rate of perceived exertion 1–10 scale; COR: cerebral oxygen response increase in O2Hb per liter.
Participant age, Hoehn and Yahr Class, and treadmill data during 10 minutes of forward and 10 minutes of backward exercise (n = 22).
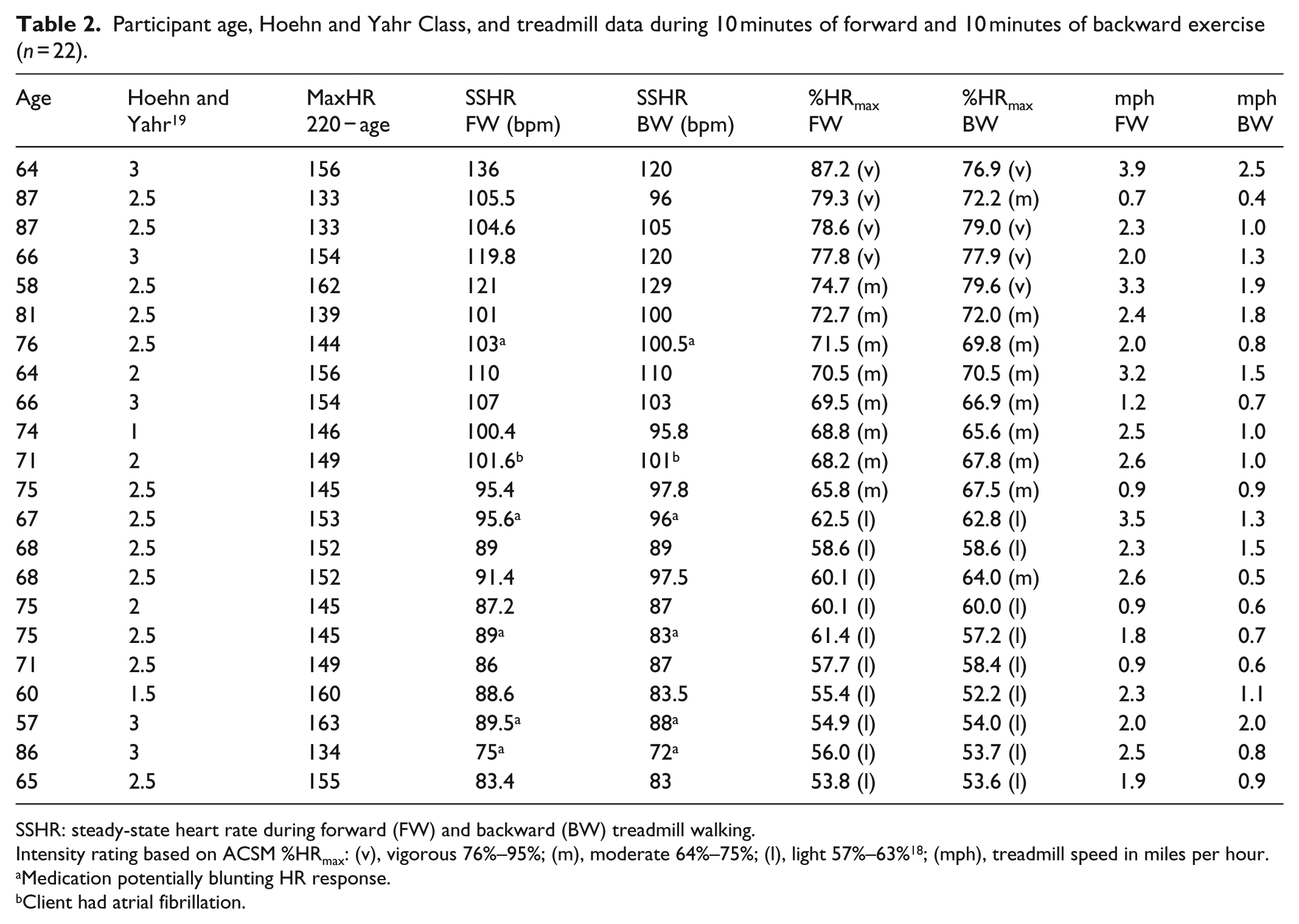
SSHR: steady-state heart rate during forward (FW) and backward (BW) treadmill walking.
Intensity rating based on ACSM %HRmax: (v), vigorous 76%–95%; (m), moderate 64%–75%; (l), light 57%–63% 18 ; (mph), treadmill speed in miles per hour.
Medication potentially blunting HR response.
Client had atrial fibrillation.
Discussion
The primary goal of this study was to determine whether cardiovascular measurements are consistent during both forward and backward treadmill walking under test–retest conditions and to establish MDC95 values for HR, BP, RPE, and COR, during steady-state exercise in people with PD. In addition, we sought to identify the intensity level of treadmill exercise when individuals with PD who were currently involved with an exercise training program were allowed to self-select their preferred walking speed.
Physical activity has become an important therapeutic intervention for those with PD, helping reduce complications of sedentary living, reducing symptoms, and assisting in the improvement of gait and balance. Treadmill training is the exercise modality most frequently employed with this population, as it is highly specific for day-to-day ambulation. Previous research has shown variable cardiovascular response to exercise in individuals with PD when compared to a healthy age-matched population 11 yet relatively consistent responses have been found when comparing on versus off medication periods. 10 This study compared the cardiovascular response including cerebral oxygenation to two separate steady-state treadmill exercise sessions with the timing of the PD medications being held constant (on medication). Treadmill exercise ICCs(2,1) were good to excellent for HR, systolic blood pressure (SBP), and RPE, and low MDC95 were found for HR and RPE (Table 1). The higher MDC95 value found for SBP may result from the large SD noted in this study (Table 1).
Self-selected treadmill speed by the participants was based either on their current treadmill training work or on their perception of effort (RPE scale). As noted previously, all but two participants walked at a slower speed backward compared to forward. This is not unusual, as it has been reported that at a given speed, FW treadmill work causes a greater cardiovascular stress than does BW. 20 For individuals with PD who may have greater gait impairment with BW, it is likely they would find it more tolerable to walk at a slower pace backward.
Even with the difference in the FW and BW speeds, all participants were able to complete their treadmill sessions with HRs that are within the target HR recommendations from the AHA/ACSM (50%–90% HRmax, Table 2). 18 According to the guidelines, 10 participants in this study would be considered to be exercising at a light intensity (57%–63% HRmax), 8 at a moderate intensity (64%–75% HRmax), and 4 at a vigorous intensity (76%–95% HRmax). Although all 22 were within the target HR recommendations, almost half would be considered to be exercising at light intensity. Two individuals whose HRs were classified as moderate intensity were taking medications that could blunt the rise in HR, while three classified as low intensity were on similar medications. Wonisch et al. 21 studied the effect of the beta-blocker Bisoprolol (5 mg/day) on the cardiovascular response to maximal exercise testing in 10 healthy male subjects utilizing a crossover design. They noted a mean 19 beats per minute (bpm) reduction in maximal HR when on the beta-blocker compared to the placebo. If a conservative 10–15 bpm reduction in maximal HR was applied to the individuals in this study who were taking medications that blunt HR response, there would have been a greater number of participants exercising in the moderate or vigorous classification. However, applying a specific numerical reduction in maximal HR when calculating HR-based exercise intensity using the 220 − age equation can be problematic as the individual response to medications can vary as can the dose and type of HR lowering medication.
Along with the five individuals on medications that likely blunted HR response, all participants were allowed to hold onto the handrail with their free hand. Holding onto the handrail while walking on a treadmill has been shown to reduce HR response and overall cardiopulmonary effort. 22 This may have been an additional factor causing HR’s to be slightly reduced during exercise and could have misclassified some individuals in the study to a lower intensity.
Whether encouragement to exercise at a higher intensity will generate greater overall benefits for those with PD is still being debated. However, recent research suggests that exercising at a higher intensity may incur greater improvements in symptom reduction and cognitive function in this population when compared to exercise at lower intensity.23,24 The ICC(2,1) for COR indicates excellent test–retest reliability for both forward and backward treadmill exercise (0.92 and 0.92, respectively, Table 1) with small MDC95 values at 1.24 and 0.92 for FW and BW, respectively. In addition, COR was stable or increased slightly during treadmill exercise which is a similar response seen in a healthy population during this type of exercise. 25 Previously, we reported a reduction in COR during two FOG episodes in a single client. 26 It is unknown if this atypical COR occurs with other individuals during their FOG episodes. In this study, no individuals demonstrated FOG, although one participant did experience a slight loss of balance that required stoppage of the treadmill for a little over 60 seconds. During this time, the participant remained standing and cerebral O2Hb dropped, but the participant did not report lightheadedness or any other symptom and his BP remained stable.
Study limitations include a small sample size, daily timing of the individual’s primary PD medication, day-to-day pathological variations of PD, upper extremity tremor, and no assessment of cognitive function. Generalizability of the results apply primarily to clients in Hoehn and Yahr Stage 2–3 (90% of the study population).
Conclusion
Treadmill exercise training can be included in PD exercise programs with relative confidence in test–retest reliability of HR/BP response during either FW or BW. Additionally, RPE appears to be a consistent indicator of self-reported training intensity demonstrating a low MDC95 value. Cerebral O2 changes during low to vigorous intensity treadmill walking demonstrate a similar response in individuals with PD as the response seen in healthy populations. Finally, individuals with PD, previously exposed to higher intensity exercise, appear to consistently self-select walking speeds which induce HRs within recommended guidelines for positive cardiovascular adaptations. In this study, over half of the clients self-selected an exercise intensity categorized as moderate or vigorous, indicating a tolerance and perhaps even a preference for higher intensity exercise.
Clinical Messages
Good to excellent test–retest reliability was found for forward (HR = 0.99, SBP = 0.90, RPE = 0.89, COR = 0.92) and backward (HR = 0.99, SBP = 0.84, RPE = 0.82, COR = 0.92) walking in clients with PD.
Low MDC95 values were found for HR (4.9 and 4.8), RPE (1.0 and 1.6), and COR (1.2 and 0.92), during FW and BW, respectively.
All treadmill exercise HRs attained were within an intensity of 54%–87% of the client’s predicted maximal HR, which is the approximate HR intensity range for cardiorespiratory fitness as recommended by the AHA/ACSM.
Footnotes
Acknowledgements
We would like to acknowledge Elizabeth Paly, PT, DPT, GCS, and students from the Concordia University Wisconsin class of 2014 and 2015 who assisted with data collection; Paul Wangerin for his assistance with statistical analysis; and all the clients who gave of their time to be involved in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Concordia University Wisconsin Institutional Review Board (IRB REFERENCE #: 13-7). SUBMISSION TYPE: New Project STUDY TITLE: [417093-1] Clinical significant change in functional tests and treadmill exercise in individuals with Parkinson disease.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.