
Abstract
Abstract
Purpose
Kabuki syndrome is characterized by distinctive facial features, skeletal anomalies, persisting fingertip pads with dermatoglyphic abnormalities, postnatal growth deficiency and mental retardation. This report reviews our results in the operative treatment of hip dislocations in patients with Kabuki syndrome.
Methods
Between 2001 and 2009, seven dislocated hips (three unilateral and two bilateral hips) in five patients (all girls) were operatively treated at our institution. The operative treatment consists of open reduction, femoral derotation varus osteotomy, pelvic osteotomy (Salter in one and incomplete periacetabular osteotomy in six hips) and capsular plication. The age of the patients at the time of surgery ranged from 2.4 to 5.7 years, with an average of 3.6 years.
Results
The follow-up postoperative period ranged from 3.2 to 6.3 years, with an average of 5.0 years. At the final follow-up, all patients reported no click and no pain, and showed well-contained hips by radiographs. All seven hips were graded as Severin class I-II. One patient presented as having habitual dislocation of the hip 4.4 years after surgery. Computed tomographic (CT) scans revealed posterior acetabular wall deficiency, which was not corrected by the anterolaterally directed Salter osteotomy. The incomplete periacetabular osteotomy provided sufficient posterolateral coverage of the acetabulum.
Conclusion
Operative treatment combining open reduction, femoral derotation varus and incomplete periacetabular osteotomies, and capsular plication provided successful results in patients with Kabuki syndrome who had the characteristics of hip instability such as ligamentous laxity, muscular hypotonia and posterior acetabular wall deficiency.
Introduction
Kabuki syndrome, originally known as Kabuki make-up syndrome and Niikawa-Kuroki syndrome, is a multiple malformation/mental retardation syndrome that was first described in Japan in 1981 [1, 2], but is now known to occur in many other ethnic groups [3–5]. To date, more than 350 cases have been identified in the literature, and disease incidence is estimated at 1/32,000 [6–8]. Kabuki syndrome is mostly sporadic, although some familial cases have been reported [9]. Inheritance is thought to be autosomal dominant or X-linked recessive [9].
The most distinctive feature is the peculiar facial appearance with long palpebral fissures, eversion of lower lateral eyelids, arched eyebrows, depressed nasal tip and prominent ears that are reminiscent of an actor's make-up in Kabuki, the traditional Japanese theatre [1]. The term “make-up” has been discarded from the name of the syndrome to prevent parental confusion and offense [3, 10]. Other specific features are mild to moderate mental retardation, skeletal anomalies, dermatoglyphic anomalies such as prominent fingertip pads, joint laxity and postnatal growth deficiency [1–8]. Cardiovascular defects, gastrointestinal and genitourinary tract anomalies, otologic and ophthalmologic abnormalities, seizures, endocrine anomalies and immunodeficiency have also been reported [1–8].
The skeletal anomalies first described in Kabuki syndrome were spinal abnormalities (butterfly vertebrae, sagittal cleft vertebrae and scoliosis), hand anomalies (cone-shaped epiphyses, brachydactyly and clinodactyly) and hip dislocation [1, 2]. More recently, pseudarthrosis of the clavicles [11], recurrent dislocation of the patella [12, 13], cleft hand [14], syndactyly [4], tarsal coalition [4] and congenital talipes equinovarus [15] have also been reported.
Hip dislocation in Kabuki syndrome is well recognized, with the incidence of hip dislocation reported to be 18–62 % [3–5, 16]. However, the literature on the management of hip dislocation is rare [16]. Although a sheltered living environment is needed, patients with Kabuki syndrome will achieve independent daily living and will live until their mid and perhaps late adult years in the absence of major visceral anomalies and immunodeficiency [3, 17]. The ambulatory and functional potential becomes poor without adequate treatment. The purpose of this study was to review our clinical and radiographic results in the treatment of hip dislocations with Kabuki syndrome.
Patients and methods
Between 2001 and 2009, seven dislocated hips in five patients (all girls) with Kabuki syndrome were treated at our institution. Kabuki syndrome is clinically diagnosed based on the recognition of its five main characteristics, which are distinct facial features, skeletal abnormalities, dermatoglyphic abnormalities, mild to moderate intellectual disability and postnatal short stature. The details of the five patients are shown in Table 1. There were three unilateral and two bilateral hip dislocations.
Patient data
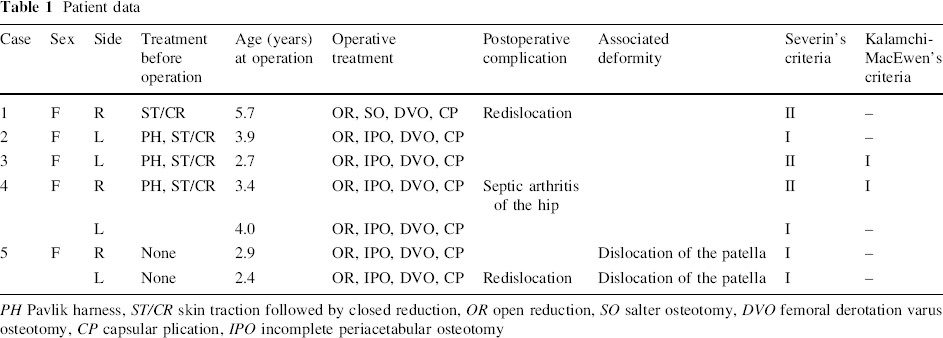
PH Pavlik harness, ST/CR skin traction followed by closed reduction, OR open reduction, SO salter osteotomy, DVO femoral derotation varus osteotomy, CP capsular plication, IPO incomplete periacetabular osteotomy
Two unilateral and one bilateral hip dislocations had been treated by a closed method with the use of a Pavlik harness at another institution (cases 2–4). The harness treatment failed in all four hips. The four hip dislocations (cases 2–4) and one unilateral hip dislocation (case 1) in a patient who visited us at age 10 months were successfully reduced by 4-week skin traction followed by closed reduction and 3-week plaster-cast immobilization. All five hips that received non-operative treatment were contained well and were stable before the patients began to walk; however, they were subluxated or dislocated after walking age, and subsequent surgery was required in the five hips. One patient with bilateral hip dislocations presented to us at age 2.1 years and was treated operatively at 2.4 years on the left hip and at 2.9 years on the right.
The operative treatment consists of open reduction, femoral derotation varus and pelvic osteotomies, and capsular plication. The age of the patients at the time of surgery ranged from 2.4 to 5.7 years, with an average of 3.6 years.
Open reduction was performed using Salter's modification of the anterior Smith-Peterson approach. The capsule was incised circumferentially adjacent to the acetabular rim. The rigid obstacles of thickening inverted limbus, the ligamentum teres and pulvinar (intra-articular fibrofatty tissue) were thoroughly removed for concentric reduction of the dislocated hip. The transverse acetabular ligament was also divided to decrease the pressure on the femoral head. A redundant portion of the capsule was excised, and plication of the anterior and superior capsule was completed.
Femoral derotation varus osteotomy was combined with open reduction in all seven hips to better achieve hip congruity and to reduce the risk of avascular necrosis. Pelvic osteotomy was also performed in all seven hips using the Salter technique [18] in the first hip and the incomplete periacetabular osteotomy in the latter six hips. We changed the technique of the pelvic osteotomy from a Salter osteotomy to the incomplete periacetabular osteotomy to prevent postoperative acetabular retroversion. The anterior supraacetabular region was preserved instead of being cut bicortically as in the previous reports [19, 20] to prevent anterior acetabulum from spreading (Fig. 1). The cut was extended posteriorly into the triradiate cartilage. All of the cuts involved the lateral cortex of the ilium only, whereas the medial cortex was left intact. Two bone grafts from the femoral osteotomy site and/or from the ilium were used to maintain the correction. The smaller one was placed laterally, and the larger one was placed posteriorly to provide posterolateral coverage of the acetabulum. A unilateral spica cast was applied for postoperative immobilization, with the hip slightly flexed in abduction and internal rotation. The cast was removed 5–6 weeks after surgery, and physical therapy was started. Full weight-bearing was allowed at 8 weeks after surgery.
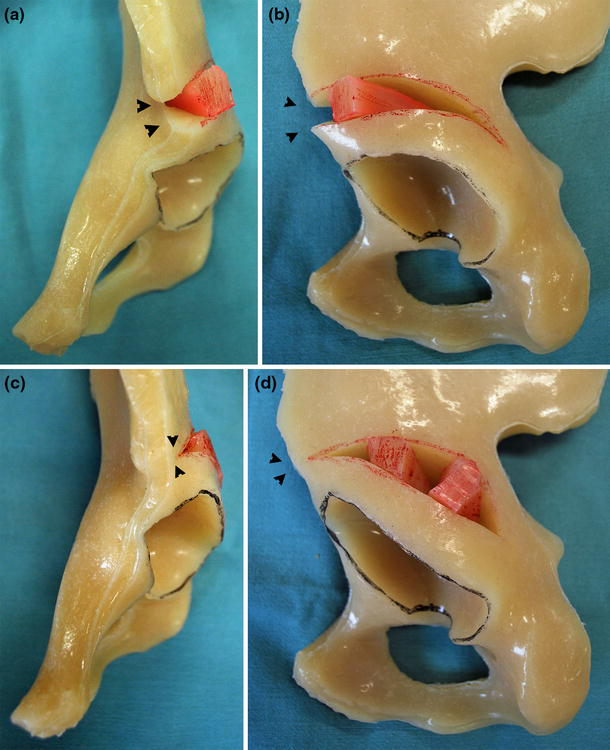
Two types of incomplete pericapsular osteotomy are shown. The curved osteotomy involved the lateral cortex only and extended to the triradiate cartilage, with the medial cortex left intact in both types of osteotomy.
We evaluated the results according to the criteria of Beguiristain et al. [21], which deem that the result is good when the patient has no click, no pain and a well-contained hip demonstrated by plain radiographs.
Radiographic results were classified according to the method of Severin [22]. The presence of avascular necrosis of the femoral head was graded according to the criteria of Kalamchi and MacEwen [23], as follows: group I, changes affecting the ossific nucleus; group II, lateral physeal damage; group III, central physeal damage; group IV, total damage to the femoral head and physis.
Results
The follow-up postoperative period ranged from 3.2 to 6.3 years, with an average of 5.0 years. At the final follow-up, the result was good in all seven hips. All patients reported no click and no pain, and showed well-contained hips by radiographs.
At the final follow-up, four hips were graded as Severin class I, and three hips were graded as Severin class II. Avascular necrosis was seen in two hips. The two hips were graded as Kalamchi and MacEwen group I.
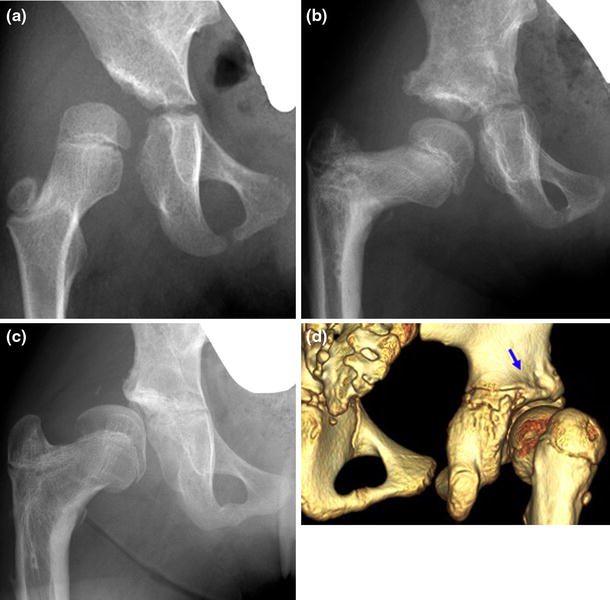
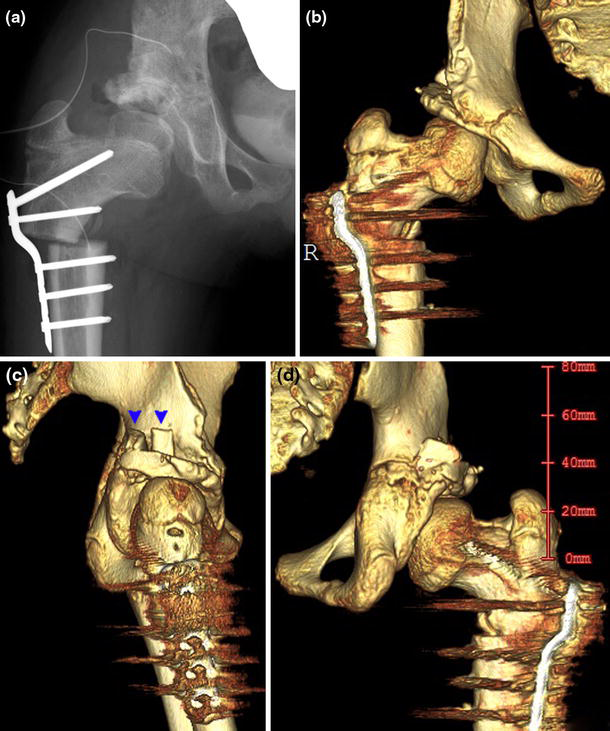
Two hips redislocated after surgery. One hip redislocated 6 weeks after the initial open reduction because of the decreased abduction and internal rotation in the spica cast. Open reduction and capsular plication were performed. The other hip presented as habitual dislocation at 10.1 years of age, 4.4 years after the initial open reduction (Fig. 2). Salter osteotomy was combined at the time of initial open reduction. The complaints noted by the parents were occasional limp and a sensation of clicking in the hip. On physical examination, the hip was reproducibly dislocated posteriorly with adduction and flexion, and reduced with abduction and extension. The habitual dislocation developed to a fixed dislocation, and the occasional limp progressed to a severe limp. Despite the appearance of adequate coverage of the acetabulum laterally following the Salter osteotomy by radiographs, three-dimensional CT scans revealed a marked deficiency of the posterior wall of the acetabulum (Fig. 2d). Open reduction was performed at 11.1 years of age in combination with femoral varus and the incomplete periacetabular osteotomies and capsular placation (Figs. 3, 4).
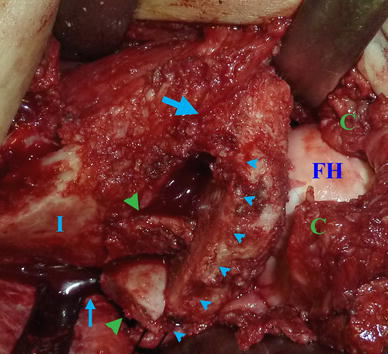
Intraoperative photograph of case 1 showing exposure of the ilium (I) to the sciatic notch. A retractor is placed in the sciatic notch (small arrow). The femoral head (FH), joint capsule (C) and osteotomy site (small arrowheads) are visible. Note that the anterior supraacetabular region (large arrow) is not cut, and the medial cortex is left intact. The bone grafts (large arrowheads) from the ilium are placed posteriorly and laterally to provide posterolateral coverage of the acetabulum
Postoperative radiograph (
One patient developed septic arthritis of the hip 4 months after surgery and was treated successfully, with surgical debridement and intravenous antibiotics.
One patient who presented to us at 2.1 years of age had toeing-out gait and genu valgus. Ultrasonography and magnetic resonance (MR) imaging were performed to obtain a diagnosis of bilateral dislocation of the patella and preoperative evaluation. The bilateral patella dislocations were treated operatively by means of lateral release, medial plication and medial transfer of the lateral patellar tendon.
Discussion
Kabuki syndrome is clinically diagnosed in our series, but the recent exome sequencing identified the mixed lineage leukemia 2 (MLL2) gene mutations responsible for Kabuki syndrome [24]. MLL2 gene mutations were found in 81 out of 110 families (74 %) with Kabuki syndrome [25]. A significantly greater number of MLL2 gene mutation-positive cases presented with short stature and renal anomalies than did MLL2 gene mutation-negative cases [25]. Use of whole exome sequencing in MLL2 gene mutation-negative cases will likely prove genetic heterogeneity in Kabuki syndrome in the near future [25].
The incidence of hip dislocation with Kabuki syndrome was reported to be 18–62 % [3–5, 16], but hip dysplasia had a lower incidence (12 %) in the neonatal period [26], which shows it is caused by congenital and developmental factors [16].
Ligamentous laxity and muscle hypotrophy are the major pathologic factors in dislocations with Kabuki syndrome. This condition is similar to the other conditions with ligamentous laxity such as Down syndrome. The incidence of dislocations with Down syndrome occurring between walking age and adolescence was reported to range between 1.3 and 7.0 % [27]. Untreated hips were found to develop to fixed subluxation, dislocation, progressive dysplasia with difficulty in walking and often painful osteoarthritis [27].
In our patients with Kabuki syndrome, closed reduction failed at the time when patients started to walk because of ligamentous laxity, and thus subsequent open reduction was necessary. Open reduction should be performed at the time of initial reduction. Open reduction was performed in combination with femoral derotation varus and pelvic osteotomies and capsular plication to achieve stable hip reduction.
Woolf and Gross [27] reported another factor of dislocation, posterior acetabular wall deficiency, in patients with Down syndrome. Salter and Pemberton osteotomies have been useful in managing dysplastic acetabula by providing additional anterolateral support over the femoral head. However, unlike the dysplastic acetabulum in developmental dysplasia of the hip, the deficiency of the acetabulum related to neuromuscular disorders, Down syndrome and Kabuki syndrome was more posterior and required an alternative to the Salter or Pemberton osteotomy. The incomplete periacetabular osteotomy provided sufficient posterolateral coverage of the acetabulum. To provide sufficient posterolateral coverage of the acetabulum, we modified the incomplete periacetabular osteotomy described before [19, 20] (Fig. 1): (1) The anterior supraacetabular region was preserved instead of being cut bicortically as in the previous reports [19, 20], thus preventing anterior acetabulum from spreading; (2) bone grafts from the femoral osteotomy site and/or from the ilium were placed posteriorly and laterally to provide posterolateral coverage of the acetabulum.
One patient developed septic arthritis of the hip 4 months after surgery. This was probably due to the increased susceptibility to infection in patients with Kabuki syndrome.
Toeing-out gait and genu valgus were present in one patient. Ultrasonography confirmed the diagnosis of bilateral dislocation of the patella. Diagnosis of dislocation of the patella could be delayed because of the low suspicion of the disease, few complaints from the mentally retarded patients and, because the patella ossifies between 3 and 5 years of age, the invisibility of patellae on radiographs [28]. Orthopedists should be aware of this possible complication. Previous authors have reported successful results using the Elmslie–Trillat procedure [12] or tibial tuberosity transfer [13]. Early diagnosis was obtained in our patient, and the bilateral patella dislocations were treated by lateral release, medial plication and medial transfer of the lateral patellar tendon with good results.
At the final follow-up, all patients reported no click and no pain, and all seven hips were graded as fulfilling the Severin class I-II criteria. Although long-term follow-up is necessary, operative treatment combining open reduction, femoral derotation varus and the incomplete periacetabular osteotomies, and capsular plication provided successful results in patients with Kabuki syndrome who have the characteristics of hip instability and posterior acetabular wall deficiency.
Footnotes
None.
Acknowledgments
None of the authors received financial support for this study.