
Abstract
Purpose:
The purpose of this study is to retrospectively analyze children treated conservatively in our hospital to explore the clinical characteristics of children with traumatic atlantoaxial joint infra-anterior dislocation complicating odontoid fracture and the therapeutic effects of treatment.
Methods:
Patients with atlantoaxial joint infra-anterior dislocation complicating odontoid fracture received conservative treatment, which comprised three steps: cervical traction (2 weeks), plaster fixation (2 months), and brace fixation (3 months).
Results:
We treated three patients (boy:girl = 0:3, mean age = 2.5 years old) from 2017 to 2020, the diagnoses were all traumatic C1-2 infra-anterior dislocations associated with odontoid fracture (Anderson and D’Alonzo classification type II: three cases, Hosalkar type IB: two case and IC: one case), with or without cervical spinal cord injury. The C1-2 infra-anterior dislocations were all successfully reduced by gentle traction with the halo method (case 1) or occipital-jaw (cases 2 and 3) for a mean of 18.3 days (19, 15, 21 days), after which the Calot plaster vests (head–neck–chest plaster vests) were fitted and maintained for 2 months, without operation. Braces were maintained for 3 months after the Calot plaster vests were removed. All patients achieved fracture healing and recovered from the spinal injury.
Conclusion:
In young children, atlantoaxial joint infra-anterior dislocation complicating odontoid fracture usually occurred at the odontoid synchondrosis and belonged to Anderson and D’Alonzo classification type II or Hosalkar type I. Conservative treatment achieved good results (dislocation reduction, bone healing, recovery of neurological symptoms).
Level of evidence:
Level IV case series.
Introduction
Traumatic atlantoaxial joint infra-anterior dislocation with odontoid fracture (ADOF) is very rare, especially in children. Upper cervical fractures and dislocations are often the result of high-energy trauma and are associated with significant mortality.1 –4 Many children with severe ADOF die immediately as a result of the injury, and some die later if they are not diagnosed in time. Even if the injury is found in time, because the children are too young, many hospitals are not equipped to carry out surgical treatment, nor can they perform correct conservative treatment of ADOF, which often leads to adverse consequences such as paralysis and even death at a later date. There have been few reports describing ADOF associated with contiguous or non-contiguous cervical spinal cord injury.5 –8
Management algorithms that work for adults often are not suitable for children, and diagnosis, appropriate treatment, and nursing can pose significant challenges. 2 Most trauma centers may only treat one case successfully in many years, and obtaining more appropriate treatment experience is difficult. Experience of successful ADOF diagnosis, conservative treatment, and nursing is very scarce. Routine advice on the treatment of ADOF is urgently needed. Here, we report three cases of traumatic ADOF (Anderson and D’Alonzo classification 9 and Hosalkar Classification 10 ) in very young patients with or without neurological deficit in our hospital.
This study aimed to review our treatment experience and explore the characteristics of ADOF in children to provide useful information for timely and correct conservative treatment of ADOF.
Methods
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the institutional ethics board of our hospital. Since the participants were children (<18 years old), written informed consent was obtained from their parents to participate in the study. The patients’ parents agreed to publish this study that includes information or images that could lead to identification of the patients, and the patients’ parents signed the informed consent for publication of identifying information/images in an online open-access publication.
We searched the orthopedic database at our hospital for patients with a diagnosis of ADOF who had undergone conservative treatment between 2017 and 2021. Patient demographics, diagnoses, causes, duration from injury to transfer to our hospital, pre-treatment symptoms, traction type, traction period, Calot plaster vest (head–neck–chest plaster vest) and head–neck–chest brace period, post-conservative treatment symptoms, and complications were recorded. Radiographs and computed tomography (CT) images were reviewed to determine the atlantoaxial joint infra-anterior dislocation and odontoid fracture. Magnetic resonance images (MRIs) were reviewed to determine the presence of signal cord changes for spinal cord injury. Post-treatment radiographs or CT scans were reviewed to determine union.
The conservative treatment comprised three steps (Figure 1):
First, cervical traction. Occipital-jaw traction was gently applied. If occipital-jaw traction fails, skeletal traction (using a halo frame) will be applied under bedside sedation and local anesthesia. The traction weight ranged from 1/10 to 1/7 of the patient’s body weight, and traction was maintained for about 2 weeks.11 –13
Second, plaster vest fixation. Under general anesthesia, a Calot plaster vest (head–neck–chest plaster vest) was fixed after X-rays confirmed the reduction of ADOF and maintained for about 2 months.
Third, brace fixation. When X-rays and CT scans confirmed that the fracture had healed, 14 the Calot plaster was removed and replaced by a head–neck–chest brace for about 3 months to protect from neck reinjury.
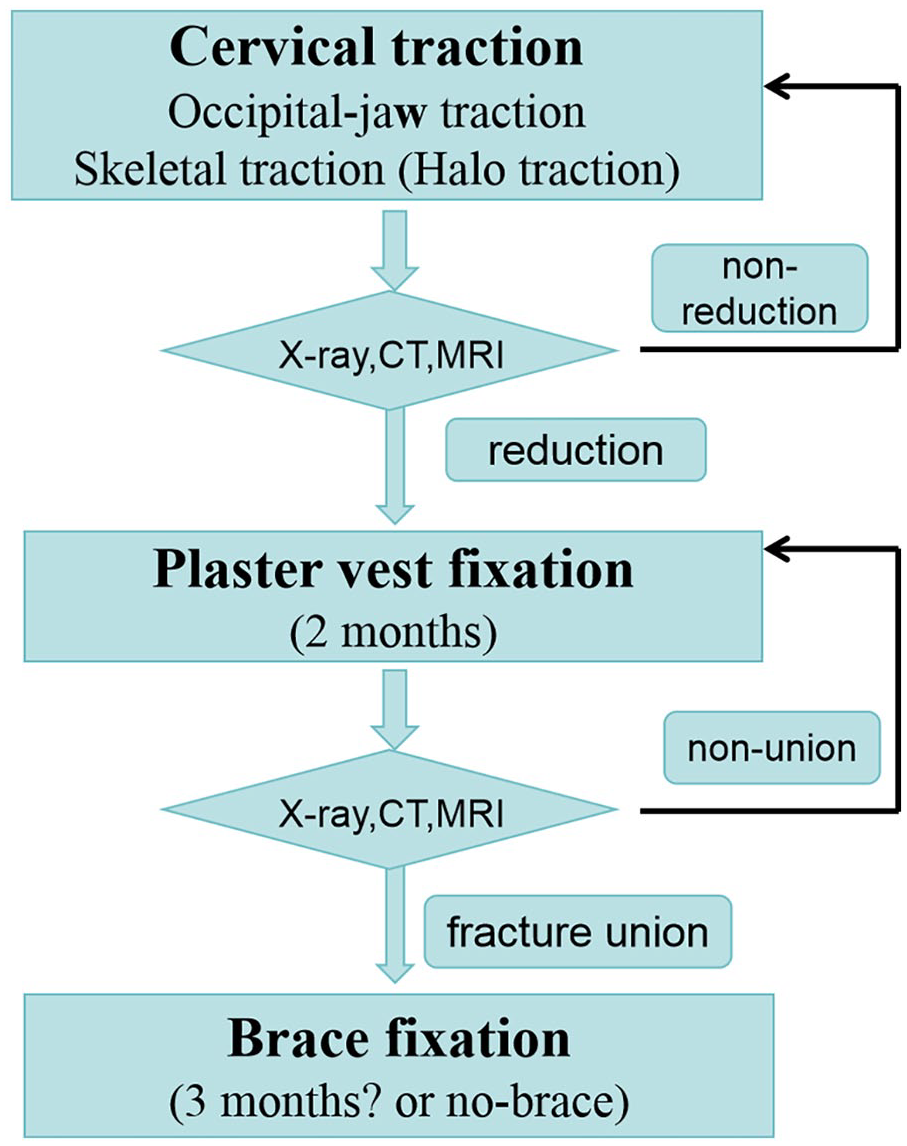
Treatment flow chart.
Results
Three children (all girls) with ADOF received conservative treatment. The mean follow-up was 36 months (range = 23–61 months). The mean age at initial treatment was 2.5 years old (range = 2.2–2.7 years). The mean time interval between injury and onset of orthopedic treatment was 5.3 days (range = 3–10 days). All the fractures occurred at the base of the epistropheus odontoid process, all belonging to the Anderson and D’Alonzo Classification Type II, with case 1 belonging to Hosalkar Type IC, and cases 2 and 3 belonging to Hosalkar Type IB. Traction type included one use of halo traction and two instances of occipital-jaw traction. The mean traction period was 18.3 days (range = 15–21 days). The Calot plaster vests were maintained for 2 months, and head–neck–chest braces were maintained for 3 months. There were no complications during the treatment. One patient with right hemiplegia had recovered well 1 year later. Painless and unrestricted active range of motion (ROM) of the C-spine and bony consolidation were observed in all patients.
Case 1
This was a 2.2-year-old girl who was being held by an adult in the passenger seat when two cars collided, and she suffered neck injuries in the road traffic incident. Immediately, the girl was found in an obtunded and moaning state with no movement in the right limbs; myodynamia of the right upper limb was grade 0 and that of the lower limb was grade 0. Immediately, the child was sent to a hospital nearby. CT showed no abnormalities, and an MRI was not performed because sedation was unavailable. Five hours after the accident, the child’s consciousness gradually turned clear, stimulating crying upset. After the neurologist’s consultation, considering the possibility of cervical spinal cord injury, steroid (methylprednisolone) shock therapy (30 mg/kg/15 min, 5.4 mg/kg/23 h) was given to reduce spinal cord edema.
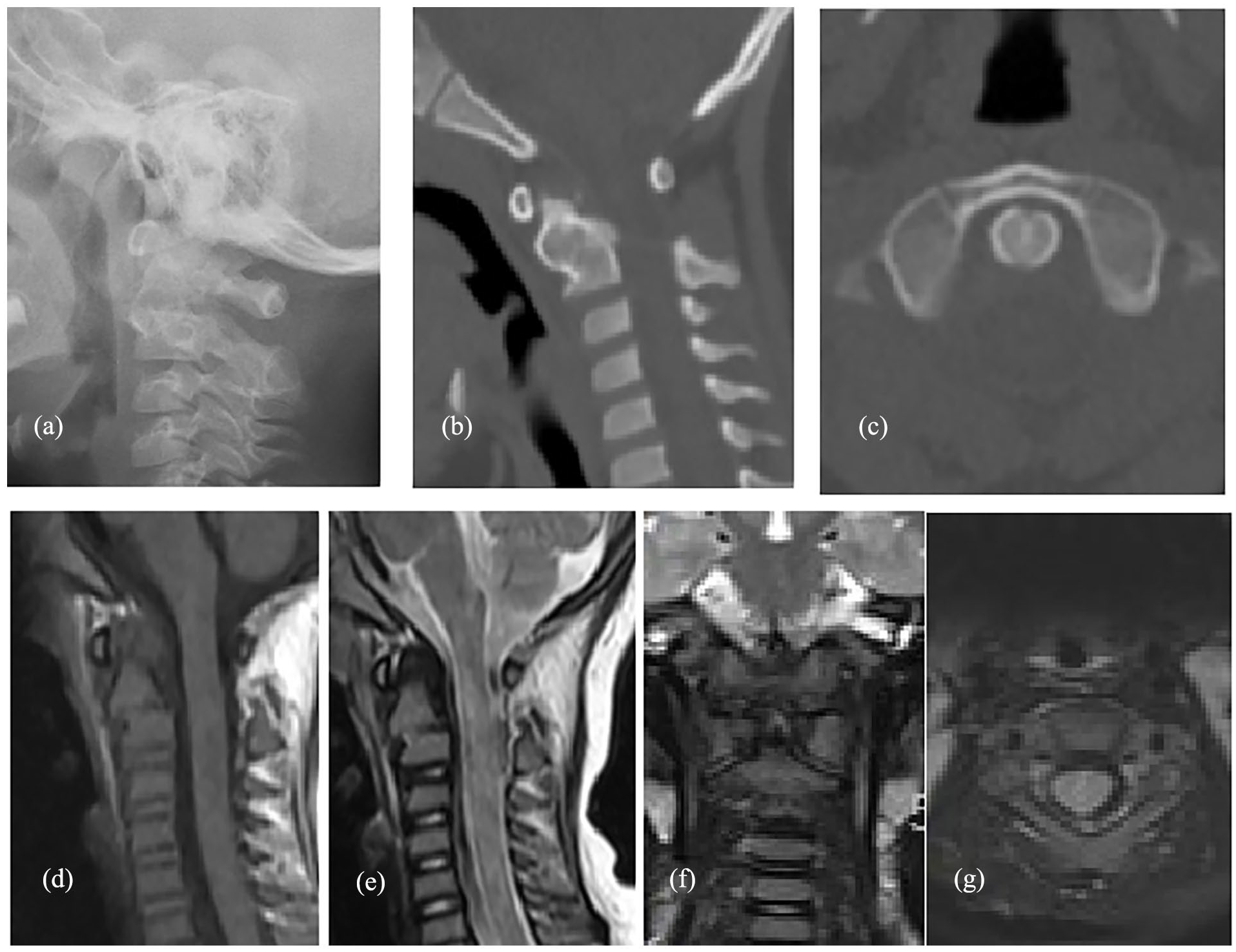
Three days later, the patient was transferred to our hospital. In our hospital, an X-ray examination suggested that the relationship between the odontoid and the position of the vertebral body was abnormal and suggested odontoid fracture. CT scans 7 and MRI confirmed C1-2 dislocation and odontoid fracture, and the MRIs also showed that the odontoid and atlas were displaced forward and upward, the broken end was close to the anterior edge of the cervical spinal cord, and the local subarachnoid space was narrowed (Figure 2). Muscle tension of the right upper and lower limbs was normal (Ashworth Score 0); in contrast, myodynamia of the right upper limb was grade 0 and that of the lower limb was grade II. Because of the patient’s young age, it is impossible to complete all the physical examinations, for example, the patient’s right limb’s sensation cannot be checked. In our hospital, the patient was given methylprednisolone therapy for 5 days (2 mg/kg/24 h).
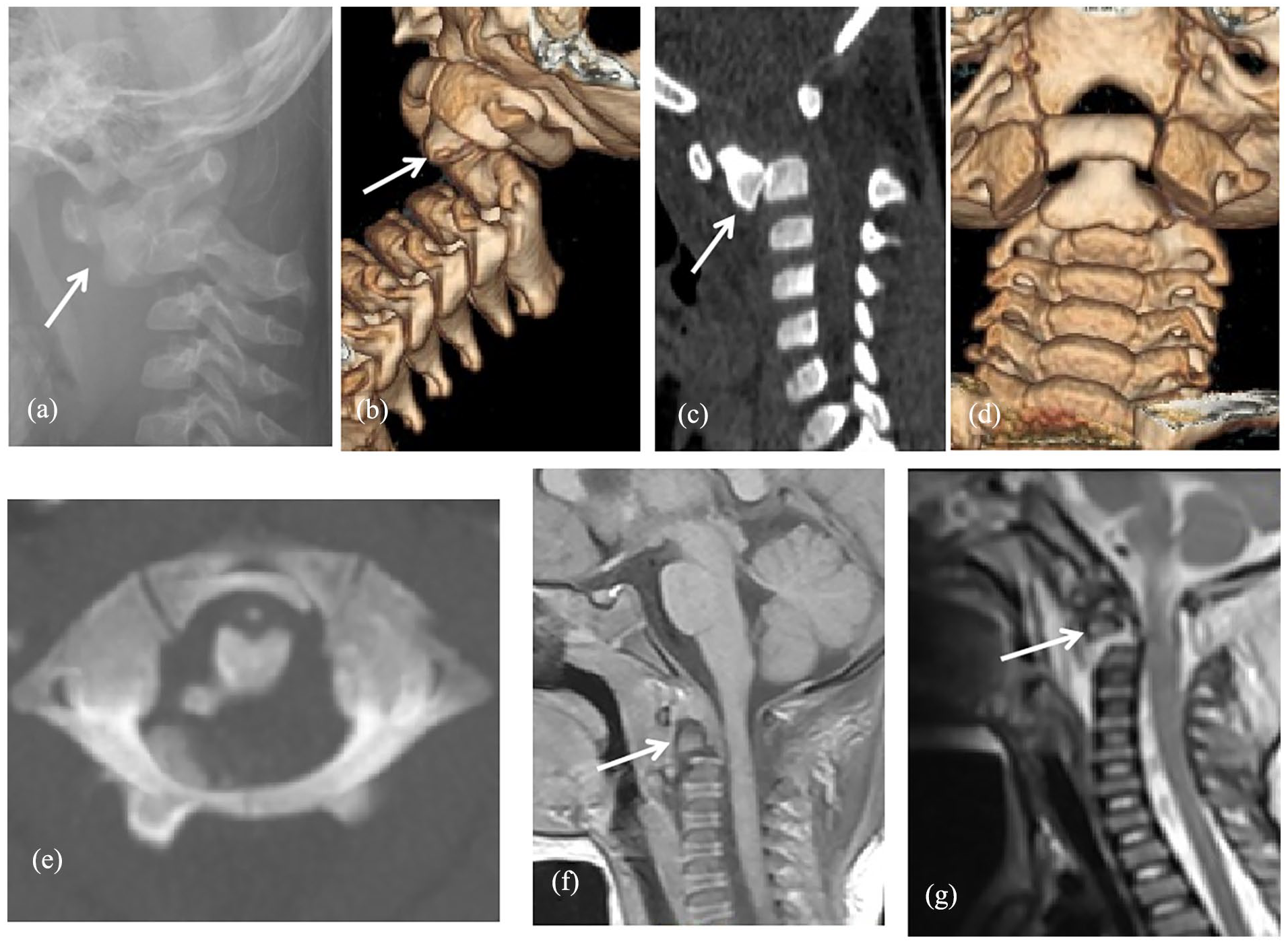
Case 1: A 2.2-year-old girl with ADOF (Anderson and D’Alonzo classification type II, Hosalkar Type IC). (a) Lateral radiograph (a) showing an atlantoaxial joint infra-anterior dislocation of C1 on C2 with infra-anterior displacement of the proximal fragment of the odontoid (white arrow; type II fracture of Anderson and D’Alonzo classification). (b–g) CT scans, (b–e) MRI images, and (f and g) showing infra-anterior dislocation of C1 on C2 (white arrows) with odontoid fracture of Anderson and D’Alonzo classification type II and Hosalkar Classification type IC.
At first, occipital-jaw traction was applied with 1.5 kg (nearly 1/10 of the patient’s body weight) as the traction weight. Three days later, the lateral radiography showed non-reduction of C1-2 infra-anterior dislocation with odontoid fracture. Skeletal traction was gently applied using a halo frame under bedside sedation and local anesthesia instead of occipital-jaw traction. Two kilograms (1/7 of the patient’s body weight) were used as the initial traction weight, and this was maintained. After 3 days, X-rays showed that reduction of the traumatic C1-2 dislocation and odontoid fracture had been successfully achieved (Figure 3). However, the distance between the cervical vertebrae was too large after reduction, so we gradually reduced the traction weight to 1/10 of the body weight, and subsequent radiography indicated good spacing and stable reduction. Ten days after Halo traction, myodynamia of the right upper limb was grade II and that of the lower limb was grade II.
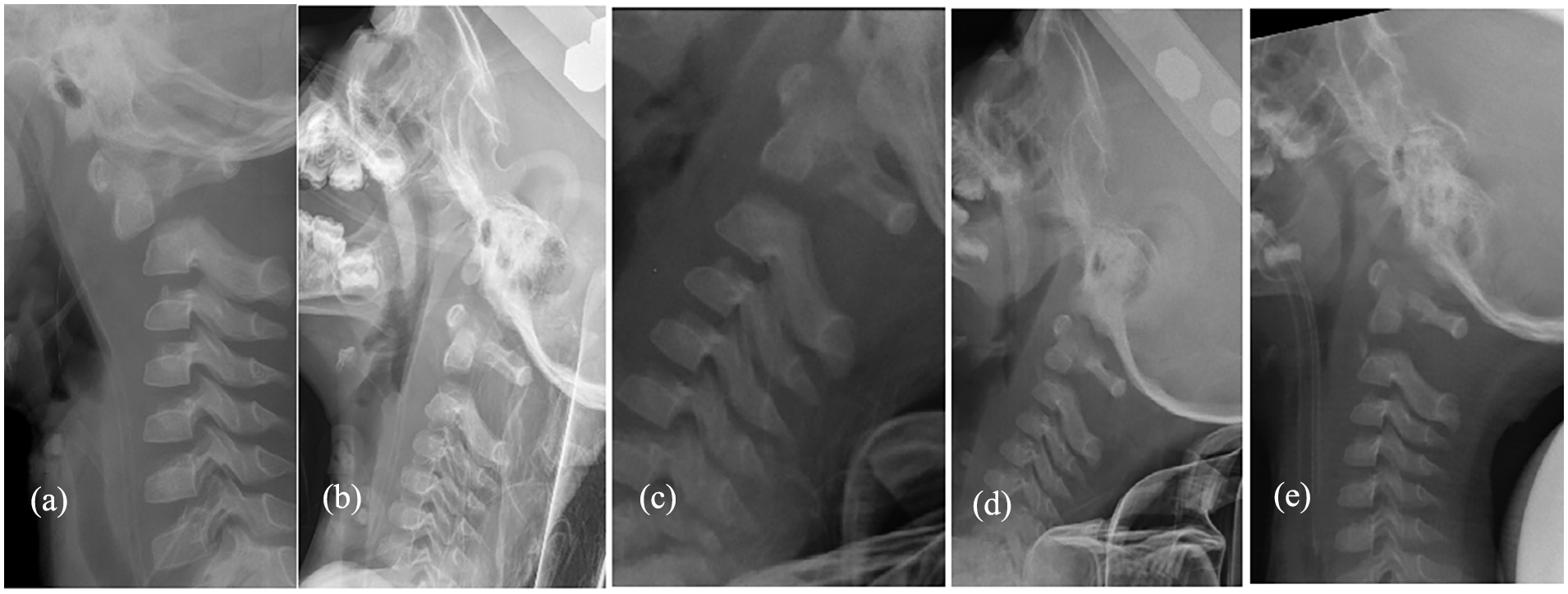
Case 1: Lateral radiography (a–e) showing successful reduction of C1-2 infra-anterior dislocation with odontoid fracture by skeletal traction (halo frame): (a) 1 day before traction; (b) 3 days after traction, the image confirms distraction of the odontoid fracture and the posterior elements of C1 and C2, it indicates the weight excessive and traction weight needs to be gradually reduced; (c) 6 days; (d) 14 days after traction; and (e) during the installation of Calot plaster vest (head–neck–chest plaster vest).
Because the patient was too young, C1-2 dislocation and odontoid reduction could not be maintained by appropriate inter-fixation, such as plate or screw, and long-term traction was also not suitable or safe. Thus, 19 days after traction, under successful anesthesia, the patient was placed in the “cross” position on a Jackson bed in the back position and subjected to occiputal-jaw traction and hip traction, protecting the cervical vertebrae. The halo frame was removed after routine disinfection, and then the patient was fitted with the Calot plaster vest (head–neck–chest plaster vest), with the anterior chest and abdomen part of the plaster removed for decompression to aid breathing. Meanwhile, bedside X-rays showed a good reduction in the extent of atlantoaxial joint dislocation. Later, MRI and CT re-confirmed the correct reduction (Figure 4). Meanwhile, the symptoms of right hemiplegia gradually improved, 24 days after Halo traction (5 days after installing the Calot plaster vest), myodynamia of the right upper and lower limb were both grade IV, and the child could raise upper limbs and wave to grab something, walk with a stable gait, and run with a slight limp.
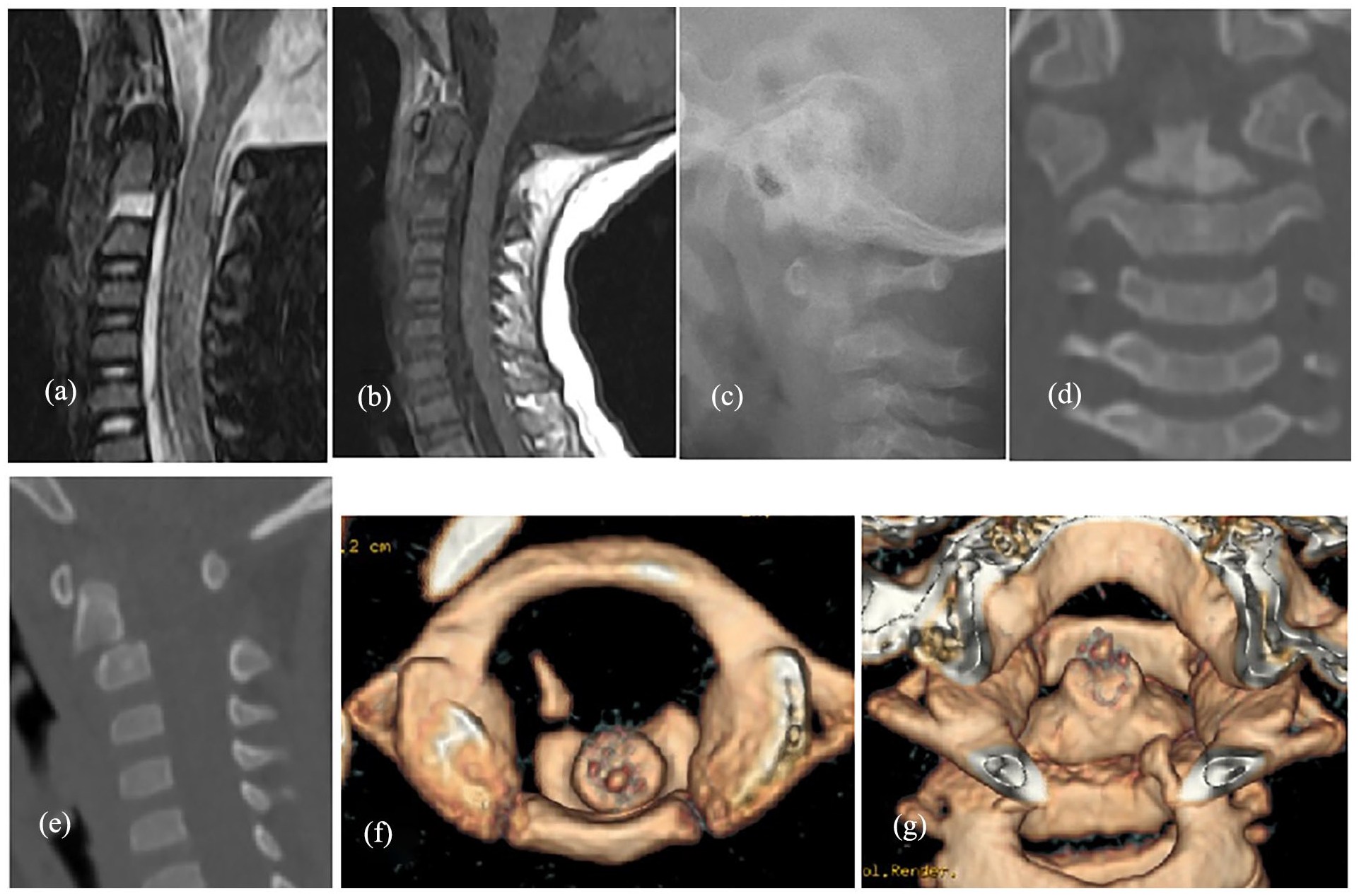
Case 1: (a–g) MRI, X-ray, and CT images showing successful maintenance of reduction in ADOF after installation of the Calot plaster vest. MRI (a, b) 3 days after fitting the vest; X-ray (c), CT (d–g) 1 month after fitting the vest.
Two-and-a-half months after the injury, the patient did not complain of neck pain; myodynamia of the right upper and lower limbs was both grade V. The Calot plaster vest was removed and a head–neck–chest brace was fitted and maintained for 3 months. One year after injury, plain radiographs, reconstructed two-dimensional and three-dimensional CT scans, and MRI of the cervical spine showed C1-2 joint reduction and healing of the C2 fracture in an acceptable position, with no abnormal motion of the C1-2 segments (Figure 5). Physical examination confirmed complete recovery of accompanying hemiplegia, with myodynamia of right limb grade V, muscle tension Ashworth Score 0, and painless and unrestricted ROM of the neck.
Case 1: (a-g) X-ray (a), CT (b,c), and MRI (d-g) 1 year after reduction following ADOF.
Case 2
This was a 2.7-year-old girl, who fell from the eighth floor of a building (based on the emergency medical history, and inpatient record). The patient was diagnosed at another hospital with traumatic ADOF (Anderson and D’Alonzo classification Type II, Hosalkar Type IB) and cervical spinal cord injury (MRI showed a slightly higher FS signal on local T2WI in the dorsal spinal cord at the Cervical-2 level), without neurological signs (accompanied by normal muscle tension, normal myodynamia with grade V), and the patient was only immobilized with a neck brace for ADOF. The patient had also suffered distal fractures of the right tibia and fibula, and rib fractures. Three days after the injury, the patient was transferred to our hospital.
Occipital-jaw traction was applied, and lateral radiography showed reduction of C1-2 infra-anterior dislocation. Fifteen days later, under general anesthesia, the patient was immobilized in a Calot plaster vest which was maintained for 2 months, without operation.
Two months later, the MRI showed fracture healing, without neurological signs, although spinal cord injury was still present. Then, the Calot plaster vest was removed, and a head–neck–chest brace was installed and maintained for nearly 3 months (Figure 6).
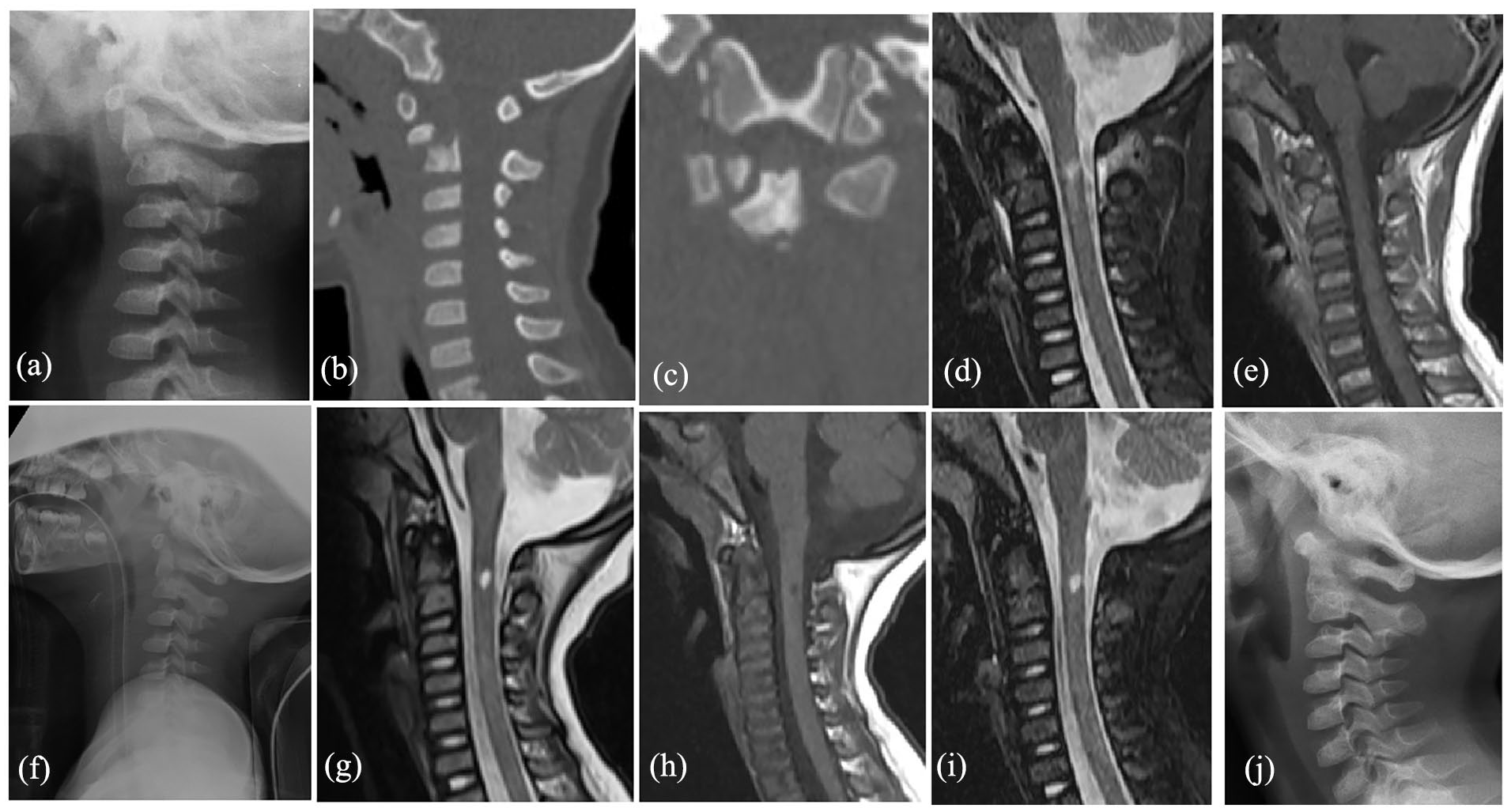
Case 2: A 2.7-year-old girl with ADOF (Anderson and D’Alonzo classification type II, Hosalkar Type IB). (a–c) Lateral radiograph and CT images showing ADOF. (d and e) MRIs showing ADOF and cervical spinal cord injury. (f and g) Lateral radiography (f) and MRI (g) showing successful reduction of C1-2 infra-anterior dislocation (during installation of head–neck–chest plaster vest, 15 days after occipital-jaw traction). (h, i) MRI showing bone healing 2 months after installing Calot plaster vest, although central myelomalacia still present. (j) Lateral radiography showing odontoid fracture healing 4 months after injury.
Case 3
This was a 2.5-year-old girl, who was accidentally pulled by her parents (based on the emergency medical history, and inpatient record), and consequently experienced pain and restricted ROM of the neck for 10 days, accompanied by normal limb muscle tension, and normal muscle strength with grade V. Ten days after the injury, the patient was sent to our hospital. X-ray, CT, and MRI images showed ADOF (Anderson and D’Alonzo classification Type II, Hosalkar Type IB) without cervical spinal cord injury, and with no neurological signs. Occipital-jaw traction was applied. Twenty-one days later, under successful anesthesia, the girl was fixed in a Calot plaster vest which was maintained for 2 months, without operation. Nearly 3 months after the injury, X-rays and CT scans showed fracture healing, the head–neck–chest plaster vest was removed, and a brace was fitted and maintained for 3 months (Figure 7).
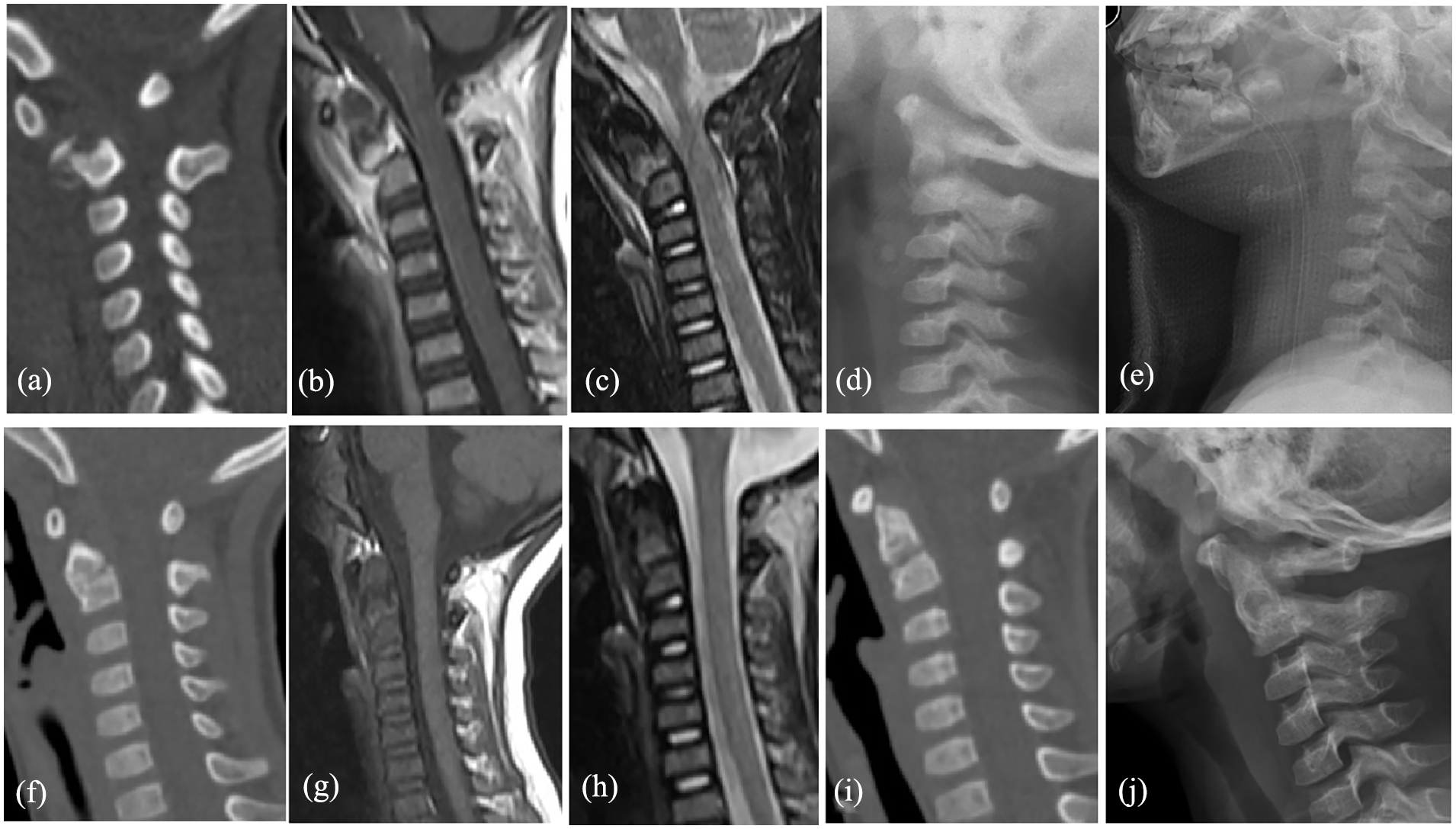
Case 3: A 2.5-year-old girl with ADOF (Anderson and D’Alonzo classification Type II). (a–c) CT (a) and MRI (b, c) showed ADOF 9 days after injury. (d) Lateral radiographic images showing the in-reduction process of C1-2 infra-anterior dislocation, 8 days after occipital-jaw traction and 18 days after injury. (e–h) Lateral radiography (e), CT (f), and MRI (g, h) showed successful reduction of C1-2 infra-anterior dislocation (during installation of Calot plaster vest), 21 days after occipital-jaw traction and 34 days after injury. (i) CT showing reduction of C1-2 and recovery 2 months after installing Calot plaster vest. (j) Lateral radiography showing odontoid fracture healing, 1.5 months after removal of Calot plaster vest and 4.5 months after injury.
Discussion
Traumatic ADOF in children is a complex and unstable injury, which is rarely reported.5 –8,15 Upper cervical spine (occiput to C3) injuries are more likely in younger children, for various anatomical reasons such as ligamentous laxity, relative head size, and incomplete ossification of the synchondroses. They are the most common cervical fracture in children under 7 years old. Above 8 years old, patterns of injury are increasingly likely to involve the lower cervical spine, resembling those seen in the adult.16 –18
In young children, open-mouth odontoid X-ray images are difficult to obtain, and the C1/C2 vertebrae are not visualized clearly in the anterior–posterior (AP) projection; thus, only the lateral projection may suggest an upper fracture.19 –21 In young children who have suffered neck injuries, especially those resulting from traffic accidents or falls, CT or MRI scans are recommended to diagnose an ADOF.
To date, a definitive treatment strategy has not been established. Treatment options in adults, including halo vest, cervical brace, anterior screw fixation, and posterior C1-2 fusion, are still controversial.9,22,23
Although there is insufficient evidence to suggest that any particular external immobilization method is better than another, external stabilization remains the treatment of choice for most cases. Razii et al.24,25 suggest that in such patients, even a fracture pattern with considerable angles can be successfully treated conservatively. Fassett et al. 26 reviewed the outcomes of 45 patients with conjunctival cartilage fractures and reported a fusion rate of 93% with external fixation, whereas Mandabach et al. 26 reported successful fusion of 80% pediatric C2 fractures using the halo device.
Hosalkar et al. 10 found that displacement of a fracture at the level of the synchondrosis of >100% (type IC) or a serious displaced fracture above the level of the synchondrosis (type II) indicates surgical arthrodesis (C1-2). In other situations, in situ immobilization in a halo body jacket or closed reduction with immobilization in a halo jacket has been suggested.
In our experience, all the ADOFs occurred at the base of the odontoid. According to the Hosalkar Classification, 10 case 1 belonged to type IC (suggested staged surgical arthrodesis; C1-2), while cases 2 and 3 belonged to type IB. All the patients underwent closed reduction with immobilization in a Calot plaster vest (head–neck–chest plaster vest), which resulted in bone healing and painless unrestricted ROM of the C-spine. These findings are in accordance with the results reported by other authors on non-operative treatment of C1/C2 fractures in young children.3,4,10
Occipital-jaw traction was the first choice, if cervical reduction could not achieved, Halo traction would be applied. We used halo traction for case 1 after failing in the initial occipital-jaw traction treatment of ADOF. Halo traction requires drilling holes and inserting half-nails into the skull to install the halo ring. The Halo device offers more precise positioning of cervical alignment and interferes less with mandibular movements, but potential risks include pin site infections, loosening/dislodging of the pins, and neurologic complications.27,28 So, we used occipital-jaw traction instead of halo traction in cases 2 and 3 and suggest using occipital-jaw traction as the preferred method.
Compared with previously reported cases, the cases we reported had the following characteristics. First, the patients were very young, all only 2 years of age. Second, prompt diagnosis and correct treatment were difficult: 67% (2/3 cases) diagnoses were delayed, with the duration before admission ranging from 3 to 10 days; only one of the three cases was diagnosed but not treated correctly. Third, Hosalkar 6 revealed that children with open synchondrosis had a comparatively lower incidence of traumatic brain injury, a higher rate of missed diagnosis, and a shorter mean stay in hospital. After such an injury, the spinal cord can be crushed by the displaced fracture, resulting in severe hemiplegia in some cases. Our cases confirm Hosalkar’s view. However, after traction and application of a Calot plaster vest, the patient recovered well, could have unrestricted ROM of the neck, and returned to life and activity like before the onset of symptoms, with no pain. Finally, in these cases, we provide complete X-ray, CT, and MRI images and photographs during the treatment to fully describe these processes to help other surgeons treat ADOF.
These specific injuries may usually be the results of shearing force that may include horizontal force or distraction forces on the neck.29,30 A biomechanical study was carried out using a child dummy to simulate a real car crash test, and it was revealed that frontal collision with absorption velocity ≥40 km/h was a typical injury mechanism in motor vehicle accidents of children under 3 years old. Neither child had neurological deficits, which is consistent with the literature where nerve damage has only been found along with head injuries. 31
Taking case 1 as an example, the girl was in the passenger seat (not obeying the traffic rules) and received a lateral impact force during the traffic accident. The child’s body was held by an adult, but the neck was not protected. The C1-2 dislocation with odontoid fracture resulted from horizontal force to the child’s head and hyperflexion of the neck, and at the same time, squeezing the cervical spinal cord caused right limb hemiplegia. Unlike the literature, 31 this child had no head injury, but the spinal cord in the neck was damaged, which also caused hemiplegia.
Cervical traction is mentioned in much literature, but there is almost no uniform standard for traction weight. Verhofste et al. suggested the mean halo-gravity traction was 29% ± 13.0% of body weight in adolescents 32 (nearly 1/6~2/5), Oae K suggested Halo traction of 10–30 kg weight was applied in adults 33 (nearly 1/10~1/7 of body weight). Therefore, we gradually explored in the clinic, that children are lightweight, and do not cooperate, it is best to achieve the ideal traction weight at one time. Traction weight is difficult to control. In case 1, 1.5 kg weight was used and could not achieve reduction of C1-2 infra-anterior dislocation with odontoid fracture in occipital-jaw traction at first. Later, 1/7 of the body weight was used in Halo traction, and the radiography indicated that the weight was too extreme, so we taper off. It is recommended that traction weight starts at 1/10 of the patient’s body weight and gradually increases.
Because of the traction, the spinal cord compression was relieved and the neurological symptoms improved. After the successful initial reduction of ADOF, this reduction was difficult to maintain by traction. If C1-2 joint fusion is performed by surgery as in adults, the future neck movement of the child will be adversely affected, and there was no sufficiently small internal fixation tool available. The use of the head–neck–chest plaster vest and brace overcame the above problems and ultimately achieved a good therapeutic effect. There is no consensus on the cervical immobilization period. After the open reduction with internal fixation, the patient was treated with immobilization in a cervical orthosis from 2 to 4 months in adults.5,7,15,34,35 In children, a rigid head–neck–chest plaster vest (such as Minerva cast, Halo vest, or Calot vest) could provide more stability to immobilize the close reduction of ADOF for 2 to 3 months. After the removal of the plaster vest, some authors suggested the children wear a soft collar brace for additional about 2–4 weeks.14,24,36 Repeat CT or flexion/extension radiographs of the cervical spine showed remodeling toward normal alignment with no evidence of instability at least 6 months after injury.24,36 Some authors suggested patients with Down Syndrome wore the head–neck–chest brace for 3–6 months after the operation. 37 We worried that the patient was too young and be injured again after the removal of the plaster vest, so we adopted brace protection for 3 months. In the future, with the increase in experience, we will consider gradually shortening the wearing time of the brace.
Case 1 had neurological symptoms, was given methylprednisolone shock therapy in the hospital nearby, and accepted methylprednisolone therapy for 5 days. Cases 2 and 3 had no neurological symptoms; they were not treated with the steroid therapy. There are few rehabilitation guidelines for concomitant neurological problems for pediatric ADOF; thus, we are working to find a standardized rehabilitation protocol for these patients in the future.
There were few available experiences to draw upon. For such patients, careful physical examination, X-ray, CT, MRI, and evaluation of the entire cervical spine could produce correct diagnoses. Careful nursing, positive cervical traction, and correct use of a head–neck–chest plaster vest and brace may be the keys to achieving ADOF reduction and ultimately, successful treatment.
The weaknesses of this study were that our follow-up was relatively short, and the number of children treated was relatively small.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241267107 – Supplemental material for Conservative treatment for traumatic atlantoaxial joint infra-anterior dislocation complicating odontoid fracture in young children: A case series
Supplemental material, sj-pdf-1-cho-10.1177_18632521241267107 for Conservative treatment for traumatic atlantoaxial joint infra-anterior dislocation complicating odontoid fracture in young children: A case series by Chunxing Wu, Yiming Zheng, Chuang Qian, Peng Huang, Bo Ning and Dahui Wang in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
All the authors have approved the final contents of the submission, been actively involved in the planning and enactment of the study, and have also assisted with the preparation of the submitted article.
Author contributions
C.W. contributed to manuscript preparation, performed measurements, and statistical analysis. Y.Z., C.Q., P.H., and B.N. performed measurements, cases collection, and statistical analysis. Dahui Wang contributed to study design, supervision, and validation.
Consent to participate
Since the participants were children (<18 years old), written informed consent from their parents to participate in the study had been obtained. The patients’ parents agreed to publish this study that includes information or images that could lead to identification of patients, and the patients’ parents signed the informed consent for publication of identifying information/images in an online open-access publication.
Consent for publication
The patients’ parents agreed to publish this study that includes information or images that could lead to identification of patients, and the patients’ parents signed the informed consent for publication of identifying information/images in an online open-access publication. The article has not been submitted elsewhere. The authors have read the Submission Guidelines and the paper conforms to this guide in all respects. The authors of this submission confirm that we have not published the same or a very similar study with the same or very similar results and major conclusions in any other journals. These include English or non-English language journals and journals that are indexed or not indexed in PubMed, regardless of different words being used in the article titles, introduction, and discussion. All the authors have approved the final contents of the submission, been actively involved in the planning and enactment of the study, and have also assisted with the preparation of the submitted article. The authors of this submission understand that dual submission refers to publication in any language and that dual submission will result in academic sanctions which will include the blocking of all authors to prevent their future submissions to Journal of Children’s Orthopedics.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by institutional ethics board of Children’s Hospital of Fudan University (No. (2020) 523). All the authors have approved the final contents of the submission, been actively involved in the planning and enactment of the study, and have also assisted with the preparation of the submitted article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key Research and Development Program of China (No. 2021YFC2701003) and the Science and Technology Commission of Shanghai Municipality (No. 21Y11911500).
Availability of data and material
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request. All data generated or analyzed during this study are included in this published article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.