
Abstract
Purpose:
This study aimed to compare the clinical and radiographic outcomes of traction to assist reduction in patients with late-detected developmental dislocation of the hip using the Petit-Morel technique versus the Bryant overhead traction technique, and to compare the clinical and radiographic outcomes of these two traction techniques with immediate closed reduction.
Methods:
A comprehensive systematic search of the MEDLINE/PubMed, EMBASE, and Web of Science databases was performed to identify relevant studies. Studies on Petit-Morel and overhead traction techniques and immediate closed reduction were then screened, selected, and data collected; included studies were assessed using the Methodological Index for Non-Randomized Studies criteria.
Results:
In total, 22 studies met the inclusion criteria. The Petit-Morel group had a successful reduction rate of 87% while the overhead traction group had a successful reduction rate of 67.1%, and the immediate closed reduction group had a successful reduction rate of 78.4% (Petit-Morel versus overhead traction, p < 0.001; overhead traction versus immediate closed reduction, p < 0.001, Petit-Morel versus immediate closed reduction, p = 0.021). The Petit-Morel group had an overall avascular necrosis rate of 2.7%, compared to 10.6% for overhead traction and 21.5% for immediate closed reduction (Petit-Morel versus overhead traction, p = 0.001; Petit-Morel versus immediate closed reduction, p < 0.001; overhead traction versus immediate closed reduction, p < 0.001). The Petit-Morel group achieved a satisfaction rate of 86.4% according to the Severin classification, as compared to 71.2% in the overhead traction group and 76.4% in the immediate closed reduction group (Petit-Morel versus overhead traction, p < 0.001; Petit-Morel versus immediate closed reduction, p = 0.018; overhead traction versus immediate closed reduction, p = 0.195).
Conclusion:
Petit-Morel and overhead traction techniques did not outperform immediate closed reduction in terms of redislocation rates, and radiological satisfaction, the Petit-Morel technique, has lower clinically significant avascular necrosis rates than overhead traction and immediate closed reduction.
Level of evidence:
Level III.
Introduction
Developmental dislocation of the hip (DDH) is a common orthopedic condition in pediatric patients. Diagnosis and treatment of newborns with DDH have been revolutionized by neonatal screening by clinical examination and ultrasound, but remain problematic for those with late-detected DDH.1 –4 The preferred treatment methods for patients younger than 18 months with late-detected DDH are closed reduction (CR), immediate or after a period of traction, and immobilization with a spica cast. 1
While traction to gradually reduce a dislocated hip is not a new concept, it deviates from the immediate CR (ICR) that is typically performed in most institutions worldwide. In particular, research suggests that traction may reduce the incidence of femoral head avascular necrosis (AVN) and the need for open reduction (OR) as opposed to immediate reduction.5 –10
There are two techniques commonly used to apply traction to treat DDH: the Petit-Morel (PM) technique 8 (Figure 1) and the Bryant technique 11 (Figure 2). Both procedures aim to gradually reduce a dislocated hip without forceful reduction. This principle suggests that gradual reduction stretches the soft tissues, thus reducing the risk of AVN, which is thought to result from excessive pressure on the hip joint. The two techniques share the same principles, although the traction is applied differently. The PM technique begins with traction along the plane of the bed and progressively increases hip flexion and internal rotation as the reduction progresses. In contrast, the Bryant technique is performed with the hip at 90° of flexion and the knee extended throughout all stages of the treatment. At the end of the traction period, both techniques require immobilization of the hip in a spica cast to facilitate penetration of the femoral head into the acetabulum.8,12,13

Photo of the PM technique showing abduction and internal rotation of the hip to facilitate reduction of the proximal femoral epiphysis into the acetabular cavity. 10

Several publications have reported treatment outcomes for both traction methods, although no direct comparisons have been made between the radiographic and clinical outcomes of the PM technique and the overhead Bryant technique.5,6,14 In addition, there is currently no consensus on the benefits of this approach, as there is no definitive evidence on whether preliminary traction with either technique is superior to immediate reduction in terms of rates of AVN, residual acetabular dysplasia, and reduction failure in patients with late-detected DDH.1,14 –16
The primary objective of this systematic review is to compare the clinical and radiographic outcomes of traction to assist reduction in patients with late-detected DDH using the PM technique versus the OHT technique. The secondary objective is to compare the clinical and radiographic outcomes of these two traction techniques with ICR.
Materials and methods
Literature search
A comprehensive search of the MEDLINE/PubMed, EMBASE, and Web of Science databases was conducted from their inception through August 2023. The Boolean search operators and terms used for this search were as follows: ((((((((((((((((Hip Dislocation, Developmental) OR (Developmental Hip Dislocations)) OR (Developmental Hip Dislocations)) OR (Developmental Hip Dislocations)) OR (Developmental Hip Dislocations)) OR (Developmental Hip Dysplasias)) OR (Dysplasia, Developmental Hip)) OR (Hip Dysplasia, Developmental)) AND (Closed Reductions)) OR (Reduction, Closed)) OR (Reductions, Closed)) OR (Closed Reduction)) OR (Reduction, Closed)) OR (Reductions, Closed)) AND (Traction)) OR (Preliminary traction)) OR (Pre-reduction traction). Without exception, this exact set of search terms was used to conduct the literature search in all selected databases. The use of multiple databases and multiple variations of the search terms significantly reduced any potential bias in the selection of articles. We prepared and presented the results of our systematic review in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement.
Eligibility criteria
Studies were eligible for inclusion if they met the following criteria: (1) otherwise normal children with DDH treated with the PM or OHT technique or ICR; (2) articles published in English; and (3) studies reporting on a series of at least 10 hips with a follow-up of ≥ 5 years. We did not include studies with a shorter follow-up because late-onset symptoms could not be excluded. Other exclusion criteria included children with underlying diseases and syndromes, such as cerebral palsy or hip dislocation due to teratology, opinion or review articles. We also screened the reference lists of included articles for additional relevant studies.
In addition, the quality of the included literature was assessed using the Methodological Index for Non-Randomized Studies (MINORS) item quality evaluation checklist; only studies with MINORS > 12 were included. 17
Study selection
Three investigators independently reviewed article titles and abstracts, excluding duplicates, using the inclusion criteria as a guide. The senior investigators had the final say in cases of disagreement. For all studies that successfully passed the initial screening and for those that required clarification, a full-text evaluation was performed to determine eligibility. Specific data extracted from the selected studies included: (1) general study details such as author name, year of publication, and study duration; (2) type of treatment: PM technique, OHT technique, and ICR; (3) patient demographics, such as age at treatment, gender, duration of treatment, average follow-up; (4) details of surgical treatment, if any; and (5) key outcome measures, including AVN rate, Severin classification, reduction rate, incidence of redislocation, and total hip arthroplasty (THA) at long-term follow-up. Redislocation was defined as evidence of hip dislocation on anteroposterior (AP) pelvic radiographs at the time of postoperative follow-up. In this study, late diagnosis was defined as children with an average age of more than 3 months at diagnosis or those who had a delayed review or investigation as part of the screening program.18,19
Evaluation of the AVN
There are several classification systems for grading the severity of AVN, including the Kalamchi–MacEwen 20 and Bucholz–Ogden 21 systems. In both classifications, Type 1 AVN represents reversible ischemia without collapse and is not considered clinically significant. The rates of clinically significant AVN, defined as Type 2 or higher according to the Kalamchi–MacEwen and Bucholz–Ogden classification systems, were documented. Types 3 and 4 AVN, representing partial and complete collapse of the femoral head, respectively, were also considered clinically significant and were combined into a collective Type 3 group for analysis. In cases where the AVN pattern was non-specific, we could only make a distinction of its presence or absence.
Evaluation of the outcome
Considering the works of Bache et al. 22 and Koizumi et al., 23 we considered Severin 24 Grades 1 and 2 as satisfactory, while Grades 3–6 were considered unsatisfactory results.
Statistical analysis
Qualitative statistical analysis was performed using SPSS (IBM SPSS Statistics for Macintosh, version 25.0). When available, statistical analyses were performed, including chi-square and Student’s t-tests to compare categorical and continuous variables, respectively. For multiple comparisons, Bonferroni correction was applied (α = 0.05/3 = 0.0167). Due to limited and heterogeneous reporting, these data could not be combined in a meta-analysis. A p-value of less than 0.05 was considered to be statistically significant.
Results
Study selection and general characteristics
The initial online literature search identified 4433 publications (1239, 1425, and 1769 in MEDLINE/PubMed, EMBASE, and Web of Science, respectively). A total of 4376 were excluded, and 5 review articles were identified for further evaluation of additional references. As a result, 52 full articles were retrieved for review and confirmation of eligibility. Reference list searches identified two additional articles for a total of 54 studies for review. After review, a total of 32 articles were excluded: 4 were either meta-analysis or reviews, 11 had inadequate follow-up or documentation of AVN, 14 used a different treatment method; and 3 did not clarify the treatment protocol. This left 22 studies (1589 patients and 2187 hips) that met all the inclusion criteria. Four studies had the two same first authors but provided sufficient independent data to use the information from each study (Figure 3). The mean MINORS 17 score of the included studies was 16.2 ± 3.4.
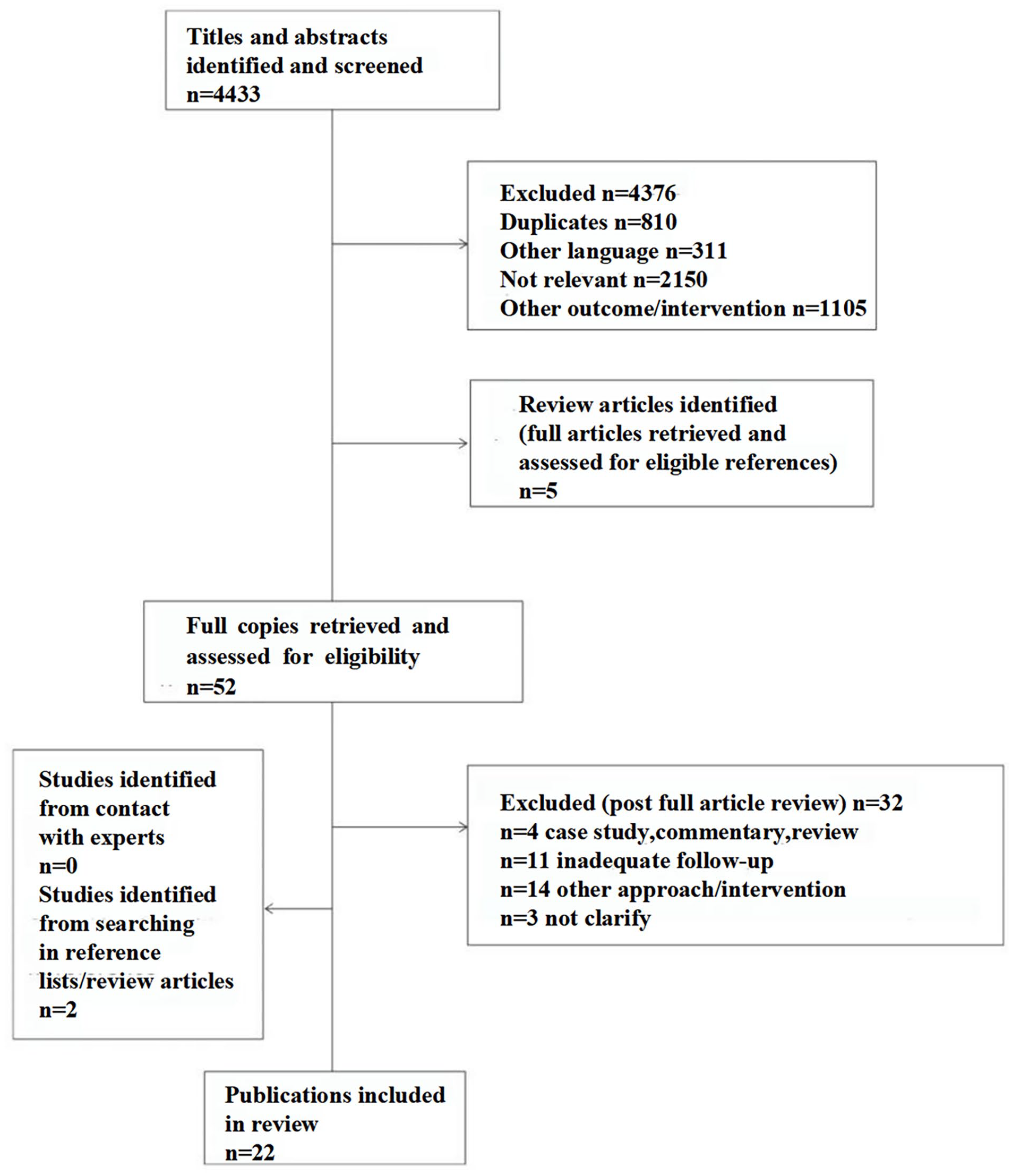
Literature review flowchart.
Demographics of included studies
A total of 186 hips (n = 93 patients but one article did not report the number of patients) with late-detected DDH underwent traction with the PM technique, with a mean age at treatment of 21.7 (mean age range from 19 to 23) months and a mean follow-up period of 20.2 (5 to 43) years. In the OHT technique group, there were 1289 hips (n = 762 patients but one article did not report the number of patients) with a mean age at treatment of 10.2 (mean age range from 3.7 to 33 months) and a mean follow-up of 11 (0.25 to 40) years (Table 1). In the ICR group, 712 hips (n = 480 patients but two articles did not report the number of patients) were treated at a mean age of 14.4 (mean age range from 7.9 to 27.3) months with a mean follow-up of 10.6 (2 to 67) years (Table 2). Of the nine available articles, the mean traction time was 27.2 (17–70) days in the PM group and 23.8 (8–76.3) days in the OHT group (p = 0.07).
General characteristics of the included studies.
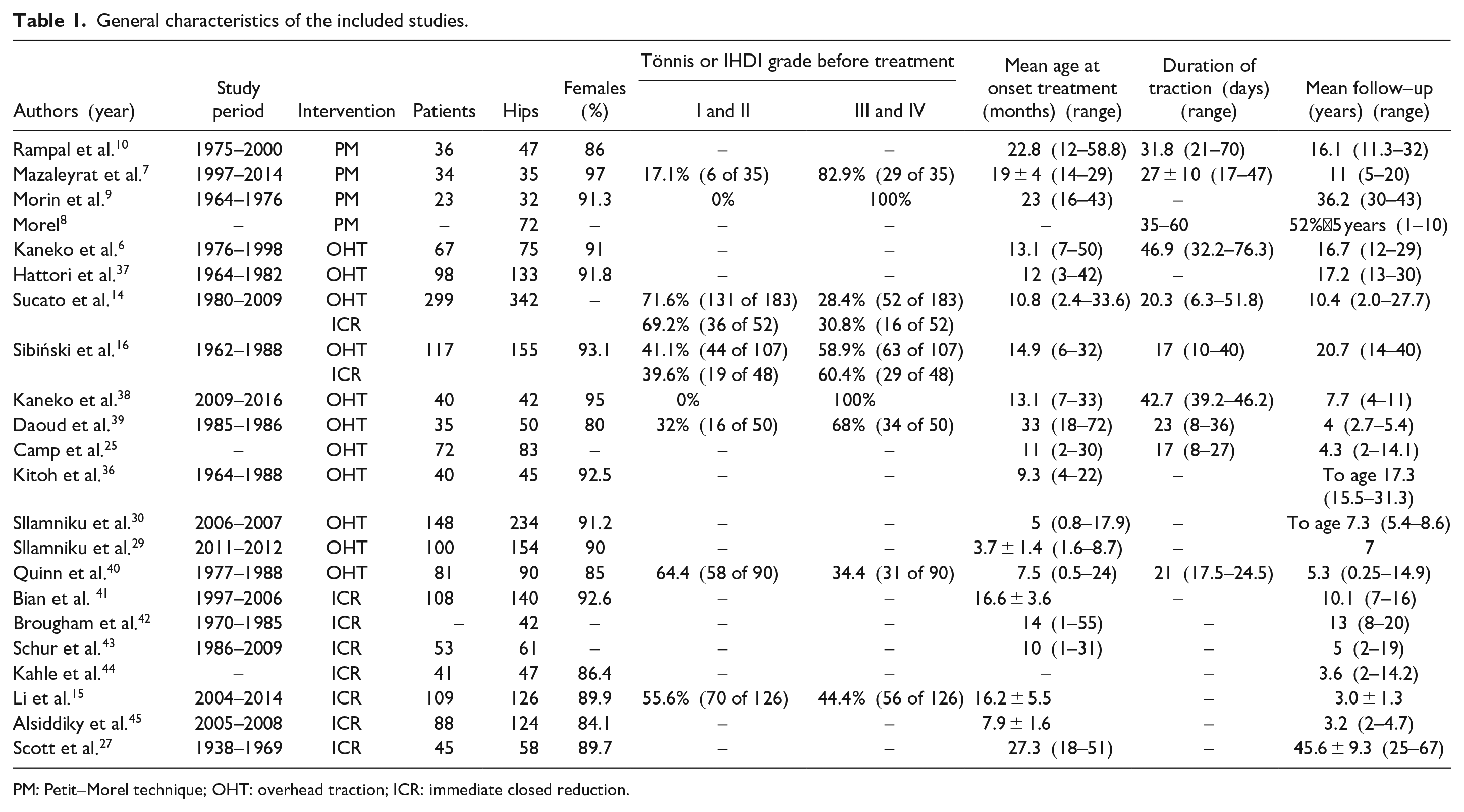
PM: Petit-Morel technique; OHT: overhead traction; ICR: immediate closed reduction.
Demographic characteristics of the included studies.
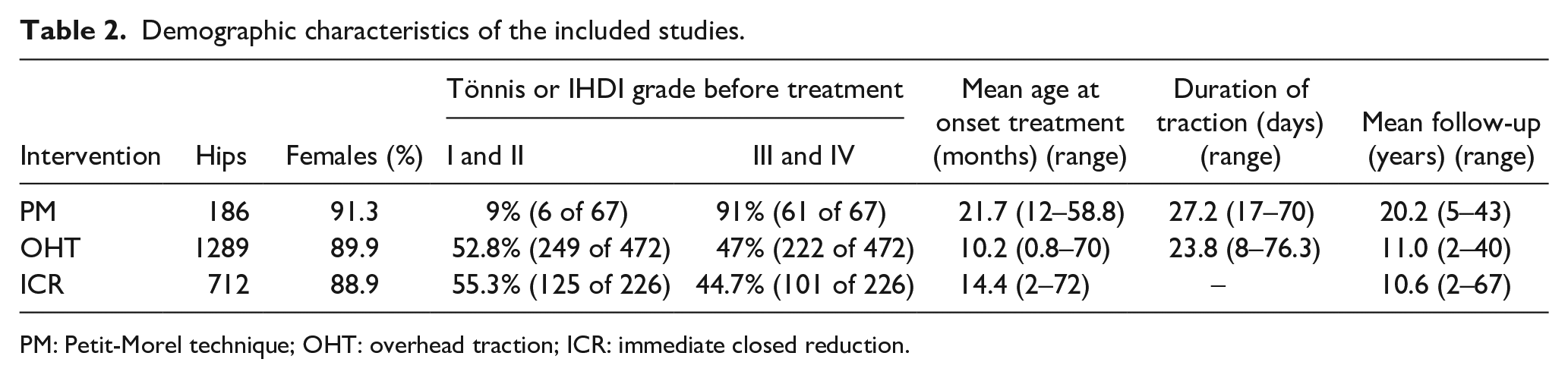
PM: Petit-Morel technique; OHT: overhead traction; ICR: immediate closed reduction.
Parameters evaluated included reduction rate, incidence of overall and clinically significant AVN, redislocation rate, THA rate, and Severin grade. Notably, 20 studies were conducted at a major medical center and 1 study was a multicenter study, although funding sources were not disclosed in 2 of 21 papers. Two studies specifically compared ICR and OHT techniques (Table 3).
Clinical outcomes of patients included in the study.
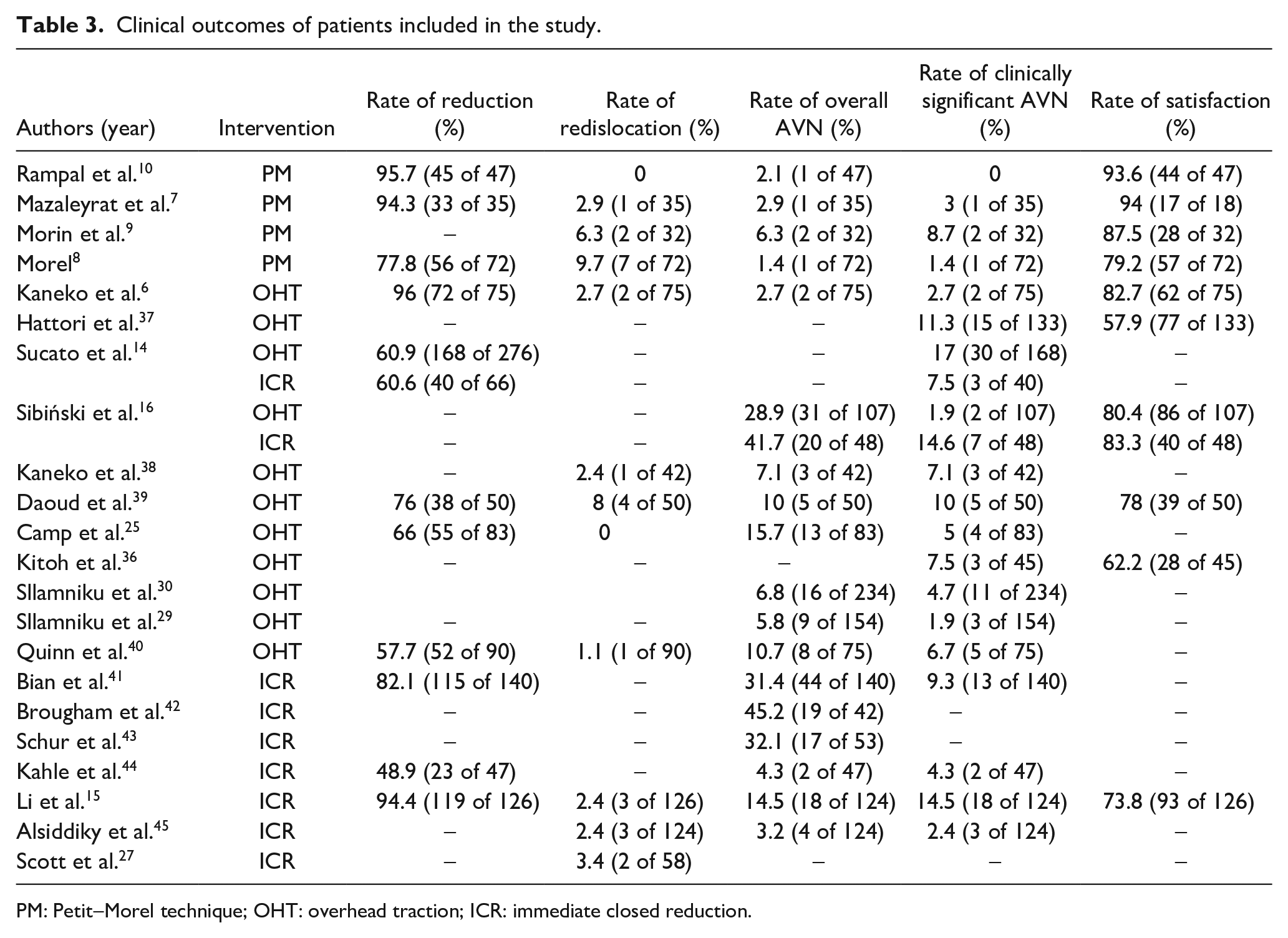
PM: Petit-Morel technique; OHT: overhead traction; ICR: immediate closed reduction.
Rate of successful reduction
In total, 12 studies reported successful reduction rates. The PM group had a reduction rate of 87% (134 of 154 hips), while the OHT group had a reduction rate of 67.1% (385 of 574 hips), and the ICR group had a reduction rate of 78.4% (297 of 379 hips). Statistically significant differences in reduction rates were observed between the PM and the OHT groups (p < 0.001), and between the OHT and ICR groups (p < 0.001), but the difference between PM and ICR groups was not statistically significant (p = 0.021, p-values are significant at p < 0.0167) (Table 4).
Comparison of the therapeutic effects of different types of treatment modalities.
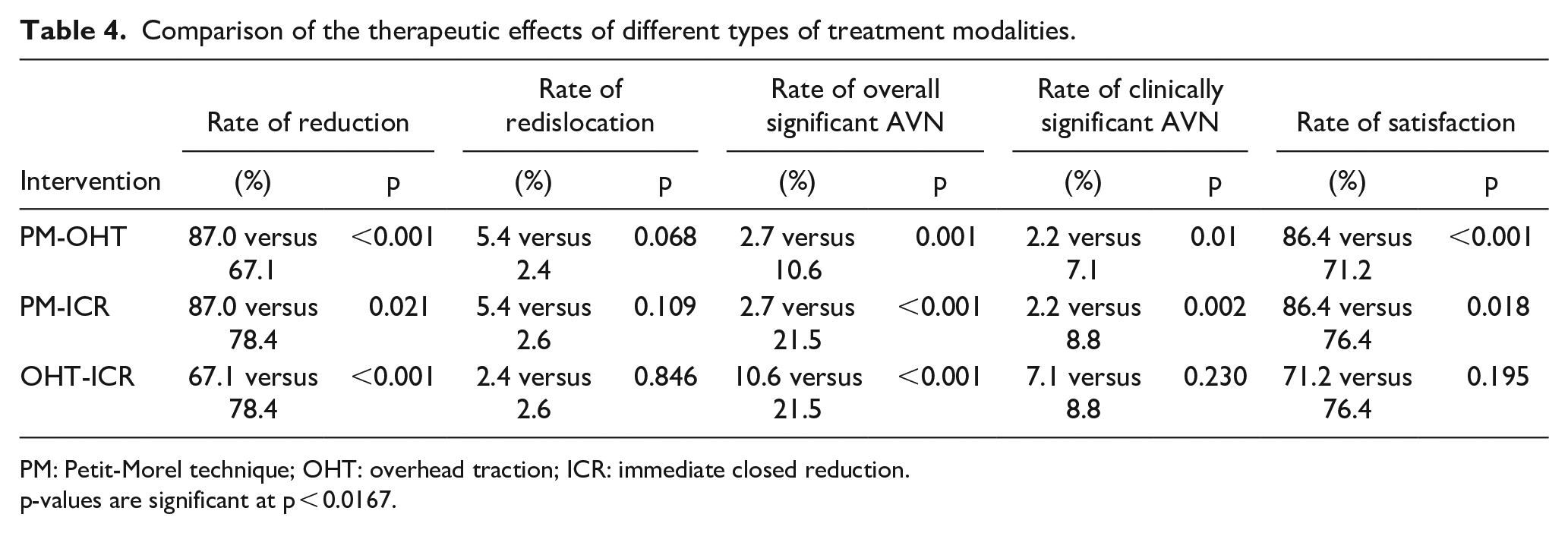
PM: Petit-Morel technique; OHT: overhead traction; ICR: immediate closed reduction.
p-values are significant at p < 0.0167.
Early complications
Of the included literature, early complications were considered by two articles. In Camp et al.’s 25 study, two patients had skin irritation after treatment with OHT method, and while in Rampal et al.’s 10 study, no patients had related complications after treatment with PM method.
Rate of redislocation
In total, 12 studies reported redislocation rates: the PM group had a rate of 5.4% (10 of 186 hips), while the OHT group had a rate of 2.4% (8 of 340 hips), and the ICR group had a rate of 2.6% (8 of 308 hips). However, there was no significant difference between the three groups (PM versus OHT, p = 0.068; PM versus ICR, p = 0.109; OHT versus ICR, p = 0.846) (Table 4).
Rate of overall AVN and clinically significant AVN
Notably, 18 studies included data on the incidence of overall AVN. The PM group had a rate of 2.7% (5 of 186 hips), compared to 10.6% (87 of 820 hips) in the OHT group, and 21.5% (124 of 578 hips) in the ICR group. Statistically significant differences in clinically significant AVN rates were observed when comparing the PM group against to both the OHT and ICR groups (PM versus OHT, p = 0.001; PM versus ICR, p < 0.001; OHT versus ICR, p < 0.001).
Moreover, 19 studies included data on the incidence of clinically significant AVN. The PM group had a rate of 2.2% (4 of 186 hips), compared to 7.1% (83 of 1166 hips) in the OHT group, and 8.8% (46 of 523 hips) in the ICR group. Statistically significant differences in clinically significant AVN rates were observed when comparing the PM group against to both the OHT and ICR groups (PM versus OHT, p = 0.01; PM versus ICR, p = 0.002; OHT versus ICR, p = 0.23) (Table 4).
Rate of THA
The rate of THA at last follow-up visit was reported in two studies. In the PM group, the rate was 3.1% (1 of 32 hips) after 33 years of follow-up; while in the ICR group, 29% of the hips had undergone THA at 40 years of follow-up. In both samples, the percentage of THA nearly doubled over the next decade, increasing to 50% (29 of 58 hips) at 48 years. Notably, no cases of THA were reported in the OHT group with a mean follow-up ranging from 4 to 20.7 years.
Rate of radiological satisfaction
A total of 11 studies recorded the Severin grade at the final follow-up. The PM group achieved a satisfaction rate of 86.4% (146 of 169 hips), as compared to 71.2% (292 of 410 hips) in the OHT group and 76.4% (133 of 174 hips) in the ICR group. Statistically significant differences in satisfaction rates were found only between the PM and OHT groups (PM versus OHT, p < 0.001; PM versus ICR, p = 0.018; OHT versus ICR, p = 0.195, p-values are significant at p < 0.0167) (Table 4).
Discussion
The aim of this systematic review was to compare the clinical and radiographic outcomes of traction (PM and OHT techniques) to assist reduction versus ICR in patients with late-detected DDH. While this study found that in patients with late-detected DDH, we observed that the PM and OHT techniques did not outperform ICR in terms of redislocation rates and radiologic outcomes, and the PM technique has lower clinically significant AVN rates than OHT and ICR.
Despite the fact that several studies have compared the OHT technique to ICR, there is a lack of research comparing the outcomes of different traction techniques or comparing the PM technique to ICR. Furthermore, there are no reports comparing THA rates between the three different reduction modalities, PM, OHT, and ICR. Therefore, caution should be exercised when interpreting data supporting or opposing the use of traction, as it is still uncertain whether traction is more effective than ICR in the long term.26,27
Specifically, Graf Type III and Type IV were eccentric hips with a poor bony roof, flattened rim, and labrum pressed up and down, respectively.28 –30 Femoral head AVN is a serious complication associated with the pathologic changes induced by DDH and its treatment. It causes deformity and premature joint degeneration. Our analysis showed a clinically significant AVN rate of 2.2% in the PM group as opposed to 7.1% in the OHT and 8.8% in the ICR groups. This difference is likely due to the precise and gradual descent and femoral head positioning facilitated by the PM method.7 –10 The gradual reduction allows for stretching of the contracted soft tissues, leading to a decrease in the incidence and severity of growth disturbances of the proximal femoral epiphysis while minimizing vascular disruption to the proximal femur. This may reduce the incidence and severity of growth disturbances of the proximal femoral epiphysis and facilitate reduction.8,10,16 Our results suggest that while ICR has some advantage over traction, it does not provide the same degree of protection against AVN as gradual techniques.
The goal of treatment of DDH is to achieve a stable, well-centered reduction that restores normal hip anatomy and function while preventing AVN.8,10 The PM method is more effective in reducing DDH, with a success rate of 87% compared to OHT (67.1%) and ICR (78.4%) techniques. The progressive and gentle reduction also results in better preservation of the reduction, resulting in a redislocation rate of 5.4%, similar to OHT and ICR techniques.
Treatment satisfaction results confirm the efficacy of the PM technique. A satisfaction rate of 86.4%, based on the Severin classification, surpassed the success rate of the OHT and ICR techniques. Despite OR being an option to handle reduction obstacles and dysplasia, it poses a risk for joint damage.31,32 The PM technique balances less invasive treatment with good reduction quality. Morel suggested using hip traction with abduction and internal rotation to gradually reduce the dislocated hip, and later correcting residual acetabular dysplasia with pelvic osteotomy. 8 Younger age at reduction also is important to allow for acetabular remodeling, 10 although the mean age of patients undergoing CR with PM technique was higher than with other techniques.
When the two traction techniques were compared, the PM technique produced better results than the OHT technique. This may be due to differences in the orientation of the traction. However, the PM technique requires hospitalization,7 –10 whereas the OHT technique can be performed in an outpatient setting, improving access and reducing costs, although it is dependent on parental compliance.5,25 In addition, OHT protocols are not well standardized.33 –35 Differences in specific techniques, traction force, abduction and rotation, inpatient versus outpatient settings, and the total traction duration could have a significant impact on outcomes.5,6,36 Monitoring for compliance with outpatient traction was generally inadequate.5,25 Inpatient admission for PM traction or transition to inpatient OHT for the last 1–2 weeks before reduction may optimize outcomes when compliance is uncertain. In addition, although it was not possible to perform a detailed cost analysis, it is worth mentioning that ICR is less expensive in terms of cost and time for patients and families compared to PM and OHT because there is no need for long-term traction and the associated hospitalization.
The current systematic review of the literature showed no clear advantage of preliminary traction over immediate reduction of a dislocated hip, although the PM technique has a lower rate of AVN and a higher rate of concentric reduction than the other techniques. However, the number of cases treated with PM is 10 and 6 times lower than those treated with OHT and ICR, respectively, which could explain the lower complication rate despite the longer average follow-up. In addition, the age of patients treated with the PM technique was significantly higher (21.7 months) than that of patients treated with OHT (10.2 months) and ICR (14.4 months). Hips treated with the PM technique are therefore more mature and less exposed to the risk of AVN than those treated with the other techniques.1,8,10 The management is different in the infant where the hips have not been subjected to weight-bearing and in children as old as 5 or 6 years. However, due to the limitations of the original literature, it was not possible to collect relevant information on the weight-bearing age of the children and it was not possible to perform an effective subgroup analysis. This study included patients with a mean age ranging from 3.7 to 33 months, with individual differences, but the vast majority of the age distribution was concentrated between 0 and 3 years.
This analysis has limitations worth noting. The studies we included were retrospective case series, which may have introduced some selection and observer bias. Patient factors such as age, plaster cast immobilization after traction, duration of cast application, and severity of hip dislocation may have differed between groups, affecting the results. Moreover, in this study, spanning nearly five decades, imaging and treatment modalities have evolved, although the principles supporting the CR methods by progressive traction remained the same. Therefore, the analysis of our results should be interpreted with caution, although the impact of modern imaging technology has not influenced the modality of treatment, as the basic principles remained the same. High-quality studies that compare results in a prospective manner, with strict control of outcome variables, would provide more robust evidence. Nonetheless, we collected several studies to establish a substantial sample size with sufficient follow-up. This allowed us to compare the effectiveness of traction techniques with ICR and determine their outcomes. Recently, Scott et al. 27 conducted a study on managing DDH in children diagnosed after 18 months old. Participants were followed for at least 40 years while the outcomes of CR and OR with Salter osteotomy were compared. Both treatment options improved THA-free survival, but neither option was effective in preventing osteoarthritis or the need for THA. This finding may be related to the natural history of the disease rather than the specific treatment used. The same rationale can be applied to patients treated with traction.26,27 It is worth noting that only two of the included studies provided data on total hip replacement (THR) rates, and the results should be interpreted with caution due to limited follow-up. Therefore, it is possible that the rate would increase with longer follow-up. Further studies are needed to compare the long-term need for THR among the three treatment options.
Conclusion
In conclusion, this study found that in patients with late-stage DDH, the PM and OHT techniques do not outperform the ICR in terms of redislocation rates and radiologic outcomes, but the PM technique has lower clinically significant AVN rates than the OHT and ICR. Surgeons should consider the advantages and disadvantages of each of these three methods to adapt to local conditions, disease severity, and family expectations.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241265603 – Supplemental material for Comparative long-term outcomes of Petit-Morel versus overhead traction methods versus immediate closed reduction for late-detected developmental dysplasia of the hip: A systematic review
Supplemental material, sj-pdf-1-cho-10.1177_18632521241265603 for Comparative long-term outcomes of Petit-Morel versus overhead traction methods versus immediate closed reduction for late-detected developmental dysplasia of the hip: A systematic review by Lian Duan, Federico Canavese, Weizheng Zhou, Yufan Chen and Lianyong Li in Journal of Children’s Orthopaedics
Footnotes
Author contributions
L.D. contributed to data collection and analysis, and article preparation. W.Z. and Y.C. involved in data collection and analysis. L.L. and F.C. proposed research idea, data analysis, and article revision. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Author’s Note
Federico Canavese is also affiliated to Orthopedic and Traumatology Department, IRCCS Istituto Giannina Gaslini, Genova, Italy and DISC-Dipartimento di scienze chirurgiche e diagnostiche integrate, University of Genova, Genova, Italy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
This article does not contain any studies with human participants or animals performed by any authors. Informed consent was not required for this work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.