
Abstract
Purpose:
While children with hypermobility and/or ligamentous laxity due to coexisting connective tissue disorders might be expected to have worse outcomes after open reduction for hip dislocations, there is minimal prior research on this topic.
Methods:
All open reduction surgeries for hip dislocations performed at a single urban, tertiary-care children’s hospital from 2009 to 2023 were reviewed retrospectively. Those with connective tissue disorders secondary to a diagnosed syndrome or genetic disorder were included. Patients with <1 year of follow-up or hip instability in the setting of Trisomy 21 were excluded. Clinical and radiographic data was collected. Instances of re-dislocation, proximal femoral growth disturbance, residual acetabular dysplasia, and arthrofibrosis were recorded.
Results:
Twenty-three hips (15 patients) were included. Mean age at the time of surgery was 19.6 months (Range: 8.2–36.0 months), and mean follow-up was 4.3 years. The most common connective tissue disorder condition included was Ehlers-Danlos syndrome (13%). A majority of open reductions were performed via an anterior approach (96%). Seven hips (30%) underwent a concomitant pelvic osteotomy without femoral osteotomy and seven hips (30%) underwent both pelvic and femoral osteotomies. Twenty-two hips (96%) were International Hip Dysplasia Institute grade 1 at the final follow-up. Re-dislocation occurred in four hips (17%); eight hips (35%) demonstrated residual acetabular dysplasia, five hips (22%) demonstrated proximal femoral growth disturbance, and nine hips (39%) developed stiffness postoperatively.
Conclusions:
Patients with connective tissue disorders and ligamentous laxity have comparable rates of residual acetabular dysplasia, proximal femoral growth disturbance, and (surprisingly) stiffness as typical developmental dysplasia of the hip following open hip reduction surgery. Although the re-dislocation rate in the connective tissue disorders group was approximately 2–3 times higher, the difference did not reach statistical significance. Given that the study was limited by a low sample size, however, it is possible that the findings of no difference in residual acetabular dysplasia and proximal femoral growth disturbance were potentially due to a lack of power.
Level of evidence:
IV.
Introduction
Developmental dysplasia of the hip (DDH) includes a spectrum of hip pathology ranging from mild acetabular dysplasia to frank hip dislocation.1–4 Although estimates vary, the incidence of DDH in the US is thought to be approximately 1%, with females having a 2–4-fold increased risk over males.1–4
Increased tissue laxity might contribute to hip instability in the setting of DDH, and has been postulated as the causal link between female sex and DDH incidence.2,5 Tissue laxity may also account for the increased rates of DDH seen in patients with underlying syndromes associated with joint hypermobility (e.g., Ehlers-Danlos syndrome [EDS], Larsen syndrome, and Marfan syndrome), which have been reported to be as high as 4%.5,6
Despite this understanding, the influence of tissue laxity due to connective tissue disorders (CTD) on outcomes in the treatment of DDH is not completely clear. Sponseller et al. reported an incidence of 2% for DDH in a cohort of patients with Marfan syndrome (4 of 235), all of which were successfully treated with closed reduction alone. 7 Meanwhile, in one series of nine hips with EDS who underwent open reduction (OR) with or without femoral osteotomy for dislocated hips, 67% of hips re-dislocated. 8 Given the limitations of these small series and the fact that patients with CTD are commonly excluded from larger studies, the goal of this study was to report outcomes after OR for DDH in patients with underlying tissue laxity due to CTD at the authors’ institution.
Materials and methods
Study design and setting
After Institutional Review Board approval, all ORs performed for DDH at a single urban tertiary-care children’s hospital from 2009 to 2023 were identified using Current Procedural Terminology codes 27258, 27259, 27147, and 27156. For patients with subsequent bilateral ORs, each hip was analyzed independently. Patients were included if they had dislocated hips (defined as International Hip Dysplasia Institute [IHDI] grade II or higher) and had a diagnosed syndrome or genetic disorder associated with CTD causing tissue laxity. Hip ligamentous laxity was diagnosed in each patient by specialists (outside of orthopedics) based on clear clinical criteria and/or confirmatory genetic testing. Patients were excluded if they had <1 year follow-up, spastic or teratologic hip disease, or a history of ipsilateral hip surgery (Figure 1). Patients with Trisomy 21 were also excluded, as these patients may develop instability later in life and therefore they may represent a distinct clinical entity.
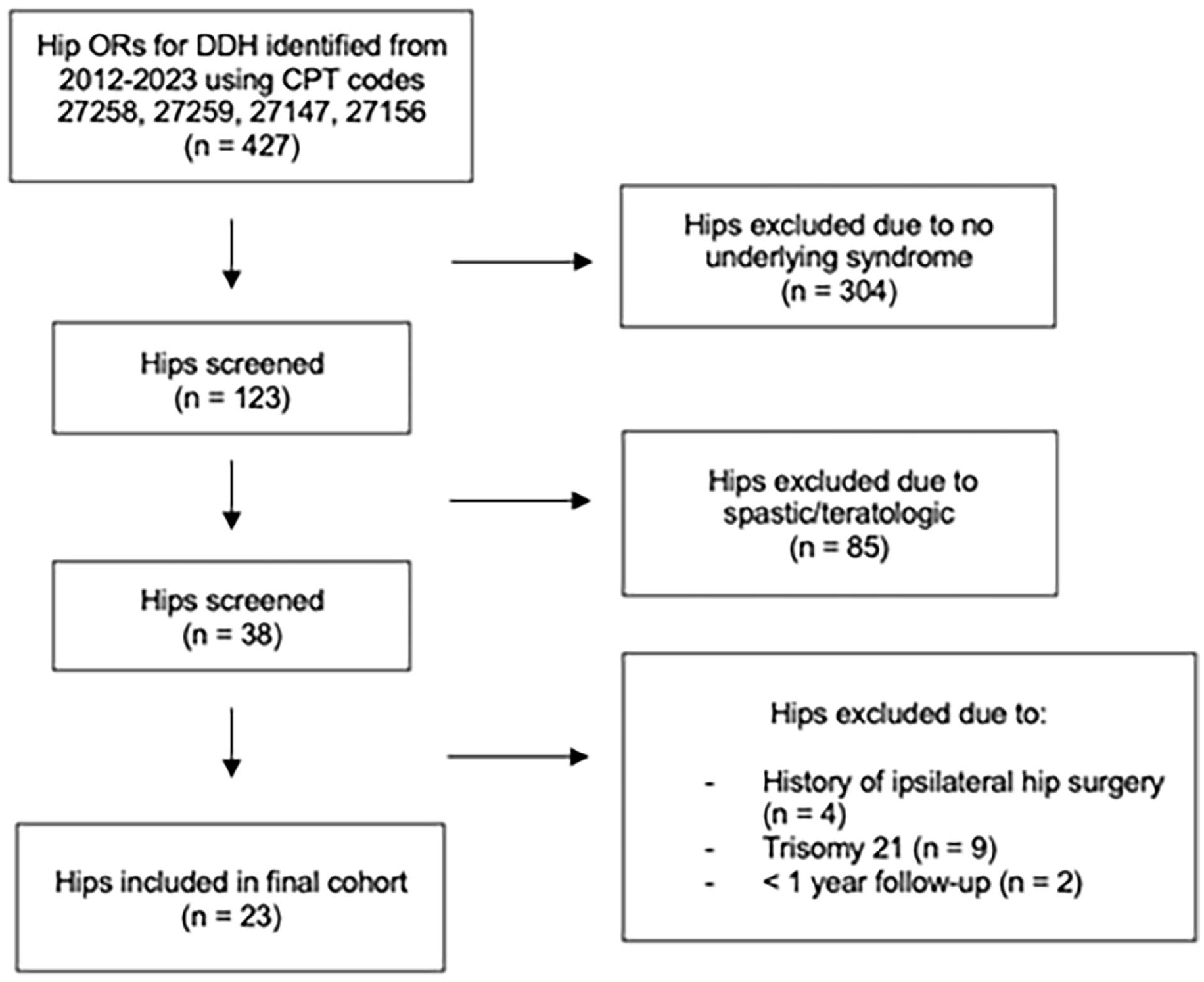
Flow chart of screening process for final patient cohort.
Data collection
Electronic medical records were reviewed to record patient demographics and preoperative clinical data (underlying diagnosis, laterality of the OR, history of brace usage, etc.). Of the 13 different diagnoses included in this study, 10 diagnoses were made objectively using genetics evaluation. Three were clinical diagnoses made by specialists without formal genetic testing. For example, all three patients with EDS were clinical diagnoses. Surgical data recorded included the approach used for OR and additional procedures, including pelvic osteotomy, femoral osteotomy, and adductor tenotomy. Postoperative data recorded included weeks in a hip spica cast after OR and the use of additional bracing. Preoperative anteroposterior (AP) radiographs were used to measure acetabular index and IHDI grade of dislocation. 9 Superior displacement was recorded as the distance from the highest point of the proximal femoral metaphysis to Hilgenreiner’s line, and lateral displacement was defined as the distance from the medial edge of the proximal femoral metaphysis to the lateral edge of the triradiate cartilage along Hilgenreiner’s line. 10 Both were normalized by pelvic width to control for age and x-ray magnification 10 (Figure 2). Intraoperative fluoroscopic images were assessed by the senior author for an inferior break in Shenton’s line which could indicate “over-reduction” or excessive pressure on the femoral head. Postoperative MRIs were used to measure the post-OR hip abduction angle while in the spica cast as described by Rivlin et al. 11
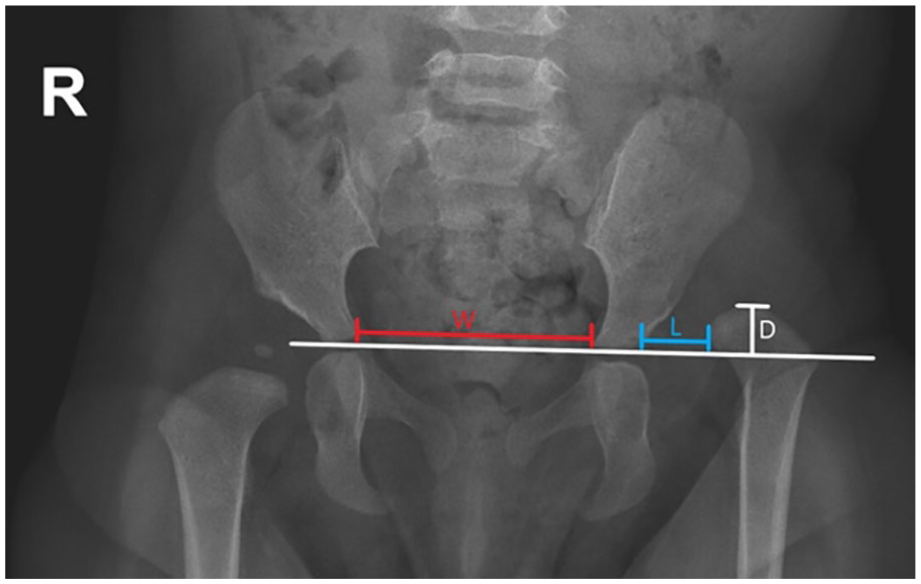
Superior displacement was defined as the perpendicular distance from the superior point of the proximal femoral metaphysis to Hilgenreiner’s line (D), normalized by the pelvic width (W). Lateral displacement was defined as the distance, along Hilgenreiner’s line, from the lateral edge of the triradiate cartilage to the medial edge of the proximal femoral metaphysis (L), normalized by pelvic width (W).
IHDI grade at the final follow-up was the primary outcome of interest. Four additional adverse outcomes were also investigated, including re-dislocation, proximal femoral growth disturbance (PFGD), residual acetabular dysplasia (RAD), and stiffness after OR. PFGD was classified by the senior author as yes/no based on Salter’s criteria using all available AP pelvic radiographs. 12 RAD was identified based on one of the two following criteria: the performance of a subsequent pelvic osteotomy for residual dysplasia or an acetabular index greater than the 90th percentile at the most recent follow-up (calculated using the normalization formula provided by Novais et al. 13 ). 14 Lastly, arthrofibrosis (stiffness) was identified based on electronic medical record documentation using previously described criteria. 17 Cases treated with premature bracing cessation and/or referral to PT for stiffness that resolved within 6 months postoperatively were categorized as mild stiffness. Cases that required more than 6 months of PT for persistent range of motion (ROM) concerns, manipulation under anesthesia, and/or inpatient rehabilitation admission were categorized as significant arthrofibrosis.
Statistical analysis
Descriptive statistics were tabulated. Clinical and radiographic variables were compared between hips with and without each of the four primary outcomes. Bivariate analysis was performed using Pearson’s Chi-squared tests, Fisher’s Exact tests for categorical variables, independent sample t-tests, and Mann-Whitney U tests for continuous variables. Statistical significance was set at p < 0.05. Statistical analysis was performed using JMP Pro v17.0.0 (SAS Institute, Cary, NC, USA).
Results
Baseline cohort characteristics
Twenty-three hips (15 patients) were included in the final cohort with a mean age at surgery of 19.6 months (Range: 8.2–36.0 months) (Table 1). The mean follow-up time for the cohort was 4.3 years (Range: 1.0–7.6 years). A majority of the hips in the cohort were left-sided (57%). Prior to OR, all hips had undergone some sort of reduction attempt: 19 hips (83%) were treated with a Pavlik harness, 12 hips (52%) were treated with an abduction orthosis, and five hips (22%) had undergone an attempted closed reduction in the operating room. Of the five hips that underwent attempted closed reduction, two cases were successful. Among the three cases that failed closed reduction, only one underwent OR immediately. Most hips were IHDI grade IV (61%) preoperatively, and the mean preoperative superior and lateral displacements of the hips were 19.1% and 34.6% of the pelvic width, respectively. The most common underlying diagnosis associated with CTD in the cohort was EDS (13%). Eight hips (42%) had an underlying chromosomal disorder (Table 2).
Summary of demographic and clinical characteristics of cohort.

Summary of underlying genetic or clinical syndromes presenting with joint hypermobility or ligamentous laxity.

Operative and postoperative management
A majority of the ORs were performed via an anterior approach (96%) (Table 3). Seven hips (30%) underwent a concurrent isolated pelvic osteotomy, seven hips (30%) underwent both a pelvic osteotomy and a femoral shortening osteotomy, and 17 hips (74%) underwent a concurrent adductor tenotomy. The decision for an additional pelvic osteotomy was made as per the surgeon’s preference based on a combination of the patient’s age and severity of dislocation. However, in general, pelvic osteotomies were routinely performed beyond 18 months of age. The decision for an additional femoral osteotomy was made intraoperatively based on tension observed during femoral head reduction. If the tension was deemed excessively tight, as per the senior surgeon, then a shortening osteotomy was performed. In addition, if femoral anteversion was thought to exceed approximately 50 degrees or if the version was thought to affect stability, then a derotation was performed.
Summary of operative and postoperative characteristics of cohort.

Of the 14 hips that underwent pelvic osteotomy, 11 (79%) were treated with a Dega acetabuloplasty, and three (21%) were treated with a Salter osteotomy. Intraoperatively, five hips (22%) had Shenton’s line broken inferiorly on fluoroscopy after reduction. Post-OR, hips were placed in a spica cast for a median of 6.4 weeks (IQR: 5.9–11.7 weeks).
Outcomes after OR
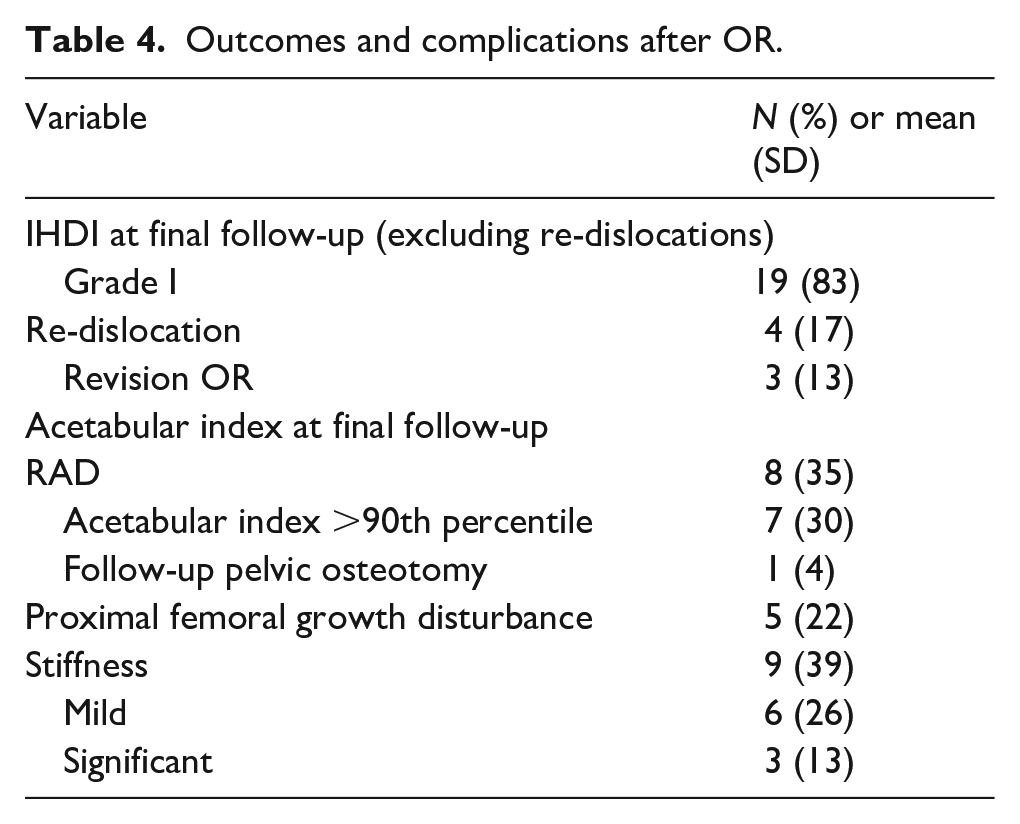
At most recent follow-up, re-dislocation had occurred in four hips (17%) (Table 4). Re-dislocation occurred at a mean of 2 months (Range: 0.83–3.1 months) post-OR. Three of these hips (13%) underwent successful revision OR, while one hip (4%) did not receive a revision OR due to parent preference and asymptomatic dislocation. The remaining 19 hips (83%) were all IHDI grade 1 at most recent follow-up. Figure 3 demonstrates an example case of a patient with EDS who successfully achieved a stable, concentric reduction after OR.
Outcomes and complications after OR.
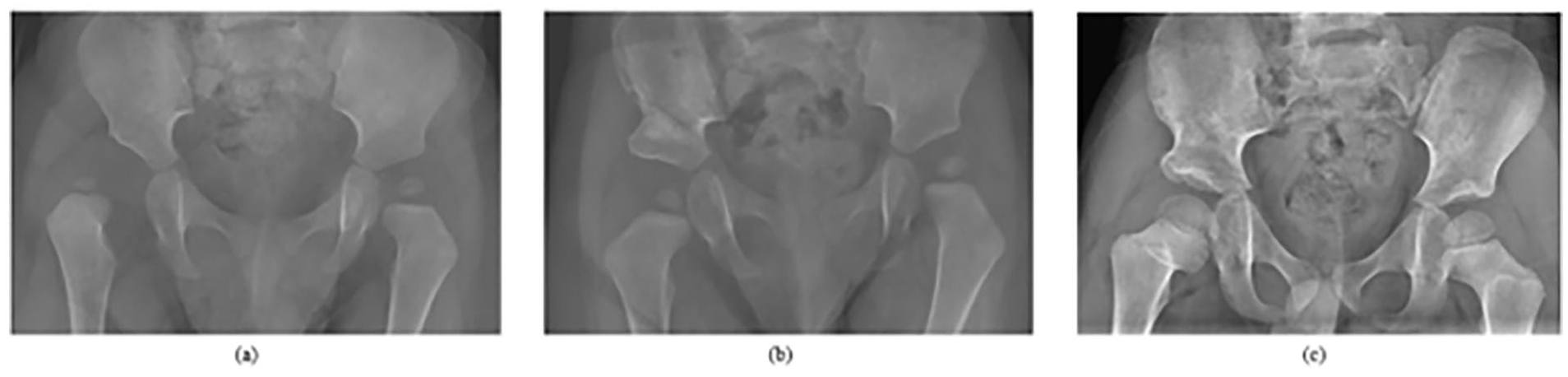
One-year-old male with a history of (a) right-sided hip dislocation in the setting of EDS. He underwent (b) OR and Dega acetabuloplasty. At his most recent follow-up (5 years post-op), he achieved (c) a stable, concentric right hip reduction.
Eight hips (35%) had RAD (one required a subsequent Salter osteotomy and seven had an acetabular index ≥90th percentile). Of the 14 hips that underwent concomitant pelvic osteotomy at the time of OR, four hips (29%) had RAD. In contrast, of the nine hips that were treated with isolated OR, four (44%) had RAD. Five hips (22%) demonstrated evidence of PFGD at most recent follow-up. Lastly, nine hips (39%) developed arthrofibrosis postoperatively: six hips (26%) developed mild stiffness, and three hips (13%) developed significant arthrofibrosis.
Bivariate analysis failed to show any difference in regard to demographic, clinical, or radiographic variables between patients who experienced and did not experience each of the four primary adverse outcomes (p > 0.05). Age at surgery was not significantly associated with re-dislocation (p = 0.37), RAD (p = 0.70), PFGD (p = 0.59), or stiffness (p = 0.38). Weeks of immobilization in post-op hip spica cast were similarly not significantly associated with re-dislocation (p = 0.14), RAD (p = 0.65), PFGD (p = 0.93), or stiffness (p = 0.47). Undergoing a prior attempted closed reduction was not associated with re-dislocation (p = 0.50), RAD (p = 0.28), PFGD (p = 1.00), or stiffness (p = 0.50). Neither the length of immobilization in a post-op hip spica cast (p = 0.47) nor the performance of an additional femoral osteotomy (p = 0.80) were associated with postoperative stiffness. Of the seven patients who underwent both pelvic and femoral osteotomies, three (43%) experienced postoperative stiffness. Of the seven patients who underwent isolated pelvic osteotomies, four (57%) experienced postoperative stiffness. Hips that underwent both femoral and pelvic osteotomies versus an isolated pelvic osteotomy did not have significant differences in re-dislocation (p = 0.19), RAD (p = 0.56), PFGD (p = 0.12), or stiffness (p = 1.00).
Discussion
Patients with joint hypermobility or ligamentous laxity due to CTD are reported to have a higher incidence of hip dislocations, but prior research detailing outcomes after OR for these patients is severely limited.5,6 The purpose of this study, therefore, was to describe the aggregate outcomes of OR for hip dislocations in patients with diagnosed CTDs. While 96% of hips in our series eventually achieved an IHDI grade 1, 13% required a revision OR due to re-dislocation, 35% of hips demonstrated RAD at most recent follow-up, 22% of hips developed PFGD, and 39% of hips developed arthrofibrosis. These findings help broaden our understanding of the outcomes of OR for hip dislocations in patients with underlying CTDs and may be useful in counseling families about postoperative expectations in this challenging patient population.
The current study found a 17% rate of re-dislocation among patients with tissue laxity due to CTD treated with OR for DDH, higher than the 7% rate of re-dislocation found in a multicenter study of non-syndromic hips. 14 Although the difference in re-dislocation rate between the multicenter study of non-syndromic hips and the current study did not reach statistical significance (p = 0.08), it is notable and confirms the prevailing notion that re-dislocation may be a greater risk after OR for DDH in those with underlying syndromes associated with ligamentous laxity. In the current study, approximately 53% of patients had bilateral hip dislocations. Each of the ORs for bilateral hip dislocations was performed via staged procedures. Although the multicenter study of non-syndromic hips by Kiani et al. did not report the percentage of their cohort that had bilateral hip dysplasia, they noted that bilateral hip dysplasia was not a significant risk factor for experiencing re-dislocation. We similarly surmise that bilateral hip dislocations likely did not influence the overall 17% re-dislocation rate in our cohort.
The current study also found that among those with CTD, there was a 35% rate of RAD and a 22% rate of PFGD after OR for DDH. In comparison, a multicenter study showed a 55% risk of RAD and 44% risk of PFGD in non-syndromic hips treated with OR for typical DDH. 14 Given the small numbers in this series, we do not think that our study truly indicates that the rates of PFGD and RAD are less in patients with CTD but rather that these complications occur in grossly similar frequencies to those of idiopathic DDH.
The results of this study highlight that although CTDs are often challenging conditions to manage, patients with CTDs who experience hip dislocations can still have satisfactory outcomes after undergoing OR. Almost 83% of our cohort did not experience re-dislocation after hip OR and maintained an IHDI grade 1 at most recent follow-up. Furthermore, the three re-dislocated hips that underwent revision OR did successfully maintain a stable reduction (i.e., IHDI grade 1). Thus, even with the challenging conditions included in this series, the IHDI outcomes after OR were reasonable in this patient population.
Few studies have previously investigated the outcomes of OR for hip dislocations in patients with underlying CTDs. Badelon et al. investigated dislocated hips that underwent OR in patients with EDS. Badelon et al. found that six of the nine hips (67%) with EDS treated with OR experienced re-dislocation after primary OR, and 22% of the hips developed new-onset avascular necrosis post-OR. 8 While their rate of PFGD was similar to the 16% rate of PFGD in the current study, the re-dislocation rate in Badelon et al. was notably higher. 8 Wada et al. 15 retrospectively analyzed seven dislocated hips with Kabuki Syndrome that were treated with OR. PFGD developed in 29% of hips post-OR, and 29% of the hips re-dislocated. 15 Matar et al. 16 reported a case of bilateral hip dislocations in a patient with Larsen syndrome and found that neither hip experienced re-dislocation throughout a 7 year follow-up after undergoing bilateral medial ORs.
Surprisingly, in spite of the underlying CTD, a significant percentage of our patients developed stiffness postoperatively. A recent study of 170 hips from our center, which utilized the same system for assessing postoperative stiffness, found a 36% rate of mild or significant stiffness following OR surgery in typical DDH. 17 In spite of the underlying ligamentous laxity, similar rates of stiffness were found in this series. As a result, our data suggests that an underlying CTD does not preclude the development of postoperative stiffness.
There are several limitations to the current study. First, the small sample size of the cohort—largely due to the uncommon nature of the conditions in this study—may limit the generalizability of findings. Because of this small sample size, the comparison between re-dislocation rates for this study compared to prior work by the senior author was likely underpowered, with post-hoc analysis showing that the current series would have needed >3 times the number of patients to achieve statistical significance for this comparison. Additionally, although our study found a PFGD rate of 22%, previous research has found that PFGD at 4 years post-op may be an underestimate of the true rate of growth disturbance due to the delayed appearance of type 2 avascular necrosis. 18 Thus, the prevalence of PFGD in our study (like most others on this topic) should be interpreted within the context of the length of follow-up. Second, although the patients included in this cohort had similar clinical presentations of DDH in the context of underlying ligamentous laxity, combining them together for study here might obscure differences in outcomes between the different syndromes and underlying diagnoses. Nonetheless, to our knowledge, this is the largest series investigating the outcomes of OR in DDH patients with underlying CTD. Third, given the retrospective nature of this study, the treatment indications and protocols were not standardized for each case. However, this was mitigated by the fact that each of these cases was performed by the same surgeon. Furthermore, another limitation of this study is that the single surgeon performing each OR may have unconsciously altered their surgical technique for patients with CTD in comparison to their technique for non-syndromic hips. Fourth, the single surgeon who performed each of the ORs in this series operates at a tertiary-care children’s hospital with a high volume of infantile DDH. Thus, the results of this study may not be generalizable to all practice settings. Lastly, this study primarily evaluates the most common complications of OR for DDH in the literature but does not capture the full spectrum of outcomes, complications, and patient-reported outcomes after OR. Despite these limitations, we believe that the findings of this study significantly expand the currently limited evidence on the outcomes of OR in DDH patients with underlying CTD.
Ultimately, in this series of patients with underlying CTD that underwent OR for DDH, 17% experienced re-dislocation, 35% experienced RAD, 22% developed PFGD, and 39% developed arthrofibrosis postoperatively. Ninety-six percent of hips eventually achieved a stable, concentric reduction (i.e., IHDI grade 1) at final follow-up. Hip dislocations in patients with underlying CTDs are complex to manage, and several factors go into decision making beyond clinical exams and radiographic parameters. Although it is often believed that patients with underlying CTD will have worse outcomes after OR, in our cohort, a vast majority were able to achieve a stable, concentric hip reduction at final follow-up. One of the limitations of this study was both the limited sample size of our cohort as well as limited follow-up until patients reached skeletal maturity. Future studies with larger enrollment could provide a direct comparison in outcomes between patients with CTD and those without. Larger studies might also elucidate any difference in outcomes between different syndromes associated with CTD and highlight any risk factors for complications in these patients. Furthermore, future studies could include 3D preoperative imaging to evaluate version and torsional differences in this unique patient population that may contribute to their outcomes after OR.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241287026 – Supplemental material for Outcomes of open reduction for hip dislocations in children with connective tissue disorders*
Supplemental material, sj-pdf-1-cho-10.1177_18632521241287026 for Outcomes of open reduction for hip dislocations in children with connective tissue disorders* by Vineet M Desai, Christopher J DeFrancesco, Stefano Cardin, Carter E Hall and Wudbhav N Sankar in Journal of Children’s Orthopaedics
Footnotes
Author contributions
V.M.D.: substantial contributions to conception and design, data acquisition, data analysis, data interpretation, article drafting, critical revision, and final approval of the version to be published; C.J.D.: substantial contributions to data acquisition, data analysis, data interpretation, article drafting, critical revision, and final approval of the version to be published; S.C.: substantial contributions to data acquisition, data analysis, data interpretation, article drafting, critical revision, and final approval of the version to be published; C.E.H.: substantial contributions to data acquisition, data analysis, data interpretation, article drafting, critical revision, and final approval of the version to be published; W.N.S.: substantial contributions to conception and design, data acquisition, data analysis, data interpretation, article drafting, critical revision, and final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: W.N.S. is a consultant for Lippincott Williams & Wilkins, Medivir, OrthoPediatrics, and Siemens Med Solutions USA, and a member of advisory board for The Pediatric Orthopaedic Society of North America.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study received Institutional Review Board approval.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.