
Abstract
Purpose:
The study aimed to compare the clinical and radiologic results of in situ pinning and modified Dunn procedure methods in stable–moderate slipped capital femoral epiphyses surgery.
Methods:
Slipped capital femoral epiphyses cases between January 2000 and December 2022 were retrospectively analyzed. Stable and moderate cases treated with in situ pinning or modified Dunn procedure and those with a follow-up period longer than 1 year were included. Two groups were formed: the in situ pinning group and the modified Dunn procedure group. Radiologically, postoperative alpha angle, Southwick angle, avascular necrosis, and osteoarthritis rates were compared. Clinically, Harris Hip Score and Merle d’Aubigné score were compared. Total complications were evaluated.
Results:
The in situ pinning group consisted of 28 patients and the modified Dunn procedure group consisted of 17 patients. The groups were similar in terms of age, gender, affected side, body mass index, Fahey/O’Brien Classification, preoperative slip angles, and follow-up time. Operation time was shorter in the in situ pinning group (p < 0.001). Postoperative Southwick and alpha angle were lower in the modified Dunn procedure group (p < 0.001). In clinical outcomes, Merle d’Aubigné and Harris Hip Score were higher in the in situ pinning group (p = 0.013, p = 0.005, respectively). The rate of avascular necrosis was higher in the modified Dunn procedure group (p = 0.048). There was no difference between the groups in terms of total complications and osteoarthritis.
Conclusions:
In situ pinning has an advantage over the modified Dunn procedure in the treatment of stable-moderate slipped capital femoral epiphyses due to shorter operative time, better clinical outcomes, and fewer avascular necrosis rates. Although Southwick and alpha angle measurements were found to be higher after in situ pinning compared to the modified Dunn procedure, this does not constitute a significant disadvantage in terms of osteoarthritis development in the mid-term.
Level of Evidence:
Level III, case–control study.
Introduction
Slipped capital femoral epiphyses (SCFE) is one of the most common hip problems in adolescence. A classification has been defined by Southwick 1 for SCFE as mild, moderate, and severe according to the slip angle. Loder et al. 2 classified the disease as stable or unstable according to the degree of weight bearing. These two classification systems are important in determining the treatment of the disease and predicting progression.
The two most commonly used methods in surgical treatment are the modified Dunn procedure (MDP) and in situ pinning (ISP) techniques. MDP is thought to be a technique that provides almost complete recovery in proximal femoral alignment, especially in unstable and moderate or severe cases, and thus prevents the development of femoro-acetabular impingement (FAI) and secondary osteoarthritis. 3 However, there is no consensus on whether it increases the possibility of disrupting the blood circulation of the femoral head.3,4 Poor functional results and the need for arthroplasty at an early age are known in patients who develop avascular necrosis (AVN) due to circulatory dysfunction of the femoral head. 4
There is no consensus on the choice of surgery in the treatment of the disease. 5 As a general opinion, in treating the disease, ISP is preferred in mild cases and MDP is preferred in moderate or severe cases. 6 In the literature review, it is seen that moderate and severe cases are evaluated together as well as stable and unstable cases.6,7 No study has been found that evaluates only “stable-moderate” cases. FAI, joint degeneration, and femoral head/neck deformities that may develop after ISP is applied in classical treatment are seen as disadvantages. In addition, it is claimed that satisfactory remodeling occurs in the femoral head and neck after ISP and that it does not cause symptoms in most early-stage cases. 8 As a result, it is not known whether a major surgery such as MDP is needed in stable–moderate cases.
The purpose of this study, specifically in the stable–moderate SCFE patient group, is to investigate the advantages and disadvantages of ISP and MDP procedures by comparing their radiological and clinical results and complications.
Materials and methods
Study design and patient selection
In this single-center, retrospective, case–control study, 126 cases who were operated on for SCFE in our clinic between January 2000 and December 2022 were examined. Radiological classification of the cases is based on anteroposterior and Lauenstein lateral radiograph; it was classified as mild, moderate, and severe as described by Southwick. 1 Loder et al. 2 classification system was used to evaluate clinically whether the fracture is stable or unstable. Fahey and O’Brien 9 classification system was used to determine the time of fracture onset as acute, chronic, or acute over chronic.
Criteria for inclusion in the study were as follows: being in the moderate group according to Southwick classification, stable slip according to Loder Classification, MDP or ISP technique was used in surgery, and the follow-up period was longer than 1 year. In the prior power analysis performed by choosing the expected power ratio = 0.90, the effect size was obtained as 0.652 and the minimum number of individuals to be included in the study was calculated as n = 34. Exclusion criteria were as follows: being in the mild (n = 34) or severe (n = 23) group, moderate/unstable slip (n = 11), follow-up period being less than 1 year (n = 9), and non-compliance with follow-up (n = 6). A total of 45 patients were included in the study. Among the cases that met the inclusion criteria, two groups were created: ISP Group (ISP-G) 28 patients and MDP Group (MDP-G) 17 patients.
Surgical technique
In our clinic, two different surgical techniques, ISP and MDP, are applied by four different experienced surgeons in the treatment of moderate–stable cases. The choice of surgical technique is left to the preference of the surgeon in charge. While two surgeons prefer ISP in stable-moderate SCFE, the other two prefer MDP.
MDP was performed by two experienced surgeons specialized in hip surgery according to the procedure described by Leunig (Figure 1). 10 ISP operation was achieved with single screw fixation, the effectiveness of which has been reported previously. 11 The ISP procedure was performed by two other experienced surgeons. Patients were transferred to the traction table. Traction, abduction, and internal rotation were applied to the table. Then a mini-incision was made and stabilization was achieved with a 6.5-mm cannulated screw (Figure 2).
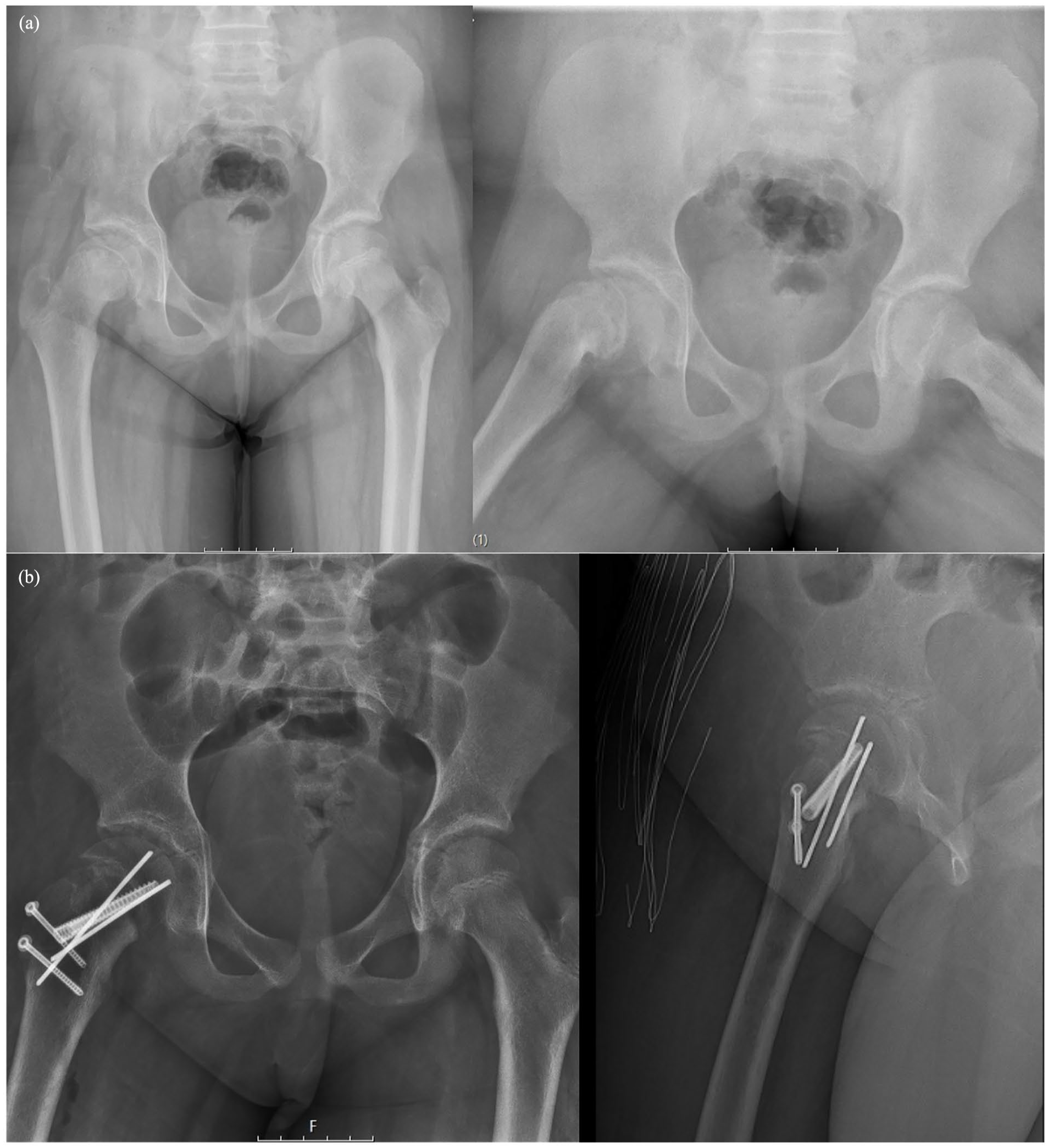
Preoperative (a) and postoperative (b) radiographs of the patient who underwent reduction and fixation with appropriate alignment by the modified Dunn procedure.
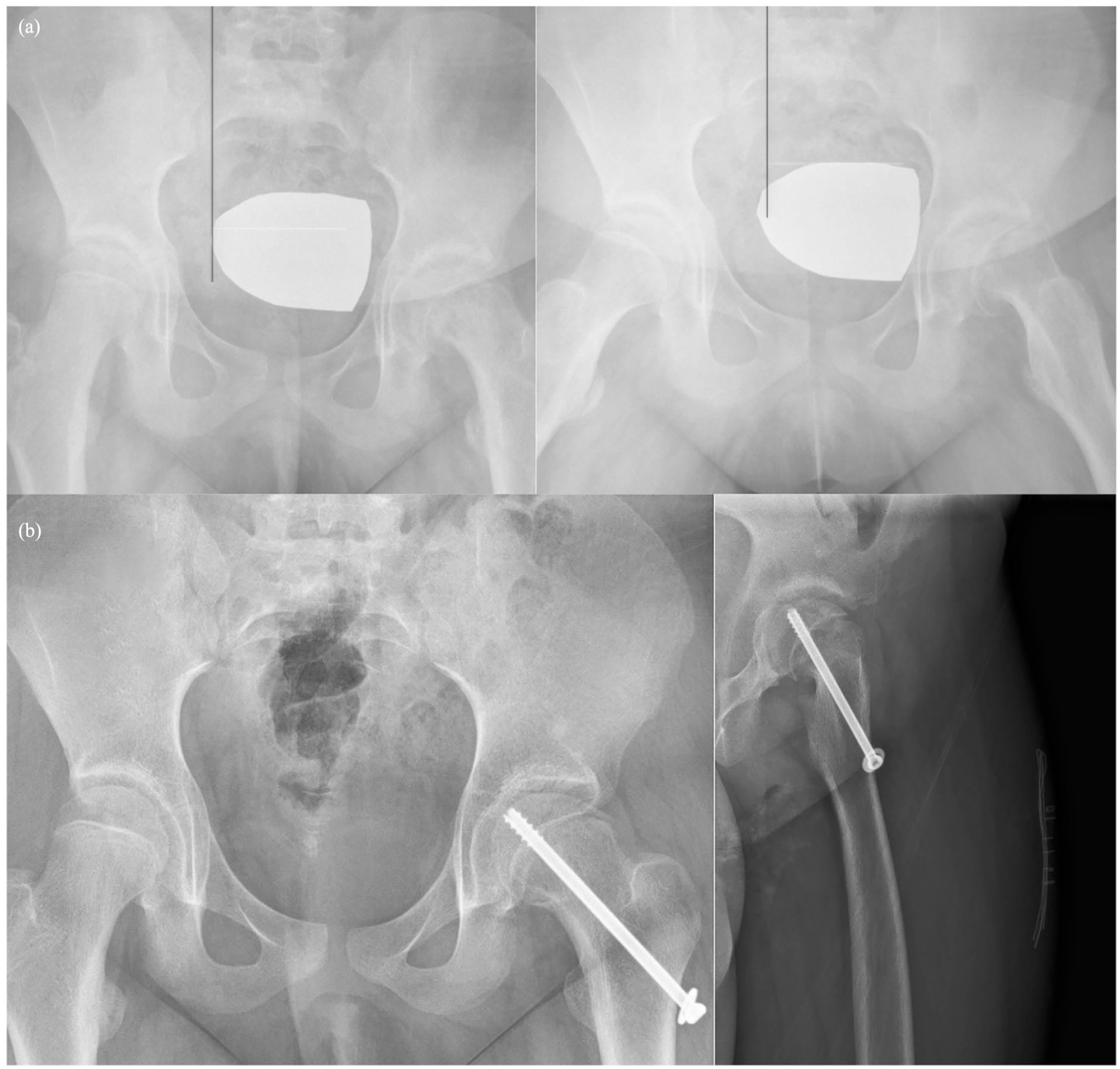
Preoperative (a) and postoperative (b) radiographs of the patient who underwent in situ pinning without reduction maneuver.
Follow-up after surgery
On the first postoperative day, hemogram tests were performed, direct radiographs were taken, and standard quadriceps and ankle exercises were started. On the second postoperative day, patients were mobilized without putting weight on the operated extremity. Patients were called for follow-up in the 1st, 2nd, 3rd, and 12th months after surgery. After that, they were invited for a yearly examination, and clinical and radiologic evaluations were performed. Mobilization with full weight bearing was allowed for the first month in the ISP surgery group, while mobilization with a full load was allowed in the MDP surgery group after the bone union was seen on radiographic images.
Clinical and radiological evaluation
The groups were compared intraoperatively in terms of surgery time. Radiologically, the postoperative alpha angle and postoperative Southwick angle were compared. All patients with suspected AVN were diagnosed using magnetic resonance imaging during follow-up visits. AVN was classified as described by Ficat. 12 Tönnis Classification of Hip Osteoarthritis13,14 was used to evaluate the development of osteoarthritis. Cases with at least stage I of the Tönnis classification were considered to have osteoarthritis (Tönnis-OA). Clinically, postoperative Merle d’Aubigné (MdA) score 15 and Harris Hip Score 16 (HHS) compared. Clinical results were evaluated at the last follow-up. Finally, total complications were compared between groups.
Statistical analysis
All analyses were performed in the SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0; IBM Corp., Armonk, NY, USA) package program. The distribution of quantitative variables was analyzed by the Shapiro–Wilk test. Independent groups were compared using the Mann–Whitney U test or independent samples t-test. The relationship between qualitative variables was investigated with chi-square analysis. Descriptive statistics of quantitative variables were shown as mean ± standard deviation or median (25th–75th percentiles). Descriptive statistics for qualitative variables were expressed as frequency (%). p < 0.05 values were considered statistically significant.
Results
ISP-G consisted of 28 patients and MDP-G consisted of 17 patients. The groups were similar in terms of age, gender, affected side, body mass index, and Fahey/O’Brien Classification (p = 0.230 p > 0.999 p = 0.719 p = 0.548 p = 0.924, respectively). The follow-up time ISP-G median was 6.7 years and MDP-G median was 6.5 years (p = 0.535) (Table 1).
Comparison of demographic characteristics of the groups.
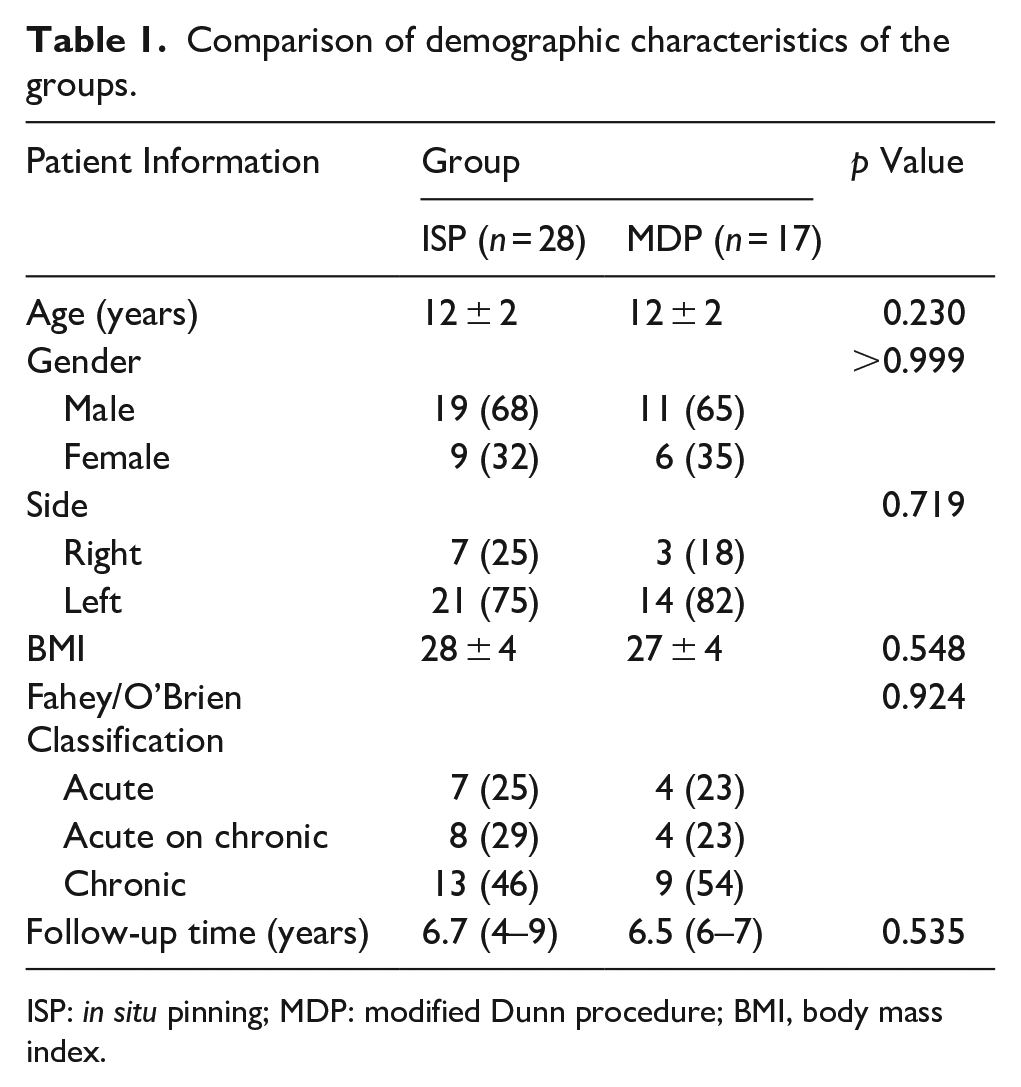
ISP: in situ pinning; MDP: modified Dunn procedure; BMI, body mass index.
Surgery time was shorter in ISP-G (p < 0.001). Proximal femur alignment became significantly more favorable with MDP-G compared to ISP-G. Postoperatively measured Southwick angle MDP-G was measured lower than ISP-G (p < 0.001). Postoperative alpha angle ISP-G was higher than MDP-G (p < 0.001). In the assessment of clinical outcomes, MdA and HHS were higher in the ISP-G (p = 0.013, p = 0.005). No difference was determined between the groups in terms of total complications and Tönnis-OA. The rate of AVN was higher in MDP-G (p = 0.048) (Table 2).
Comparison of clinical and radiological results of the groups.
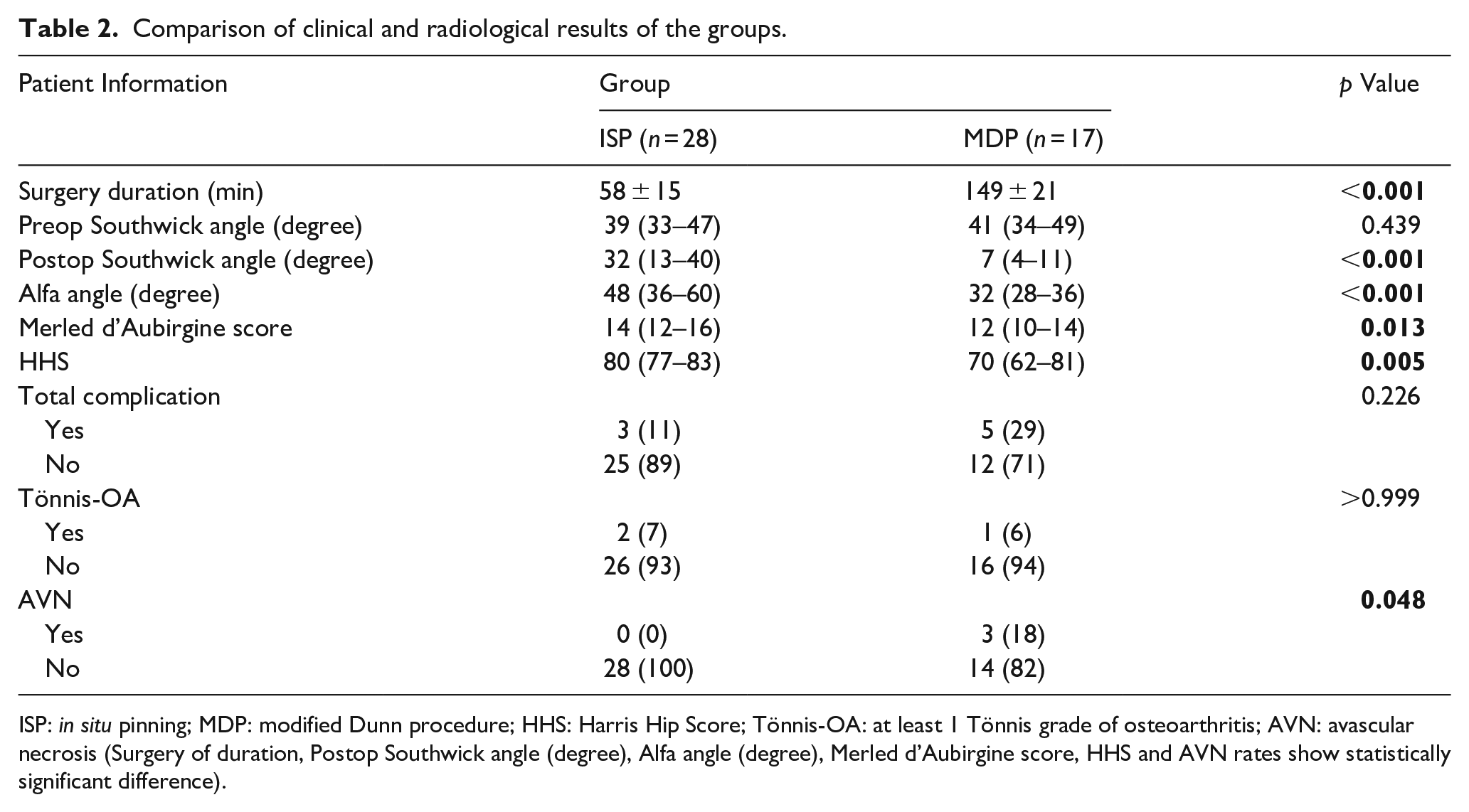
ISP: in situ pinning; MDP: modified Dunn procedure; HHS: Harris Hip Score; Tönnis-OA: at least 1 Tönnis grade of osteoarthritis; AVN: avascular necrosis (Surgery of duration, Postop Southwick angle (degree), Alfa angle (degree), Merled d’Aubirgine score, HHS and AVN rates show statistically significant difference).
MDP-G showed superficial infection in one case, while ISP-G did not show deep or superficial infection in any case. In MDP-G, AVN was determined in three cases, and in ISP-G, AVN was not seen in any case. There was a statistically significant difference between the 18% AVN rate in the MDP-G and the 0% AVN rate in the ISP-G. Two of the cases that developed AVN were determined at the 26th and 33rd weeks. The cases were in Ficat stage I and were followed up by giving NSAII. The third case in which AVN was determined was treated with total hip arthroplasty in 86 months due to the development of Ficat stage III AVN. Tönnis stage I osteoarthritis was determined in two cases in ISP-G and one case in MDP-G. Implant-related pain was determined in one case in each group. Implants that caused symptoms were removed with a secondary operation. No implant failure or non-union was determined in any case.
Discussion
Currently, SCFE treatment is a controversial issue in many aspects.17,18 In recent years, ISP has been thought to be the gold standard treatment method in SCFE cases. However, since anatomical reduction could not be achieved after ISP, the development of FAI and the risk of osteoarthritis led to the search for new treatment. 19 In 1964, the open reduction technique described by Dunn 20 was used for SCFE. However, due to the increase in the development of AVN, it was modified by Ganz et al. 21 in 2001 and claimed to reduce the risk of AVN.
There is no consensus on the selection of the surgical method according to the angle of slippage in the treatment of SCFE. It is theoretically possible to perform ISP regardless of the angle of epiphyseal slippage. In a long-term study of 21–47 years after diagnosis, Boyer et al. reported that the rates of chondrolysis and AVN were low in the ISP procedure performed without reduction and that it could even be applied in moderate and severe cases. 22 However, screw placement is difficult during practical application and the risk of complications after ISP in severe SCFE with a slip angle greater than 60° is increased. 17 In a study performed by Accadbled et al. 19 to determine the sliding angle at which ISP can be safely applied, the maximum sliding angle was found to be 35°. It has been reported that the risk of FAI development increases at varying rates if ISP is performed in cases above this degree of angle. DeVries et al. demonstrated that stable SCFE cases can achieve excellent mid-term results with ISP. 23 However, it has been reported that in severe cases, deformity surgery can be planned according to the development of FAI, and it is not necessary to correct the cam-type deformity that may develop prophylactically. 23 If left untreated, FAI can cause serious problems such as pain, labral tears, and arthritis. 24 However, it has been shown that the proximal femur can be remodeled as a result of compression between the femur and acetabulum. 25 There are findings showing that the MDP procedure is safer and more effective in the postoperative period in terms of FAI, and that proximal femoral anatomy can be achieved, thus reducing the need for secondary operations.26,27 The degrees of slip angle in our study were between 30° and 60°. Radiologic alpha angle measurements were higher in ISP-G patients. It is known that the increase in alpha angle is associated with FAI. However, according to our study, although there were higher alpha angles after ISP, no significant difference was determined between the groups in terms of osteoarthritis development in the mid-term.
The MDP approach in the treatment of SCFE is increasing in popularity. Many articles have been published in recent years about the results of SCFE cases in which MDP was applied.28 –30 Novais et al. 31 compared ISP and MDP in stable/severe SCFE cases and showed that MDP had higher clinical satisfaction and fewer reoperations and that MDP was superior in this respect. However, no difference was determined between the groups in terms of complications such as AVN and osteoarthritis. In the study by de Poorter et al. 32 involving the follow-up of mild and moderate SCFE hips after ISP operation, generally, good functional and radiologic results were demonstrated at an average follow-up of 18 years and there was no indication for open procedures in these hips. However, in severe SCFE, the results were found to be much worse, and open reduction was recommended. The study by Naseem et al. reported similar results; ISP was found to be successful in stable mild and moderate cases. 33 The study by Agashe et al. 28 with 30 patients who underwent MDP included 20 moderate, 10 severe, 19 stable, and 11 unstable patients. As a result of this study, successful clinical and radiological results after MDP were reported. They claimed that the MDP procedure should be the first choice in moderate and severe SCFE cases. In a similar study, Galletta et al. compared the results of ISP and MDP operations in stable moderate and severe SCFE cases; MDP was found to be superior in terms of deformity correction amount and clinical results. In this study, similar AVN rates were determined in the follow-ups after the two procedures. 6 However, there are highly variable rates of AVN reported after MDP surgery in the literature. 34 Passaplan et al. 30 evaluated 18 patients and found 14 stable, 4 unstable, 8 mild, 8 moderate, and 2 severe groups. In this study, it was reported that MDP had low rates of osteoarthritis and AVN. Masquijo et al. 29 evaluated 21 hips and found 6 hips to be stable. The average slip angle was determined as 59°. In this study, although most of the cases were in the stable group, a high number of AVN was determined in a total of 10 patients. However, as can be seen, there is still no consensus on the risk of AVN. In all of these studies, severe and moderate cases were evaluated together. In some articles, the mild group is even included. Our study is valuable in this respect. All cases are in the stable and moderate groups. While AVN was not observed in any cases in the ISP group, AVN was observed in three patients in the MDP group, which is statistically significant. This result indicates that MDP increases the risk of AVN in this selected group.
It is known that both the amount of slip angle and the stability of the fracture may change postoperative outcomes in SCFE treatment. There are very few studies in the literature evaluating MDP results in stable cases. In a study by Slongo et al. 3 including 23 patients, the mean preoperative slip angle was 47°, and 20 of the patients were stable. MDP was applied to all cases. AVN was determined in only one case and OA in two cases. They reported the clinical results as excellent. Huber et al. 35 evaluated 30 cases of SCFE and 27 cases were found to be stable. While 17 cases were in the moderate group, 10 cases were in the severe group. All cases were treated with MDP. As a result, AVN was determined in one case and it was emphasized that the clinical results were quite successful. In contrast to these studies, in the study claiming a higher rate of AVN after unstable shifts, this rate was reported to be 24% on average. 36 Zaltz et al. 36 reported that prospective studies are needed to ensure that the rate of unstable slips is high and that the cause of AVN may be surgical technique and iatrogenic injury. In our study, which consisted only of stable shifts, a significant level of AVN was observed after MDP, suggesting that MDP surgery increases the risk of AVN regardless of stability.
In conclusion, although only stable–moderate cases were preferred in this study, AVN was reported in 18% of those who underwent MDP. This rate is 0% in ISPs. This shows us that MDP surgery itself is an important risk factor for AVN. The choice of MDP should be reconsidered in terms of the development of disability at a young age and/or the need for secondary surgery. Better alignment was measured radiologically in patients who underwent MDP. However, these results did not cause a significant difference between the two groups in terms of late osteoarthritis development. ISP is also superior in clinical scores, in conclusion, due to shorter surgery time, better clinical results, and lower risk of AVN development. In stable/moderate SCFE cases, ISP preference is superior to MDP. In this regard, the ISP procedure can be safely performed by experienced orthopedic surgeons or pediatric orthopedic surgeons in the state hospital of the moderate/stable patient group, which is very common. Only severe and or severe/unstable slips would require referral to an often distant super-specialized hip center.
The most important limitation of our study is its retrospective design and limited case group. In future studies, we believe that prospectively designed studies of patients with SCFE treated with MDP and ISP with longer follow-up periods will be of value.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241295869 – Supplemental material for In situ pinning or modified Dunn procedure? Which one is superior in slipped capital femoral epiphysis surgery? A case–control study including only stable/moderate cases
Supplemental material, sj-pdf-1-cho-10.1177_18632521241295869 for In situ pinning or modified Dunn procedure? Which one is superior in slipped capital femoral epiphysis surgery? A case–control study including only stable/moderate cases by Ali Sisman, Caner Poyraz, Bilal Akbas, Mutlu Cobanoglu, Sevki Oner Savk and Emre Cullu in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance with ethical standards
All procedures performed involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Ethical statement
The study was initiated after receiving approval from the Non-invasive Clinical Research Ethics Committee (E-53043469-050.04-541962).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.